
Abstract
Background:
New graduate role transition for nurses and teachers is stressful. Poor adaptation may manifest as insomnia, which has implications for the new professionals, their employers, and the public served. This study examines factors that impact new graduate sleep, with the aim of identifying perceived helps and hindrances to sleep-during-transition.
Methods:
Targeted content analysis of transcripts from a larger longitudinal mixed methods study comparing new graduate sleep during their first year of practice. Study participants (N = 21) answered questions in the final interview regarding the most positive and negative impact(s) on sleep during the transition year. Transcripts were analyzed and compared based on the new graduate sleep typology (i.e., Got Better, Got Worse, Stayed Varied) which emerged from the parent study.
Findings:
Most participants, regardless of sleep type, identified a person/group as most positively impacting sleep. They identified work thoughts, stress/anxiety, people, work hours/sleep schedules, and environmental factors as negatively impacting sleep. Work thoughts and stress/anxiety were mentioned together and most frequently by participants in all three sleep types.
Conclusion/Applications to Practice:
This study provided insight into new graduate nurse and teacher sleep during transition. Support persons and/or groups may be essential regardless of sleep type. Thought management/stress mitigation strategies and good sleep hygiene may also improve the sleep experiences of these new professionals. Occupational health nurses can support sleep-during-transition among new nurses and teachers by acting as sleep advocates. They may also identify a need for medical intervention and/or sleep specialists and should promote fatigue risk mitigating policies.
Background
In the 2018 to 2019 academic year, more than 335,000 education and health professions students graduated from higher education (National Center for Education Statistics [NCES], 2020). The majority likely experienced the higher education to professional practice (HEPP) role transition upon joining the workforce. Many new graduates consider this psychosocial transition process to be stressful (Gong et al., 2021; Hettich, 2010), and may affect sleep during the first year (Bannai et al., 2015; Kim & Lee, 2022). The authors present an analysis of positive and negative impacts on sleep during their first year of practice as experienced by new graduate nurses (NGNs) and new graduate teachers (NGTs). They also recommend ways occupational health nurses and other organizational leaders can support the sleep of NGNs and NGTs during their first year of practice.
The HEPP role transition process involves three distinct stages, referred to as transition shock, transition crisis, and transition recovery. This psychosocial process seems to occur over a 9- to 12-month timeframe based on a synthesis of perspectives from nursing (Duchscher, 2008), education (Corcoran, 1981; Friedman, 2000), and occupational psychology (Williams, 1999) (see Figure 1). Transition shock occurs during the initial 4 months of practice. The new graduate is aware of a steep learning curve, has a strong desire to “fit in,” often feels a pressure to “perform,” and subsequently may conceal feelings of inadequacy. During transition crisis, or months 5 to 8 of practice, the new graduate perceives a conflict between one’s ideals and current realities in the new role. The person is growing in knowledge and skills, but experiences a paradoxical loss of confidence, while feeling overwhelmed and isolated. Resolution of this stage opens the door for transition recovery (i.e., 9 months onward); the new graduate detects growth, has a new sense of calm, and feels more at ease in the role. Incomplete or inadequate transition can prolong the experience, and/or may result in the new graduate employee leaving the organization or even the profession.
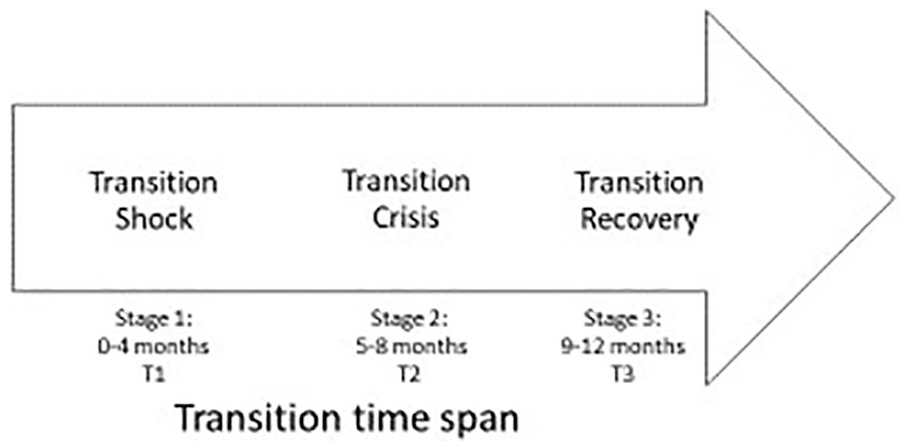
Theoretical higher education to professional practice (HEPP) role transition time span.
In the United States, nurse residency and teacher induction programs aim to orient new graduates to the organization and/or role, while supporting the transition process (Ingersoll et al., 2014; Sutor & Painter, 2020). However, problems of anxiety and stress during transition persist (Lin et al., 2020; Murray et al., 2020). Furthermore, consensus on program structure and content continues to evolve for NGN and NGTs. Most lack program-level health-related outcomes, and many do not include content involving stress reduction and/or sleep management (American Association of Colleges of Nursing [AACN], 2017; Melnyk et al., 2013; Ohio Department of Education [ODE], n.d.). Sleep content is also absent from formal teacher mentor (Mentor Modules, n.d.; ODE, n.d.) or nurse preceptor training (National Council of State Boards of Nursing [NCSBN], Learning Extension, n.d.).
Sleep deficiency among the U.S. workforce, including short sleep duration, poor sleep quality, untreated sleep disorders, and/or timing of sleep out of alignment with the employees’ circadian rhythms, places workers at risk for occupational injuries, and adverse health outcomes (Caruso et al., 2017). Little is known about NGN or NGT sleep, which is concerning for potential disruption due to adjustment or anxiety-related insomnia, that may be associated with the new employee role transition (Schwab, 2020). NGNs and NGTs providing human services, while adjusting to a new organization/role and potentially struggling with sleep, has significant implications for the new graduate, their employers, and the public. This study examines factors that impact new graduate sleep, with the aim of identifying perceived helps and hindrances to sleep-during-transition to inform occupational health nurses and other organizational leaders.
Methods
The current analysis stems from a larger longitudinal mixed methods study of NGN and NGT sleep experiences during the HEPP transition from 2019 to 2020 (Varner, 2021). Twenty-one females between 20 and 30 years old who graduated from different universities in the Midwestern U.S comprised the mixed methods sample, including 16 nurses and five teachers. All nurses worked in acute care hospital settings, while all teachers worked within public middle schools (sixth-eighth grade). Participants provided quantitative (e.g., Pittsburgh Sleep Quality Index [PSQI] survey) (Buysse et al., 1989) and qualitative (e.g., one-on-one semi-structured interview) data three times during the first year of practice (i.e., once during each transition stage). The team developed a typology of new graduate employee sleep-during-transition by merging the quantitative PSQI results, the most prevalent qualitative sleep experiences (e.g., good, varied, poor), and the theoretical HEPP transition stages. These types reflected the new graduates’ overall sleep experience during transition: Got Worse, Got Better, and Stayed Varied. Most of the participating new graduates were in the Got Worse or Stayed Varied sleep types. See the parent study for more details (Varner, 2021).
For this article, the team completed a summative content analysis of responses (Hsieh & Shannon, 2005) from the 21 participants to targeted open-ended questions during the third/final one-on-one phone interviews which occurred during April to June 2020. Theoretically, participants would be in transition recovery when their perspectives of the new reality are more accurate (Williams, 1999). Investigator 1 asked participants: “What or who made the single most positive impact on your sleep during this transition year and why?” and “What or who made the single most negative impact on your sleep during this year and why?” Investigator 1 conducted all interviews, which were audio recorded, transcribed verbatim, reviewed for accuracy, and analyzed using MAXQDA software for reliability. Furthermore, Investigators 1 and 2 coded data and identified categories in partnership. Transcripts were analyzed and compared based on the new graduate sleep typology (i.e., Got Better, Got Worse, Stayed Varied), which emerged from the parent study (Varner, 2021) for interpretive validity.
This parent study was approved and monitored by the University of Cincinnati’s Institutional Review Board.
Results
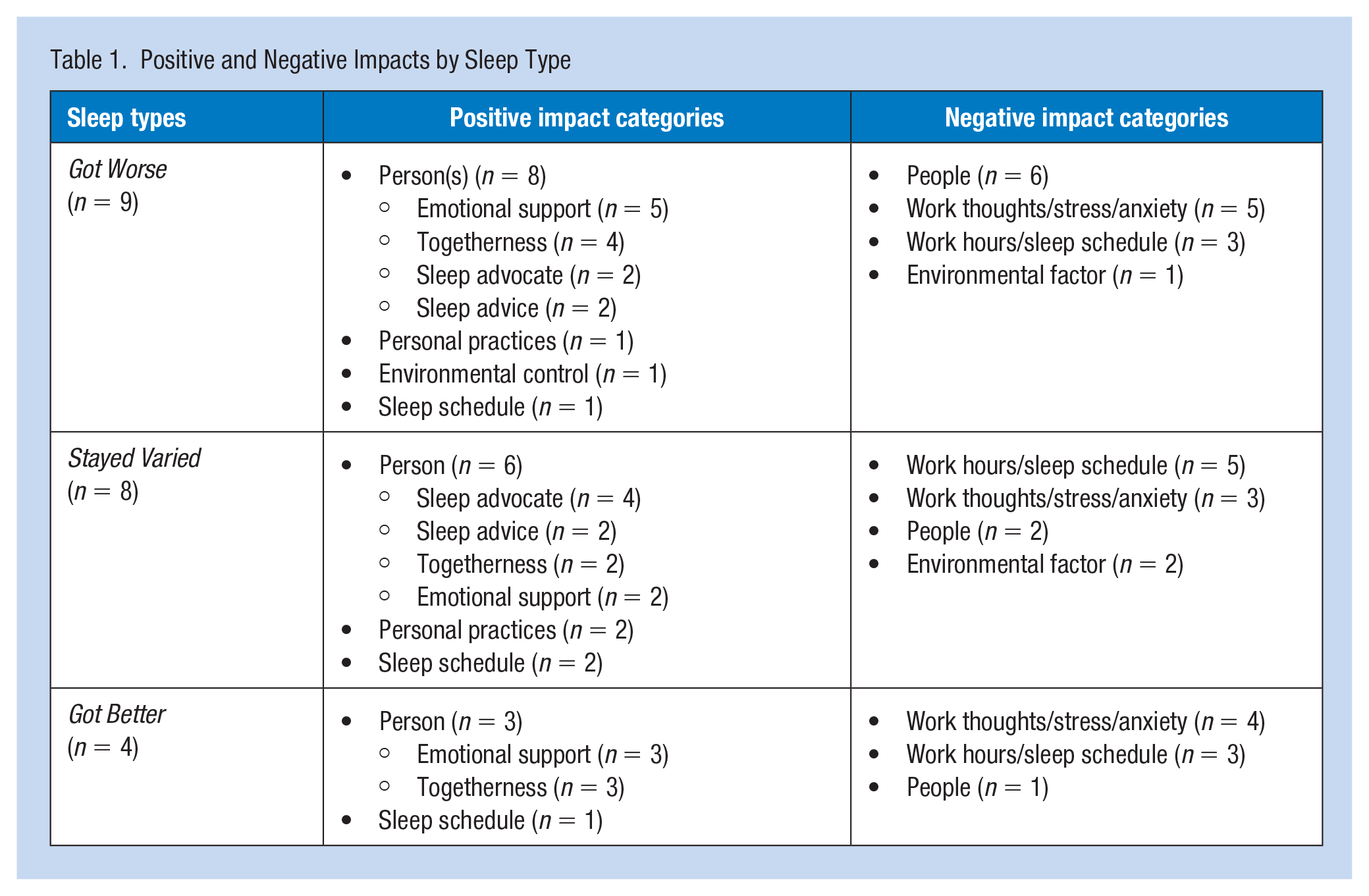
After nine or more months of professional practice, the 21 participants reflected on their sleep experiences over the past year. Regarding “what or who” made the single most significant positive and negative impacts upon their sleep-during-transition, some participants provided one distinct response, while others provided combination responses. Rationales provided were similar and insightful. Analyses of these responses identified positive and negative impacts upon sleep. Frequencies of categories by sleep type are given in Table 1. Supporting quotes were collected during a third interview between March and June 2020. Pseudonyms starting with N (e.g., Nia) refer to NGNs, while names starting with T (e.g., Tosha) represent NGTs.
Positive and Negative Impacts by Sleep Type
Positive Impact on Sleep
For positively impacting sleep-during-transition, a few nurses mentioned the categories of personal practices (e.g., prayer, mediation, consistent bedtime routine), environmental controls (e.g., blackout curtains), and sleep schedule (e.g., self-scheduling at work). However, almost every NGN and NGT (n = 17) mentioned a particular person or group of persons as making the single most positive impact on their sleep. These people were from both personal (e.g., parent, sibling, bed partner) and professional (e.g., co-workers) settings, and sometimes a combination (e.g., a parent, sibling, best friend, roommate who was also a nurse or teacher).
Participants described four characteristics of these individuals/group who positively impacted sleep and described some as having several of them. These people provided emotional support particularly through empathetic listening and a sense of togetherness. They also might be sources of sleep advice and/or sleep advocates.
Regarding emotional support, almost half of the participants mentioned family, friends, and/or co-workers as being the person one would call or talk to “vent,” “de-stress,” or “decompress.” Nevaeh talked about her best friend, who was also a night shift nurse. They kept the same work schedule and called each other on their way home from work “. . . we just vent . . . talk about our nights . . . it’s a good feeling to get all that (negative energy) out before I get home.” Regarding a friend, Nayeli shared “It’s always been fun hanging out (with her) and stuff . . . I just felt more relaxed.” Nalani described how she and a peer nurse acted as “resource for each other with breaking down our days and what we’ve been going through.” Nicole described her boyfriend as a “comfort when I’ve had hard days . . . he lets me verbally process everything and just get if off of my chest, and out of my head.”
Regarding togetherness, some participants mentioned individuals/groups who helped the new graduate to not feel “alone” or more “normal.” This togetherness involved a sense of comradery within the new role, as well as sleep. Nova mentioned “being together (with coworkers) when we’re super tired together, or when we have a lot of energy together. They have definitely carried me along on more tired days and more tired nights.” Nakita described having a roommate working night shift as well. “So, I’m like, ‘if I’m missing out on something, so is she.’ So, we’re in it together.” These individuals also helped normalize the transition experience. After talking with a friend, Nayeli shared, “I would fall asleep being like, ‘okay, things aren’t as crazy as it seems.’” Tosha described talking with a teaching peer who had transitioned recently. She said,
So helpful to know that, “yeah, those thoughts are normal,” and “all teachers think and feel that way” . . . It made me not feel alone . . . and that made me feel better about myself and made me less likely to postpone sleep (using phone at bedtime).
Two nurses mentioned preceptors as building confidence and supporting the transition experience.
Several participants described someone who was a sleep advocate. Whether family, friend, or co-workers, sleep advocates either affirmed the new graduates’ need for sleep, and/or helped them to prioritize it. Natalie reflected,
Sometimes I feel bad about sleeping during the day. I should have been awake for this . . . and mom’s like, “No, you need your sleep. Take care of your body and take care of your patients.” She’s really good at reminding me.
Sleep advocates would also help around the house, provide a quiet environment, and ensure adequate time for sleep. Noor shared her partner would “do dishes and just do all the little things that need to be done, but if I am doing them, it means I’m not sleeping.” Regarding her boyfriend, Nala observed “he has been so helpful, I think because he probably values my sleep even more than I do.” Taylor talked about how two people (e.g., a friend and a parent, both teachers) “drilled into me the fact that teaching does not need to be my entire life.” She mentioned it was very helpful “realizing that I can go to bed. I did what I could, and it might not have been perfect, but that’s okay. You can still rest well.”
Finally, a few nurses mentioned people who provided sleep advice, particularly with adjusting to night shift. These people shared sleep experiences and strategies that worked for them. Nakita talked about how a roommate who had switched to nights just 1-month prior who shared sleep advice stating, “that was just so helpful . . . with that transition and what to anticipate and what worked for her.” A couple others mentioned seeking information from co-workers. Nova mentioned “a lot of them have been doing it longer, so they know what to do and they know how to sleep better and things like that.”
Negative Impact on Sleep
Regarding negative impacts on sleep, the new graduate participants provided a range of categories, including environmental factors, work hours/sleep schedule, work thoughts, stress/anxiety, and people. Environmental factors usually involved noise (e.g., pets, roommates) and/or aspects of one’s living arrangement (e.g., light from windows, living downtown). The category of work hours (i.e., adjusting to nights, long hours), also involved adapting one’s sleep schedule to accommodate work/personal lives. Nevaeh observed,
. . . multiple times a week it was a mental battle of “okay, you have to sleep, even though they (friends) are doing this (activity)..” . . . I think that was a difficult pill to swallow, that I can’t be involved in everything.
Tera identified “not being on top of it (sleep schedule)” during the work week as a problem. Nia pointed out “sometimes I watch an extra episode (on TV) when I probably should be going to bed.” While many participants mentioned the category of work hours/sleep schedule as negatively impacting sleep, there were differences in frequency by sleep type (see Table 1). For example, Got Worse participants mentioned work hours/sleep schedule (e.g., adjusting to night shift) the least, while Stayed Varied type, who were all nurses, addressed it the most frequently.
Participants mentioned work thoughts and stress/anxiety in tandem and the most frequent, including seven nurses and all five teachers. People involved others who disrupted sleep like Noor’s children, or a parent calling Nevaeh during the day when she was sleeping. A couple participants mentioned people in their lives who were not mindful of their sleep needs like Nala sharing “My mom isn’t exactly very helpful in my sleeping habits. If I do go home or visit, she’s always like, ‘Oh, you can just drive down like the day of,’ and I’m like, ‘No, mom, I have to sleep.’”
More than half of participants provided a response that intertwined work thoughts, stress/anxiety, and people. Stress/anxiety was both a byproduct of thinking back on past work (e.g., rumination) and prompted one to think about future work more (e.g., worry). People associated with work might be the “source” of the stress/anxiety. For example, Nevaeh observed how one of her preceptors
put a lot of doubt in my mind . . . she was very, very, very tough on me to the point that I almost think it wasn’t helping and that’s part of the reason why I was so stressed (and not sleeping).
Tessa reflected “Students. . . . there always was a student of the day who I lost sleep over.” She went on to explain that some of the “sleep loss” involved reflecting on her performance as a teacher, in relation to student behaviors. “‘What am I doing as a teacher that is not meeting your needs?’ Typically, I didn’t lose sleep over their academics. Typically, it was over a social interaction.” Other work thoughts could involve both people the new graduate was thinking about, and what other people were thinking about the new graduate. Taylor observed, “what keeps me up . . . is just like this fear of what other people thought of me, and do they think I’m doing a good job, or are they thinking that I’m messing everything up?”
Discussion
Connecting to support persons/group, along with adequate management of stress, anxiety, and/or work thoughts, and good sleep hygiene are important strategies for supporting sleep-during-transition. Those with worsening sleep may need to seek medical intervention and/or a sleep specialist. Fatigue mitigating policies are also important considerations.
Connecting to Support Person(s)/Group
One primary strategy for improving sleep-during-transition relevant to all three sleep types was having support person(s)/group. This finding aligned with the Support aspect of the 4S system used by Anderson et al. (2012) in counseling adults in transition. A person’s Situation (i.e., timing and circumstances of transition), Self (i.e., beliefs regarding sleep), Support (i.e., family, friends, co-workers, organizational), and Strategies (i.e., past and present ways of coping) are either assets or liabilities to the current transition experience.
However, support systems are often disrupted during transition, and part of the process involves developing new ones (Anderson et al., 2012; Meleis, 2010; Williams, 1999). Transition programs like nurse residency programs and teacher induction programs aim to increase support using strategies like mentors/preceptors and debriefings to moderate the experience (Meleis, 2010). Shernoff et al. (2016) explored the use of school psychologists in providing support for NGT as they adjust to the new role. Social workers and chaplains within healthcare systems may facilitate debriefing sessions and provide one-on-one support. Despite the presence of formal transition support in this study, though, most new graduates experienced varied or worsening sleep (see Varner, 2021).
Managing Stress, Anxiety, and/or Work Thoughts
Stress, anxiety, and/or work thoughts negatively impacted the sleep of new graduates in varying degrees for all three sleep types. This finding aligned with Epstein et al.’s (2019) study where NGNs described “cognitive arousal” causing sleep problems, including ruminative thinking and anticipatory stress. Cropley et al. (2006) noted rumination in schoolteachers as disturbing sleep. Maladaptive cognitions (e.g., worry, rumination) are known contributing factors for insomnia in young adults (Zamani et al., 2022).
New graduates, regardless of hours worked or shift, might benefit from existing strategies designed to help manage work thoughts. Stress management and decreased worrying can decrease psychophysiological arousal found with heightened psychosocial stress (Irish et al., 2015). Relaxation and mindfulness (e.g., stress reduction) can promote sleep, though individual characteristics and circumstances may influence their effectiveness (Irish et al., 2015). The Stress Management and Resiliency Training (SMART) program (Park et al., 2013) has four main components for building resilience, including mind–body skills (e.g., medication, relaxation), traditional stress management techniques, adaptive coping skills (based on cognitive behavioral and other therapy approaches), and healthy lifestyle behaviors of which sleep is addressed, along with exercise, nutrition, and social support. Training involves didactic content, experiential exercises, and small group/debriefing sessions by a trained clinician. Dossett et al. (2021) completed a quality improvement cohort study utilizing the SMART program and observed a significant reduction in perceived stress (p < .001) and enhanced global mental health (p = .001) among healthcare providers. Sampson et al. (2020) found a significant decrease in stress and anxiety among new nurses with a similar program MINDBODYSTRONG at 6 months. However, impact on sleep was not detailed in either Dossett et al. (2021) or Sampson et al. (2020).
Encouraging Good Sleep Hygiene
Some participants mentioned personal practices, environmental controls, and consistent sleep schedules as positively impacting sleep-during-transition. These identified positive impacts align with good sleep hygiene, which includes the general lifestyle/behavioral (e.g., diet, exercise, caffeine/alcohol use) and environmental (e.g., light, noise, room temperature) elements that promote sleep (Edinger et al., 2021; Irish et al., 2015). While some nurses in this study might have had good sleep hygiene, Epstein et al. (2019) found that new Swedish nurses lacked effective sleep management strategies.
Originally established in the treatment of mild to moderate insomnia, sleep hygiene recommendations generally do not require a sleep specialist or clinician. Sleep hygiene practices include exercise, stress management, noise reduction, sleep timing, daytime napping, and limiting substance use (e.g., nicotine, caffeine, alcohol). It may also involve some information regarding “normal sleep” and changes in sleep patterns based on age (Edinger et al., 2021; Irish et al., 2015). Sleep timing (e.g., consistent sleep/wake times) and napping are relevant sleep hygiene topics for both nurses and teachers. Furthermore, the American Thoracic Society recommended educating workers regarding the impact of work hours upon sleep duration and quality, as well as associations with workplace injury and sleepiness (Mukherjee et al., 2015).
Mukherjee et al. (2015) also proposed that healthcare providers should receive “a greater level of education on sleep hygiene” (p. 1451), which would hopefully translate into education of patients and enhanced public education programs. This observation could also be said for teachers, as they educate pupils. Occupational health nurses could partner with human resources and/or professional development departments to provide sleep education to new professionals, however, it is not recommended as a single component intervention for chronic insomnia.
Referring to a Sleep Specialist
New graduates might describe acute insomnia, which usually involves problems falling asleep (i.e., sleep-onset), staying asleep (i.e., sleep maintenance), or a combination (Schwab, 2020). They may not feel rested upon waking and may experience excessive daytime sleepiness. Adjustment insomnia typically improves when stress and/or the anxiety wanes (Schwab, 2020). However, after 3 months of frequent symptoms (e.g., at least three times per week), a new graduate may need medical intervention and/or a sleep specialist for chronic insomnia disorder (Zamani et al., 2022).
The American Academy of Sleep Medicine practice guidelines for chronic insomnia include a multicomponent approach like cognitive behavioral therapy for insomnia (CBT-I) (Edinger et al., 2021) by trained sleep professionals. CBT-I involves a combination of one or more cognitive therapy strategies (e.g., sleep regulation education), along with stimulus control instruction (e.g., bed when sleepy, out of bed if unable to sleep, consistent wake-time, no napping), and/or sleep restriction (e.g., limiting time in bed to sleep duration). It may also include sleep hygiene education and relaxation techniques. This approach may decrease the need for pharmacological therapy (Edinger et al., 2021). New graduates with poor and/or worsening sleep should be encouraged to seek support from a sleep specialist.
Developing Fatigue Risk Mitigating Policies
Numerous nurses in the larger parent study talked about not having a break and/or even being able to eat during their 12-hour shifts. Some new graduates talked about being cautious to not sit down at work for fear of falling asleep. Most teachers in this study described long hours (e.g., working all day, taking work home in evenings and weekends). Normalizing workplace naps and nap policy (e.g., providing nap room) have long been discussed (Baxter & Kroll-Smith, 2005; Lerman et al., 2012), however, fatigue risk management implementation remains varied in the United States (Caldwell et al., 2019). Occupational health nurses should advocate for the establishment and/or enforcement of fatigue risk mitigating policies like ensuring breaks and encouraging naps, which may be particularly relevant for all new graduate employees (Honn et al., 2019; Lerman et al., 2012).
Future Research
While there is a growing body of literature related to sleep and transition, more work remains. Further interdisciplinary research should explore new graduate employee sleep-related beliefs (e.g., sleep self-efficacy, dysfunctional beliefs, and attitudes about sleep) as they transition (Eidelman et al., 2016). For example, the Charlotte Attitudes Toward Sleep (CATS) scale was validated among the U.S. college students (Peach & Gaultney, 2017) and could be tested among new graduates. Intervention studies involving sleep outcomes could include comparing debriefing approaches (Van Patten & Bartone, 2019), CBT programs (Crain et al., 2017; Edinger et al., 2021; Sampson et al., 2019), and electronic sleep supports (Ebert et al., 2015; Thiart et al., 2015) within the context of transition programs.
Some limitations for this analysis warrant discussion. First, NGTs had limited representation. Also, it is possible new graduates interested in sleep and/or research were more likely to participate in this study. However, results from this study align with findings from other qualitative studies on sleep in NGNs noted above. Findings between nurses and teachers in this study were congruent, though with some differences among night shift working nurses. Effect(s) of the global pandemic and Black Lives Matter demonstrations that occurred during the third wave upon participant sleep are uncertain. Although the final interview included targeted questions regarding the pandemic and their transition, majority of participants pointed to other factors impacting their sleep.
Table 2 is a summary table that was developed for new graduates, occupational health nurses, and organizational leaders. The team combined participant insights into the summary table regarding positive and negative impacts on sleep with pertinent literature to develop recommendations for supporting sleep-during-transition.
Supporting New Graduate Nurse and Teacher Sleep-During-Transition Recommendations
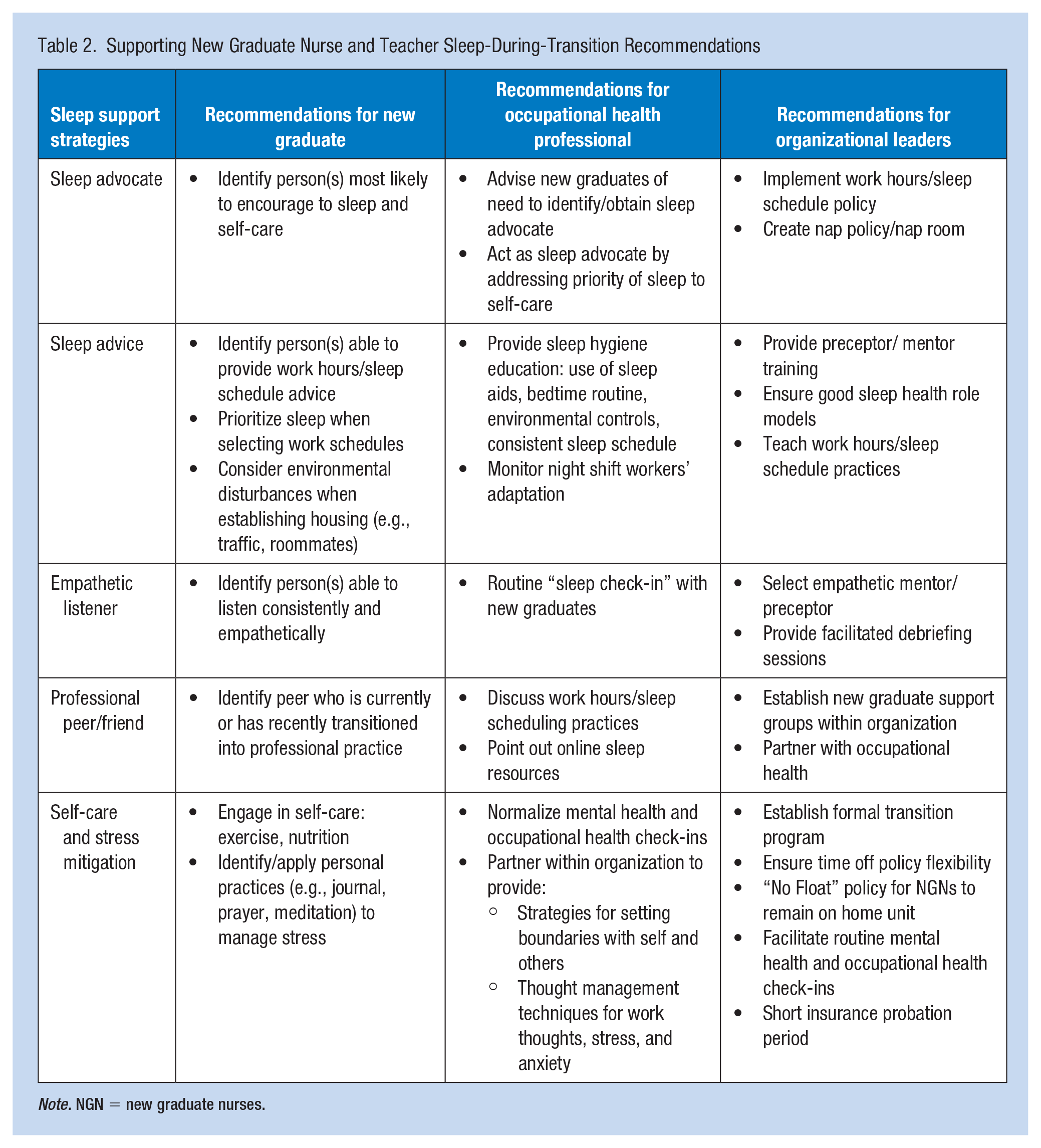
Note. NGN = new graduate nurses.
Some limitations for this analysis warrant discussion. First, NGTs had limited representation. Also, it is possible new graduates interested in sleep and/or research were more likely to participate in this study. However, results from this study align with findings from other qualitative studies on sleep in NGNs noted above. Findings between nurses and teachers in this study were congruent, though with some differences among night shift working nurses. Effect(s) of the global pandemic and Black Lives Matter demonstrations that occurred during the third wave upon participant sleep are uncertain. Although the final interview included targeted questions regarding the pandemic and their transition, majority of participants pointed to other factors impacting their sleep.
Implications for Occupational Health Practice
Organizational leaders should support new graduate sleep, the place where work and home intersect (Varner, 2021). Occupational health nurses are uniquely positioned to impact 4Ss of transition (Anderson et al., 2012) related to sleep. They can assess the new graduates’ Situation, as well as influence Self and Strategies by being empathetic listeners helping new graduates explore sleep-related beliefs, practices, and barriers, while advocating sleep (e.g., Support).
Information seeking is an essential precursor to new employee adjustment (Saks & Gruman, 2018), but the degree to which the new employee seeks information may be partly determined by the perceived “cost” or social impact of seeking it (Teboul, 1995), particularly if they are of an ethnic/racial minority (Teboul, 1999). Furthermore, new graduate employees may have limited information seeking for poor sleep due to factors like having to find new healthcare providers after geographic relocation or probationary insurance periods. Other concerns potentially hindering information seeking to manage stress, anxiety, and/or troubling work thoughts may include fear of being perceived as “incompetent” or mental health stigmas (Anderson et al, 2012; Williams, 1999).
Proactive interaction with occupational health nurses may facilitate early identification of new graduates with varied or worsening sleep. They also should encourage new graduates to identify a family member, friend, and/or co-worker who can listen empathetically, understand the profession, is able to provide sleep advice, and/or advocate for sleep during the first year of practice. Human support is essential to healthy new graduate transition (Gong et al., 2021), and may be particularly relevant to sleep-during-transition.
Conclusion
The NGN and NGT role transition experience may last for approximately 1 year and involve three stages: transition shock, transition crisis, and transition recovery. Based on findings from the larger longitudinal mixed methods study of NGNs and NGTs, many new graduates had varied or worsening sleep experiences (Varner, 2021). Reflecting on their sleep experiences of the past year, these new graduates indicated a support person(s) and/or group made the single most significant positive impact upon their sleep. Stress, anxiety, work thoughts, and people negatively impacted new graduate sleep-during-transition during the first year. Occupational health nurses could help support new graduate sleep-during-transition with the provided recommendations.
Applying Research to Occupational Health Practice
In this study, the authors present findings from a targeted content analysis of transcripts from a larger longitudinal mixed methods study exploring the sleep of new graduate nurses and teachers during their initial year. During the final interview, 21 female participants addressed the most positive and negative impact(s) on sleep. They identified a person/group as most positively impacting sleep, while negative factors included work thoughts, stress/anxiety, and people. Work thoughts and stress/anxiety were mentioned together and most frequently by participants.
Support persons and/or groups may be essential to the sleep of new nurses and teachers. Thought management/stress mitigation strategies and sleep hygiene may also improve the sleep experiences of these new professionals. Occupational health nurses can support sleep-during-transition among new nurses and teachers by acting as sleep advocates on individual and organizational levels. Proactive interaction may lead to early identification of new graduates with poor sleep and intervention for worsening sleep.
Footnotes
Acknowledgements
The authors extend their special thanks to Dr. Sinem Toraman for assistance with data analysis for this manuscript.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Kendra VARNER was supported by the National Institute for Occupational Safety and Health (NIOSH) through the University of Cincinnati Education and Research Center (5T42OH008432-12) and the Jonas Foundation Nurse Leader Scholarship. These organizations were not involved in the conduct of this research project.
Ethics Approval
This study was approved through the University of Cincinnati’s Institutional Review Board.