
Abstract
Background:
We sought the opinions of health care workers (HCWs) at a designated COVID-19 facility receiving the first cases to identify workplace modifications and inform effective changes to maximize health and safety at the onset of a crisis.
Methods:
A cross-sectional study utilized open- and close-ended questions gathered demographic and work details, experiences and perspectives on infection control, communication, support, and the workplace. Qualitative data were analyzed thematically and quantitative were analyzed using descriptive statistics.
Findings:
Of 340 HCWs, most approved of the organization’s response to minimizing risk (81.0%), infection control training (81.1%), and supplies (74.3%). Key actions included up-to-date guidelines (93.6%) and specialized infectious diseases clinics (94.9%). Conclusions: HCWs rated the organization’s adaptive changes highly, noting areas for improvement such as transparency and timeliness of communication. Incorporating input from HCWs when responding to health crises was beneficial to maximize staff health and safety and consequently that of patients.
Keywords
Background
The COVID-19 pandemic affected nearly every country in the world (Worldometer, 2021). Health care systems, and consequently their workers, were simultaneously tending to people infected with a highly contagious disease and adapting practices to best protect their workforce.
Health care workers (HCWs), defined as people who deliver care and services to the sick including aides, waste handlers (Joseph & Joseph, 2016), hospital volunteers, and administrative workers (Centers for Disease Control and Prevention, 2016), are concomitantly at high risk (Amnesty International, 2021) while being a critical resource in fighting the pandemic.
Protection of staff and patients has required adaptations by health care services and workplace environments (Legido-Quigley et al., 2020). Incorporating the opinions of frontline HCWs can optimize staff well-being and the effectiveness of health service changes (Vindrola-Padros et al., 2020). Work health and safety legislation in Australia (Australian Government, 2011) and other countries (e.g., Federal Ministry of Justice, 1996; Parliament of the United Kingdom, 1974) emphasizes and endorses the involvement of all workers in ensuring a safe workplace. Beyond physical safety, workers communicating concerns and opinions can facilitate positive outcomes, creating a work environment responsive to the needs and concerns of its workers (Holland et al., 2013). Reflecting on and evaluating past experiences can foster preparedness for future situations and help mitigate risk and longer-term consequences.
This study aimed to explore HCWs’ views about measures implemented in response to the first wave of the pandemic and to elicit their opinions on how best to prepare for the future. Their experiences and perceptions will assist in providing a safe and healthy workplace for this evolving pandemic and future crises.
Methods
We conducted a retrospective cross-sectional survey of HCWs at a public hospital in New South Wales (NSW), Australia, following the peak of the first wave of the COVID-19 pandemic in 2020.
Study Population and Participant Recruitment
Participants were employed at one of the largest tertiary hospitals in Australia with over 800 beds, approximately 6,000 staff, expertise in all fields of medical care, and one of the first designated facilities to treat COVID-19 patients in NSW. The survey was conducted between November 3, 2020 and January 31, 2021. Staff who during mid-March to mid-May 2020 had worked in departments that were most likely to be affected by the pandemic (COVID-19 ward, COVID-19 testing clinic, Emergency Department, Intensive Care Unit, Respiratory Department, Cardiology and Infectious Diseases) and staff responsible for the hospital’s response to COVID-19 were invited to participate. A link to the online questionnaire was distributed via email; a reminder was sent after 3 weeks. A hard copy version was also available. In December 2020, the study was opened to all hospital staff, acknowledging the impact on the work environment of all staff. Flyers containing the study QR code were distributed to staff and promotional posters with the QR code and a web link to the questionnaire were distributed at the hospital.
Ethical approval was obtained from the Western Sydney Local Health District’s Human Research Ethics Committee (2020/ETH01674). Participants provided informed consent before completing the anonymous questionnaire which concluded with four sources for assistance should they have any concerns they wished to discuss.
Data Collection Instrument
The questionnaire, designed and pilot tested by the researchers, included close-ended questions which asked about staff’s demographics, professional role, experiences, and their perspectives on infection control, communication, support, flexible working practice, and workplace culture during the first wave of the pandemic. It also included two open-ended questions: “What did you value most from the changes implemented by your employer in response to COVID-19?” and “What would you have liked your employer to have done, or done differently, to better support you during the COVID-19 pandemic?”
Data Analysis
Quantitative data were analyzed using Stata (StataCorp, 2015) to describe the numbers and proportions of HCWs who reported a particular experience or opinion. Chi-square test was used to determine the significant differences between occupational groups. Fisher’s exact test was used for cell sizes less than five. Responses to the open-ended questions were analyzed using thematic analysis (Guest et al., 2011).
Results
Out of the 432 HCWs who completed the survey, 340 (78.7%) answered the close-ended questions. Most participants (39.4%) were nurses and medical doctors (17.4%) (Table 1). The majority (77.8%) of participants had a patient-facing role. Two in five (40.4%) worked in high-risk areas including the COVID-19 ward/clinic (8.0%), intensive care unit (19.9%), emergency department (11.6%), and infectious diseases (0.9%). Seventy-six (22.5%) had a manager/supervisory role.
Characteristics of Healthcare Workers and Their Work Roles (n = 340)
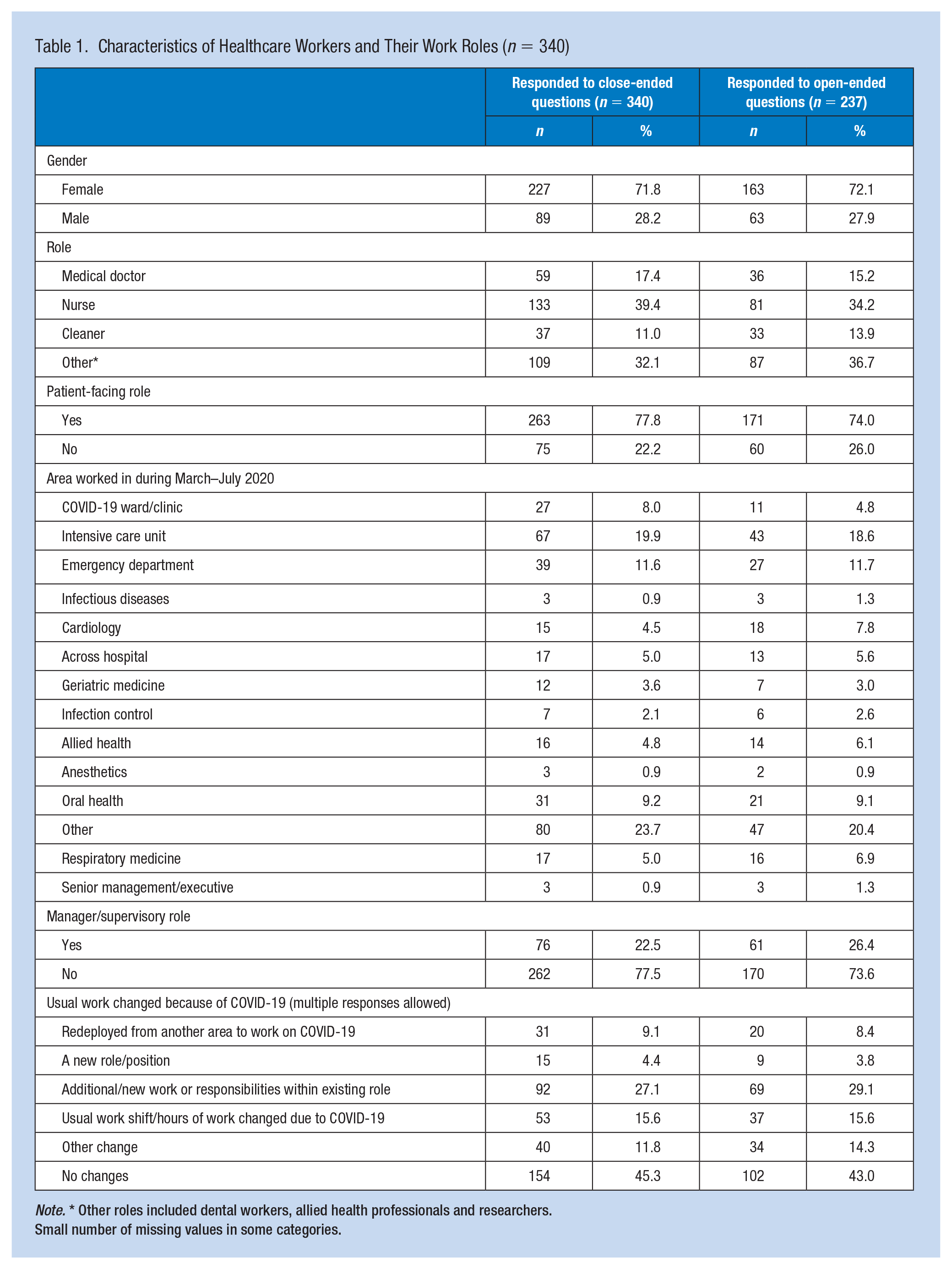
Note. * Other roles included dental workers, allied health professionals and researchers.
Small number of missing values in some categories.
More than two-thirds (69.7%) of respondents answered the open-ended questions. This subgroup was similar to the respondents of the close-ended questions.
Quantitative Findings
HCWs’ experiences and perceptions of the changes encountered during the pandemic indicated the organization was rated most positively on infection control, including adequate safety training (81.1%), and most poorly on addressing the impact of COVID-19 on career progression (26.4%) (Table 2). Doctors were generally less positive than others in their evaluations. Doctors were the most concerned that personal protective equipment (PPE) would run out (74.6%), most likely to encounter circumstances where patient care was compromised (62.7%) and least likely to have opportunities to express concerns to their manager (52.5%). However, doctors were the least aware of conflict between HCWs (22.0%).
Workplace Experiences of Health Care Workers During the Height of the Pandemic (March–May 2020)
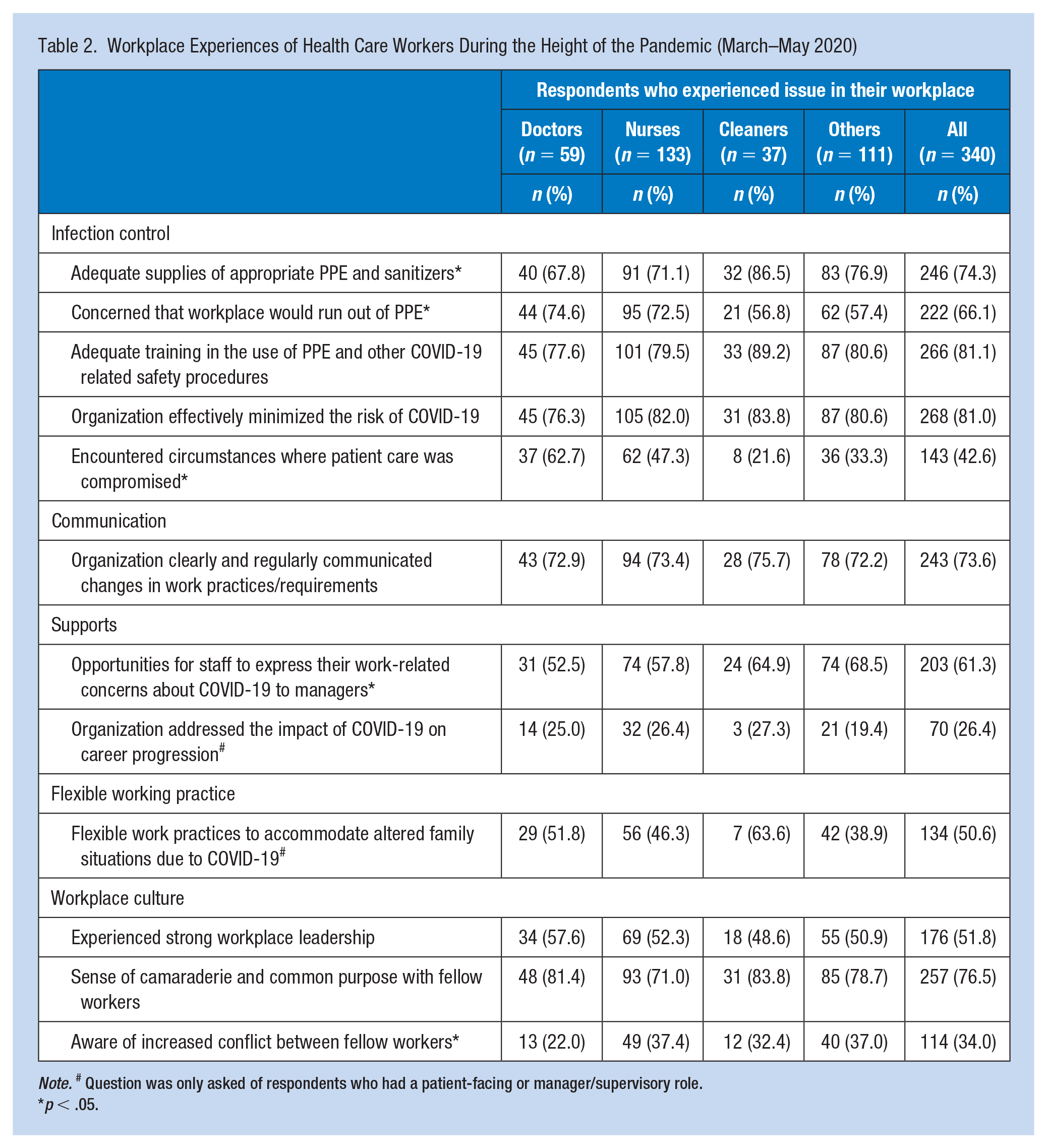
Note. # Question was only asked of respondents who had a patient-facing or manager/supervisory role.
p < .05.
Ratings by HCWs in patient-facing or manager/supervisory roles on the usefulness of measures to prepare for and respond to future pandemics (Table 3) indicated that most (94.9%) rated specialized clinics for patients with suspected infection as useful/extremely useful. Fewer (63.6%) rated centralized storage and supply of PPE similarly. Responses were similar irrespective of role.
Measures for Preparing for or Responding to Future Pandemics
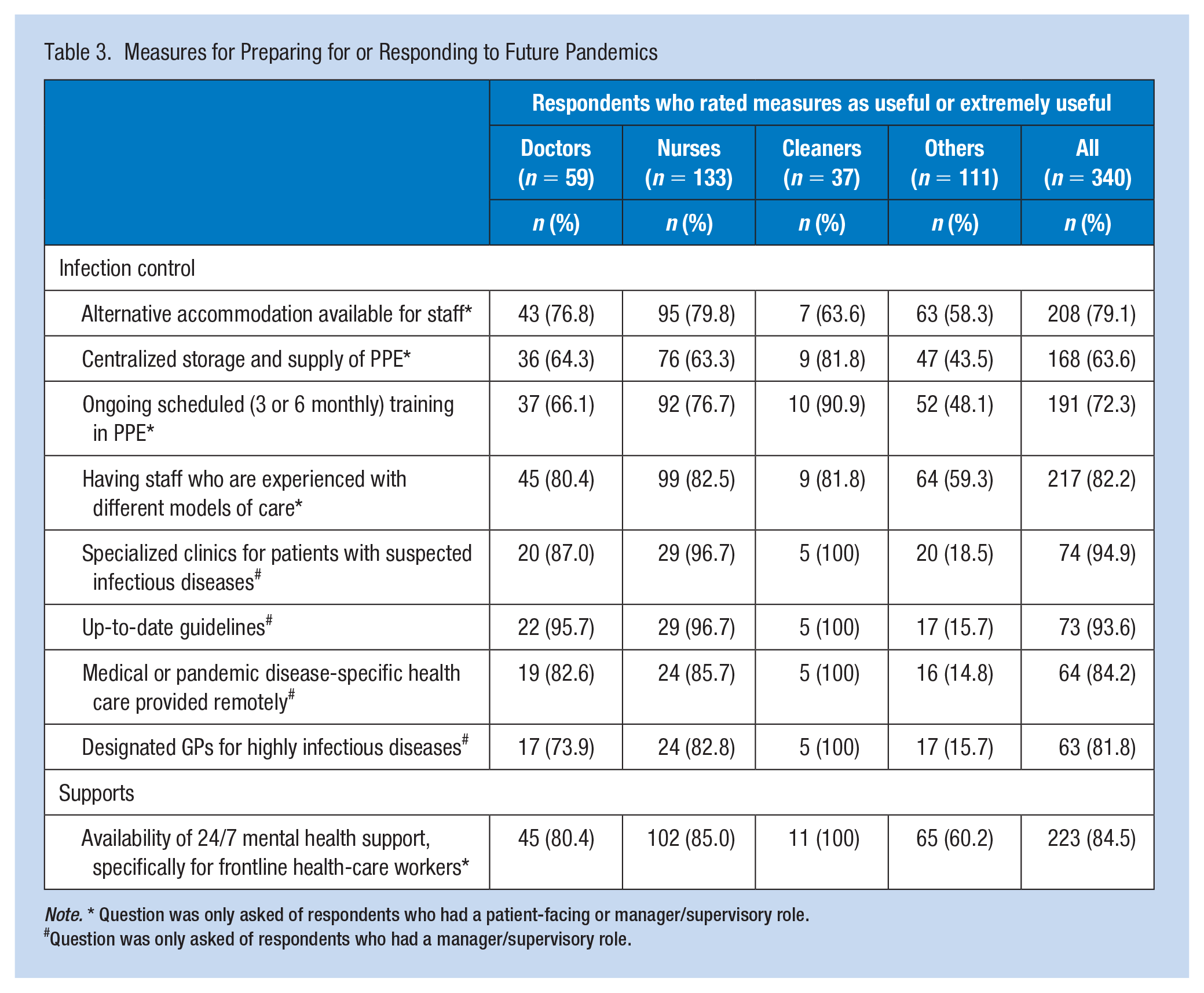
Note. * Question was only asked of respondents who had a patient-facing or manager/supervisory role.
Question was only asked of respondents who had a manager/supervisory role.
Qualitative Findings
Infection control (40.2% of all 209 responses), followed by communication (14.3%) were the most common themes identified in the open-ended responses about the change most valued (Supplementary Table 1). Cleaners most valued changes in infection control (56.3% of cleaners), while flexible working practices were most valued by other HCWs (22.0%).
Changes HCWs would have liked implemented to better support them during the pandemic (Supplementary Table 2) most frequently related to infection control (28.1% of the 196 suggestions) and communication (22.7%). Doctors were most likely to give suggestions about infection control (39.3% of all doctors) and communication (32.1%), while nurses’ focus was on support (22.4%).
Exploration of Issues Raised by HCWs—Quantitative and Qualitative Results Combined
Infection control
Having specialized services clinics for patients with suspected infectious diseases was thought to be extremely useful (94.9%) (Table 3). A doctor praised the organization for “quickly making a negative pressure room in the Emergency Department.” However, the location of the COVID-19 ward and testing clinic was of concern: “People looking for the clinic would remove their masks to ask for directions on the way there which defeated the purpose of the masks.” (Nurse). It was suggested that the “COVID-19 testing . . . [be] in a separate building from the main hospital” (Nurse).
Three-quarters of HCWs felt they had adequate supplies of appropriate PPE and sanitizers as per the NSW guidelines. “We had everything we needed for protection—what we needed we got” (Cleaner). However, PPE should be suitable, fit properly, of quality, and comprehensive e.g., “correct protective gear N95 masks not surgical masks” (Nurse), with “. . . full face gowns” (Doctor).
Centralized storage and supply of PPE were rated as extremely useful or useful by 168 HCWs. A nurse valued “Having access to a centralized PPE storage . . . to keep staff safe and [provide] peace of mind knowing [that] it was sufficiently stocked.” Two-thirds of HCWs worried that their workplace would run out of PPE.
Health care workers (81.1%) considered training in the use of PPE and other COVID-19-related safety measures was adequate. “Training using PPE, donning, doffing, sanitizers, making sure staff are comfortable to work with COVID patients” (Cleaner) to “[make] sure we were safe when in contact with patients” (Cleaner). The majority of HCWs supported ongoing scheduled PPE training.
Managers (93.6%) highly valued having up-to-date guidelines, which should be “along the same path as directives given by our professional advisory bodies” (Doctor) and “consistent [because] it was too hard to keep up with all the changes” (Other HCW).
Health care workers (81%) felt that the organization had effectively minimized the risk of COVID-19 through modified work practices. Changes most valued were strict screening, limits on visitor numbers, social distancing, and mask wearing. Despite these, some (42.6%) staff had encountered circumstances where patient care was compromised. Health care workers also wanted “Mask wearing enforced and temperature checks on arrival of staff and visitors during the night . . .” (Admin staff) and “Every patient tested before being transferred to [a] general ward” (Nurse).
The hospital was praised for “The quick response to safety of staff by making [the] work area a safe place and [ongoing] checking and stocking of required gears” (Admin). However, some HCWs thought that “PPE should [have been] made mandatory since the early stage” (Nurse) and “Fit testing of the masks should have been completed at the beginning of the pandemic” (Nurse).
Most HCWs rated measures to prepare for future pandemics as useful/extremely useful: having staff who were experienced with different models of care for pandemic preparedness; medical or pandemic disease-specific health care provided remotely to reduce the burden on hospitals; designated health care providers for highly infectious diseases; and “. . . a pandemic management plan appropriate for each facility” (Oral health worker).
Communication
Health care workers felt that changes in work practices and requirements were clearly and regularly communicated. There was “staff information on the intranet” (Admin) and “daily information updates” (Admin). However, some HCWs thought that there should be “Clearer updates on restrictions/news” (Doctor) and “highlighting what is no longer [current] practice” (Nurse).
Health care workers would have welcomed identified avenues of communication that would have avoided “. . . whispers (i.e., informal communication that results in dissemination of inaccuracies) still happened.” Clinical staff also felt there was insufficient “transparency around decisions” and the application of rules, which fostered perceptions that “Some staff seemed to be being paid to stay home and not work for [any] reason, while others are expected to pick up the slack.”
Health care workers felt that information from those at the front line was unexploited particularly in decision-making. “Upper managers [should be] listening/communicating with grass-root workers asking about issues/problems rather than just communicating with managers” (Nurse). Managers should “Appreciate thoughts and planning of ground staff” (Nurse) on issues such as “how [the] restructure of ICU [Intensive Care Unit] during the pandemic negatively affected the frontlines” (Nurse).
Some HCWs expressed concern that communication was not timely, sometimes causing inconvenience or not allowing sufficient time to respond to the changes, for example, “I was moved multiple times during the peak and each time I felt that I was only informed a day or two before, which became unsettling. I was never sure what to expect, one day to the next.” (Nurse)
Support from organization
Health care workers (84.5%) thought that the availability of mental health support was useful/extremely useful. An administration worker was thankful for “. . . being recognized by [my] manager when my mental health was suffering and advised to use EAP [employer assistance program] which I did.” However, a wider range of support options such as “onsite counselling” (Nurse)—would have been appreciated.
Some HCWs would have liked “Increased leave for stress and other mental health related issues” (Nurse) and “COVID sick leave” (Allied health) because “It was extremely difficult wearing the cost of unpaid sick days while waiting for COVID test results” (Allied health).
Two-thirds of HCWs felt they were provided opportunities to express work-related concerns about COVID-19. However, only a quarter felt that the impact of COVID-19 on career progression had been addressed. Many HCWs were redeployed to work in COVID-19-related areas. They felt that “The redeployment increased . . . stress and instead of improving our continuing education we were made to work on something very unfamiliar and extremely distressing” (Nurse). The negative impact on career progression could have been ameliorated by “better discussions with staff prior to redeployment” (Oral health services).
Flexible working practices
Half of the HCWs expressed that the organization had provided flexible working practices in the form of “work from home” (Admin), “. . . to limit . . . the chance of being infected” (Oral health). The implementation of working from home policies could have been improved as “it was not easy to organize permission to work from home” (Allied health). Added to the challenge was the unavailability of necessary equipment, leading some to suggest that the organization should “provide appropriate equipment, rather than having to use [one’s] own (laptop)” (Admin).
Workplace culture
Half of the HCWs thought that the organization’s leadership in responding to COVID-19 was strong. A cleaner thought that “They [the organization] did their best.” Three-quarters felt a sense of camaraderie and common purpose with their fellow workers, which was echoed by a member of management who “. . . felt at the height of the pandemic we worked well to continue to deliver a high standard of care while preparing for the unknown . . .” (Other HCW). However, one-third were aware of increased conflict between fellow workers. Perceived unequal rostering for working in COVID-19 areas led one HCW to suggest that managers “could have allocated all the staff members fairly to look after COVID patients, as certain staff were getting COVID patients frequently” (Nurse).
Discussion
Health care workers at a designated COVID-19 facility in Australia during the first wave of COVID-19 pandemic were generally favorable in their evaluation of the infection control measures and communication efforts implemented by the organization. Issues relating to infection control and communication were frequently raised in the open-ended questions, indicating their importance to a pandemic or emergency situation. Generally, doctors tended to be less positive than others in their perceptions.
Employers have a legal obligation to provide a safe workplace, but this was particularly challenging in the initial stages of the pandemic. For HCWs, in the context of an infectious disease, especially one that is novel and deadly, protecting oneself, one’s loved ones, colleagues, and patients is a prime concern. While some HCWs expressed gratitude for the organization’s response, others stated that more should have been done or changes implemented sooner to improve safety.
Health care workers were concerned about the COVID-19 ward and testing clinic being located at the far end of the main hospital building, potentially enabling transmission of the virus. Clearly visible signs at the main entrance and at points along the way directing people to services would have been useful. The risk of infection if air from the COVID-19 ward leaked to other areas prompted the suggestion that the COVID-19 ward and testing clinic be separated from the building in an easy-to-find location. Concerns about the safety of COVID-19 facilities have also been reported recently for another hospital in Sydney (Scherer, 2021). Separate mobile hospitals dedicated to treating only COVID-19 patients can minimize infection of nonpandemic patients, whose utilization of hospital services has been reduced by a third due to fear of infection (Hategeka et al., 2021; Moynihan et al., 2021).
Health care workers identified the importance of PPE being suitable and well stocked, having regular training and receiving consistent guidelines, issues also raised by other HCWs (Ananda-Rajah et al., 2021; Nguyen et al., 2021; Vindrola-Padros et al., 2020). Some thought the guidelines were not sufficiently strict or timely as early in the pandemic masks were not comprehensively or effectively used. The inconsistent use of masks could have resulted from the confusion caused by the World Health Organization’s recommendation at the beginning of the pandemic that masks were not necessary (Chan et al., 2020).
Similarly, HCWs thought infection control measures should have been implemented earlier and be stricter. A preference was expressed for mandatory use of PPE from early on as opposed to HCWs initially being denied PPE (Hennequin, 2020; McCauley, 2020). Lack of knowledge about the disease and insufficient supplies could explain restrictions for full PPE use only with confirmed positive cases. One suggestion was to continue screening people at the hospital entrance after hours and at night.
Communication is not only key to keeping workers informed, but promotes feelings of being valued as it reduces conflict, increases engagement, and fosters teamwork (Bosworth, 2021). While HCWs valued regular updates, they also sought more detailed, transparent, and timely and multidirectional communication. Early in the pandemic, the organization and other health authorities issued many guidelines and policies as information and knowledge about severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and COVID-19 evolved. Inconsistencies and contradictory information between updates were common, highlighting the need for HCWs to stay up-to-date with the latest guidelines and regulations. Clarification of HCW’s role and requirements, especially for those redeployed to COVID-19 wards, would improve efficiency and reduce the risk of stress and anxiety. Transparent decision-making would minimize misunderstandings and conflicts. Furthermore, ongoing communication between managers and staff would support a mutual understanding of needs and concerns and an optimal working environment. Where possible, communication of change should be timely to allow for necessary adjustments.
Promoting and maintaining staff well-being is an essential aspect of a safe and healthy workplace (Black Dog Institute, 2021), which can be easily overlooked. Similar to other studies, mental health support was a common theme in the open-ended responses (Hennequin, 2020; Nguyen et al., 2021; Stubbs et al., 2021; Turner et al., 2021; Vindrola-Padros et al., 2020). Some HCWs expressed a preference for counseling and psychological support over the general meditation and wellness sessions that were offered, highlighting the real need for individual mental health support. Health care workers also desired financial support in terms of paid leave when they are furloughed because of contact with a COVID-19 case or the presence of flu-like symptoms.
For many HCWs, especially clinical staff, the nature of their role would have precluded many options for flexible work. Achieving a balance between HCWs’ desires and work demands can be a challenge, requiring innovative thinking to adapt tasks and processes to avoid inappropriate staffing and allow flexibility without compromising output. A “fair rostering” that is transparent and encouraging of feedback might be welcomed by HCWs.
While most HCWs felt a sense of camaraderie, some conflict still existed. Causes of workplace conflict include poor communication, an overwhelming workload, and unclear roles and responsibilities (Brownstone et al., 2021)—issues which were raised by our HCWs. Actively addressing these concerns may reduce conflict and further promote a sense of team spirit. In 2020, HCWs had concerns about appropriate and adequate PPE supplies, a vaccine was not yet available, and they were at high risk of infection (Hendrie, 2020; Nguyen et al., 2020; Quigley et al., 2021); not surprisingly, some HCWs were less willing to work (Hill et al., 2021; Johnson & Butcher, 2021). In 2022, PPE availability was no longer a concern and vaccines were readily available, which, along with fair rostering and increased mental health support may help to reduce anxiety and bolster HCWs against challenges. Attention to communication, workload, and responsibilities during “normal” and pandemic operation alike should support a positive workplace culture and patient care (Sergeant & Laws-Chapman, 2021).
The use of mixed methods allowed us to describe patterns in experiences and perceptions and provide more in-depth analysis of details from participants, many of whom had a patient-facing role. The reasonably large sample size for the qualitative component enabled thorough exploration of experiences, perceptions, and recommendations.
Recall bias may have affected results as the survey was conducted half a year after the period we were investigating. Participants may have been influenced also by up-to-date knowledge about COVID-19 and might have compared their experiences with current standards, changing their perceptions to be more or less critical. Furthermore, some participants in managerial or supervisory roles might have been biased in their judgment of the hospital’s response as they were more directly involved in the decision-making.
Implications for Occupational Health Practice
Infection control measures and communication stood out as the issues HCWs were most passionate about in terms of changes they valued and where they desired better support from the organization to achieve a safe and effective workplace now and into the future. Good infection control depends on knowledge of the pathogen, mechanisms for protection and the availability of necessary equipment, with communication that goes beyond the simple transfer of information to effectively mobilize a workforce.
Throughout the pandemic, health services need to quickly adapt to new and evolving situations to safeguard the physical and mental health and safety of staff and patients. To maximize the effectiveness of the changes to systems and practices, addressing HCWs’ opinions and perceptions about their working environment is essential. The results of this study are relevant to not only health services in Australia but to other health services dealing with the outbreak of a highly infectious disease.
Applying Research to Occupational Health Practice
Health care workers reported positive experiences and perceptions about their workplace environment during the first wave of the COVID-19 pandemic describing strong organizational leadership that placed infection control as a top priority, adequate availability of PPE and opportunities to express work-related concerns about COVID-19. They also offered suggestions health care services should consider when determining and mandating changes to protect the safety and well-being of staff and patients, while maintaining service delivery. Suggestions included: designated facilities to treat COVID-19 patients, separated from the main hospital; suitable, properly fitted, high quality and comprehensive personal protective equipment; regular COVID-19 safety training; up-to-date and consistent guidelines; timely infection control measures; clear, regular, transparent, and multidimensional communication; on-site mental health support; availability of sick leave and COVID-19-related leave; support for staff career; support for working from home; and fair rostering for frontline positions. Ensuring HCWs’ concerns are addressed will maximize the effectiveness of changes in providing a safe and healthy workplace. These suggestions are relevant across geographical settings and are applicable to any infectious disease outbreak.
Supplemental Material
sj-docx-1-whs-10.1177_21650799221102299 – Supplemental material for Using the Experiences and Perceptions of Health Care Workers to Improve the Health Care Response to the COVID-19 Pandemic
Supplemental material, sj-docx-1-whs-10.1177_21650799221102299 for Using the Experiences and Perceptions of Health Care Workers to Improve the Health Care Response to the COVID-19 Pandemic by Lieu Thi Thuy Trinh, Joanne M. Stubbs, Nicole Gilroy, Suzanne Schindeler and Helen Achat in Workplace Health & Safety
Footnotes
Acknowledgements
The authors would like to thank the participants for their valuable involvement, Jing Kong for her invaluable advice and support in engaging study participants, Thomas Solano and Ramon Shaban for their assistance in the early phase of the project, Leendert Moerkerken for his expert assistance with SurveyMonkey, Rakhi Mittal for her assistance in promoting the study to hospital staff and comments, and Veth Guevara for comments.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.