
Abstract
Background:
As shift workers, nurses are at an increased risk of drowsy driving because of long hours at work and/or short sleep periods between shifts.
Methods:
In this study, a descriptive cross-sectional cohort design was used to examine the prevalence of drowsy driving among nurses.
Findings:
An electronic survey was sent to 7,217 nurses of which 2,205 (30.5%) completed the survey. Thirty percent (672 nurses) reported having dozed off while driving during their commute to work. In addition, 44.6% (976) of nurses disclosed feeling unsafe or uncomfortable during their commute due to drowsiness or fatigue.
Conclusion/Application to Practice:
As shift workers, nurses are subject to drowsy driving and its untoward effects. Healthcare leaders and nurse executives are in a position to evaluate and explore fatigue mitigation strategies such as napping, as this may prove to be beneficial in supporting nurse well-being and public safety.
Background
The National Highway Traffic Safety Administration (NHTSA) estimates that drowsy driving is responsible for 72,000 crashes, 44,000 injuries, and 800 deaths annually (U.S. Department of Transportation, National Highway Traffic Safety Administration [NHTSA], 2017). Both NHTSA and the Centers for Disease Control (CDC) have identified shift workers as having an increased risk of drowsy driving because they typically work irregular shifts, night shifts, and/or long hours. Nurses make up a significant portion of the shift worker population as hospitals are open 24 hours to serve and meet community needs (U. S. Bureau of Labor Statistics [BLS], 2022).
According to the CDC, drowsy driving is when someone operates a motor vehicle while fatigued or sleepy (Centers for Disease and Control [CDC], n.d.) Signs and symptoms of drowsy driving include frequent yawning, rapid blinking, and drifting outside of the lane and in severe cases, falling asleep at the wheel (CDC, n.d.). The dangers of drowsy driving are far reaching and extend beyond self-harm. In fact, researchers have found that the impairment of individuals who drive while fatigued mirrors the impairment that occurs when driving while intoxicated. Furthermore, mounting evidence suggests that being awake for 18 hours or more results in the same level of impairment as someone having a blood alcohol content of 0.05% (Geiger-Brown & McDonald, 2021; Saadat et al., 2018; “Practice Safe Driving,” 2017). The legal blood alcohol content level limit in all 50 U.S. states is 0.08% (U.S. Department of Transportation, NHTSA, n.d.).
Although inpatient hospital nurses in the United States customarily work 12-hour shifts, some nurses routinely work beyond the scheduled 12-hour period due to care coordination, required documentation, and/or unexpected patient condition changes (Min et al., 2019). As a result, nurses may be at an increased risk for being awake for prolonged periods of time. For example, if a nurse works a 12-hour shift (07:00–19:00) and gets off on time, he or she still has to allot time for a commute home, to prepare or pick up a meal, take care of any household or family responsibilities, for example, child care, assist children with homework, shower/bathe, prior to actually being able to attempt sleep. These activities can account for an additional 4 to 6 hours in most cases, which would result in the individual nurse being awake for 18 hours or more. According to Westwell et al. (2021), night shift nurses typically get an average of 5.5 hours sleep between shifts. Furthermore, nurses working consecutive 12 hours shifts have insufficient time to recover between shifts and subsequently develop sleep debt (Mulhall et al., 2019; Parry et al., 2018).
While extensive research has been conducted to evaluate the prevalence and impact of drowsy driving among ground and air transportation industry workers, more research is needed to gain an in-depth understanding of nurses’ risk for drowsy driving as well as the frequency of occurrence. In addition, previous research has primarily focused on the number of hours of sleep received when assessing drowsy driving risks. While quantity of sleep is an essential element of data to analyze when evaluating drowsy driving, confounding factors (i.e., number of hours worked), which can impede a person’s ability to obtain adequate sleep should also be studied. Therefore, this study examines the prevalence of drowsy driving among nurses, and explores nurses’ interest in interventions that may reduce accidents related to drowsy driving.
Methods
A descriptive cross-sectional cohort design was used to examine the prevalence of drowsy driving among nurses and whether hours worked, and sleep quantity are related to drowsy driving. Workforce management software was used to identify employed registered nurses and licensed practical nurses. An electronic questionnaire was then emailed to the targeted population for voluntary completion. Nurses who had accepted an offer of employment but had not attended new employee orientation at the time of the survey period were excluded. The survey included a total of 25 questions, of which 24 were multiple choice style and one question was of the open-ended style. Supplemental material provides a complete list of questions that respondents answered.
The research protocol was submitted to and approved by the Institutional Review Board.
Results
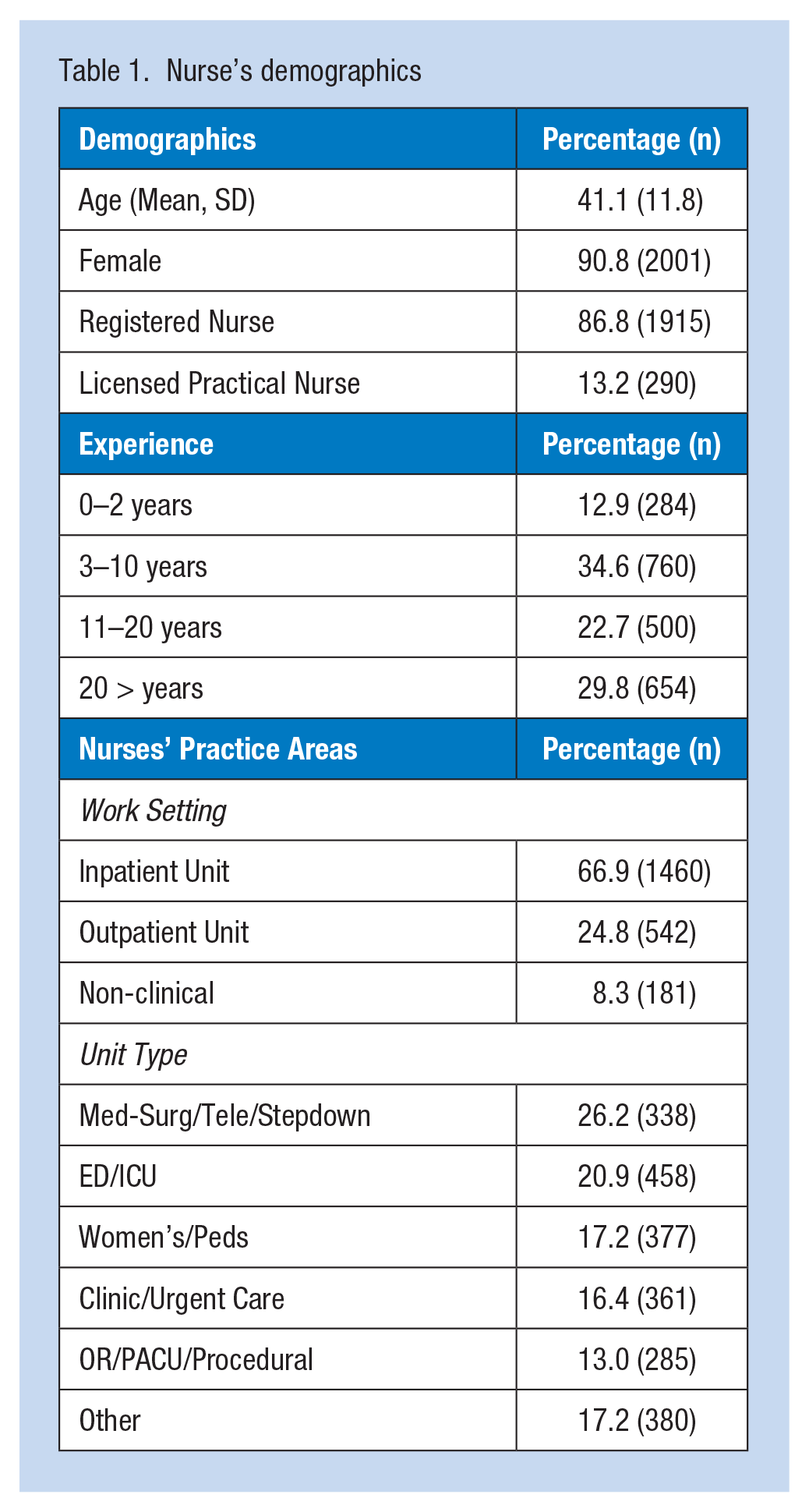
The electronic survey was sent to 7,217 nurses who met the inclusion criteria, of which 2,205 (30.5%) completed the survey. The mean age of survey participants was 41 years old. Registered nurses (RNs) comprised 86.8% (n = 1,915) of survey respondents, and 90.8% of respondents were female. The experience of participants ranged from 0 to 20+ years. Table 1 provides in-depth sample demographic details.
Nurse’s demographics
Of those who completed the survey, 30% (672 nurses) reported having dozed off while driving during their commute home from work (Figure 1). In addition, 44.6% (n = 976) of nurses disclosed feeling unsafe or uncomfortable during their commute due to drowsiness or fatigue (Figure 1). When asked about fatigue mitigation measures, 32.1% (n = 705) expressed being extremely interested in the ability to take a 15- to 30-minute nap during their shift as a means to reduce drowsy driving (Figure 2). However, 32.7% of respondents verbalized being highly unlikely to take advantage of an Uber/Lyft offering, and 30.4% reported being highly unlikely to utilize a hospital-affiliated hotel as a means to mitigate drowsy driving (Figure 2).
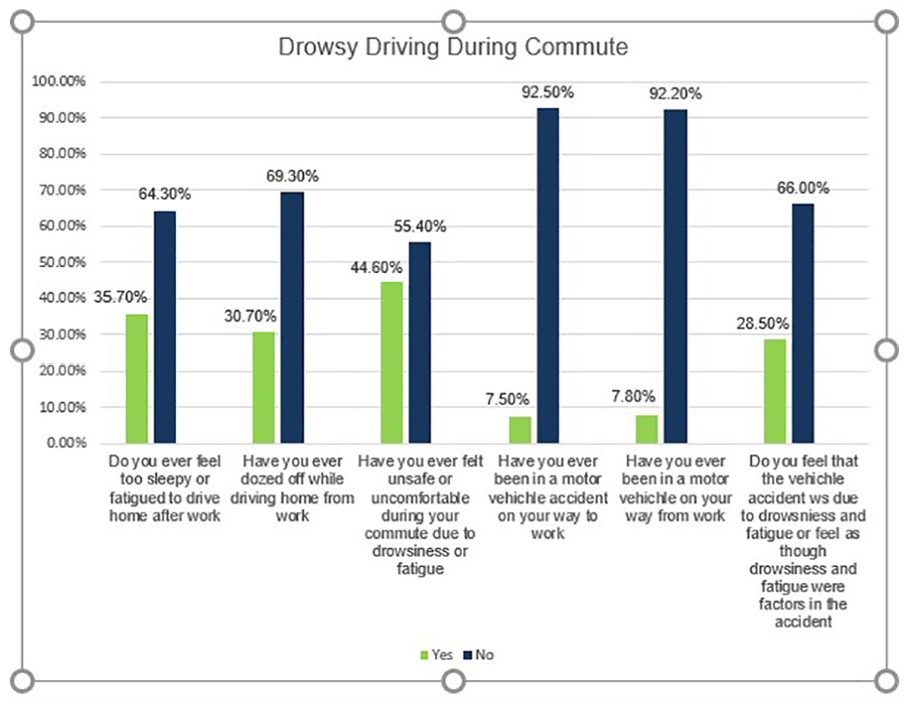
Drowsing driving during commutes.
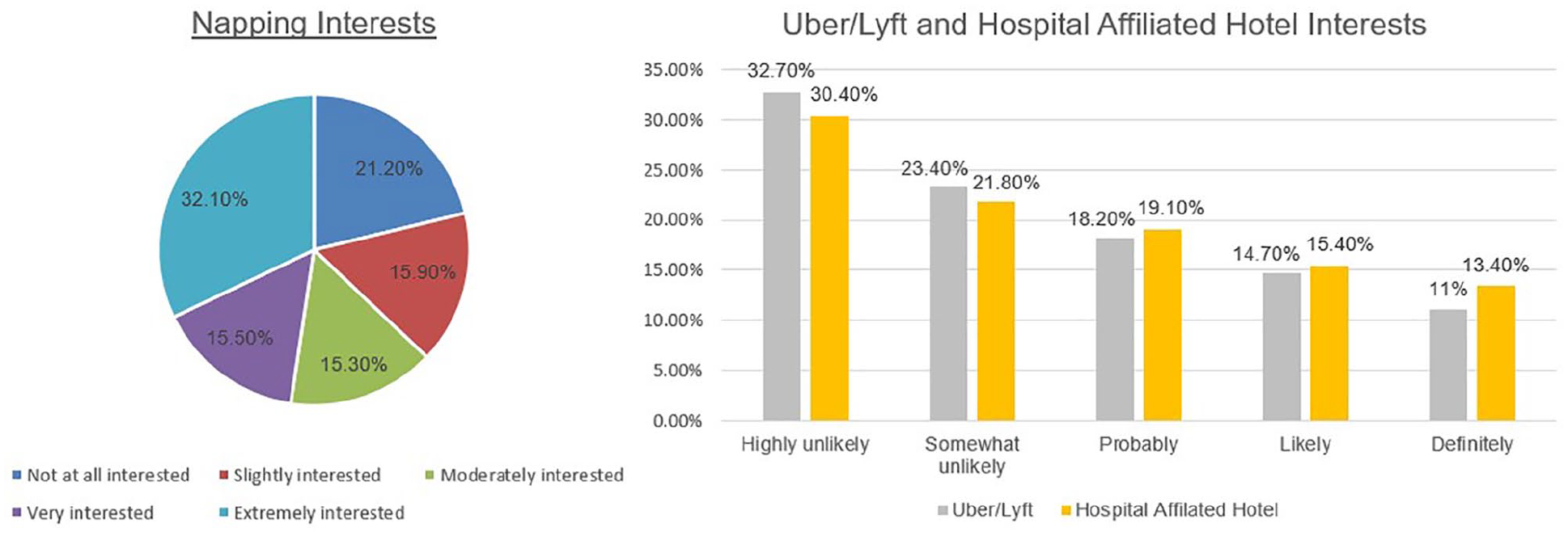
Drowsy driving prevention interests.
Several themes and commonalities emerged in relation to which specific unit/department type a nurse worked. Emergency department and critical care nurses commonly reported challenges with long commute times, ability to take uninterrupted lunch breaks, coffee breaks, and restroom breaks during their shifts. In addition, these nurses routinely expressed naps would be beneficial on night shifts. Equally, women’s health and pediatric nurses verbalized opinions that napping on night shift would help significantly with feelings of fatigue and drowsy driving. Clinic and urgent care nurses consistently reported that fatigue was more of a challenge when they worked in the inpatient setting and/or night shift. In addition, they expressed that fatigue was related to underlying health conditions such as pain or arthritis. Operating room, postanesthesia care unit (PACU), and procedural care nurses consistently reported a challenge with obtaining adequate rest and sleep secondary to on-call shift requirements and the time between their next scheduled shift. Similarly, medical-surgical/telemetry and stepdown nurses shared concern related to the inability to get sufficient rest and sleep due to long shift lengths.
Discussion
In this study, the prevalence of drowsy driving among nurses was evaluated. It was found that 30% (n = 672) nurses reported having dozed off while driving during their commute from work. This finding supports prior research conducted by Smith et al. (2020), which examined the prevalence in which nurses experienced drowsy driving as well as the interventions used to mitigate the untoward effects of driving while drowsy. Sixty percent of participants reported experiencing drowsy driving at least once a week, whereas the remaining 40% of participants reported experiencing drowsy driving more frequently, for example, after every shift.
A secondary purpose of this study explored nurse’s interest in fatigue mitigation strategies such as napping, Uber/Lyft, or hospital-affiliated hotels to reduce the likelihood of drowsy driving. Just over twenty-one percent (21.2%) verbalized that they were not interested in the option to nap during their shift. Nearly seventy-nine (78.8%) of nurses expressed some level of interest in the ability to take a 15- to 30-minute nap during their shift, while 32.1% expressed extreme interest in the ability to do so. Although nurses have expressed an interest in the practice of napping, most hospitals and healthcare systems in the United States have policies that prohibit nurses from being able to nap at work, even during lunch breaks or coffee breaks. Nurses are the largest work force segment of employees in the healthcare industry and work long, irregular hours, often taking on-call shifts likened to physicians and residents (Ma & Stimpfel, 2018). Most hospitals provide designated sleep rooms and/or on-call rooms for physicians and residents as a means to mitigate fatigue, but similar spaces for nurses are rare. In a study to evaluate the state and presence of fatigue risk management systems (FRMS) in hospitals across the United States, nurse sleep spaces/rooms were reported in only 4% of surveyed hospitals (Steege et al., 2017). High-reliability industries such as aviation have strategically invested in several strategies to reduce and mitigate fatigue to include daily and weekly hour restrictions/limitations, anonymous fatigue self-reporting, allowance of napping and safe scheduling (IATA, 2015). Therefore, in addition to examining rest spaces, nurse executives and leaders should consider the need for sleep and rest when creating and approving nurse’s work schedules (Westley et al., 2020). More research is needed to understand the best approach to overcome the barriers to implementing fatigue risk management controls such as napping in nursing.
Only 11% of respondents expressed strong interest in the option to take an Uber/Lyft home after their shift in an effort to prevent drowsy driving, whereas 32.7% shared that they would be highly unlikely to take advantage of an Uber/Lyft offering. Free text comments provided by respondents highlighted the rationale behind this response. Participants expressed concern related to logistics surrounding the Uber/Lyft and hospital-affiliated hotel offerings. For example, respondents asked “How would I get back to my car if I caught an Uber home?” Similarly, other comments included, “I cannot stay at the hotel after my shift, I have to get home to my children. This would not work for me.” Qualitative findings from this study also revealed that fatigue mitigation strategies may need to vary based on department, unit type, specialty area. For example, emergency room and critical care nurses reported different concerns related to drowsy driving than operating room/PACU/procedural area nurses. Further research is needed to understand how specific shift characteristics such as type of shift, shift length, may impact drowsy driving and fatigue-related risks.
Data for this study came from a single healthcare system, which may limit its generalizability. In addition, self-reporting survey data rely on individual participant’s recollection of events and memory. Despite these limitations, there are implications for practice. As shift workers, nurses are at risk for drowsy driving and its untoward effects. Healthcare leaders and nurse executives should evaluate and explore fatigue mitigation strategies such as napping, as they may prove to be beneficial in supporting nurse well-being and public safety.
Applications to Professional Practice
An electronic survey revealed that nurses, like other shift workers, are at risk for drowsy driving given their irregular and nontraditional work hours and schedules. Thirty percent of nurses reported having dozed off while driving during their commute to work, while 44.6% of nurses disclosed feeling unsafe or uncomfortable during their commute due to drowsiness or fatigue. Drowsy driving not only impacts the nurse but also the public safety of other motorists. Therefore, nurse leaders and occupational health experts should explore and implement mitigation measures such as napping, fatigue risk management programs, and safe scheduling practices.
Supplemental Material
sj-docx-1-whs-10.1177_21650799221111300 – Supplemental material for Drowsy Driving Among Nurses: Potential Impetus to Support Napping
Supplemental material, sj-docx-1-whs-10.1177_21650799221111300 for Drowsy Driving Among Nurses: Potential Impetus to Support Napping by Jlynn A. Westley, Jessica Peterson and Bianca Cook in Workplace Health & Safety
Footnotes
Conflict of Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The research protocol (IRB ID: 2019.339) was submitted to and approved by the Institutional Review Board. The IRB declared the study was exempt and issued a full waiver of HIPAA authorization for the study on October 19, 2019.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.