
Abstract
Sleep problems may have negative effects on work–life balance, overall health, and safety. We aimed to investigate the association between sleep disorders and absenteeism and delay to work (being late or tardy) among the working adult population. The study was conducted by using data from a large survey of working adults who participated in the Turkish Adult Population Epidemiology of Sleep Study (TAPES) managed by Turkish Sleep Medicine Society (TSMS). Secondary analyses was employed to examine absenteeism and delay to work and their associations with sleep problems, including sleepiness by Epworth Sleepiness Scale (ESS), parasomnias, sleep apnea (by Berlin Questionnaire), sleep quality (by Pittsburgh Sleep Quality Index), and restless leg. History of any absenteeism and delay to work was observed in 276 (18%) and 443 (29%) out of 1,533 working adults, respectively. In the multivariate analyses, absenteeism was associated with younger age, female gender and poor sleep quality, while delay to work was associated with younger age, poor sleep quality, parasomnia, and sleepiness. In the presence of absenteeism and delay to work, sleep disorders including sleepiness, poor sleep quality, and parasomnia should be considered. Such evaluation may improve worker well-being and provide some additional benefits in terms of increasing productivity and lowering work-related costs.
Introduction
Sleep is considered vital for preserving daytime cognitive function and physical, mental, and social well-being. Sleep insufficiency may be harmful to workers’ wellness and may have negative effects on work–life balance, as well as overall health and safety at work. Consequently, the burden might be significant at both the individual and societal levels (Skaer & Sclar, 2010).
Insufficient sleep can result from many sleep-related problems. The International Classification of Sleep Disorders (ICSD) schema lists criteria to distinguish between more than 80 different sleep-related problems including chronic sleep deprivation, which is the condition of not having enough sleep (Léger, Guilleminault, Bader, Lévy, & Paillard, 2002; Sateia, 2014). Because sleep deprivation alters cognitive and motor functions, it can be associated with negative work-related outcomes including absenteeism, reduced productivity, and occupational accidents (Daley et al., 2009; Godet-Cayré et al., 2006; Kleinman, Brook, Doan, Melkonian, & Baran, 2009; Léger et al., 2002; Sivertsen et al., 2009; Swanson et al., 2011). Decreased sleeping hours has been shown to have a positive relationship with productivity loss (Gingerich, Seaverson, & Anderson, 2017) or vice versa (Chen, Schultz, Li, & Burton, 2018). There is accumulating evidence implicating sleep disorders as important contributors to work-related outcomes (Allen, Bansback, & Ayas, 2015; Jurado-Gámez, Guglielmi, Gude, & Buela-Casal, 2015; Rajaratnam, Licamele, & Birznieks, 2015; Reynolds et al., 2017). An increased awareness is needed regarding that these issues are very often due to unrecognized sleep disorders that are mostly manageable and that their adverse outcomes can be prevented.
In this study, the investigators aimed to examine the association between sleep disorders and absenteeism, as well as delay to work among the working adult population, using the data from the Turkish Adult Population Epidemiology of Sleep Study (TAPES) conducted by the Turkish Sleep Medicine Society (TSMS; Ardic et al., 2013).
Materials and Method
Study Population
This study consisted of a sample of individuals who participated in the large population-based study (TAPES), which investigate the prevalence of sleep problems in Turkey (Ardic et al., 2013). TAPES sample size was calculated and selected by TurkStat (Turkish Statistical Institute), which was conducted to represent the adult population demographics of Turkey. In TAPES, the sample included 56 of Turkey’s 81 provinces. Block and household address selection for sampling was carried out through simple random sampling. In the final stage of sampling, subjects in the sampled households were selected by using a table of random numbers after listing the individuals who were 18 years of age or older within the house.
Data Collection
A questionnaire consisting of 132 questions was used. The SAM Research Institution performed the implementation and supervision of the interviews against remuneration as per a contract signed on the behalf of the Society. The questions were determined by the TSMS Executive Board and consisted of data on demographics, occupational history, educational and socioeconomic status, health problems, sleeping habits, affective and psychotic symptoms, sleep complaints, and sleep disorders. Data were collected by questionnaire via face-to-face interview. The draft questionnaire was revised after a pilot study was conducted in four centers in Istanbul, Ankara, Izmir, and Kayseri that are accredited according to European Sleep Research Society criteria and eligible to provide education for Sleep and Disorders. Survey scales were tested for reliability and content validity (Chronbach’s α > 0.70).
In this secondary analysis, the data were analyzed to examine absenteeism and delay to work and their associations with sleep problems, which were determined by the questionnaire among the working individuals.
Instrument-Variables Selection
In this current study, we obtained the data from the TAPES questions regarding demographics, occupational history, educational status, socioeconomic status, health problems, sleeping habits, depressive symptoms, sleep complaints, and sleep disorders. We compared sleep disorders positive screening results between the ones who had a history of absenteeism and delay to work, which they were defined as one or more day absence from work and being late for work, respectively, without any obvious reasonable explanation, with participants who had no absenteeism and no delay to work.
Parasomnias are defined as undesirable physical events or sensory experiences that occur with every intro, during or arousing from sleep (Vaughn, 2017). Parasomnias were determined by inquiring about the presence of sleepwalking, sleep terror, sleep talking, REM (rapid eye movement) behavior disorder, sleep paralysis, and sleep-related eating disorder (Ardic et al., 2013). Parasomnia was defined in the analysis as ever-never having one or more of these conditions. Insomnia was defined as difficulty initiating sleep, difficulty maintaining sleep, or fragmented sleep at least three times a week for a month or more, or early morning awakening at least once a week in the prior month (Diagnostic and Statistical Manual of Mental Disorders; 4th ed.).
The Epworth Sleepiness Scale (ESS) was used to assess excessive daytime sleepiness. ESS has been previously validated in Turkish (Izci et al., 2008). Sleepiness is defined as a score above 10 on the ESS. Questions on restless legs syndrome (RLS) were adapted from the criteria proposed by the International Restless Legs Syndrome Study Group and previously used in an epidemiological investigation of RLS in Turkey (Sevim et al., 2003).
The Berlin Questionnaire was used to define obstructive sleep apnea (Netzer, Stoohs, Netzer, Clark, & Strohl, 1999). A positive score in at least two of the three categories, which included questions on snoring, witnessed apneas, daytime sleepiness, hypertension, and measurement of body mass index, was defined as high risk (Netzer et al., 1999). Quality of sleep was assessed by the Pittsburgh Sleep Quality Index (Buysse, Reynolds, Monk, Berman, & Kupfer, 1989).
Ethics Statement
Ethical approval was obtained from the Scientific Research Assessment Commission of Hacettepe University. Informed consent was signed by all the participants before the interview. In the consent form, it was stated that personal information would not be used in the reporting of the results and participants seeking medical help would be consulted by TSMS. A separate letter signed by the TSMS chair and principal investigator was provided, which briefly explained the potential benefits of the study.
Statistical Analysis
Descriptive statistics for numerical variables were expressed as means ± standard deviations (SD) and categorical variables were presented as frequencies (%). Two by two comparisons of distributions were tested by chi-square test or the Fisher’s exact tests. The independent-sample t test was used to compare the differences of means between groups. According to the results of the univariate analyses, multivariate logistic regression models were created. SPSS software, 15.01 (Customer no: 114,094; Chicago, Illinois, 2001), was used for the statistical analyses. An alpha level of 0.05 was chosen for statistical significance.
Results
Among the sampled 5,520 people, the response rate for the questions on working status, either positive or negative, was 90.9% (n = 5,021). Participants who were working and whose data were available for absenteeism and delay to work were included in the analyses (Figure 1).
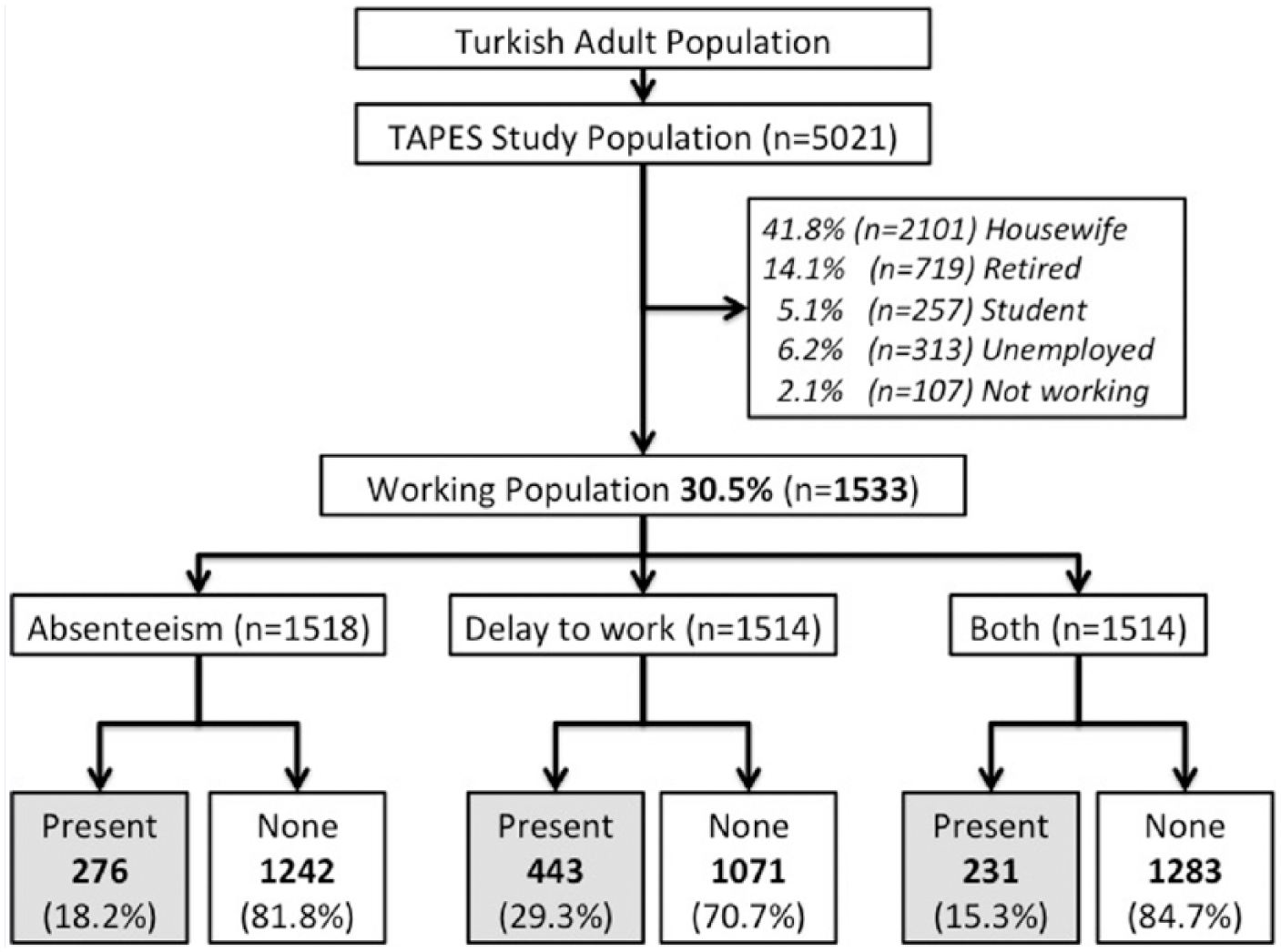
Flow diagram for participants included in the study.
The demographic parameters, working conditions, and determined sleep problems of the working individuals who participated in the survey are presented in Table 1. A total of 1,533 working individuals, 1,279 males (83.4%) and 254 (16.6%) females with an average age 36.2 ± 10.6 (range 18-78), were evaluated in the study. Most (79.6%) were living in an urban area, 90.0% worked a regular day shift, 43.7% walked to work, 21.6% had more than 30 minutes of commuting time, and 30.9% had an unpaid job or were self-employed. The common sleep problems determined among the working individuals, in decreasing order, were parasomnia (19.2%), poor sleep quality according to the Pittsburgh Sleep Quality Index (17.0 %), high risk of sleep-disordered breathing according to the Berlin Questionnaire (9.1%), insomnia according to the DSM-IV definition (6.1%), sleepiness according to the ESS (5.2%), and restless leg syndrome (2.7%).
The Demographic Characteristics, Working Conditions and Determined Sleep Problems of the Working Population a
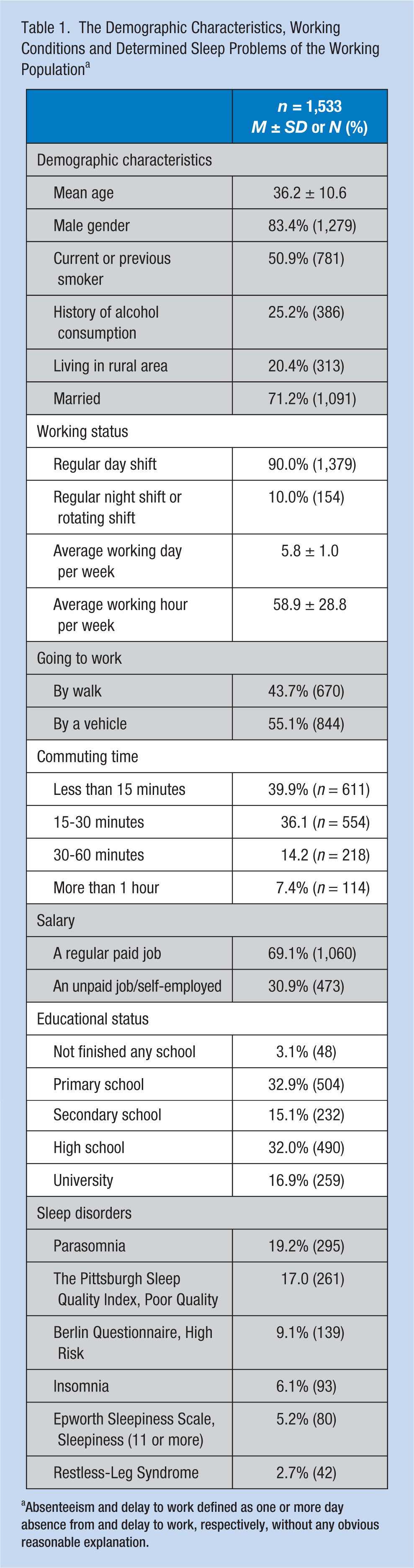
Absenteeism and delay to work defined as one or more day absence from and delay to work, respectively, without any obvious reasonable explanation.
History of absenteeism, delay to work, and both absenteeism and delay to work, for at least one day, among the working individuals were 276 (18.2%), 443 (29.3%), and 231 (15.3%), respectively (Table 2). In the univariate analyses, absenteeism and delay to work was more common among females relative to males but did not reach statistical significance (22.0% vs. 17.9% and 30.4% versus 28.6%, respectively). Absenteeism was significantly more common among younger relative to older workers (34.7 ± 10.2 versus 36.5 ± 10.2, p = .012), and those who reported sleepiness (26.9% vs. 17.7%, p = .040), poor sleep quality (39.8% vs. 16.0%, p = .000), and parasomnia (24.6% vs. 16.7%, p = .002). Similarly, delay to work was significantly more common among younger workers relative to older workers, (34.3 ± 9.9 vs. 36.9 ± 10.7, p = .000), those who reported sleepiness (46.2% vs. 28.3%, p = .001), poor sleep quality (42.6% vs. 26.6%, p = .000), insomnia (43.8% vs. 28.4%, p = .003), and parasomnia (43.3% vs. 25.9%, p = .000).
Comparison of the Workers Who Did and Did Not Have Absenteeism, Delay to Work, or Both in the Prior Year
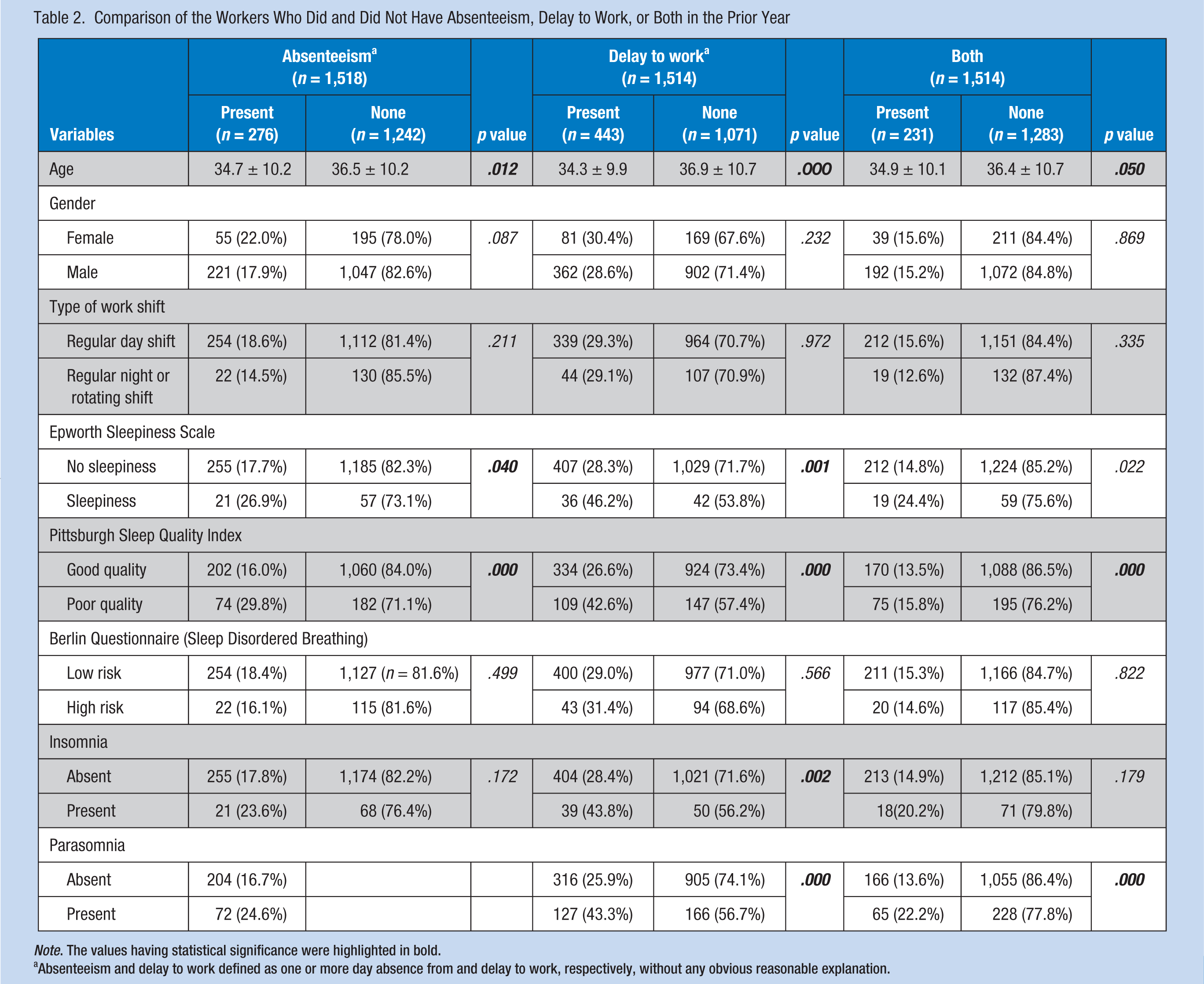
Note. The values having statistical significance were highlighted in bold.
Absenteeism and delay to work defined as one or more day absence from and delay to work, respectively, without any obvious reasonable explanation.
In the evaluation of the combined group, having a history of both absenteeism and delay to work was significantly associated with poor sleep quality and parasomnia (Table 2). Delay to work was significantly more common among workers who had a commuting time between 15 and 30 minutes, compared to the other subgroups.
In multivariate analyses, female gender, (odds ratio [OR] = 1.36, 95% confidence interval [CI] 1.02-1.80), age younger than 35 years (OR = 1.73, 95% CI 1.35-2.22), and having poor sleep quality (OR = 2.05, 95% CI 1.54-2.73) were significantly associated with absenteeism. Age younger than 35 years (OR = 1.80, 95% CI 1.46-2.24), poor sleep quality (OR = 1.74, 95% CI 1.32-2.28), sleepiness (OR = 1.71, 95% CI 1.09-2.70), and parasomnia (OR = 1.83, 95% CI 1.42-2.36) were significantly associated with delay to work (Table 3).
Result of Multivariate Analysis of the Associated Risk Factors for Absenteeism and Delay to Work
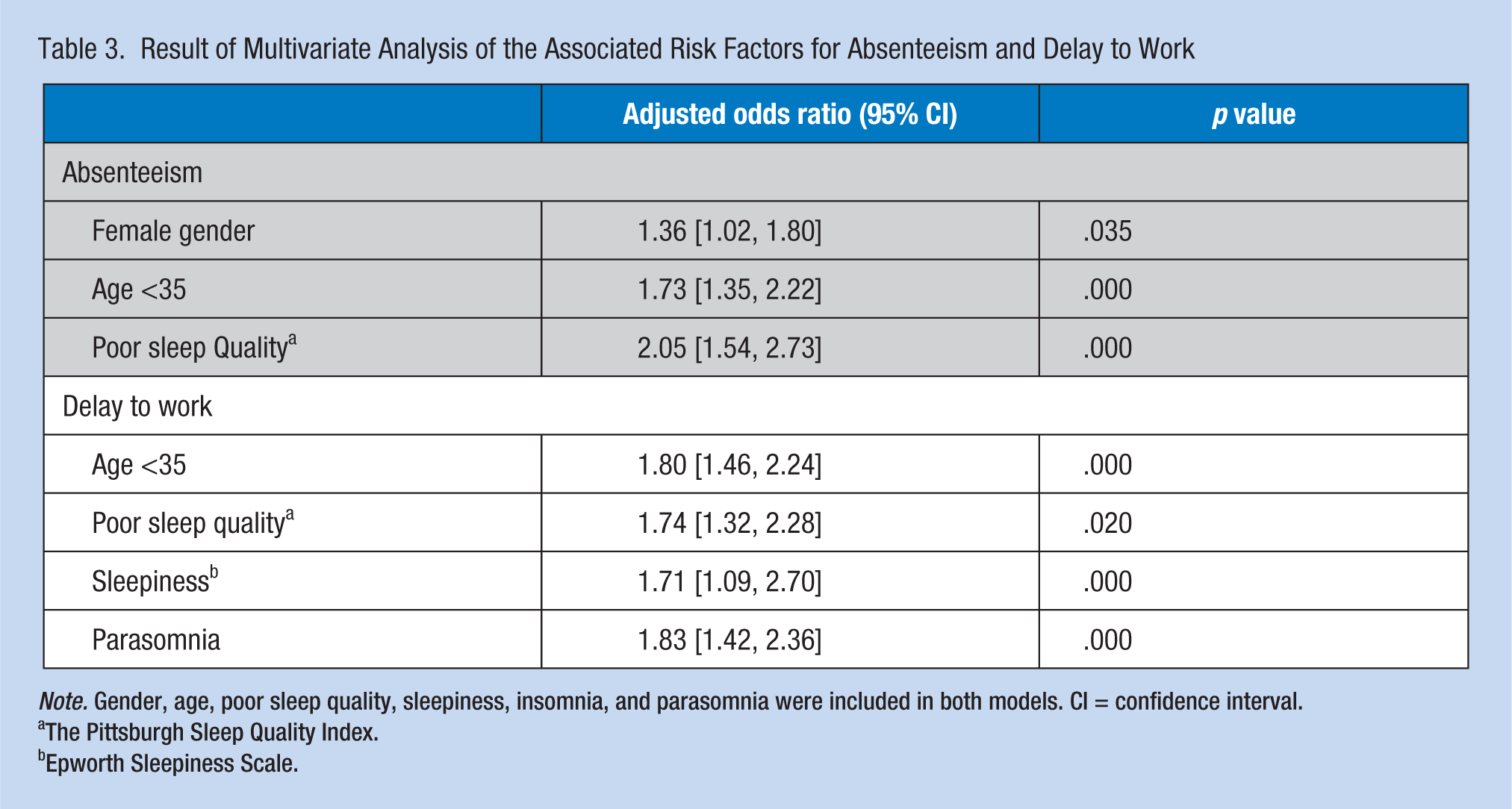
Note. Gender, age, poor sleep quality, sleepiness, insomnia, and parasomnia were included in both models. CI = confidence interval.
The Pittsburgh Sleep Quality Index.
Epworth Sleepiness Scale.
Discussion
This study indicated that a history of absenteeism and delay to work among the working individuals was 18.2% and 29.3%, respectively, and some sleep disorders might be associated with these conditions. Parasomnia and poor sleep quality were the most common sleep disorders. While absenteeism was significantly higher among the workers with younger ages, sleepiness, poor sleep quality, and parasomnia, delay to work was significantly higher among the workers with younger age, sleepiness, poor sleep quality, insomnia, and parasomnia. Absenteeism was associated with younger age, female gender, and poor sleep quality, and delay to work was associated with younger age, poor sleep quality, parasomnia, and sleepiness.
Sleepiness constituted an important part of absenteeism and delay to work in our study. Sleepiness implies a propensity to doze off or fall asleep unintentionally during the day, especially in passive situations (Freitas et al., 2017). The sleepiness rate was 5.2% in our study and was an independent risk factor for the subjects who reported delay to work. The prevalence of sleepiness varies from 4% to 31% in different studies. Insufficient sleep and sleep disorders cause sleepiness. An association between sleepiness and the risk of sustaining an occupational injury in nonshift daytime workers has been reported (Liu et al., 2000; Melamed & Oksenberg, 2002). Hypersomnia patients reported higher health care use and medication use, and social transfer income and thus represent a significant socioeconomical burden (Saini & Rye, 2017).
Insomnia was also significantly associated with delay to work in our study. In addition to its nocturnal effects, insomnia has a significant negative impact on an individual’s daily functioning including impaired work performance, lower physical and social functioning, an overall lower quality of life, and an increased risk for subsequent development of the psychiatric disease. The economic cost of insomnia related to loss of productivity, work-related accidents, absenteeism, and health care costs is enormous (Drake, Roehrs, & Roth, 2003). For this reason, awareness of sleep disorders in work life and investigations to determine the interaction between sleep and work may lower the costs, in terms of health promotion, directly or indirectly.
Poor sleep quality was significantly associated with absenteeism and delay to work, in both univariate and multivariate analyses, in our study. Poorer sleep has been shown to be associated with lower self-assessed working capacity and insomnia was found as a significant driver of absenteeism in other cross-sectional (Bolge, Doan, Kannan, & Baran, 2009; Daley et al., 2009; Kleinman et al., 2009; Léger et al., 2002; Leigh, 1991; Liu et al., 2000; Melamed & Oksenberg, 2002; Mulgrew et al., 2007; Philip et al., 2006) and cohort (Godet-Cayré et al., 2006; Sivertsen et al., 2009) studies. Leigh found that insomniacs had a 1.4 times higher average monthly sickness absence rate compared to those who did not report sleep trouble (Léger et al., 2002). Our finding was not consistent with a cross-sectional study that concluded that insomnia complaints may not be predictive of absenteeism (Daley et al., 2009). The differences may be due to the different types of questions inquiring about absenteeism. However, in a study using the work productivity and activity questionnaire (WPAQ) questioning only the last 7 days, insomniacs had greater work time missed than those in the noninsomnia group (Leigh, 1991). Similarly, the Pittsburgh Sleep Quality Index has been used to define good sleep and its association with absenteeism (Avidan & Kaplish, 2010; Godet-Cayré et al., 2006; Kleinman et al., 2009).
Parasomnias were the most common sleep problem in our study. Although parasomnia was significantly more common in absenteeism and delay to work, there was only an association between parasomnia and delay to work in the multivariate analysis. Parasomnias are a group of disorders exclusive to sleep and wake-to-sleep transition that encompass arousals with abnormal motor, behavioral, or sensory experiences (Buysse et al., 1989). These events occur during entry into sleep from wakefulness or during arousals from sleep and are augmented by the sleep state. Parasomnias can affect the patient’s quality of life and that of their partner. There is no specific study, according to our best knowledge, that has analyzed the relationship between parasomnias and absenteeism or delay to work.
There was no association between absenteeism and delay to work and high risk of sleep-related breathing disorder in our study. Mulgrew et al. (2007) followed sleep apnea patients prospectively, and found a relationship between work limitation and ESS, but not with sleep apnea. However, some of the studies reported sleep apnea as a predictor for work disability, which caused an increased risk of lost workdays prior to the diagnosis of sleep apnea (Jurado-Gámez et al., 2015; Sjösten et al., 2009).
In our study, only 2.7% of the working individuals had the symptoms of RLS and we could not find any statistically significant association between RLS and absenteeism and delay to work. Similar to our findings, RLS symptoms were not reported more frequently in those who had occupational accidents or absenteeism in a study conducted by the National Sleep Foundation (Swanson et al., 2011).
Commuting time has been found to be linearly related to sleep duration on delay to work (Petrov et al., 2018). Compared with short commutes, individuals with moderate commutes were found to have greater sleep duration variability in the same study. In our study, we found that moderate commute time, between 15 and 30 minutes, was associated with delay to work. For this reason, absenteeism and delay to work might be affected by several factors, and each case needs to be evaluated carefully from different perspectives, including cultural, age, and gender. The lower rate of female workers and male dominance in the Turkish working sector may also reflect the cultural difference of labor. The high rates of absenteeism and delay to work among younger and female workers may also have a cultural and socioeconomical influence that needs to be elucidated with further studies.
One of the limitations of our study was the lack of polysomnographic examination, which is often considered the standard method for diagnosing sleep-related breathing disorders, determining the severity of the disease, and evaluating various other sleep disorders. The self-reported nature of our data collection may have introduced information bias. Because of the cross-sectional design of the study, it is difficult to make causal inferences from our findings. The strengths of our study include the ability of the survey to represent the whole nation and to include all sleep disorders by using validated questionnaire and definitions.
In conclusion, our study suggests that absenteeism and delay to work were associated with some sleep disorders. Thus, in the individuals who had a history of absenteeism and delay to work, sleep disorders should be considered as a potential cause and they should consult a sleep medicine physician if this persists.
Implications for Occupational Health Nursing Practice
The study findings indicate that some sleep disorders including sleepiness, poor sleep quality, and parasomnia might be associated with absenteeism, delay to work, or both. Occupational health nurses should be aware that unrecognized sleep disorders can be the cause of absenteeism or delay to work and can affect overall health and safety at the workplace. These conditions are mostly manageable and their adverse outcomes can be prevented. In workers presenting problems with absenteeism or delay to work, an assessment of possible sleep problems is suggested. Among workers identified with a potential problem, a consultation with a sleep medicine specialist is recommended.
Applying Research to Practice
Absenteeism and delay (being late) to work may be associated with some sleep disorders. In the presence of absenteeism and delay to work, sleep disorders including sleepiness, poor sleep quality, and parasomnia should be considered as a potential cause and the worker should be referred to a sleep medicine specialist. Such evaluation may improve well-being and also provide some additional benefits in terms of increasing productivity and lowering work-related health care costs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Hikmet Firat is an associate professor in the department of pulmononology, Ankara Diskapi Yildirim Beyazit Education & Research Hospital, Ministry of Health. His main research area is sleep medicine.
Melike Yuceege is an associate professor in the department of pulmononology, Ankara Diskapi Yildirim Beyazit Education & Research Hospital, Ministry of Health. Her main research area is sleep medicine.
Sibel Kiran is an associate professor in the department of Institute of Public Health Hacettepe University, Ankara, Turkey. Her main research area is occupational epidemiology, occupational health, and work and sleep medicine.
Metin Akgun is a professor in the Department of Pulmonary Diseases, School of Medicine, Ataturk University, Erzurum, Turkey, and Scientific Committee Chair of Turkish Thoracic Society. His main research areas are COPD, silicosis, and sleep medicine.
Ahmet Ugur Demir is a professor in the department of Pulmonary Diseases, School of Medicine at Hacettepe University, Ankara, Turkey. His main research areas are epidemiology and sleep medicine.
Murat Aksu is a professor in the department of Neurology, School of Medicine at Acibadem University, İstanbul, Turkey. His main research areas are sleep medicine and epilepsy.
Sadik Ardic is a professor in the department of Pulmonary Diseases, School of Medicine at Kafkas University, Kars, Turkey. His main research areas are COPD and sleep medicine.
Derya Karadeniz is a professor in the department of Neurology, School of Medicine at Cerrahpasa University, İstanbul, Turkey. Her main research areas are sleep medicine and neurologic movement disorders.
Zeynep Zeren Ucar is an asssociate professor in the department of pulmononology, Suat Seren Education & Research Hospital, Ministry of Health, İzmir, Turkey. Her main research area is sleep medicine.
Serhan Sevim is professor in the department of Neurology, School of Medicine at Mersin University, Mersin, Turkey. His main research areas are sleep medicine and neurologic movement disorders.
Oya Itil is a professor in the department of Pulmonary Diseases, School of Medicine at Dokuz Eylul University, İzmir, Turkey. Her main research areas are pulmonary oncology and sleep medicine.
Hikmet Yilmaz is a professor in the department of Neurology, School of Medicine at Celal Bayar University, Manisa, Turkey. His main research areas are sleep medicine, epilepsy, and neurologic movement disorders.