
Abstract
Background:
The accommodations sector is one of the largest employers of immigrant and minority workers in the United States. Hotel housekeepers represent the industry’s largest workforce while facing difficult work conditions, health hazards, and psychological stress. This is one of the few empirical studies that address the working conditions of housekeepers in the United States and their perspective of health challenges they face.
Methods:
A cross-sectional survey study was conducted with hotel housekeepers (N = 140) in Florida and in collaboration with the local labor union as a rapid assessment of occupational health and safety risk exposures, work-related injuries, coping mechanisms, and perceived management responses. Experienced union workers recruited study participants and administered interviewer-administered surveys. The analysis included descriptive statistics and multivariate regression.
Findings:
Sampled hotel housekeepers were found to work under significant time pressures to complete excessive workloads and to experience chemical and biological exposures and physical and psychosocial strains. Poor work equipment/insufficient supplies had a negative impact on hotel housekeepers’ health, these include heavy wet towels vacuum cleaners having a significant effect on (p < .001) sprains and strains. Poor cleaning supplies had a significant effect (p < .001) on chemical burns. Other significant findings are provided in the article.
Conclusion/Application to Practice:
While housekeeping work conditions include many challenges, relatively simple changes by hotels’ management can provide potential relief and improve workers’ health and safety outcomes, such as functional equipment, sufficient inventory, management support, and proper rest breaks—subsequently increasing workers’ health and reducing accidents, and thus potentially improving productivity at a relatively low cost.
Keywords
Background
Approximately 53 million people hold low-wage jobs in the United States; of these, 53.7% are women, 47.6% minorities (Hispanic, Black, Asian), and 21.3% immigrants (Metropolitan Policy Program, 2019). Many of these low-wage jobs are in the hospitality industry, where minorities hold more than 65% of the jobs (BLS, 2019), and Hispanics represent 25.3% of the total number of people employed in this sector in the United States (BLS, 2016). Housekeeping is the largest occupation segment within the hospitality industry, representing nearly 23.3% of all hospitality industry employment (BLS, 2018).
Disproportionate risk exposures to Hispanic hotel housekeepers have been well documented and include physical strains and hazards (Hsieh & Chen, 2020), chemical and biological exposures (e.g., toxic cleaning solutions, contaminated objects, human tissue/body secretions, human excreta, mold, microbial contaminants) (CCOHS, n.d.), and psychosocial hazards (e.g., job content/uncertainty, workload/pace, time pressure, organizational culture, discrimination, bullying, harassment) (Hsieh et al., 2016). Earlier studies reveal that occupational injury rates of frontline hospitality sector workers exceed the national average for service sector workers and also have the highest rate of fatal and nonfatal injuries in the United States, as reported by The International Union of Food, Agricultural, Hotel, Restaurant, Catering, Tobacco and Allied Workers’ Associations (IUF; Manovich, 2018). As in other employment sectors, workers who lack legal documentation are at risk of exploitation and intimidation by their employers and supervisors, who pressure workers into accepting poor or unsafe work conditions (De Castro et al., 2010; Moyce & Schenker, 2018).
Hispanic hospitality workers’ quality of life is acutely intertwined with their economic conditions, and they often experience housing, food, and income insecurity (Sönmez et al., 2017). Many housekeepers struggle with poverty, reside in economically depressed and dangerous neighborhoods, and have little to no access to social services, affordable health care, or health insurance (Hsieh et al., 2016, 2017). High levels of strain can result in chronic stress over time, particularly when additional hardships are added, such as social, health, familial, and/or legal issues (Feaster et al., 2019). Several studies on hotel workers’ occupational health—employing both ethnographic fieldwork and survey research—have documented that the workers’ psychological well-being is often jeopardized by the stress of constant time pressures to finish assigned rooms (Hsieh et al., 2016, 2017; Lin et al., 2021).
Florida has the second-highest number of hotel housekeepers in the United States, with 80,900 people working for a mean hourly wage of US$11.20 (annual mean wage of US$23,300; BLS, 2018). This state is also home to the third-largest Hispanic population in the United States (Budiman, 2020). In Florida, there were 439,277 hotel and motel rooms to meet the needs of nearly 125 million visitors in 2018. Florida’s tourism industry recorded an estimated US$125 million in earnings and supported 1.5 million jobs (Visit Florida, 2019). Orlando (located in Central Florida) alone recorded 75 million visitors the same year, making it the most visited destination in the United States, enjoying over US$71 billion in economic impacts and supporting 41% of the local workforce (~499,000 jobs) (Associated Press, 2019).
This study aims to answer the following questions:
Methods
This community-based participatory research utilized a cross-sectional survey conducted among hotel housekeepers in collaboration with the Unite Here Union, Local 737 in Orlando, Florida. Previous research (Hsieh et al., 2016, 2017) indicated that immigrant hotel housekeepers are a hard-to-reach population due to fear of exposing their illegal immigration status and concerns of retaliation from employers for speaking openly about their workplace experiences and issues. Furthermore, managers were reluctant to give researchers permission to interview their workers. To gain access to hotel housekeepers willing to participate in this study, we collaborated with the local office of the Unite Here Union in Orlando. Unite Here is a vocal advocate for local workers’ rights for higher wages, lower workloads, access to health care, and other benefits. Workers were willing to share their experiences with union officers, thereby enabling the study team to collect data. Unite Here has a diverse membership of nearly 11,000 workers, comprised of African Americans, Latinos, and Asian Americans who work across Central Florida at Walt Disney World, Hilton Hotel, Orange County Convention Center, and many other notable hotels and attractions in the area. The Union has become an invaluable community partner in our ongoing work with hotel housekeepers and other hospitality sector workers.
The study sample was recruited from approximately 300 to 400 union members who were hotel housekeepers. Spanish-English bilingual members and associates of the Union administered the surveys to enable translation, following brief training on survey administration and probing for answers. This interviewer-administered survey method was deemed most appropriate for several reasons: (a) the target population’s limited language proficiency and education levels required assistance from English-Spanish bilingual persons to complete the survey, (b) concerns of members of minority groups over their immigration status warranted a high level of trust between study participants and survey administrators—having surveys administered by individuals they already knew through the union and who they trusted was deemed more appropriate than using a team of field researchers they had never met, (c) housekeepers who feared retribution from their employers for speaking about their work conditions required an interview environment they felt comfortable in and interviewers they knew to be their advocates—this helped to assure study participants to speak more freely, and (d) the interviews took place after work house in the comfort of study participants’ homes where they felt free to speak without having to rush and in a non-work environment. Study participants were first informed of the confidentiality of the interview and that no identifying information would be collected. They were told of the voluntary nature of their involvement and of their rights both in written and in oral instructions. Following this, they gave their signed informed consent. Each interview lasted approximately 60 minutes and was conducted in Spanish or English, depending on the language proficiency level and preference of the participant. Study participants did not receive cash incentives for their time. The Institutional Review Board of the University of Central Florida approved the conduct of this study.
Survey Instrument
To reflect the concerns of Orlando hotel housekeepers and to further explore their work and health conditions, two focus-group discussions (four and six people, respectively) with local hotel housekeepers at the Union premises were conducted. Information gathered from the focus groups was utilized for further instrument development. The final instrument included questions on the following: (a) personal background, (b) overall work experience, (c) workload and physical work conditions, (d) work equipment and supplies, (e) health and safety at work, (f) work-related body pains and injures, and (g) methods of dealing with workplace injuries, illnesses, and stress. The survey questions were pilot tested on three hotel housekeeping supervisors in Orlando, Florida, and minor wording modifications were made for clarity.
Survey questions were adopted from Hsieh et al.’s (2016) study of Hispanic/Latina hotel housekeepers in North Carolina. Part 1 of the survey instrument includes demographic information on age, gender, nativity, race, and ethnicity. Part 2 asked questions regarding participants hotel housekeeping work experience, including housekeeping tenure, hourly pay, tips, and health insurance. In Part 3, respondents are asked to rank a list of potential issues (e.g., heavy/broken linen carts, heavy linen, insufficient equipment, cleaning solutions that irritate the skin) and asked to respond using a 4-point Likert-type scale (from no problem at all to a big problem). Part 4 focuses on various health issues participants have experienced because of their work (e.g., knee pain, chemical burns, sprains/strains, injury from slips/trips/falls) on a 6-point Likert-type scale (none, very mild, mild, moderate, severe, very severe; not applicable).
Data Analysis
Data were analyzed using SPSS 22. Descriptive statistics were used to describe the housekeepers’ health issues and strategies they used to cope with work stress. Regression analysis was employed to test the impact of cleaning equipment and tools on hotel housekeepers’ work-related injuries. All assumptions (normality, collinearity, outliers, and autocorrelation) met the criteria of Peck et al. (2019).
Findings
Demographic and Occupational Profile of Study Participants
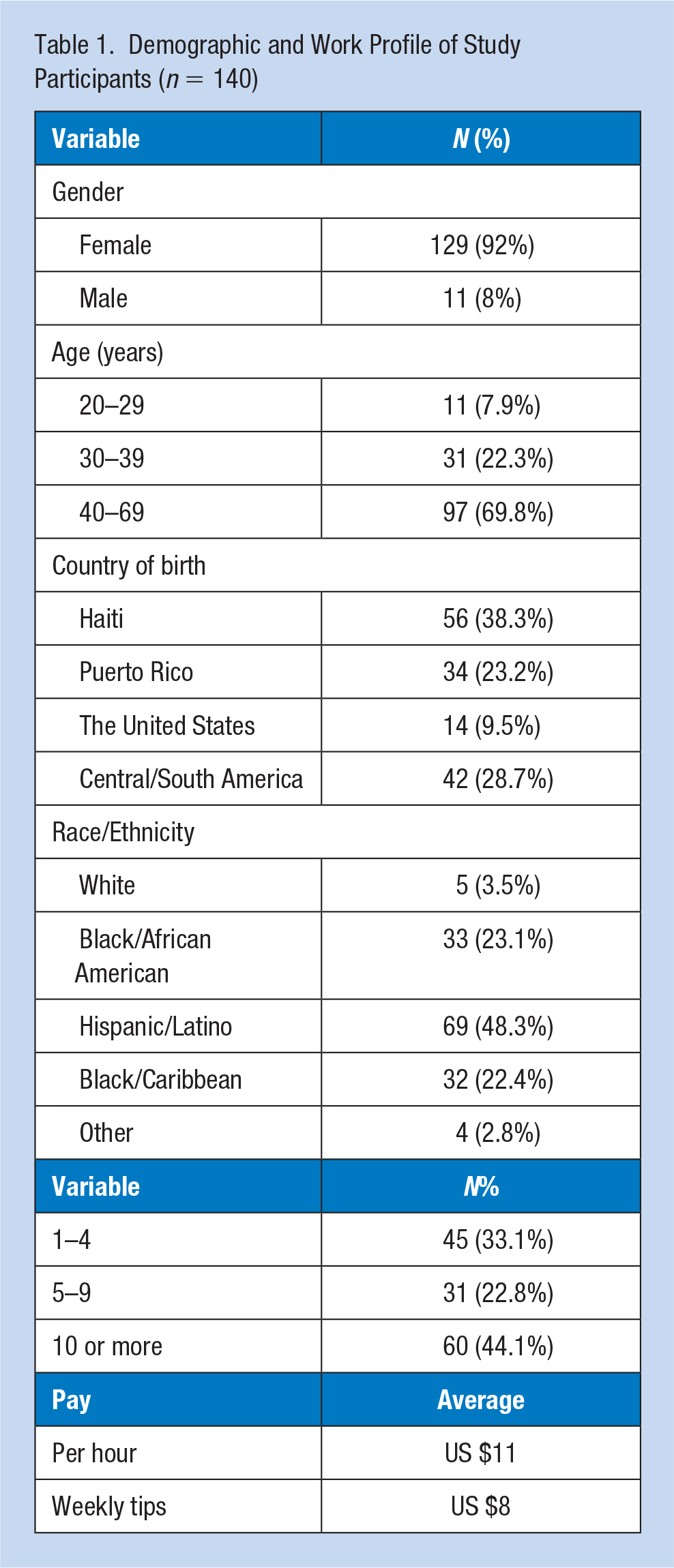
Data from 177 housekeepers were collected with the response rate of approximately 44% over the course of 2 months, yielding a total of 140 usable surveys from the Unite Here Union in Orlando. The study sample is primarily female (92%), between the ages of 40 and 69 years (69.8%), and Hispanic (48.3%), with work experience as a hotel housekeeper ranging from less than 4 years (33.1%) to 10 years or more than 10 years (44.1%) with an average hourly salary ranging from US$8.65 to US$11 and average weekly tips totaling US$8, as noted in Table 1.
Demographic and Work Profile of Study Participants (n = 140).
Health Problems and Work Injuries Experienced by Hotel Housekeepers
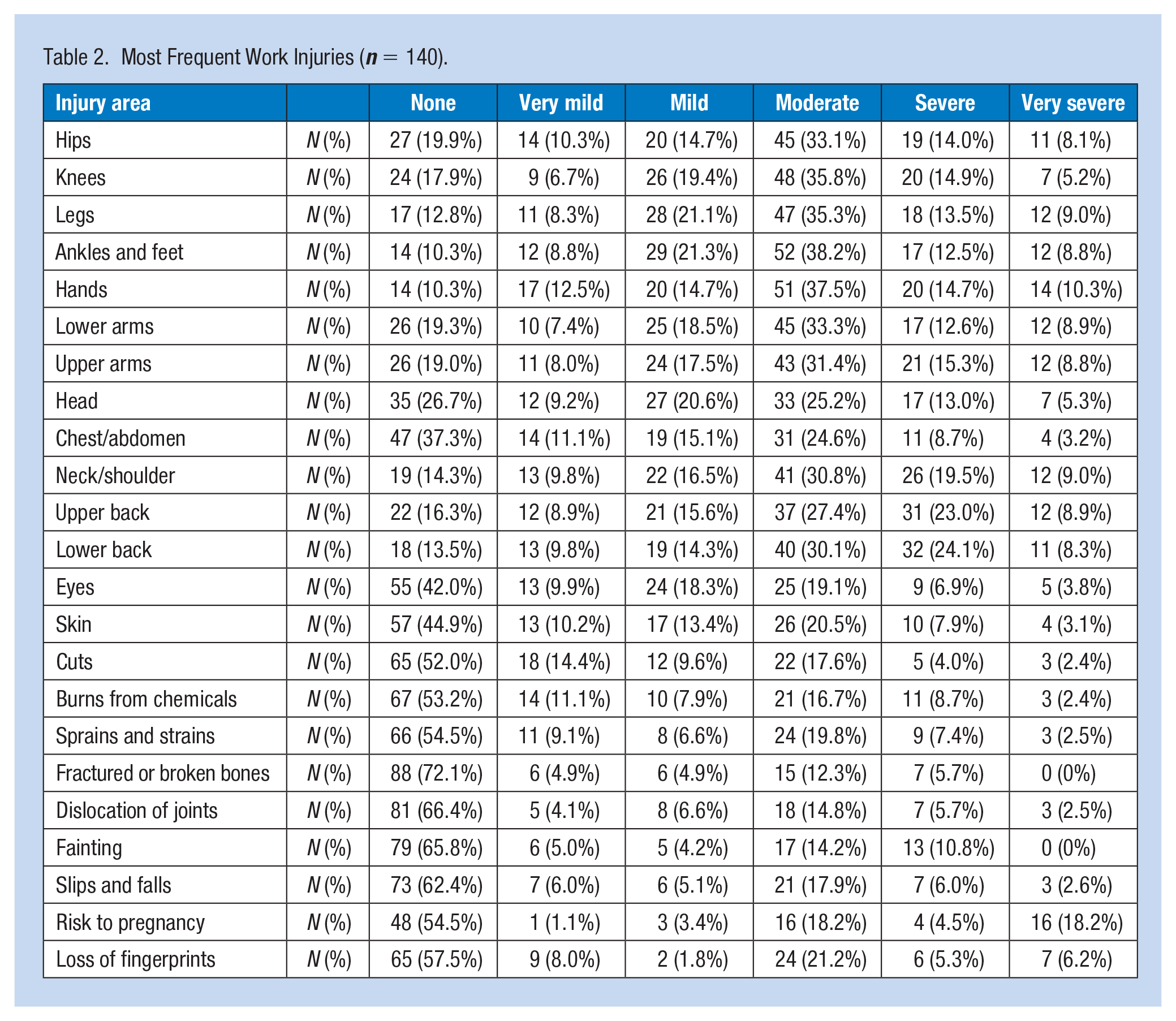
Responses to questions revealed a wide range of health problems and injuries. Housekeepers complained about moderate to very severe upper back (59.3%) as well as lower back pain (62.5%), moderate to very severe headaches (43.5%), and skin burning/itching (31.5%). Respondents also reported moderate (30.8%), severe (19.5%), and very severe (9%) neck and shoulder pain. There were substantial complaints about limbs; participants reported moderate (21.3%), severe (12.5%), and very severe (8.8%) pain in their ankles and feet, attributable to spending many hours on their feet. Furthermore, many reported moderate (37.5%), severe (14.7%), and very severe (10.3%) pain in their hands, as well as moderate to severe pain in lower arms (54.8%), upper arms (55.5%), and legs (57.9%). A third (30%) of respondents reported moderate to very severe sprains and strains, resulting from their work. Many (49.9%) reported their belief that their work presents a moderate to very severe risk to woman who are or were pregnant. Nearly a third (27%) of respondents reported skin burns from chemicals used to clean bathrooms, with another 32.7% of study participants reporting the loss of their fingerprints over time due to chemical exposure and despite wearing gloves. Finally, 25% of respondents reported moderate to severe cases of fainting on the job from fatigue, as noted in Table 2.
Most Frequent Work Injuries (n = 140).
Cleaning Equipment and Supplies
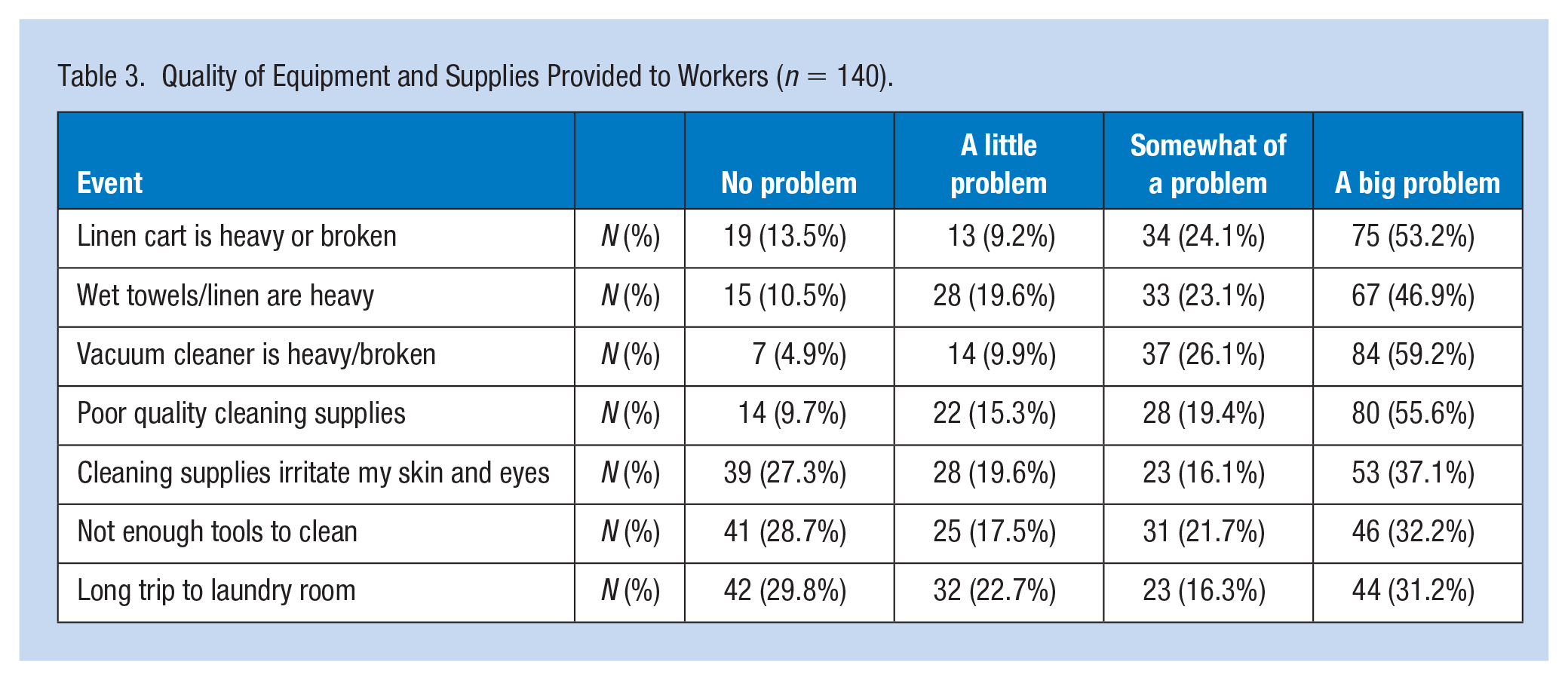
Study participants expressed strong concerns over the equipment and supplies provided by their employers, with 75% reporting that the cleaning supplies do not work well. Nearly 70% indicated that linens and wet towels are too heavy to carry, 85.3% said that vacuum cleaners are either too heavy to lift easily or broken, 53.8% indicated that there are not enough tools to clean the rooms properly, 77.3% reported that linen carts are too heavy to carry easily or broken, and 47.5% reported very long distances between the rooms they clean and the dirty linen room, to where they are required to take the used linen and towels.
Relationship Between Work Supply and Work-Related Injuries
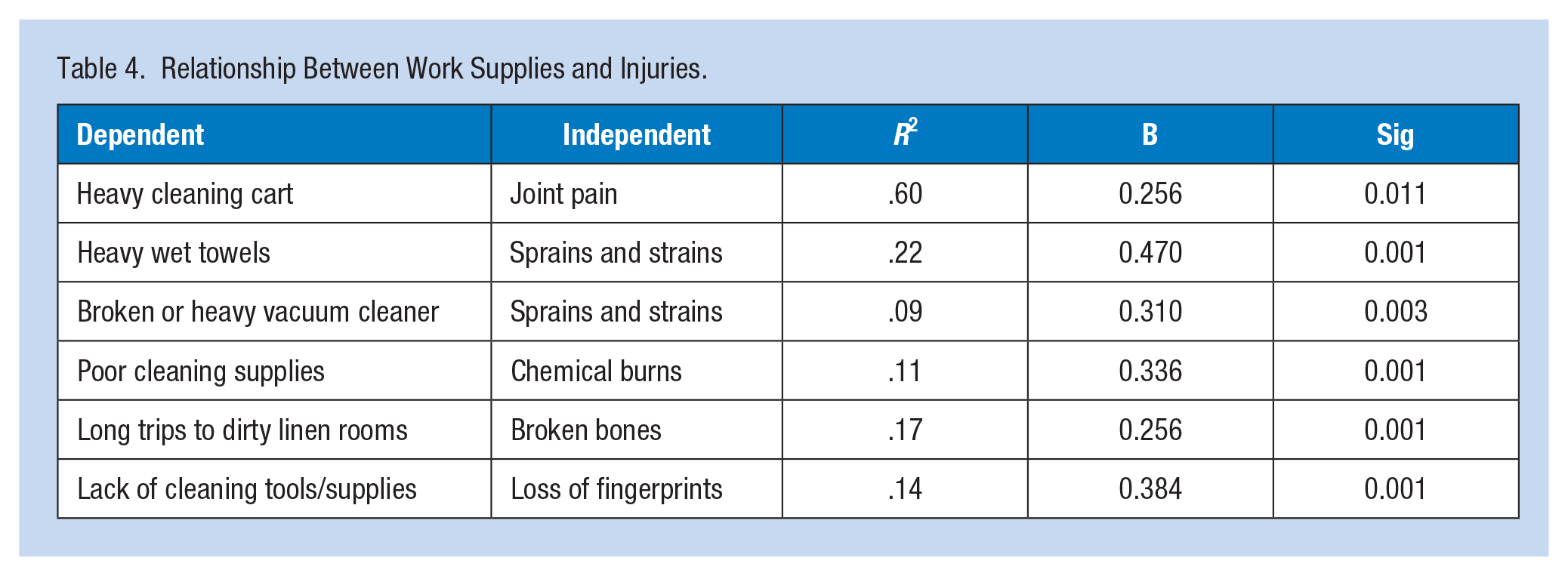
Problems with the linen cart had a significant effect on housekeepers’ joint pain (β = 0.256, p = .11); carrying heavy wet towels (β = 0.47, p < .001) and using broken or heavy vacuum cleaners (β = 0.31, p = .003) had a significant effect on health issues such as sprains and strains. Chemical burns were significantly related to inadequate cleaning supplies (β = 0.336, p < .001), and broken bones were significantly related to the long trips carrying dirty linens and towels to the dirty linen storage area (β = 0.256, p = .001). Finally, the lack of proper tools (e.g., high-quality protective gloves) was associated with the gradual loss of fingerprints (β = 0.384, p = .001), as noted in Tables 3 and 4.
Quality of Equipment and Supplies Provided to Workers (n = 140).
Relationship Between Work Supplies and Injuries.
Housekeepers’ Coping Mechanisms
Personal unhealthy behaviors, while present, were not found to be prevalent among the study participants. For example, 90% reported they do not smoke, and 67.6% do not use sedatives. However, 51.8% use analgesics/painkillers (i.e., ibuprofen/aspirin) regularly, and a little less than half (49.6%) use over-the-counter (OTC) medications to relieve pain. In addition, more than half (50.7%) reported calling in to work sick to avoid working regularly, 22.6% reported frequently crying, 25.9% used humor to cope with their difficulties, and 32.6% spent more time on religious activities as a coping mechanism, as reported in Table 5.
Coping Mechanisms Used by Workers (n = 140).
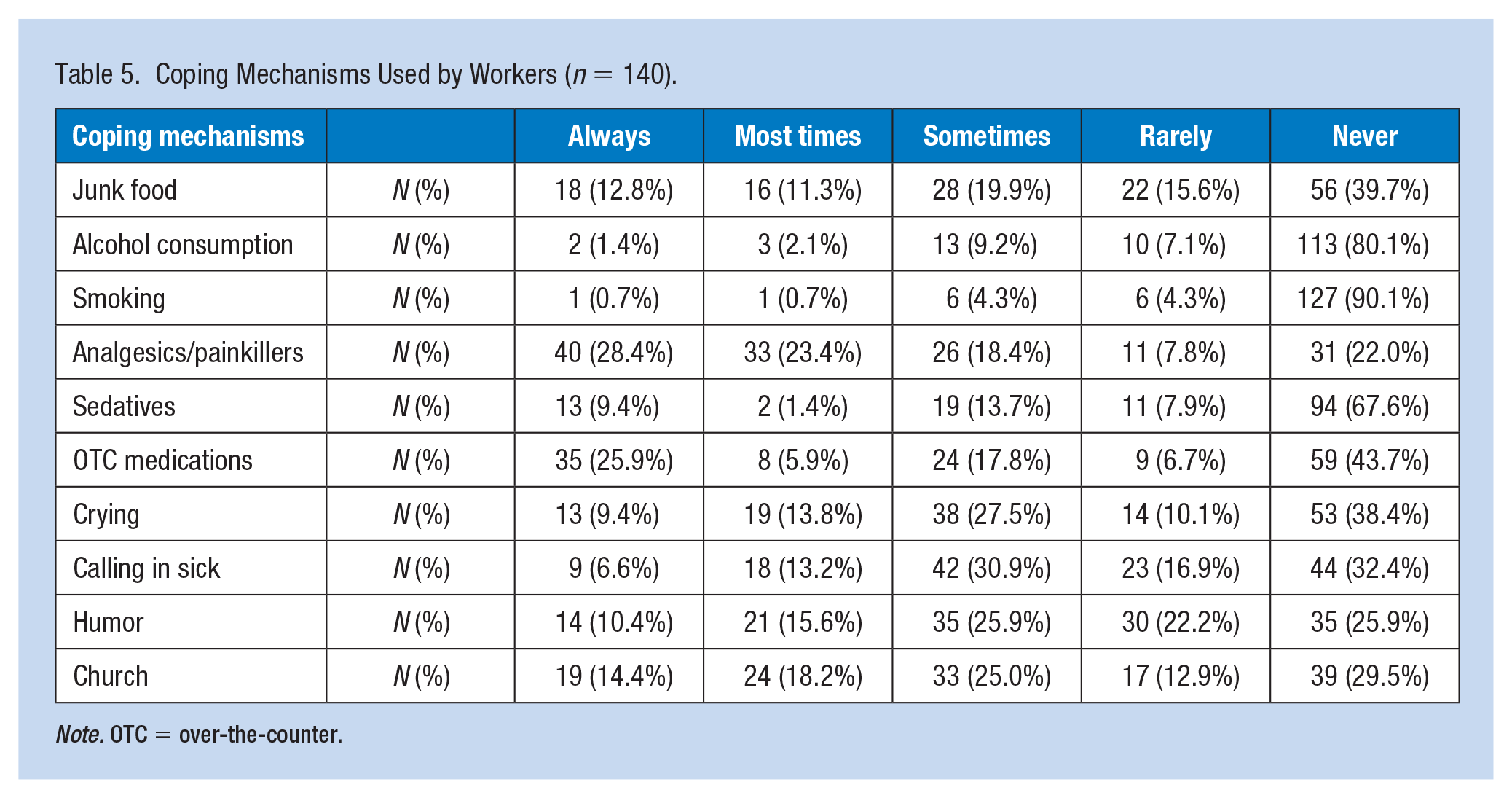
Note. OTC = over-the-counter.
Discussion
The accommodation sector relies heavily on millions of hotel workers, and this workforce contributes significantly to the hospitality industry as well as to the U.S. economy (Adams et al., 2020). Despite this, this study provides empirical evidence of poor working conditions, including occupational hazards and lack of appropriate equipment and hazard controls. Previously ample anecdotal evidence showed difficulties associated with hotel housekeepers’ working conditions, but there was limited empirical evidence due to the challenges of collecting data directly from workers. Overall results show that housekeepers suffer serious musculoskeletal pain due to strenuous physical work and a lack of support to ease the workload. In addition, poor cleaning supplies and broken/poor necessary work equipment contribute to additional injuries, of which some are irreversible. Finally, strenuous work creates additional psychological concerns in which participants used coping mechanisms such as crying, religious activities, and some resort to absenteeism to ease their stress.
Increasing emphasis on globalization, technological advances, and growing trade and tourism has caused the hotel industry to grow exponentially over the years, but the highly competitive nature of the industry together with its seasonality impacts employer’s attitudes toward hotel employees and hiring practices, especially among immigrants and minorities (Elshaer & Marzouk, 2019). The hospitality industry and occupational health and safety regulators must address these health and safety issues.
Immigrant and minority workers in hotel housekeeping jobs who participated in this study worked under great time pressures, endured excessive workloads not easily completed without foregoing needed breaks, faced biological or chemical exposures, and earned minimum or slightly above minimum wage. This study found that the most often reported severe-to-very severe body pain resulting from cleaning hotel guestrooms was in the lower back, upper back, and the neck/shoulder region. This is consistent with the findings from hotel housekeepers in Las Vegas (Krause et al., 2002). Participating Florida housekeepers reported highly frequent use of analgesics/painkillers and OTC medications which also supported the significant and chronic physical pain they suffered due to their cleaning jobs. In terms of work injuries, a risk to pregnancy, loss of fingerprints, and sprains and strains were the most frequent severe injuries experienced by the workers. This study provides evidence of the impact of poor work equipment/insufficient supplies on injuries such as joint pain, broken bones, loss of fingerprints, and chemical burns. This finding underscores the fact that housekeepers continue to face difficult work conditions and continue to be exposed to health and safety risks (Premji & Krause, 2010), further reinforcing the importance of providing appropriate ergonomic cleaning tools and sufficient supplies to hotel housekeepers so that they can mitigate the occurrence of their work-related injuries. It is worth noting that these immigrant housekeepers’ low-income levels and limited access to health insurance and medical services leave them even more vulnerable to health and safety challenges (Sanon, 2014).
Recommendations
Employers are responsible for conducting hazard assessments and must acknowledge that cleaning hotel guestrooms is a physically demanding job with time pressures that jeopardize hotel housekeepers’ physical and mental health over time. There are numerous improvements that can be incorporated into the jobs to improve workers’ occupational health and safety. Nearly three quarters (71%) of our study participants suggested assignment of fewer rooms to clean; instead of assigning tasks based solely on room numbers (a quota), managers could consider assigning housekeepers a number of guestrooms per shift based on factors such as the level of dirtiness of rooms, regular versus suite versus VIP room, number of checkout rooms, number of stay-over rooms, and number of beds in a room. Managers could also consider assigning housekeepers guestrooms on the same floor to minimize the time and energy required to travel between floors, especially while pushing heavy linen carts. Another recommendation is to provide workers with reasonable access to restrooms in the same buildings as their work assignments so that meeting basic biological needs does not create unnecessary strain and/or stress due to the time involved in rushing between buildings. Management should provide sufficient and appropriate cleaning tools, including purchasing ergonomic cleaning carts and lighter vacuum cleaners that are easy to maneuver to help eliminate physical strain on housekeepers. For example, one study showed that simply replacing factory-installed wheels on cleaning carts with solid plastic wheels reduces physical strain on housekeepers and injury claims (Intilli, 1999). Further empirical evidence showed that fitted sheets and mattress lift tools reduce biomechanical exposures by 48% (Harris-Adamson et al., 2019). It is also important that hotels enforce periodic break times to allow physical recovery and that appropriate spaces are provided for these breaks. It is suggested that hotel housekeeping departments have a system in place to track the inventory of cleaning materials and guest amenities and ensure that these items are well stocked for housekeepers’ use.
Furthermore, managers should consider offering stress management programs to equip employees with skills (e.g., breathing and muscle relaxation exercises) to cope with stress (Biding & Nordin, 2014). Other intervention programs such as health education training, health screening, and using mattress lifting tools have been linked to reduced stress and anxiety, improved cardiovascular disease risk, and reduced body mass index (Adams et al., 2020).
Limitations
This study has several limitations. First, we surveyed housekeepers who were familiar with—though not necessarily members of—the local Unite Here union and, as a result, may be more knowledgeable, through discussions with colleagues and friends, about their worker rights than other housekeepers. Future studies could extend to housekeepers who are not affiliated with a union. Second, the issue of housekeeping work during pregnancy came up several times, but the survey did not ask specifically if participants were pregnant at the time. This was because some of the interviewees were male, and we wanted to minimize pointed personal questions that would feel like an invasion of privacy. Because the hospitality industry is predominantly female (Lin et al., 2021), future studies could explore hotel workers who are pregnant. Pregnancy can make women more vulnerable in physically and mentally strained situations and an interesting research direction may be to explore the specific threats and experiences encountered by pregnant hotel workers at their workplace.
Conclusion
In summary, this survey study makes an important contribution to the current understanding of the work conditions of hotel housekeepers. The findings from this study emphasize the strong need for improvements to the occupational health and safety of immigrant and minority workers in the hotel industry. This study reinforces that hotel housekeepers are regularly exposed to physical, chemical, biological, and psychosocial hazards in the workplace and that these lead to various work-related conditions and/or injuries. Hotel housekeepers work under great time pressures to complete their daily assignments and even forego lunch or restroom breaks. Many of the housekeepers surveyed reported working with ongoing musculoskeletal pain and using simple OTC medications to cope. It is clear that much of the pain that housekeepers experience can be avoided using proper and functional equipment, such as linen carts that can be pushed easily over various types of floor coverings (e.g., carpet), as well as basic personal protective equipment (e.g., durable gloves and goggles to protect from harsh chemicals, knee pads for cleaning tile floors).
This study highlights that while housekeeping is an essential workforce which hotels rely on to function, the needs of housekeepers go unmet, and they are treated as expendable workers. Hotel corporations are strongly urged to review the work conditions that their essential workforce is exposed to (e.g., workload, work hours, pay, health benefits, work design).
Applying Research to Occupational Health Practice
Hotel housekeepers require access to professional occupational health services due to the nature of their work. The risks outlined here, including ergonomic, heavy lifting, lack of access to bathrooms and breaks, chemical exposures, job stressors such as time pressure, and lack of hazard communication training and safety training, suggest that a coordinated safety, industrial hygiene, and occupational health program is indicated. In addition to the occupational health hazards, these workers often struggle with income, housing, food insecurities, limited access to healthcare, and language problems. They also experience social exclusion, discrimination, exploitation, and family traumas, among other issues. Living with protracted health inequities, hotel housekeepers remain among the most underserved and understudied populations. Access to occupational health, safety, and ergonomic services could reduce the impact of the work exposures and prevent many work-related health conditions.
Footnotes
Acknowledgements
The authors thank Jeremy Haicken, President of Unite Here Local 737, and his associates, who were instrumental in collecting these data. The authors also thank all the hotel housekeepers who shared their experiences with us as part of this research study.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics
Approved by IRB at UCF
Approval date: March 22, 2017
IRB number: SBE-16-12266
Research ID: ra-168082
Review type: exempt determination
Approved as: human participant research that is exempt from regulation
Author Biographies
Valeriya Shapoval, PhD, is an assistant professor at Rosen College of Hospitality Management, University of Central Florida. Her work focuses on organizational behavior, occupational physical and mental health, big data analysis, and tourism management.
Sevil Sönmez, PhD, is a professor and associate dean in the College of Business at the University of Central Florida. Her interdisciplinary research focuses on the intersection of work, health, and leisure.
Yu-Chin (Jerrie) Hsieh, PhD, is an associate professor in the Saunders College of Business at the Rochester Institute of Technology. Her research interests include hospitality-related human resources, hospitality education, and hotel employees’ occupational health.
Yorghos Apostolopoulos, PhD, is an associate professor of population health and founding director of the Complexity and Computational Population Health Group at Texas A&M University. His work converges at the nexus of social epidemiology, occupational health, and health policy within the framework of complex systems science.