
Abstract
Introduction
Decent working time in the health sector is critical to providing quality care, and balancing health workers’ well-being with the requirements of 24/7 healthcare provision. Nursing and midwifery staff, comprising the largest group in the health workforce, play a crucial role. Understanding their experiences and challenges related to duty rosters is essential for improving work conditions, job satisfaction, and ultimately, the quality of care.
Objective
This study aims to explore the experiences of nurses and midwives with the hospital duty roster at selected health facilities in Ho, the Volta Region of Ghana.
Method
A qualitative research method with a phenomenological approach was employed to capture the nuanced experiences of nurses and midwives regarding the hospital duty roster. A semistructured interview guide facilitated data collection, ensuring a comprehensive exploration of participants’ experiences. Three selected health facilities in Ho, the Volta Region of Ghana, served as the study's location. The study recruited 20 participants (nurses and midwives) to reach data saturation. The collected data were transcribed verbatim and analyzed through thematic content analysis, using a deductive approach. Researchers reviewed the raw data, generating initial codes to capture new concepts of interest.
Results
The duty roster often demonstrated organizational flaws negatively impacting the health, well-being, and job performance of nurses and midwives, consequently affecting patient care quality. The study identified that these healthcare professionals faced significant risks of work-related stress, burnout, and mental health problems due to ineffective coping strategies toward the hospital duty roster. Findings from the study also demonstrated that nurses and midwives prefer day shift because of its short time and the availability of all groups of professionals to help manage cases as compared to a night shift.
Conclusions
The findings underscore factors influencing nurses’ choice of shift patterns, emphasizing the need for further research to explore the extent to which nurses’ preferences are considered when designing hospital duty rosters. Such insights can contribute to improving both the working conditions of healthcare professionals and the overall quality of patient care.
Introduction
In a 24/7 healthcare system, nurses, and midwives along with other healthcare staff are required to work using a myriad of different duty rosters to keep services running and maintain patient care (Ohene et al., 2022). A hospital roster is a method of constructing work timetables for hospital staff which includes the number of staff on duty, budgeting, and other nursing functions and also meeting management's request. It also includes the names of the employees, their ranks, and various dates and times they appear to be working (Pistoria, 2022).
Nurses and midwives are a vital part of the healthcare sector and are the major group in the health profession because of the constantly human-facing nature of their work. Not only do they need to perform the “task-based” aspects of their work well evidenced by attentive, accurate care provision; but they also need to perform the “relational” aspects of their roles well and consistently which is evidenced by caring, empathic treatment of patients (Querstret et al., 2020). The workforce is the most essential and critical resource of the healthcare system and principles need to be established to ensure a clear understanding and consistency in the approach to the effective and efficient utilization of the workforce to ensure safe “rostering” is in place (Brook & Kemp, 2021). Out of the 43.5 million global healthcare workforce, 20.7 million are nurses and midwives (World Health Organization, 2022). Nurses’ shift has been organized by dividing the day into specific shifts and this has been practiced for many years with the world's most popular shift work hours being 8 or 12 h but there are variations in shift patterns between countries (Ejebu et al., 2021). In Europe, five shift types are allocated to nurses; the early shift, day shift, late shift, night shift, and rest shift (Ejebu et al., 2021).
In Ghana, the Ghana Health Service and Christian Health Association of Ghana (CHAG) ensures that the hospital duty roster for nurses and midwives is in a range of shifts and shift patterns. Nurses and Midwives in Ghana operate mostly on a three-shift system over 24 h or 12 h. This shift arrangement involves the morning shift, afternoon shift, day shift, and night shift; within a four-week (28-day) roster period (Asamani et al., 2019). Some nurses and midwives are involved in a rotating shift basis; alternating between morning, afternoon, and night shifts while some nurses work on a normal shift (8am-5pm) basis (CHAG, 2022). Interestingly, 12-h shifts mostly run smoothly as compared to the three-shift system over 24 h. Most health facilities adopt the 6-6-12 system instead of 8-h. The challenges associated with this shift system are regarding its indecorous pattern and implementation among nurses and midwives (Pfeifer, 2022).
The hospital duty roster has been an important tool for healthcare personnel to provide continuity and quality of care to their clients (NSW Health, 2022). Nursing managers are responsible for generating nurses’ duty rosters for all nurses and midwives in a particular health facility (Ejebu et al., 2021). According to Wright and Mahar (2013), the nurse in charge of a particular hospital unit is also responsible for generating shifts and attendance based on the characteristics of the nurses and midwives and this helps in decision-making and enhances direct patient care.
A poor or inflexible duty roster can be detrimental to the nurses’ and midwives’ health and well-being and indirectly leads to poor patient outcomes such as increased mortality rates, and infections, due to prolonged hospital stays (Ejebu et al., 2021). According to Leso et al. (2021), inflexible nurses’ and midwives’ roster induces significant changes in cognitive processes. It can also lead to nurse burnout, stress, physical health disruption, job dissatisfaction, obesity, injuries, and a wide range of chronic diseases and also have shift work-related sleep disturbances (insomnia, shortened sleep, frequent sleep interruptions, irregular sleep cycle). Inflexible nurses’ roster has been associated with family-related conflicts and social life problems.
Nurses and midwives adopt coping mechanisms toward the hospital duty roster to avoid burnout and fatigue at work. They either develop avoidant coping strategies where they completely keep away from the work for a while to rest or have their shifts modified in a way that can be favorable to them and their patients (Koning, 2014). For employers to implement useful measures to mitigate the effects of the indecorously structured hospital duty roster, it was necessary to describe the lived experiences of nurses and midwives with the use of indecorous hospital duty rosters in Ho, the Volta Region of Ghana.
Literature Review
Shift work, including extended hours, night shifts, and on-call schedules, is essential for providing 24/7 services, yet it poses challenges to the nurse (Ejebu et al., 2021). The negative impacts include fatigue, sleep deprivation, and medication errors as highlighted in studies like Ejebu et al. (2021); Moreno et al. (2019), and Sagherian et al. (2017).
Despite the challenges of shift work, Lu et al. (2019) informed that working in shifts helps nurses to dedicate more time to personal and career development by furthering their studies. Nurses on the night shift might go to classes during the day, rest, and work without compromising their performance. In the end, such nurses will be in a better position to provide outstanding quality services to patients and the entire hospital.
In overcoming the snags, Mohd Nasir et al. (2021), suggest efficient scheduling practices, and avoidance of consecutive days, will contribute to minimized medical errors, fatigue, and stress, resulting in improved organizational performance. Longitudinal studies by Ose et al. (2019); and Suter and Kowalski (2021), emphasize the importance of voluntary shift changes, choice, and flexibility for nurses’ well-being. Shorter shifts and staff rotations have been documented as a coping mechanism for nurses (Ejebu et al., 2021). Other studies highlighted napping strategies (Koning, 2014; Merchaoui et al., 2017).
Despite the various research done on hospital duty effects, there's a dearth of literature on nurses’ actual experiences while using an indecorous duty roster. This study aims to describe the lived experiences of nurses and midwives with the use of an indecorously structured hospital duty roster at selected health facilities in Ho, the Volta Region of Ghana.
Method
Study Design
This study used a qualitative method with a phenomenological approach to describe the experiences of nurses and midwives regarding the use of indecorous rosters and how it affects them. According to Doyle et al. (2020), phenomenological research design aims to accurately and systematically examine a phenomenon based on participants’ subjective accounts and provides insight into a better understanding. This descriptive phenomenological approach was suitable because it described all the necessary information regarding the study objectives and covered a good number of the target population (nurses and midwives working at selected facilities in Ho municipality). It provided a detailed investigation, distilling the core and significance of their difficulties, preferences, and perceptions. This approach enables a thorough comprehension of the many elements influencing their job experiences.
Study Setting
This study took place in the Ho municipality, bordered by Adaklu and Agotime-Ziope Districts to the South, Ho West District to the North and West, and the Republic of Togo to the East. Encompassing 2,361 square kilometers, it constitutes 11.5% of the region's total land area (Arku et al., 2008). Ho, the administrative capital of the Volta Region, houses three government-owned health facilities: The Ho Teaching Hospital, Ho Polyclinic, and Ho Municipal Hospital. By including these diverse facilities (a clinic, a municipal hospital, and a teaching hospital), the study aimed to capture a comprehensive understanding of nurses’ and midwives’ experiences across various healthcare contexts as responsibilities and equipment availability differ at each level within the healthcare system in the Ho municipality.
Research Questions
The participants answered research questions regarding their experiences with the hospital duty roster, the challenges they face using the duty roster, and the coping mechanisms they adopt to overcome the challenges.
Sample
This study population included all registered general nurses and midwives with at least 1 year of working experience at the selected health facilities. This is because 1 year of experience was sufficient enough for the nurses and midwives to have experience with an indecorous hospital duty roster.
Purposive sampling was employed in this study. All the nurses and midwives from the selected institutions who met the inclusion criteria were eligible to be interviewed. However, the study recruited 20 participants (nurses and midwives) to reach data saturation. Saturation was reached when additional data did not lead to any new emergent them (Saunders et al., 2018). Campbell et al. (2020) defined purposive sampling as a nonprobability sampling in which researchers rely on their judgment when choosing members of the population. This sampling technique was chosen because this research focuses on particular characteristics of a population that are of interest which will best enable participants to answer the research question. The study included nurses and midwives working at the selected facilities for at least 1 year and willing to consent to take part in the study.
Inclusion Criteria
Inclusion criteria refer to characteristics that your potential participants must have to participate in the study (Garg, 2016). This study included nurses and midwives who were working in the accident and emergency unit, maternity ward, medical ward, and surgical ward for at least 1 year, running any of the shift patterns, and were present at the time of data collection as well as willing to take part in the study.
Exclusion Criteria
Exclusion criteria are any characteristics that potential participants might have that would disqualify them from participating in the study (Garg, 2016). This study excluded nurses and midwives who were on maternity, annual and study leave, rotation nurses who worked at the selected hospitals as well as all student nurses who were doing their clinical practical at the selected hospitals during data collection.
Ethical Consideration
The study was approved by the Ethical Review Committee of a university. Approval was also obtained from selected facilities and individual participants signed the consent form as appropriate. The nature, purpose, and procedure of the study were explained to the participants. Participants were informed that participation in the study was completely voluntary and that they might drop out at any time without consequence. Confidentiality and anonymity were ensured by assigning pseudonyms to participants’ names and years of work experience.
Research Instrument and Data Collection Techniques
A semistructured interview guide was used based on the study objectives. A semistructured research questionnaire consists of both closed-ended and open-ended questions to gather sociodemographic data, and explore participants’ apprehensions and issues related to their duty roster, how it affects them, and their coping mechanisms (Patino & Ferreira, 2018). A semistructured questionnaire was chosen for its flexibility in gathering insights on a specific issue. A pretest (pilot study) involving three nurses and midwives was conducted to enhance the interview guide's validity. Participants were informed and the time and venue for the interview was scheduled based on their convenience. Data collection occurred in December 2022, involving face-to-face interviews with nurses and midwives who provided informed consent. The interviews, lasting 30 to 45 min, were conducted in English, recorded digitally, and supplemented with detailed field notes.
Data Management and Analysis
The outcomes of the interview were analyzed using thematic content analysis. A satisfactory thematic content analysis, according to Braun et al. (2023), depicts the thematic content of interview transcripts (or other texts) by detecting common themes in the texts presented for analysis. Thematic content analysis is a method of presenting qualitative data in a descriptive manner. The data from the recorded interviews was transcribed and categorized. The data was compared with notes taken during the interview process to check for possible omissions or additions. The data was subsequently integrated using the thematic content analysis technique. Codes were developed into themes and subthemes for the write-up. The researchers reviewed and discussed the categories and themes to ensure that participants’ views were represented. The researchers transcribed all the audio tape-recorded information verbatim into readable texts after listening to the audio severally. Direct quotations from participants were presented to ensure that the participant's responses were reflected in the study. Field notes were also reviewed to add depth to the analysis.
Rigor
The study's trustworthiness was ensured by implementing the principles of authenticity, reliability, conformability, and transferability (Forero et al., 2018). To ensure research quality, participant-generated data were cross-checked for accuracy (member tests), enhancing credibility and confirmability. All participants were interviewed using the same manual for consistency (reliability). Peer debriefing further ensured comprehensive data coverage. Transferability was guaranteed by providing detailed documentation, enabling other researchers to replicate the study (Dartey et al., 2022). The authors used the COnsolidated criteria for REporting Qualitative research Checklist.
Results
Demographic Characteristics of the Study Participants
The study recruited 20 participants to reach data saturation as shown in Table 1. The gender distribution of professionals in the study indicates a higher percentage of females (85%) compared to males (15%). Half (50%) of the participants were between the age range of 29 and 33 years. The marital status revealed that majority (60%) are single. Among participants, 65% were registered nurses, 15% were enrolled nurses, and 20% were midwives. Work experience varied, with 30% having 1 to 2 years, 50% with 3 to 4 years, and the remaining 20% distributed across 5 to 10 years. Participants were primarily from the medical unit (40%), followed by 20% from the maternity unit, and 20% each from the emergency and surgical units.
Sociodemographic Data of Participants.
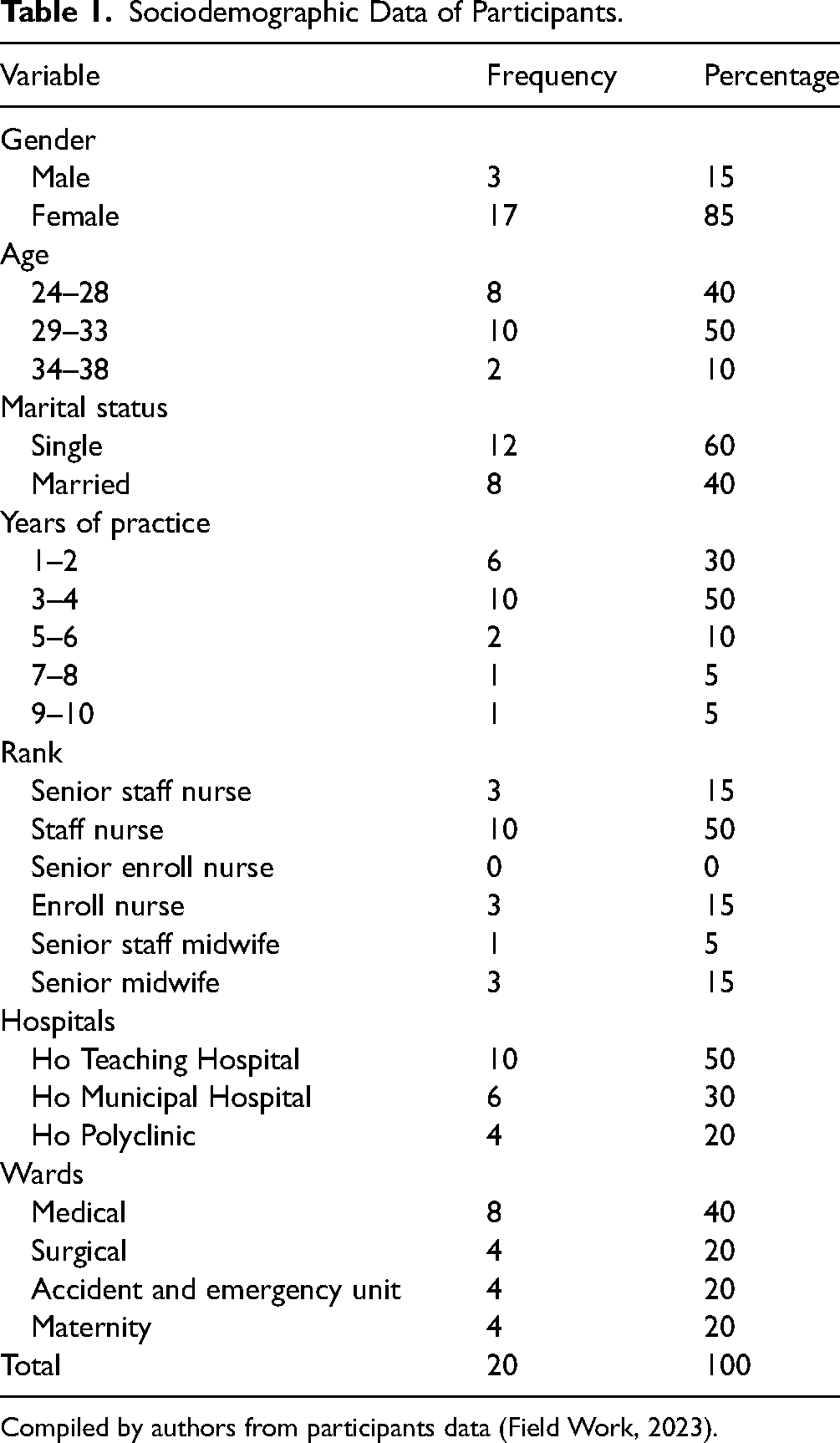
Compiled by authors from participants data (Field Work, 2023).
Emerged Themes
Table 2 shows the summary of the emerged themes and subthemes. The study identified three main themes, with nine subthemes, providing a detailed exploration of the research areas. These subthemes are seamlessly integrated under their respective major themes, offering a comprehensive analysis. The findings, enriched with pertinent quotations, vividly capture the essence of each theme and subtheme, making certain a participant-centered viewpoint and a sophisticated comprehension of their experiences. The emerged subthemes include Opinions on roster schedules, Shift preferences, Health-related issues, Insecurity, Limited social life, Inadequate family time, Sleep-induced strategies, Acceptance of duty roster, and Management of activities.
Summary of the Themes and Their Respective Subthemes.

Compiled by the authors based on thematic content analysis of participant interviews (Field Work, 2023).
Theme 1: Perception of Nurses and Midwives on Indecorous Duty Roster
The study participants were asked to express their perceptions regarding the hospital duty roster. Their Opinions were on the roster schedules, and their shift preferences.
Opinions on Roster Schedules
Eighteen participants stated that their current shift system is stressful. They asserted that, though the current shift schedule is stressful, it varies with the workload on particular days and the unavailability of logistics also plays role in making it more tedious to them. Some participants expressed the following words: …The morning shift is particularly hectic and stressful but I am used to it. When you don’t have enough logistics and you are under-staff, the shift becomes stressful for you. (P12, 4 years hospital work experience). … Because of the workload, the afternoon shift is very tedious. That is when clients usually come for admission; the morning shift is intermittent, but the afternoon shift is a whole course on its own. (P6, 10 years hospital work experience).
Shift Preferences
Seventeen participants expressed their views on which of the shifts they prefer. To this, they emphasized that the day shift is better because of the short time as compared to a night shift and the availability of all groups of professionals to help manage cases that may be coming to the hospital. Some participants expressed these thoughts as follows: …Okay, the day shift has a shorter duration. And you know, you have everybody on deck (you have everybody around; doctors, specialists, the physiotherapist, and everybody that is needed for health care). So, should there be an emergency, we can quickly work as a team. But with night shift, you are restricted, you have to call and be waiting. Should there be an emergency right now we'll have to be calling and be waiting for response from the other health professionals before we can do something that is why I prefer day to a night shift. (P14, 4 years hospital work experience). …I prefer afternoon shift because the time I get to do my chores and take care of the needs of my children. I could do my chores and have my children prepared for school, unlike the morning shift where I will be so tight to do my chores, prepare my kids for school and at the same time prepare for work in the morning. (P9, 6 years hospital work experience).
However, three participants believe that no shift should be preferred over another because there are patients who may require care at any time on the duty roster, and thus a professional should be available to attend to them. Some participants expressed these thoughts:
… Oh, I think that at every point in time, the patient needs somebody to take care of them.
So, I don't really have a preference when it comes to shift schedules. (P1, 2 years hospital work experience). … We should be allowed to run the shifts that will be favorable for us and there should be consistency among the shift. (P4, 3 years hospital work experience).
Theme 2: Consequences Associated With the Use of Indecorous Duty Roster
This theme examines the consequences that the nurses and midwives face with the use of indecorous rosters. It presents findings regarding the experiences of the nurses and midwives as they work on the various wards. Details are presented in subsequent paragraphs.
Health-Related Issues
According to the participants, the continual use of improperly structured duty roster is detrimental to their health. They usually suffer headaches, general body pains, high blood pressure, psychological challenges, and even irregular menstruation, especially after a night shift schedule. Here are a few expressions about health issues that affect nurses and midwives: …Per my experience, the health challenge I normally face is having continuous headache anytime I run night shift. For that reason, I was asked not to run night shift again. It also affects my blood pressure at times because I don’t rest. (P4, 3 years hospital work experience). …Usually, I do experience general body pains due to accumulated stress from day shift. (P13, 5 years hospital work experience).
Three participants expressed thoughts on exhaustion as well: …Personally, when I am tired, it slows down my performance, for example, something I should do in 30 min I might end up using one hour or more. (P13, 5 years hospital work experience).
Also, 10 participants expressed that they do experience psychological challenges with regards to the duty roster. Often times they experience emotional disturbances and get depressed. These are some psychological issues that nurses and midwives in this study have encountered with regards to the duty roster: … The stress that comes with work schedule gets me emotionally disturbed at times. (P5, 2 years hospital work experience). … Okay, when I’m fatigued, I sometimes become so depressed and I don't feel like working when I come for my shift. (P20, 2 years hospital work experience).
Insecurity
Not all the challenges from the use of indecorous duty roster were on physical health but some has to do with participant's personal security. The majority of the participants expressed that they stay far away from their respective places of work and so, closing late especially after an afternoon shift (2 p.m.–8 p.m.) schedule exposes them to danger and they feared for their lives. Some expressed thoughts that best fits this subtheme are as follows: …Where I am staying currently is very far. When I close at night it is very risky to get there, and the road to my place is not good, and armed robbers too are around, even though I haven’t been robbed before. (P3, 3 years hospital work experience). …When I came to Volta region, that was in 2017, there used to be no street light on my route and we those who had no car or anyone to pick us, it was risky for us. I was pregnant with my first child too. I used to walk around with pepper spray and a shocker. (P13, 5 years hospital work experience). Five participants believe that when the closing time for the afternoon shift is reviewed it will help alleviate them from their fears. To this end an expressed suggestion by participants view to this assertion is that: …I suggest they make the shift more flexible especially the afternoon shift should close earlier than 8 p.m. (P15, 2 years hospital work experience).
Limited Social Life
Majority of the participants mentioned that they are unable to socialize as they want because of the nature of duty roster. Also, study participants are of the view that, their social life have been severed, all thanks to the hospital duty roster. Some expressions are: …Sometimes I wish to attend an event somewhere, but it conflicts with my work schedule, so I have to forfeit where I have to go. I miss important gatherings. (P16, 4 years hospital work experience).
Also, three participants lamented on how indecorous duty roster has affected their relationships with friends: …it has profound effects on my relationship with friends. you see in this hospital, we run the duties throughout the week with just two random days off. So, for example, if there's a wedding happening during the weekend, and then you're for duty on weekend, you are unable to go so you end up missing out on that part. And also, during the holidays too you are at work unless you get that particular day off. So, if there's an event or a program, you miss out on that. During Christmas you sometimes don’t enjoy Christmas holidays because you are at work throughout to the New Year. So yeah, I am unable to be with my family and friends. (P11, 2 years hospital work experience). …The roster makes me unable to attend events and people do not believe it is because of the job demand that is why I am not able to show up at ceremonies. It has altered my family life and relationship with old friends. They hold grudges and complain about my inability to be with them. (P14, 4 years hospital work experience).
Inadequate Family Time
Participants were worried that the nature of their duty roster even goes to extent of giving them issues in their family relationships. Majority of the expressed worry on this issue: …My family is not here with me, and with my one day off duty, I can’t travel to them just for one day and comeback, so I hardly see my people. I don’t get the chance to meet all of them. I’ll say the shift is bringing disunity in the family. The shift can pose a problem to couples, because if I get married, I need to be closer to my husband, if you don’t get someone who is understanding, you might end up cheating on them or they on you, so in that case I’ll be thinking about a transfer. (P2, 3 years hospital work experience). …Sometimes you might plan activities with your family but due to the shift schedule, you have to cancel the plan. (P18, 4 years hospital work experience). …when I run night shift, and I get home late morning the next day, I don’t meet my family home. I become so tired and I’m not able to communicate with them effectively as they expect me to do when they return. I sometimes put my phone on silence so that I can sleep. For some time, I haven’t had enough time with family and friends. (P16, 4 years hospital work experience).
Theme 3: Coping Mechanisms of Nurses and Midwives With Regard to the Use of Indecorous Duty Roster
Managing mechanisms are necessary to help nurses and midwives to deal with stressors which may affect their health and well-being. Majority of the participants mentioned ways in which they try to adapt toward the hospital duty roster and these include sleep induced strategies, agreement to work any shift and management of activities when the duty roster for the month released.
Sleep-Induced Strategies
This subtheme on how participants try to cope with indecorous duty roster, especially with how to induce sleep after post night shift, they indicated that: …I take warm Milo or warm water and it helps me to fall asleep early after my night shift. (P6, 10 years hospital work experience). … I rather listen to music, it works for me … I don’t take medication to sleep because I can easily get addicted to them. (P10, 4 years hospital work experience).
In addition, some participants mentioned the use of drugs as a coping strategy. they indicated that: …I take drugs. I take sleeping pills once in a while. I finished my night shift on Monday morning, in the night I couldn’t sleep, Tuesday too I couldn’t sleep so Wednesday I took sleeping pill before I was able to sleep. It is just the work that is causing the inability to sleep. I don’t try any other mechanism apart from the pills. (P7, 8 years hospital work experience).
Acceptance of Indecorous Duty Roster
In line with coping strategies participants also indicated that have made up their mind to work with any duty roster that may come their way. In registering their views this what they said: …I just tune my mind, you know you have to come to work, so you tune your mind to the work. You make your plan based on the duty roster and the shift. (P13, 5 years hospital work experience). …I feel you can never always have what you want. So, whether I'm given morning, afternoon or night shift, I just take it as it is, and I don't try to worry so much about it. I feel like if I don't want to come for night, who should come for night? So, we have to reach that agreement and you don't come for night throughout the month or two, so there should be a balance. (P17, 3 years hospital work experience]. …I don’t have any say when it comes to the duty roster so I just accept it the way it is scheduled for the work to go on. (P18, 4 years hospital work experience).
Management of Activities
Another way participant tries to cope with the duty roster is to make plans based on their schedules with the duty roster in focus. Some of these assertion by the participants include: … I draw plans when roster is done so that I can cope. (P6, 10 years hospital work experience). …I normally try to have enough rest when I get home so I don’t come to work so tired. That is how I cope with the duty roster. (P7, 8 years hospital work experience). …I planned ahead of time. So, if I’m for the afternoon I prepare food or when I am off, I cook and store it in the fridge, and do my laundry so it doesn’t affect me much. (P14, 4 years hospital work experience).
Discussion
The study findings brought to light the preferences and experiences of nurses and midwives about the indecorous duty roster, including their perceptions and opinions on their roster schedules. The majority of the participants in this study preferred the morning shift because it is short and oftentimes all the medical teams are available albeit this was dependent on the number of patients to staff ratio and the kind of cases on the ward. This finding is consistent with Haller et al. (2018) who revealed that nurses were satisfied or preferred short shifts. Another study by Suter and Kowalski (2021) offered a perspective on how shift work was affected due to the COVID-19 pandemic and as a result of the increase in patient numbers, and workload, nurses needed to adjust shift patterns dynamically according to the workload. In the contrary, studies by Gao and Scullin (2020); Haller et al. (2018); Ose et al. (2019); and Thomson et al. (2017) showed nurses preferred long shifts (night) to day shifts. This was also observed in our study where an insignificant section of the participants expressed that they prefer the night shift because of the off days they enjoy when they are done with their duty. The extra days off and improved work–life balance were often mentioned as the reason for a preference for long shifts in several studies (Baillie & Thomas, 2019; Haller et al., 2018; Ose et al., 2019; Suter & Kowalski, 2021). It is worth noting that, having choice and flexibility around shift patterns is a known determinant of increased well-being and health (Nijp et al., 2012; Turunen et al., 2020) Therefore, interventions aimed at adjusting shift patterns should consider involving nursing staff to maintain a certain degree of choice. Further research may also explore the degree to which personal conditions affect nurses when choosing a shift. Particularly considering the indication that personal circumstances are not regularly considered by ward in-charges when designing duty rosters, which are often designed based primarily on service demands rather than staff needs (Ejebu et al., 2021; James et al., 2020; Rodriguez Santana et al., 2020) In addition, communication between ward in-charges and nurses should be strengthened to appreciate nurses’ perspective when scheduling shift schedules.
Also, the feeling of obligation nurses and midwives show towards colleagues, patients, and the healthcare system in Ghana is well reflected in our study which they need to sacrifice their health or children's health for the work or patients which typifies the “Super nurse” culture (Rainbow, 2019; Steege et al., 2017). This finding agrees with Ejebu et al. (2021) study in which nurses feel they need to sacrifice themselves, their health, or their children's health for the greater good of the nursing team and or their patients.
Nurses and midwives working night shifts described how the lack of human resources and support from other professionals, for example, other healthcare professionals led to being overburdened and not getting rest. Nurses working night shifts experienced increased autonomy and fewer interruptions to planned nursing care as a result of fewer family visits during that time. Several studies also reported similar findings in support of our study results (Ejebu et al., 2021; Landis et al., 2021; Powell, 2013)
Concerning the consequences of the use of an indecorous duty roster, nurses and midwives in this study mentioned health-related issues, insecurity, limited social life, and inadequate family time as the challenges they face due to the nature of the duty roster. Similarly, Books et al. (2020) indicated that nurses often reported detrimental mental and physical health as a result of working shifts. Fatigue and tiredness were features reported by nurses across all shift lengths, saying that nurses and midwives endure a physical burden when working shifts regardless of their length (Ejebu et al., 2021). They stated that fatigue could be manifested by physical pain, difficulty transitioning from day to night-time, and vice-versa, reduced concentration. Fatigue was often discussed in shift work that is workload, and it was found to be worsened by working more than two consecutive long shifts. This was observed in our study in which most participants reported headache or musculoskeletal pain after a night shift. This was amplified by nurses experiencing increased workload as a result of staff shortages during their shifts.
Nurses’ sleep patterns were reported to be negatively affected by long shifts, especially night shifts. This aligns with Epstein et al. (2020) study in which nurses had disturbed sleep patterns. The present study found that, following the night shift, most nurses and midwives slept the least number of hours even though they were on a rest day. This is likely due to an attempt to sleep during the day when stress hormone levels such as corticosteroids and catecholamines are at the highest levels and under the influence of the light–dark cycle and other environmental cues which promote wakefulness (Arendt, 2010). Sleep loss has been shown to decrease cognitive capabilities such as concentration, attention span, and reaction time which, in turn, increase the risk of work-related errors and accidents (Arendt, 2010). This is of great importance since nurses must maintain maximum levels of vigilance and attention during work to ensure efficient patient care and safety.
In addition, it is well-known that sleep deprivation is associated with the alteration of cardiovascular autonomic control characterized by a chronic sympathetic overactivity that may promote cardiovascular diseases (Tobaldini et al., 2017). This study registered a finding where there is an irregularity with blood pressure after a night shift and even irregular menstrual cycle. As a result of the increase in patient numbers and acuity, and, consequently, in workload, nurses highlighted the need to adjust shift patterns dynamically according to the workload. They also emphasized the importance of considering their physical and mental experience during shift scheduling.
The strategies that nurses and midwives use to deal with stress have been shown to have a strong impact on their mental health and well-being (Kinman et al., 2020). Managing mechanisms are necessary to help nurses and midwives deal with stressors that may affect their health and well-being. Sleep-induced strategies, acceptance of indecorously prepared duty rosters and management of activities are some strategies adopted by participants in this current study. All the same, with the frequent reports of fatigue, nurses and midwives in this study did not seem to deploy effective coping strategies. This is congruent with similar studies by Ejebu et al. (2021) who reported how nurses despite resorting to unwholesome eating and drinking as managing strategies to survive night shifts still experienced fatigue.
Limitation
The restricted generalizability, participant homogeneity, and dependence on qualitative interviews of this study on nurses and midwives in Ghana's Volta Region limit its breadth, even though, it provides insightful information about experiences with duty rosters.
Implications for Practice
Nurses should be involved and their preferences should be considered when designing the duty roster. There is a need for research to describe and address the effects of the hospital duty roster on nurses and midwives and the coping strategies they adopt toward the duty roster in Ghana. An evidence-based course program during training is needed to help nurses acquire self-care strategies and build effective coping and resilience for them to be able to deal with stressors on the job. An evidence-based structural frame which takes into consideration staff welfare that will guide the design of the hospital duty roster should be implemented.
Conclusion
From this study, it is evident that indecorously prepared hospital duty rosters for nurses’ and midwives’ affect their health and well-being, job performance, and the patient care they provide. Also, nurses and midwives are at considerable risk for work-related stress, burnout, and mental health problems as they do not employ effective coping strategies toward the hospital duty roster. Further research should explore the extent to which nurses’ preferences are considered when designing the hospital duty roster. Research should also strive to better describe and address effect of the hospital duty on nurses and midwives and the coping strategies they adopt toward the duty roster in Ghana.
Supplemental Material
sj-pdf-1-son-10.1177_23779608241275323 - Supplemental material for Experiences of Nurses and Midwives With Indecorously Structured Duty Rosters at Selected Health Facilities in Ho, Volta Region of Ghana: A Qualitative Study
Supplemental material, sj-pdf-1-son-10.1177_23779608241275323 for Experiences of Nurses and Midwives With Indecorously Structured Duty Rosters at Selected Health Facilities in Ho, Volta Region of Ghana: A Qualitative Study by Anita Fafa Dartey, Vivian Tackie, Comfort Worna Lotse, Dodoo Lily and Francis Mawougnon Sagbo in SAGE Open Nursing
Supplemental Material
sj-docx-2-son-10.1177_23779608241275323 - Supplemental material for Experiences of Nurses and Midwives With Indecorously Structured Duty Rosters at Selected Health Facilities in Ho, Volta Region of Ghana: A Qualitative Study
Supplemental material, sj-docx-2-son-10.1177_23779608241275323 for Experiences of Nurses and Midwives With Indecorously Structured Duty Rosters at Selected Health Facilities in Ho, Volta Region of Ghana: A Qualitative Study by Anita Fafa Dartey, Vivian Tackie, Comfort Worna Lotse, Dodoo Lily and Francis Mawougnon Sagbo in SAGE Open Nursing
Footnotes
Acknowledgments
The researchers wish to thank all participants and our able research assistant John Yesuohene Ofori for supporting this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.