
Abstract
Background:
The experience of “flow” at work correlates with positive job outputs and work-related attitudes. Very little current literature describes flow at work in physicians, who experience significant barriers to optimal work outputs, also known as flow thieves (e.g., case interruptions, documenting care). This study aimed to develop a measurement for physician flow (P-Flow) at work and examine the association of P-Flow with physician burnout, job satisfaction, and well-being.
Methods:
A pilot instrument was tested with items measuring P-Flow at work. After the pilot administration, a 14-item physician flow (P-Flow-14) scale was administered to physicians. In addition to the P-Flow-14 scale, physician respondents completed items measuring burnout, job satisfaction, and well-being.
Results:
This study specifies initial psychometric evidence of P-Flow-14 and 7-item P-Flow instruments for researchers interested in studying flow at work in physicians. For each P-Flow instrument, higher levels of the flow experience correlated with superior levels of well-being (p < .01) and job satisfaction (p < .01), and less burnout (p < .001). Results showed initial psychometric evidence of derived subscales (work absorption, clinical flow, flow thieves, work fulfillment) for application in future research. Results showed associations between flow experience by age group and physician specialty.
Conclusions/Application to Practice:
To enhance well-being and job satisfaction, physicians should aim for concentration and immersion in clinical duties while reducing unnecessary distractions. These findings can be applied by employers and can guide further research on work interruptions and patient safety. Future research can validate the P-Flow scales and subscales to assess interventions aimed to improve the physician work environment.
Background
Flow represents a state of consciousness in which an individual intrinsically enjoys and is fully immersed in an activity (Bakker, 2008). As a result of this absorption, individuals feel engrossed in the activity and strive for this peak experience (Bakker, 2008; Moneta, 2017). Flow theory establishes that individuals in this state achieve superior levels of well-being and personal growth (Gu et al., 2020). Researchers and employers seek to study and facilitate flow in workplace environments due to its linkage with positive work-related attitudes and job performance (Peifer et al., 2020).
Bakker developed the WOrk-reLated Flow (WOLF) Inventory to measure flow in the workplace, characterized by three dimensions: absorption, work enjoyment, and work motivation (Bakker, 2008). In absorption, individuals immersed in a task may forget about everything else around them including personal life obligations (Bakker, 2008). Work enjoyment results in individuals reflecting positively about their job, and motivation refers to the inherent drive to perform their professional duties (Bakker, 2008).
Peifer et al. described unfinished work tasks as “thieves of flow,” explaining how these thieves result in negative mental health in employees (Peifer et al., 2020). Physicians have numerous thieves of flow as they aim for quality patient care while balancing numerous work duties. Documented hindrances to physician work flow (e.g., interruptions, patient documenting requirements) may lead to inferior job satisfaction or poor mental health outcomes such as burnout. Physicians experience distressing levels of burnout and career dissatisfaction, which may lead to reduced job proficiency (Li-Sauerwine et al., 2020). Recognized sources of burnout among physicians include chaotic work environments, cumbersome electronic medical records (EMR) duties, and other work pressures (DeChant et al., 2019). Dissatisfaction with quality of life and work–life balance in physicians necessitates research into interventions to elevate physician wellness (West et al., 2014). Interventions to improve efficiency and satisfaction often target the EMR (scribes, medical assistants) to reduce clinical burdens and improve physician well-being (DeChant et al., 2019).
This study aimed to develop a method to measure physician flow (P-Flow) at work and determine associations with other psychological constructs commonly measured in physicians. After developing and piloting instruments to measure P-Flow at work, we determined whether higher levels of P-Flow at work correlated with superior job satisfaction, well-being, and burnout. No known study has examined P-Flow at work through developed measures, specifically to examine clinical work flow, or made associations between flow at work and burnout and well-being.
Methods
Sample and Instruments
After approval by the University of Louisville’s Institutional Review Board (IRB), the authors generated survey items reflecting the current literature on both the experiential state of flow at work and the items described as negatively impacting physician clinical flow. The two authors shared the draft instrument with physicians for feedback and administered a pilot instrument.
The pilot instrument was sent to all physicians at the University of Louisville. The data from the pilot survey were then utilized to determine which items to keep, which items to remove, and which items to modify to optimize the instrument. In determining items to keep, the authors examined item statistics and considered survey fatigue.
The second iteration of the instrument was shared via listservs, networking emails, and utilization of university email contacts. Physicians were informed to complete if they had not taken the survey in the first iteration. In addition to completing the P-Flow at work instrument developed by the authors, this second group of respondents also completed a shortened Maslach Burnout Inventory, a two-question inventory (Li-Sauerwine et al., 2020), a single-item global measure of job satisfaction (Williamson et al., 2018), the World Health Organization–5 (WHO-5) questionnaire to measure well-being (Topp et al., 2015), and the WOLF Inventory (Bakker, 2008).
Data Collection and Analysis
Data were collected via a secure, encrypted database called REDCap™. Cronbach’s α and item statistics were used to evaluate the scales and subscales developed to measure P-Flow. Two scales are presented based on data analysis and literature on flow and hindrances to P-Flow for future testing. Factor analysis (FA) was utilized to examine construct validity; principal axis factoring was used with Promax rotation. Factors were retained if eigenvalues were greater than 1. Factor loadings (and cross-loadings) were examined and classified based on data and underlying meaning of the items grouped. Pearson correlations were conducted between the newly developed P-Flow scales and the WOLF Inventory to determine concurrent validity. Pearson correlations were utilized to examine associations between the P-Flow scales and subscales measuring burnout, job satisfaction, and well-being.
Linear regressions were conducted to determine associations among gender identity, age group, training level (resident or fellow vs. attending), and specialty group with flow scores; for these, we included specialties with at least 10 subjects and also created a surgical field group which consisted of orthopedics, cardiovascular and thoracic surgery, obstetrics and gynecology (OB-GYN), neurological surgery, ophthalmology and visual sciences, otolaryngology head and neck surgery, and surgery (general). We report regression coefficients with 95% confidence intervals (CIs). Statistical significance was set at p <.05. IBM SPSS Version 27 Statistics was used for data analysis.
Results
Pilot Survey
A total of 185 physicians completed the initial survey of 27 questions to be considered for the P-Flow instrument. The 27 items yielded a Cronbach’s α level of .908. Factor analysis results indicated the 27 items resulted in a five-factor solution with 67.3% of the total variance explained. Due to survey fatigue and some items loading on to multiple factors (cross-loadings), the instrument was modified and shortened prior to the full survey administration.
Study Sample Characteristics
The P-Flow at work survey consisted of 14 items (Appendix A - See Supplemental Information). This survey was completed by 140 physicians. One-hundred sixteen (82.9%) respondents were White. Most respondents (56.4%) identified as male and practiced at an attending level (70.7%). Age groups included the following: 18–29 (N = 22), 30–39 (N = 41), 40–49 (N = 33), and 50+ years (N = 41); three subjects had an unknown age or chose not to answer. Physicians comprised multiple disciplines, with highest representation from emergency medicine (EM; 32.1%), pediatrics (22.1%), and internal medicine (IM; 14.3%). Other disciplines with representation included: anesthesiology, cardiovascular and thoracic surgery, dermatology, family medicine, neurology, neurological surgery, OB-GYN, ophthalmology, orthopedics, otolaryngology, psychiatry, radiation oncology, and surgery.
Reliability and Validity of P-Flow Scales
Based on theory and data analysis, the investigators derived two scales suitable for interpretation, decision-making, and future research consideration: a 14-item physician flow (P-Flow-14) scale and a 7-item physician flow (P-Flow-7) scale.
P-Flow-14 scale
The P-Flow-14 scale (Appendix A - See Supplemental Information) revealed a Cronbach’s α of .88. Principal axis factoring with a Promax rotation revealed four factors had eigenvalues >1. The first factor (eigenvalue = 5.8) contained four items related to work fulfillment. The second factor (eigenvalue = 2.4) contained four items related to clinical flow duties. The third factor (eigenvalue = 1.4) contained three items related to work absorption. The final factor (eigenvalue = 1.1) contained three items related to thieves of flow. The four-factor solution accounted for 75.9% of the total variance explained.
P-Flow-7 scale
The P-Flow-7 scale (Appendix B - See Supplemental Information) revealed a Cronbach’s α of .84. Principal axis factoring with a Promax rotation revealed two factors had eigenvalues >1. The first factor (eigenvalue = 3.7) contained four items related with clinical flow. The second factor (eigenvalue = 1.3) contained four items related to work absorption duties. The two-factor solution accounted for 71.9% of the total variance explained.
Associating Newly Piloted P-Flow Scales With WOLF Inventory
To examine concurrent validity, scores were compared among the P-Flow-14 and P-Flow-7 scales with the WOLF Inventory. Results showed statistically significant associations between the WOLF Inventory and the P-Flow-14 (r =.840, p < .001) and the P-Flow-7 (r = .583, p < .001) scales.
Examining P-Flow With Burnout, Well-Being, and Job Satisfaction
Pearson correlations were conducted among the full P-Flow scales and each of the subscales with the two-item burnout, global job satisfaction item, and five-item WHO Well-Being Index results (Table 1). Cronbach’s α for the two-item burnout was .77. Cronbach’s α for the WHO-5 Well-Being Index was .89. Each of the P-Flow scale results was significantly associated with the two-item burnout measure, job satisfaction, and well-being scores. Higher levels of P-Flow at work correlated with lower levels of burnout and higher levels of job satisfaction and well-being (Table 1).
Pearson Correlations: Physician Flow With Burnout, Job Satisfaction, and Well-Being (n = 140)
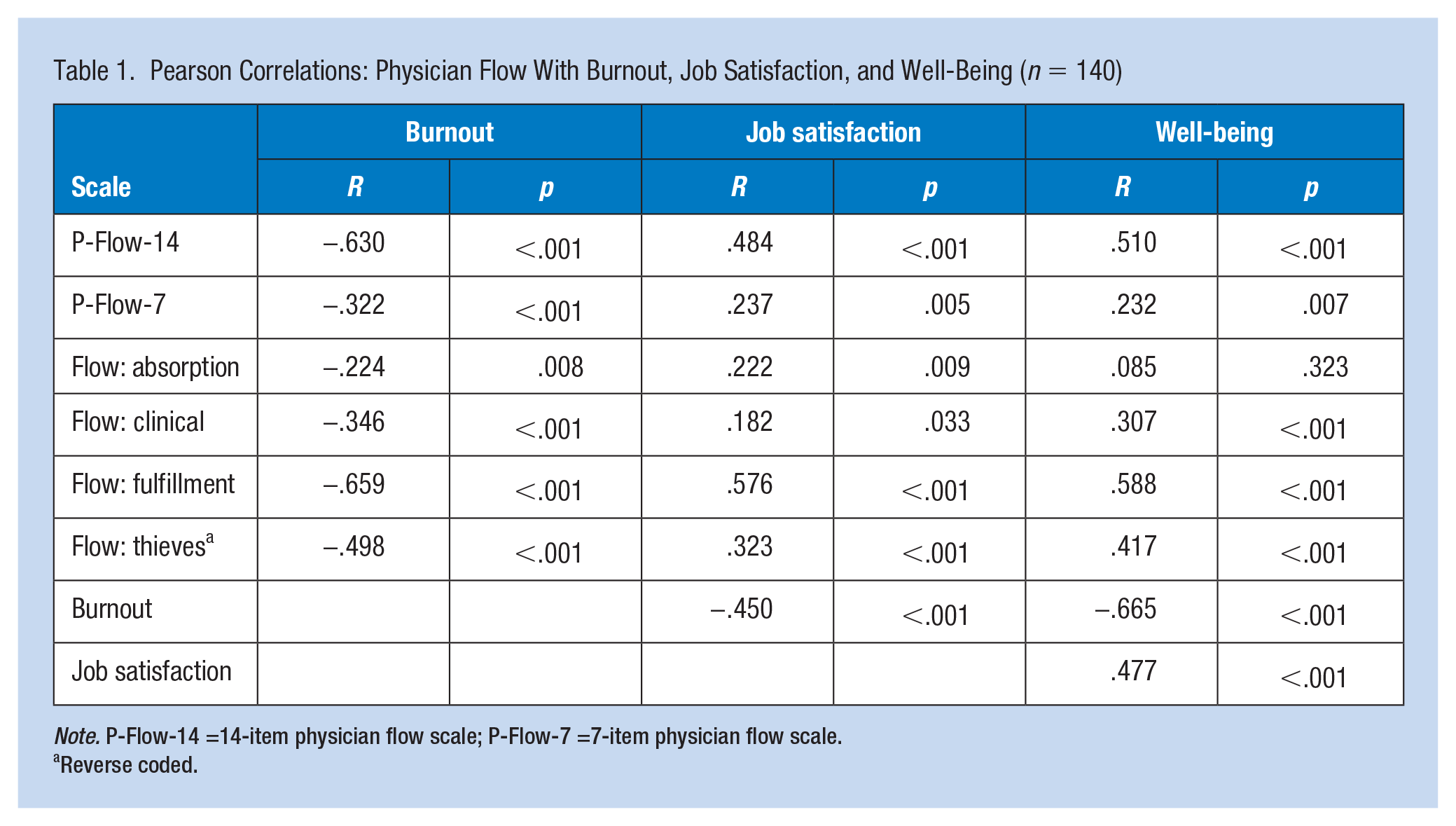
Note. P-Flow-14 =14-item physician flow scale; P-Flow-7 =7-item physician flow scale.
Reverse coded.
Gender Identity, Age Group, Physician’s Experience Level, and Specialty Differences
Group scores showed females had higher scores than males on the P-Flow-14 scale. Individuals in the 30–39 age group had the lowest scores on both the P-Flow-14 and the P-Flow-7 scales. Residents had higher scores on the P-Flow-14 scale but lower scores on the P-Flow-7 scale. Physicians employed in a surgical field had the highest scores on the P-Flow instruments, whereas pediatric physicians had the lowest P-Flow scores (Table 2).
Physician Flow Score Group Differences
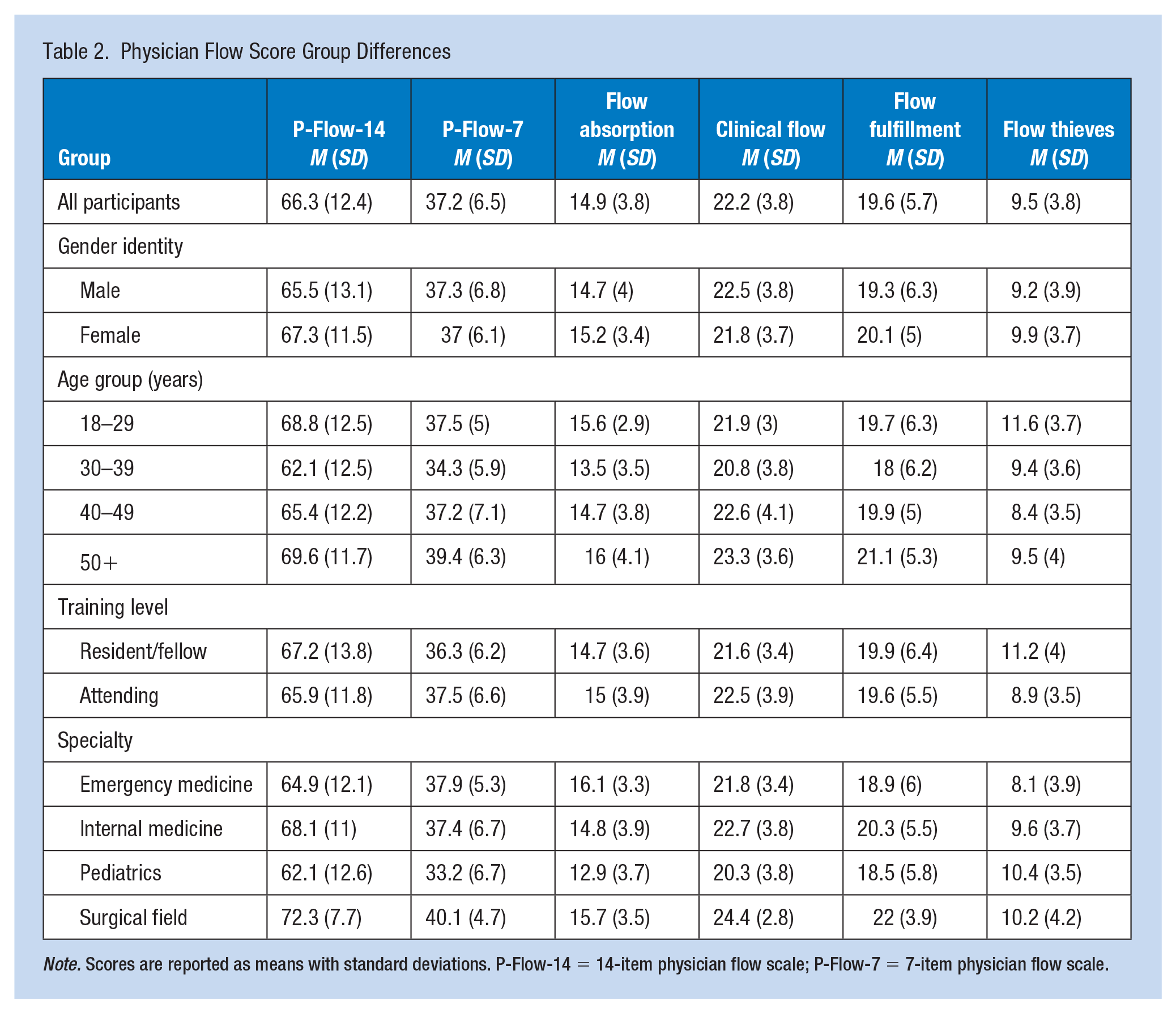
Note. Scores are reported as means with standard deviations. P-Flow-14 = 14-item physician flow scale; P-Flow-7 = 7-item physician flow scale.
Linear regression outputs (Table 3) revealed, after adjusting for gender identity, other age groups, training level, and specialty fields, individuals aged 30 to 39 years had significantly lower scores on the P-Flow-14 and P-Flow-7 scales. Older age groups had higher scores on flow absorption and flow fulfillment. In addition, after controlling for other variables, pediatric physicians had significantly lower P-Flow-14, P-Flow-7, flow absorption, and clinical flow scores. Finally, the variable found to be a significant predictor of flow thieves was practicing in EM; EM physicians experienced higher rates of flow thieves and worse levels of clinical flow after adjusting for other variables.
Regression Outputs
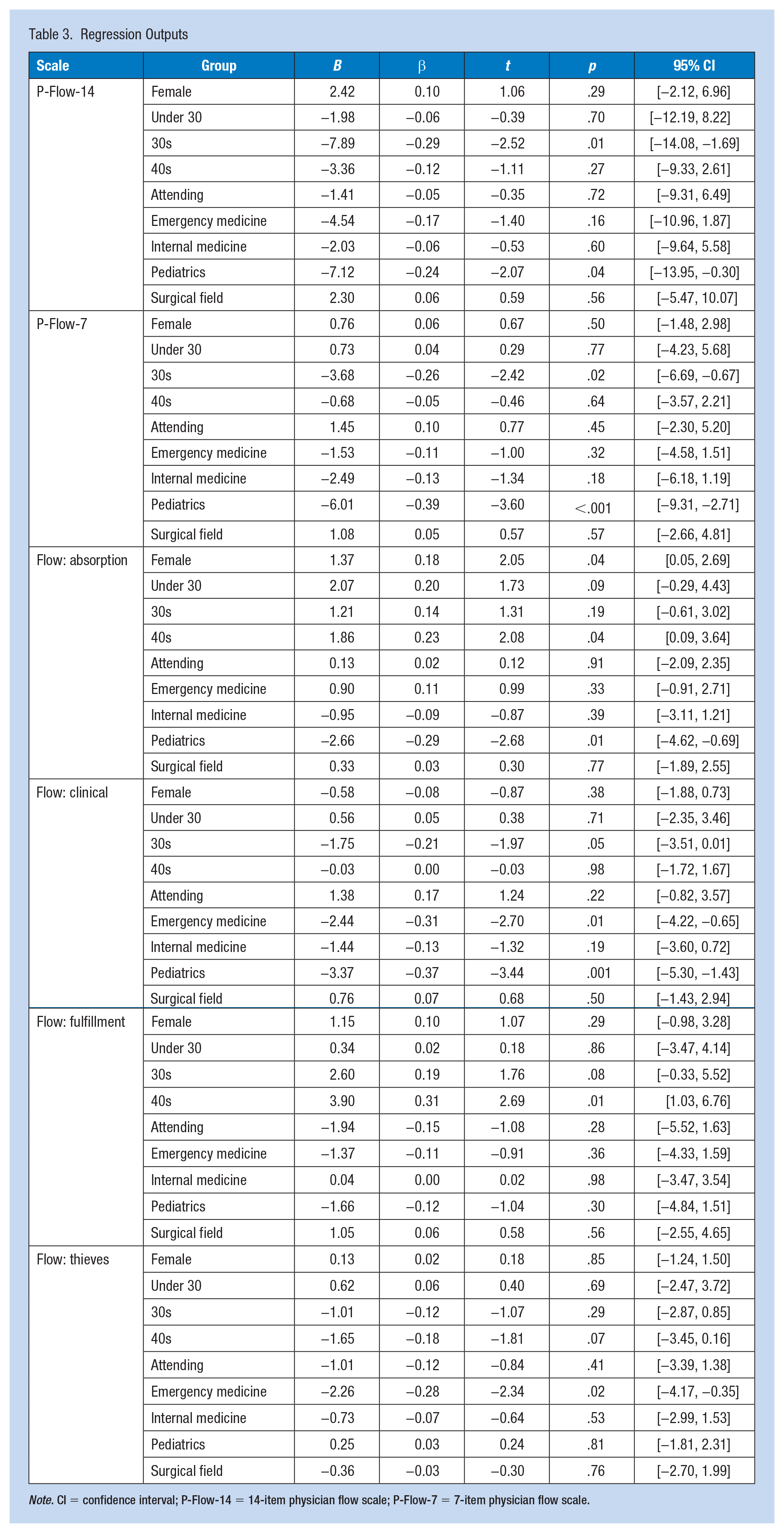
Note. CI = confidence interval; P-Flow-14 = 14-item physician flow scale; P-Flow-7 = 7-item physician flow scale.
Discussion
This work provides novel insight into the coveted experience of flow at work, a work outcome underappreciated in physicians. Higher levels of the flow experience correlated with superior levels of well-being and job satisfaction, and lower burnout. In addition to the full scales of P-Flow at work, the subscales (work absorption, clinical flow, flow thieves, work fulfillment) could have roles in future research connecting psychological concepts in healthcare professionals or quantifying effects of interventions aimed to improve the workplace.
The P-Flow-14 scale specifies P-Flow thief items including interruptions, insufficient resources, and EMR inefficiencies; these hindrances may inhibit a physician from successfully completing tasks in a timely manner. Task-switching as a result of flow thieves (e.g., interruptions) distracts physicians from the original task, leading to cognitive depletion and inefficient care (Skaugset et al., 2016). Disturbances to flow, particularly low-priority or irrelevant demands, lead to inferior quality of care provided (Blocker et al., 2017). Well-documented in physicians, interruptions hinder flow and risk harm to patients (Skaugset et al., 2016). Another potential flow thief is deprivation of quality and quantity of sleep. Research has demonstrated negative effects of sleep deprivation on flow (including immersion; Kaida & Niki, 2014). With the known importance of optimal sleep hygiene in physicians (Ferguson et al., 2019), future work could examine the interaction of P-Flow with sleep.
Academic physicians experience various disruptions that hinder important non-patient care responsibilities such as instructing/training residents during rounds (Armendariz et al., 2021). Skaugset et al. (2016) studied task-switching in EM, providing recommendations to counter flow deterrents: decrease external interruptions, recognize the impact of these interruptions, use appropriate technology to help achieve task completion, and implement sufficient work flow methodologies.
While P-Flow results did not differ by gender identity, differences emerged based on age group. Subjects in their 30s had lower levels of flow than those more experienced. Potential mechanisms include the learning curve of early clinical practice along with increased pressure and responsibilities that lessen with acquired expertise. However, residents/fellows did not significantly differ in scores compared with attendings. This difference in P-Flow by age contrasts with other work that has shown no impact of age on experience of flow (Bonaiuto et al., 2016).
In this study, pediatricians had the worst flow scores. A 2014 study examined hospital pediatricians and found on average that physicians were interrupted 4.7 times per hour; these interruptions included colleague and nursing staff interruptions as well as telephone/beeper calls (Weigl et al., 2014). Interestingly, in this study the pediatrician respondents reported lower incidence of flow thieves.
Another specialty our study found to have inferior flow experiences was EM, specifically experiencing significantly worse levels of flow thieves. Emergency medicine physicians experience interruptions at a rate 3 times more than primary care providers (Blocker et al., 2017). Interruptions in the emergency department may be necessary due to the nature of the specialty and diverse patient presentations. However, unnecessary or nonurgent interruptions hinder work flow and may increase physician stress and errors (Ratwani et al., 2017). Work flow quality improvement projects often require very little cost. In one example, the ubiquitous requests for electrocardiogram (ECG) review by EM physicians could be completed in batches or with a more integrated approach (Ioannides et al., 2021). Implementation of departmental/hospital policies that limit flow thieves may enhance physician absorption, resulting in improved physician well-being and superior patient care.
The P-Flow scales are grounded in constructs to help physicians flourish. Implementing measurements of optimal P-Flow at work, versus utilizing negative measures such as burnout, could help elucidate new understanding of how to measure physician well-being (Sikora et al., 2020). The flow instruments examine a critical aspect of physician wellness –efficiency of practice – which focuses on development of a workplace culture that enhances systems and practices to allow providers to successfully engage in patient care (Bingemann & Laubach, 2021). As a positive adversary of burnout, work engagement consists of physicians feeling absorption in their work (Shanafelt & Noseworthy, 2017). Some criticism of the WOLF Inventory includes whether the scale should include both intrinsic motivation and enjoyment (due to overlap; Happell et al., 2015). In response to this concern, the P-Flow instruments target specific items relevant to the clinical setting while also considering overlap in constructs to provide multiple options for future psychometric or exploratory studies.
Limitations
Rather than comprehensive assessments, the P-Flow scales represent succinct, easily deployable instruments. This study did not consider sufficient power/sample size prior to administering the survey. Cognizant of survey fatigue, we considered the increasing knowledge and unique wellness concepts and workplace efficiencies within physicians. The study would benefit from validation in larger, more diverse (our sample was mainly White) samples, ideally with psychometric testing of the instruments. While the sample had representation from numerous disciplines and we were able to make comparisons across some specialties, future work should increase sample sizes in these groups and expand on the comparisons by including other specialties and considering the setting of physician employment (hospital, academic hospital, private practice, etc.).
Applications to Professional Practice
This work provides a novel measurement of the phenomenon of flow at work in physicians. Attentiveness and immersion in patient care could translate to improved outcomes in patients and physicians. Administrators should seek to limit thieves of flow such as excessive documentation requirements and unnecessary work interruptions. The physician flow (P-Flow) scales could be used to assess interventions related to workplace efficiencies, increased job satisfaction, or physician well-being.
Supplemental Material
sj-docx-1-whs-10.1177_21650799221093772 – Supplemental material for Physician Flow at Work: Examining Work Absorption, Clinical Flow, Work Fulfillment, and Flow Thieves
Supplemental material, sj-docx-1-whs-10.1177_21650799221093772 for Physician Flow at Work: Examining Work Absorption, Clinical Flow, Work Fulfillment, and Flow Thieves by Jacob Shreffler and Martin Huecker in Workplace Health & Safety
Footnotes
Acknowledgements
The authors would like to thank Alyssa Thomas, Research Coordinator in the Department of Emergency Medicine, for her support of this work.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Institutional Review Board Approval
This study (#21.0114) was approved by the University of Louisville’s Institutional Review Board in spring 2021.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.