
Abstract
Background
Effective health communication is crucial for achieving positive population health outcomes. This is important for infection prevention and control (IPC), which relies on widespread public compliance to be effective. Whilst social media (SM) platforms disseminate health information, there is conflicting evidence to suggest their influence on compliance with public health guidelines.
Objective
To appraise the available evidence and determine the extent to which social media exposure contributes to public compliance with IPC measures.
Methods
A systematic protocol based on the MOOSE and PRISMA guidelines was followed. Observational studies were identified through systematic searches of four electronic databases and a hand search. Following data extraction, eligible studies were quality assessed, and the findings were integrated using narrative synthesis.
Findings
15 studies were included. The studies located presented heterogeneous designs and findings. A weak positive association was identified, with 60% of the studies observing a positive association between social media and compliance with IPC measures. 26.7% identified a negative correlation, and 13.3% identified no correlation. Several factors were identified to mediate the relationship, including knowledge and conspiracy beliefs.
Discussion
This systematic review identified a weak positive correlation between exposure to social media and public compliance with recommended IPC measures, suggesting that social media should be utilised in future IPC related communication strategies. Social media provides a cost-effective, publicly accessible platform to disseminate accurate information, and neutralise misinformation. Recommendations are made for further research to reduce the uncertainty created by the identification of heterogenous studies.
Introduction
Effective health communication is crucial for achieving positive population health outcomes (World Health Organisation [WHO], 2021). The ever-increasing utilisation of social media makes these platforms effective for the widespread, rapid dissemination of health information (Cawcutt et al., 2019). This is particularly important for infection prevention and control (IPC) during an infectious disease outbreak, where the public require clear guidance on how their behaviours can help prevent transmission of infection (Lee and Basnyat, 2012).
IPC measures, which include non-pharmacological interventions such as hand washing, social distancing and isolation (Al-Dmour et al., 2020), have been used throughout history. These behaviours were used to contain the 1918 Spanish flu pandemic, and were critical to reducing transmission, mortality and hospitalisations during the COVID-19 pandemic (Massaro et al., 2021). However, as IPC measures rely on conscious individual behaviour change to be effective (Seale et al., 2020), public awareness and understanding is fundamental to increase compliance (Public Health England [PHE], 2021). Al-Dmour et al. (2020) suggest social media campaigns are critical for improving public health behaviours, by inducing widespread behaviour change.
Recently, the use of social media for infectious disease communication has received increased academic attention (Tang et al., 2018). Despite recommendation by the World Health Organisation (2021), there is limited evidence to suggest the degree to which social media platforms contribute to infection prevention during an outbreak or epidemic (Al-Dmour et al., 2020). This is exacerbated by contradictory existing literature. Júnior et al. (2021), Ölcer et al. (2020), and Shin et al. (2021) identified social media to be associated with poor compliance with IPC measures. Whilst Guo et al. (2020) observed that social media use was associated with improved compliance. Consequently, further research is required.
The use of social media to disseminate health information may provide a tool to increase public compliance, and reduce the burden of infectious diseases within communities (Madhumathi et al., 2021). This systematic review critically appraises the evidence, to determine the extent to which social media exposure contributes to compliance with IPC measures. Recommendations inform the design of effective communication strategies and interventions for community IPC, thereby contributing to future outbreaks of infectious disease (Anwar et al., 2020).
Methods
All methods employed in the conduct of this systematic review adhere to the Meta-analysis of Observational Studies in Epidemiology (MOOSE) guidelines (Stroup et al., 2009), and the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines (PRISMA, 2021).
Search Strategy
Relevant search terms, including social media, infection prevention, infection control, non-pharmacological interventions (NPIs), behaviour change, adherence and compliance, were selected to search four electronic databases: CINAHL, Medline, PubMed and Google Scholar. This was followed by a hand search of bibliographies, using a backward searching method (Boland et al., 2017).
Inclusion/Exclusion Criteria
Inclusion criteria: published between 2011 and 2021, conducted in a community setting, focussed on non-pharmacological interventions, available in full text and published in the English language.
Exclusion criteria: Quantitative and observational. RCTs were excluded as they were not considered suitable to answer the research question.
Screening and Selection
Application of the inclusion/exclusion criteria utilised a screening and selection tool (Boland et al., 2017), piloted on 10 titles and abstracts. A random selection of 10 titles and abstracts were double screened by the same reviewer 1 week apart (Boland et al. 2017) to reduce the risk of error and establish a degree of test-retest reliability (Matheson, 2019). Duplicated studies were removed, as were those that did not meet the inclusion criteria based on their titles and abstracts. Following the resolution of any discrepancies identified from the double screening process (Boland et al., 2017), the selected titles were acquired in full-text, and assessed for eligibility for inclusion in the review.
In order to adhere to the PRISMA guidelines, this information has been presented in a PRISMA flow diagram (PRISMA, 2021). See Figure 1. PRISMA Flow Diagram of Included Studies from ‘Preferred Reporting Items for Systematic Reviews and Meta-Analyses’, by D. Moher, J. Tetzlaff, and D. G. Altman, 2009, PLoS Med, 6, p. e1000097.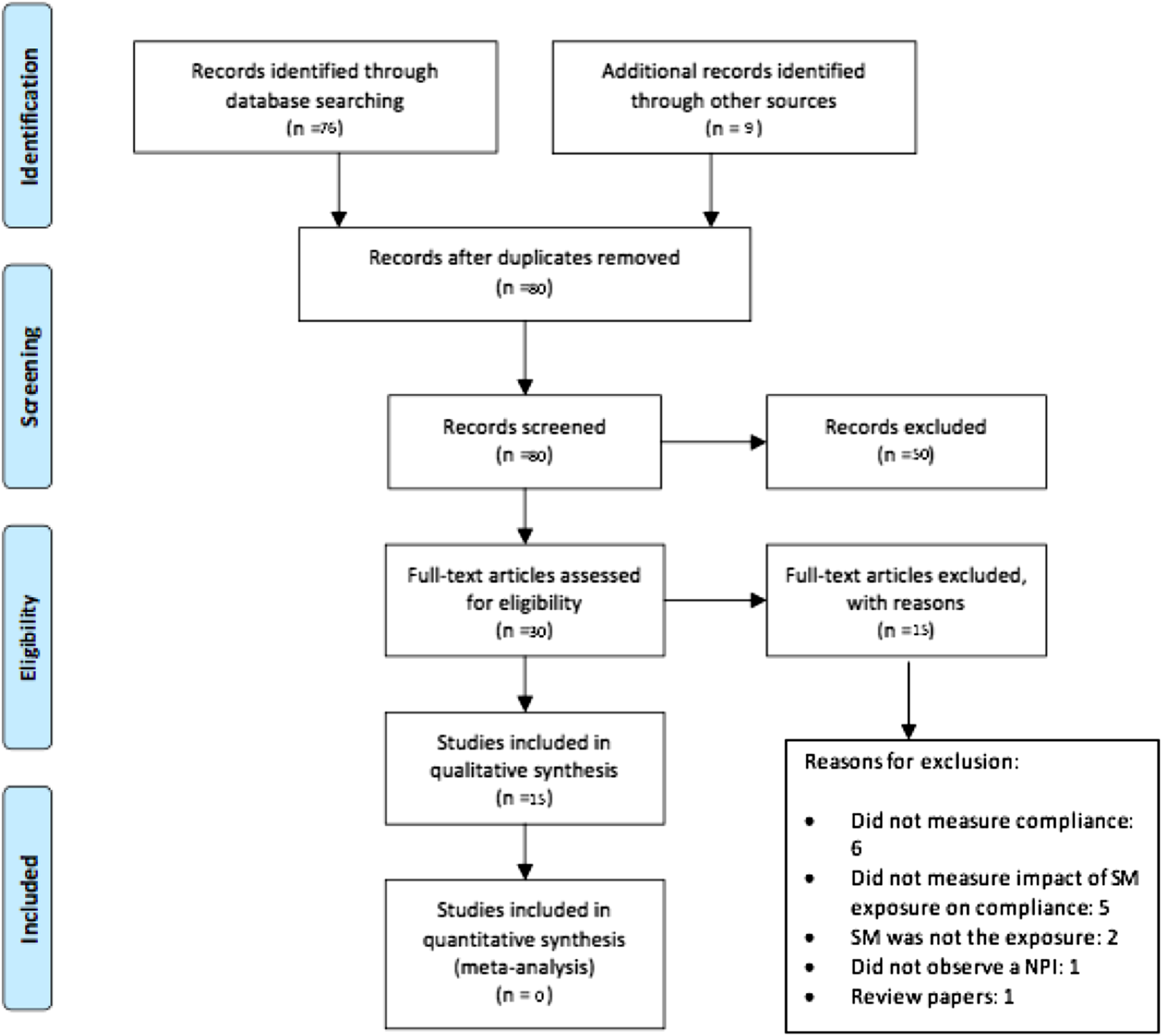
Data Reduction and Analysis
A data extraction form, adapted from the Cochrane data extraction form for RCTs and non-randomised studies (The Cochrane Collaboration, 2021), was designed to extract data relevant to the research question. Data regarding the participant characteristics, study characteristics and outcome measurements were collected.
Quality assessment was conducted after data extraction, using the Joanna Briggs Institute (JBI) checklist for analytical cross-sectional studies (JBI, 2020). Poor quality studies were not excluded from the analysis, to avoid limiting the available evidence (Boland et al. 2017).
Tables were used to present and synthesise the extracted data (Stroup et al., 2009), with narrative analysis used for qualitative synthesis of the findings (Popay et al., 2006).
A meta-analysis was not considered appropriate due to the large degree of heterogeneity between the research designs, in order to avoid the production of misleading evidence (Ioannidis et al., 2008).
Results
Results from the search, screening and selection process are presented in Figure 1. A total of 84 records were reviewed, 76 of which were identified through the database searches, and nine were identified through the hand search. Following the removal of four duplicates, the titles and abstracts of 80 studies were screened for relevance, of which 50 failed to meet the inclusion criteria and were excluded. Eligibility selection was conducted on 30 studies, with 15 excluded. A total of 15 studies were deemed to meet the inclusion criteria, and were included in the qualitative synthesis.
Study Characteristics
The study characteristics.
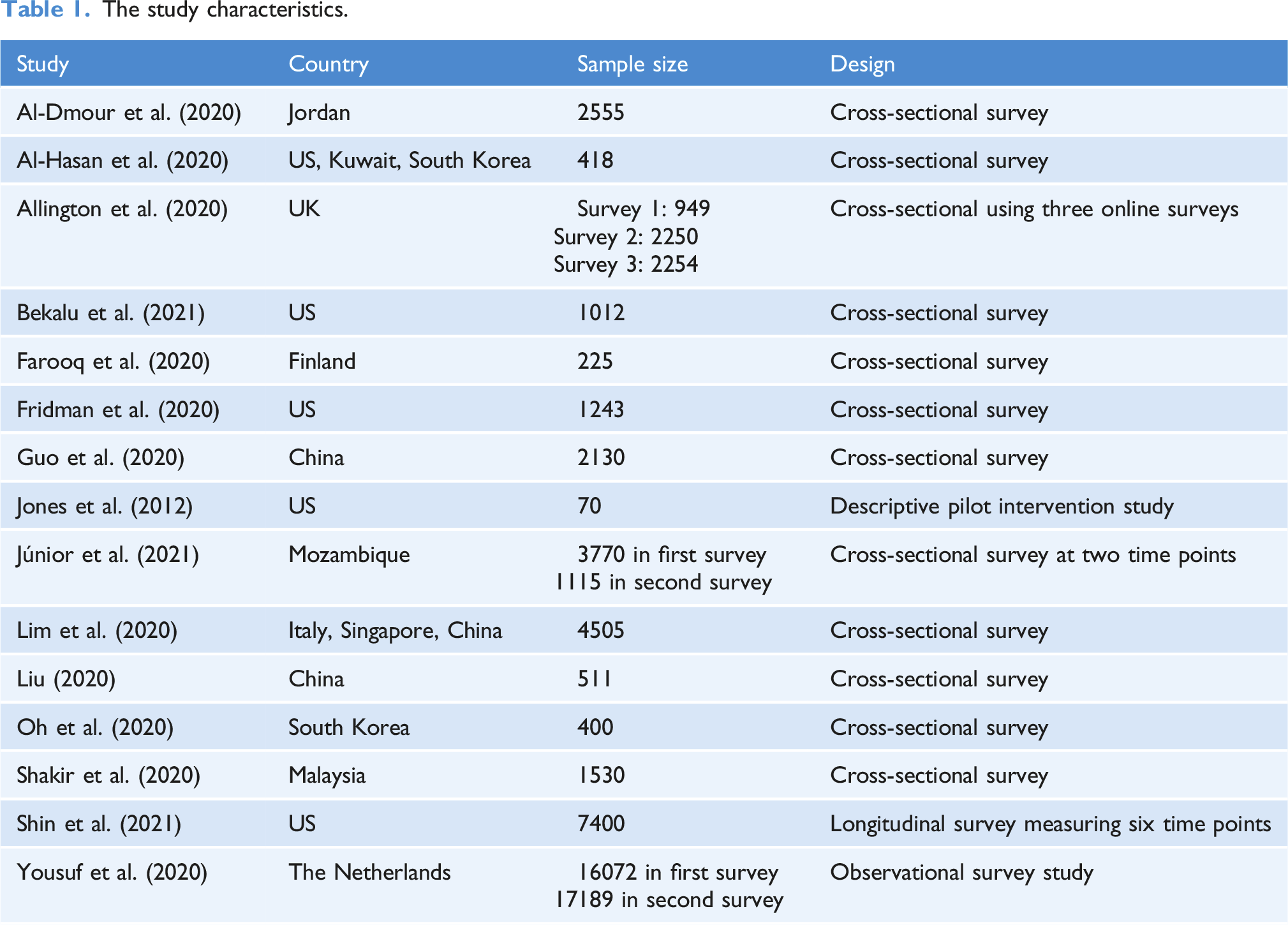
The 15 included studies were observational in design, with 80% (n = 12) using cross-sectional methods. Two studies: Junior et al. (2021), and Shin et al. (2021), measured the effects of social media on compliance with IPC measures at multiple time points, while the remaining 13 studies measured a single time point. 93.3% of the studies were published between 2020 and 2021.
A large degree of heterogeneity in sample sizes was observed, ranging from 17,189 (Yousuf et al., 2020), to 70 (Jones et al., 2012).
80% of the studies investigated the impact of social media exposure on public adherence to preventative behaviours during the COVID-19 pandemic. Most studies took place in high income countries, with one third conducted in the US. The samples of only two studies were selected from multiple countries (Al-Hasan et al., 2020; Lim et al., 2020).
All the studies were conducted online, and utilised self-report measures.
Participant Characteristics
Most study participants were adults (Al-Dmour et al., 2020; Al-Hasan et al., 2020; Farooq et al., 2020; Fridman et al., 2020; Jones et al., 2012), and when mean ages were reported, these ranged from 21.8 (Shakir, 2020), to 48.553 (Shin et al. 2021).
There were both male and females included in each study, with a slightly higher proportion tending to be female.
Where additional demographic information was reported, a high level of education was the most frequently reported characteristic.
As not all studies reported the demographic information of their sample, the population of this systematic review cannot be characterised.
Findings
The study findings.
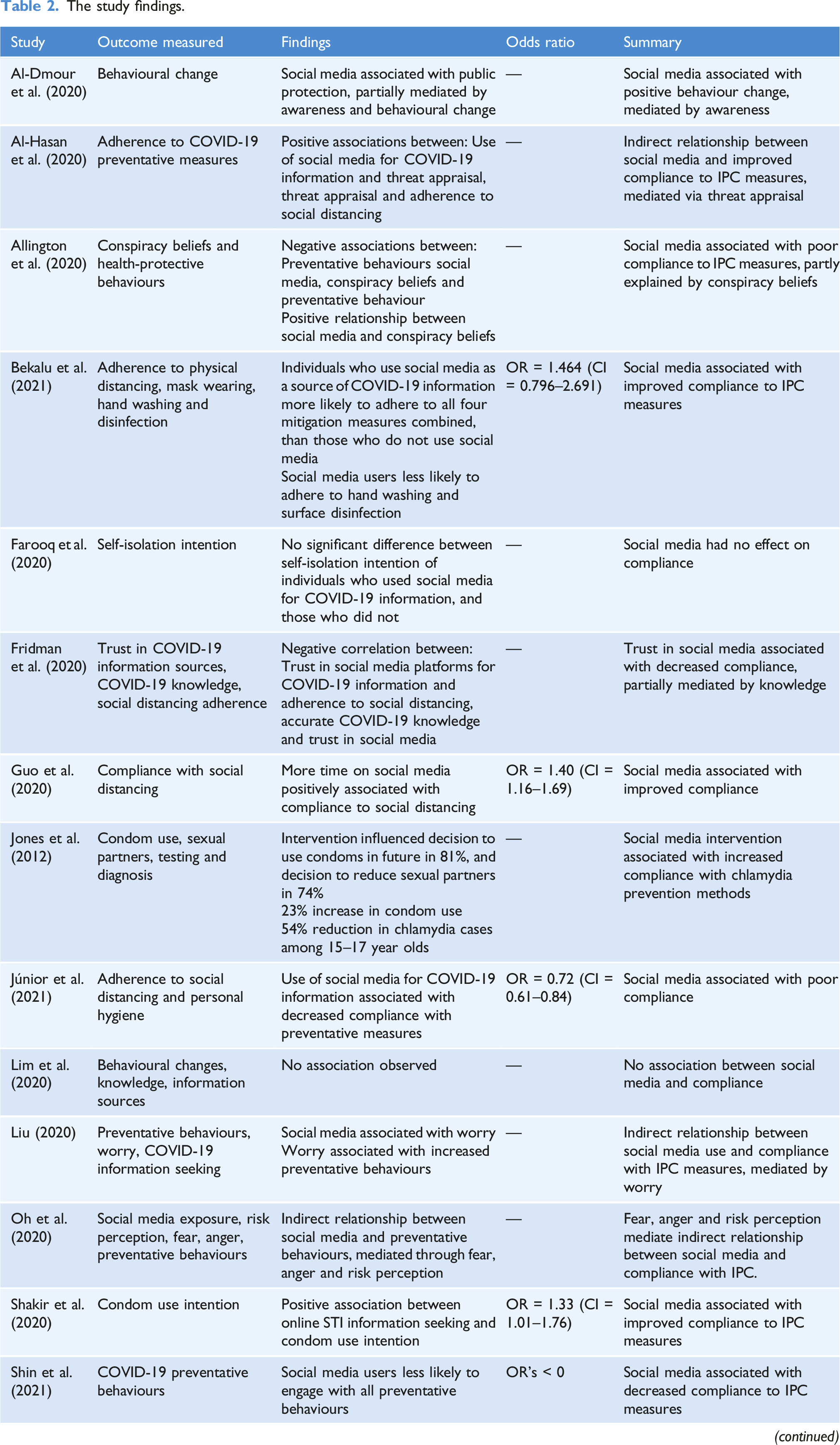
86.6% of studies measured adherence to COVID-19 preventative measures, including: social distancing, mask wearing, hand washing and surface disinfection. While some studies measured adherence to multiple COVID-19 prevention methods, others focused only on social distancing measures. Only 13.3% of studies (n = 2) measured adherence to IPC measures aimed at preventing infections other than the respiratory viruses COVID-19 and MERS.
The majority (60%) of studies identified that social media use was associated with increased compliance with IPC measures (Al-Dmour et al., 2020; Al-Hasan et al., 2020; Bekalu et al., 2021; Guo et al., 2020; Jones et al., 2012; Liu, 2020; Oh et al., 2020; Shakir et al., 2020; Yousuf et al., 2020). However, some of these studies identified the relationship to be indirect; influenced by other variables.
Conversely, 26.7% of studies (n = 4) identified a negative correlation between social media and compliance with IPC measures, suggesting that individuals who used social media were more likely to demonstrate poor compliance with recommended IPC measures (Allington et al., 2020; Fridman et al., 2020; Júnior et al., 2021; Shin et al. 2021). Two studies observed no correlation between social media and compliance with IPC (Farooq et al., 2020; Lim et al., 2020).
40% (n = 6) of studies observed the presence of variables that mediated the relationship between social media exposure and compliance with IPC measures. These findings were heterogeneous and included variables such as: awareness (Al-Dmour et al., 2020), threat appraisal (Al-Hasan et al., 2020), worry (Liu et al., 2020), conspiracy beliefs (Allington et al., 2020), fear, anger and risk perception (Oh et al. 2020). Conspiracy beliefs (Allington et al., 2020), and knowledge (Fridman et al., 2020) mediated a negative relationship between social media use and compliance with IPC measures, while the remaining factors mediated a positive correlation.
Although the use of odds ratios (OR) were the most frequently reported outcome measurement, they were only reported in 40% of the studies. The odds ratios reported were: 1.46 (Bekalu et al., 2021), 1.40 (Guo et al., 2020), 0.72 (Júnior et al., 2021) and 1.33 (Shakir et al., 2020). Of the studies that reported confidence intervals (Bekalu et al., 2021; Guo et al., 2020; Júnior et al., 2021; Shakir et al., 2020), only 25% (n = 1) crossed the line of no effect (Bekalu et al., 2021).
Quality Assessment
Quality assessment.
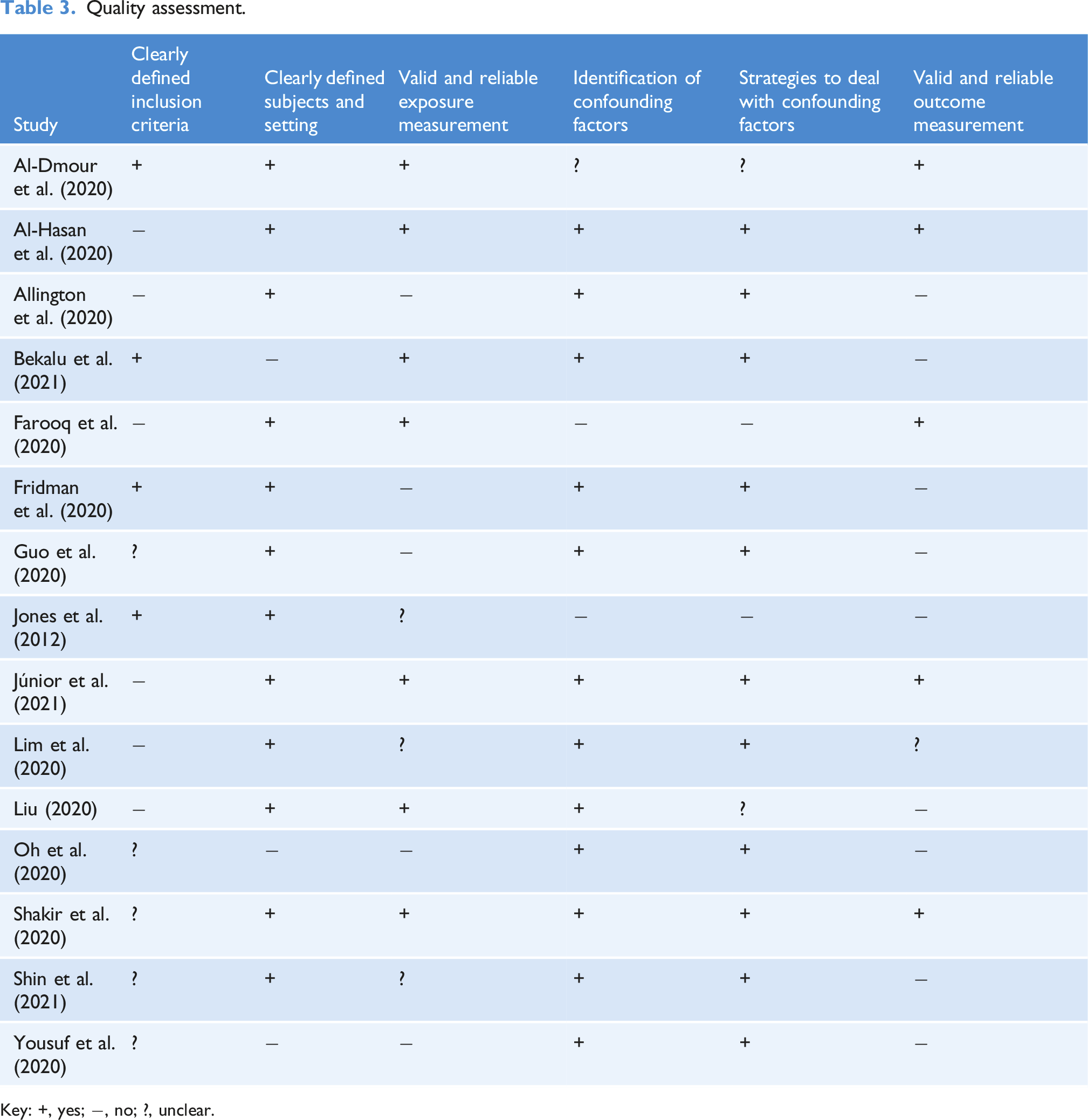
Key: +, yes;
The cross-sectional nature of the systematic review introduces an inherent risk of bias (Wang and Cheng, 2020), with self-report measures prone to recall and social desirability bias (Althubaiti, 2016). All the studies utilised self-report measures, those that were classified as ‘yes’ under the ‘valid and reliable measurement of exposure’ and ‘valid and reliable measurement of outcomes’ criteria, used pre-validated tools (Althubaiti, 2016). One third of the studies (n = 5) were classed as ‘yes’ under both criteria (Al-Dmour et al., 2020; Al-Hasan et al., 2020; Farooq et al., 2020; Júnior et al., 2021; Shakir et al., 2020).
Selection bias was frequently observed within the studies. Due to the online nature of the studies, older people, with less access to these platforms, are not represented (Guo et al., 2020). Many of the studies used non-probability sampling methods, prone to selection bias, for example: convenience sampling (Jones et al., 2012), snowball sampling (Júnior et al., 2021), purposive sampling (Guo et al., 2020) and self-selection (Al-Dmour et al., 2020).
The studies classed as having the highest risk of bias were Jones et al. (2012), Oh et al. (2020) and Yousuf et al. (2020), due to having the greatest number of criteria scored as ‘no’ or ‘unclear’. The 2020 study by Yousuf et al. was considered at particular risk of bias, due to using different study groups for the baseline and post-campaign surveys.
The studies that scored ‘yes’ on each of the JBI criteria were judged as having the lowest risk of bias, and included: Júnior et al. (2021) and Shakir et al. (2020).
Discussion
The majority of studies (60%) observed a positive correlation between the use of social media, and compliance with IPC measures. This suggests that social media is associated with a good level of public compliance with preventative behaviours, and has a role in encouraging behaviour change and adherence to public health recommendations. This finding is consistent with a systematic review by Laranjo et al. (2015), who identified that while, social media was an effective platform to encourage health behaviour change, it only produced a slight positive effect.
The positive association between social media and increased public compliance with IPC measures may be due to the social support that is prevalent on social media platforms. Centola (2013) suggests that social influences are paramount in health behaviour change, highlighting the collective dynamic within health behaviour, and the notion that individuals are more likely to adopt a health behaviour if peers have. Investigating the behavioural change techniques utilised in social media-delivered health behaviour change interventions, Simeon et al. (2020) reports social support was the most frequently identified behavioural change technique, recommending further research into behaviour change methods to identify how they could be incorporated into future social media-based health interventions.
Concurrent with Laranjo et al.’s (2015) systematic review, there was a large degree of heterogeneity between the findings, with 60% identifying a positive association, and 40% identifying a negative, or no, association. The heterogeneous findings were likely due to the methodological diversity between the studies (Sandercock, 2011).
The study samples comprised of mainly young people. This was also observed by Moorhead et al. (2013), in a systematic review of the use of social media for health communication. Fridman et al. (2020) identified younger populations to be more trusting of the information on social media platforms than older populations. Thus, as adherence to social distancing was observed to be lower in individuals who trusted social media, the results of this systematic review cannot be generalised without data regarding the influence of social media on compliance in older adults (Fridman et al., 2020).
Mediating Factors
Various mediating factors were identified between social media and compliance with IPC measures, including: awareness (Al-Dmour et al., 2020), worry (Liu et al., 2020) and conspiracy beliefs (Allington et al., 2020). It is therefore important that these variables are taken into account when designing public health messages. This is supported by Oh et al. (2020), who suggests public health communicators and policy makers take public emotions into account, in order to design effective communication strategies. There is, however, an ethical argument surrounding the notion of exploiting public emotions to promote compliance, particularly when negative emotions are in play, such as worry.
Negative Impacts of Social Media
Despite 60% of studies identifying a positive association between social media use and compliance with IPC measures, social media is also associated with poor compliance with IPC measures (Ölcer2020). Of the studies identified, 26.7% observed a negative association. This may be explained by infodemics – the rapid circulation of conflicting information on social media, creating uncertainty (WHO, 2021). Misleading advice on social media can clash with accurate advice, discouraging individuals to comply with recommendations (Ölcer et al., 2020). This presents a public health risk (Shin et al., 2021), particularly in the context of the COVID-19 pandemic, which saw vast amounts of misinformation circulated via social media (Atehortua and Patino, 2021).
Multiple studies have identified social media to be associated with misconceptions regarding public health advice, particularly conspiracy beliefs, which result in low compliance with IPC measures (Allington et al., 2020; Hammad et al., 2021). Social media sites, however, have started to provide links to credible information sources and warnings on information that may not be accurate, with the aim of combatting the spread of misinformation (Hammad et al., 2021).
Echo chambers, defined as the sharing of information between likeminded followers (Malecki, Keating and Safdar, 2021), are a feature of social media platforms that can have both positive and negative effects. Public health risks present when echo chambers are responsible for propagation of misinformation, however they can provide benefits when used for the dissemination of accurate information and advice (Malecki, Keating and Safdar, 2021). Therefore, there is potential to exploit them in this way, through the sharing of evidence-based information to neutralise misinformation (Atehortua and Patino, 2021).
Risk of Bias
The methodological diversity between the studies included in this systematic review imposed a risk of bias on the results. One consistent feature in the methodological design of the studies was the use of self-report measures. These, however, have an inherent risk of bias. Additionally, all of the studies were conducted via the internet with the majority of studies conducted during the COVID-19 pandemic, this is likely to be largely due to guidelines and feasibility during the pandemic (Hlatschwako et al., 2021). Despite the diverse and widespread utilisation of the internet and social media, selection bias remains a significant risk in online survey research, which negatively impacts the external validity of a study (Hlatschwako et al., 2021).
One third of the studies were considered to have used valid and reliable measurements of the exposure and outcomes, as a result of using pre-validated, tools. However, the remainder of the studies used non-validated surveys and scales. This may be due time constraints during the COVID-19 pandemic, particularly for those that aimed to assess behaviour early in the pandemic (De Man et al., 2021).
Impact of the COVID-19 Pandemic
Farooq et al. (2020) highlight a lack of understanding of the impact of social media-based information on behaviour during pandemics. As 80% of the studies were conducted during the COVID-19 pandemic, this systematic review has contributed to the literature gap.
Social media was widely used throughout the pandemic, both for health seeking purposes, and general usage (Anwar et al., 2020). Not only did the COVID-19 pandemic alter the way information is shared, with an increase in real-time sharing, it also shifted the perspective of global health away from traditional viewpoints, with online methods of health communication and surveillance dominating (Wang et al., 2020). The use of social media during the COVID-19 pandemic has demonstrated the need to observe messages shared on social media more closely, in order to understand knowledge gaps of users, and tailor communication messages to address them (Igoe, 2020). This may help to increase public adherence to recommendations in the future.
Implications
As most of the literature sampled young people, it can be inferred that the positive correlation between social media and compliance with IPC measures is particularly prevalent in this age group. Therefore, communicating the importance of compliance with IPC measures via social media may encourage informed behaviour change in young people, and reduce the transmission of infection throughout the population (Basch et al., 2021).
Social media can also be effective in increasing accessibility to health information; helping to reach marginalised populations, with the potential to aid the reduction of health inequalities (Moorhead et al., 2013). The diverse reach of social media platforms has been highlighted by Fridman et al. (2020), who suggested social media may be a promising tool to engage hard to reach populations.
Recommendations
Response to the COVID-19 pandemic illustrated the role of social media when disseminating crucial health information to the public. 60% of the studies reviewed identified a positive correlation between social media exposure and adherence to IPC measures. Results suggest social media should be recommended as a platform for health communication, particularly to address young people. Social media platforms are widely used by the public on a daily basis, therefore social media-based health communication can be integrated into everyday life, cost-effectively (Xin et al., 2020). As there was a weak positive association between social media and compliance with IPC measures, further, high quality research into the phenomenon is required.
Limitations
Due to the nature of the research question, there was a paucity of papers with high quality research designs. However, as these papers met the inclusion criteria, they were included in the review.
Conclusion
The identification of a positive association suggests that social media should be utilised in future public health communication strategies, to increase public compliance with public health recommendations and guidelines. Public health communicators and policymakers should take advantage of the social support that exists on social media when designing future communication strategies. In addition, it is suggested that social media is used by public health authorities to disseminate accurate, evidence-based information, whilst neutralising circulating misinformation that can lessen the impact of public health guidelines.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.