
Abstract
Background:
Auxiliary tasks such as administrative work often include tasks that are unnecessary in the view of workers but still have to be done. These tasks can threaten a worker’s self-esteem. The purpose of this study was to examine the effects of unnecessary and unreasonable tasks on musculoskeletal pain.
Methods:
Fifty-five office workers (29 male; mean age = 41.96, SD = 14.2 years) reported their unnecessary and unreasonable tasks at the beginning of the study and kept a diary of their daily musculoskeletal pain over 5 weeks, using a visual analogue scale. Other work-related risk factors (prolonged sitting), job resources (participation in decision-making), and individual risk factors (sex, smoking, exercise, body mass index, maladaptive back beliefs) were controlled for in multilevel regression analysis.
Findings:
Multilevel regression analysis with 742 reports showed unnecessary tasks (B = 4.27, p = .006)—but not unreasonable tasks (B = 3.05, p = .074)—to predict the daily intensity of musculoskeletal pain, beyond other significant risk factors, such as prolonged sitting (B = 2.06, p = .039), body mass index (B = 1.52, p < .001), and maladaptive back beliefs (B = 3.78, p = .003). Participation in decision-making was not a significant protective factor (B = −1.67, p = .176).
Conclusions/Application to Practice:
The higher frequency of unnecessary tasks—compared with unreasonable tasks—could place workers at risk for musculoskeletal pain. Work redesign that reduces unnecessary and unreasonable tasks can make a valuable contribution to worker health and safety among office workers.
Keywords
Background
Musculoskeletal disorders, such as back pain, neck pain, and pain in muscles and joints, are among the most prevalent global health problems, as reported in the Global Burden of Disease Study (Vos et al., 2015). Psychosocial aspects of work, such as shift work, conflicting demands, or time pressure have been observed to increase the risk of musculoskeletal pain (Igic et al., 2013). Repeated or enduring strain is related to musculoskeletal pain through a variety of psychological, for example, pain-related fear or individual coping styles (Boselie & Vlaeyen, 2017; Jun et al., 2019), and physiological processes, for example, decrease of heart-rate variability or increase in blood pressure (Marin-Farrona et al., 2020; Munakata, 2018), that elicit muscle tension (Minerbi & Vulfsons, 2018; Nawab et al., 2010). Observational studies, including taxi-drivers (Burgel & Elshatarat, 2017) and nurses (Elfering et al., 2018), have shown that work stressors are associated with musculoskeletal pain.
Unnecessary and unreasonable tasks are perceived as illegitimate, contribute to an increased work load, and pose a threat to workers’ confidence, according to the Stress as Offense to Self (SOS) model (Semmer et al., 2015). Illegitimate tasks have been associated with feelings of resentment, desire for revenge, sadness (Semmer et al., 2020), musculoskeletal pain (Rolli Salathé et al., 2012), and anxiety and depressive symptoms in employees at entry-level occupations (e.g., retail or service industry jobs;(Fila & Eatough, 2019). However, interactions with resources such as supervisory support or job control were only found for unreasonable tasks but not for unnecessary tasks. Fila and Eatough (2019) concluded that, unlike unnecessary tasks, unreasonable tasks are context-dependent as they describe a mismatch with the specific role in an organization. Accordingly, Semmer et al. (2019) explained that unreasonable tasks are those which one feels one should not have to do, and unnecessary tasks are those one feels no one should have to do.
According to Jacobshagen (2006), about every third work task is unnecessary or unreasonable among different occupations (e.g., teachers, office workers.), while unnecessary tasks are experienced more often than unreasonable tasks (21% vs. 13%, respectively). In this same study, mostly auxiliary tasks, such as administrative work, were experienced as illegitimate. These tasks often need to be done, but rarely give a sense of achievement when finished (Jacobshagen & Semmer, 2018).
Unreasonable tasks are maybe more severe than unnecessary tasks on self-worth related outcomes, such as depressive mood (Eatough et al., 2016), negative emotions (Pindek et al., 2018), anxiety, or emotional exhaustion (Fila & Eatough, 2018). But this might not be the case for the stress-induced muscular pain reaction.
As unnecessary and unreasonable tasks could increase musculoskeletal pain, job resources could reduce musculoskeletal pain. Also, participation in decision-making has shown to be an important job resource to reduce and avoid musculoskeletal pain (Waongenngarm et al., 2016). In a study with workers of a municipal office (Elfering et al., 2010), only those with lack of participation in decision-making suffered significantly more back pain after organizational changes.
According to Mannion et al. (2020), fear-avoidance beliefs predict a poor outcome in patients with back-pain. Thus, patients reduce activities and stay immobile, which increases the likelihood of the transition from acute to persistent low-back pain through a cycle of catastrophizing, depression, deconditioning, and disability (Panhale et al., 2016). Elfering et al. (2009) showed in a cross-sectional study in Switzerland that unfavorable back beliefs hinder recovery of low-back pain over 52 consecutive weeks. Also, maladaptive back beliefs predict future pain the most, when participants do not exercise (Elfering et al., 2015).
Based on these findings, we aimed to examine if unnecessary and unreasonable tasks were associated with daily musculoskeletal pain. We proposed that the higher frequency of unnecessary tasks make them a special threat to musculoskeletal pain. Because of common practice (Semmer et al., 2019), we also aimed to test the total illegitimate tasks scale and expected it to predict higher daily musculoskeletal pain.
Methods
This study aimed to examine the effects of unnecessary and unreasonable tasks on musculoskeletal pain in sedentary office workers employed in a federal administration in Switzerland. We also assessed other work-related risk factors (prolonged sitting), job resources (participation in decision-making), and individual risk factors (sex, smoking, exercise, body mass index, maladaptive back beliefs). This study used secondary data from an organizational health intervention study that took place in 2017 (Faes et al., 2018).
Participants
The idea of a study in office workers was presented to the top management of a Swiss federal department (Faes et al., 2018), who, in turn, gave their employees the opportunity to complete all tasks relating to this study within their working hours. All office workers from a one of their administration departments (N = 101), which worked in the same office building, joined the study-presentation in their team meeting and were asked to participate. Workers were excluded if they were pregnant, had osteosynthesis material (e.g., implants, screws.), musculoskeletal disorders, joint problems (especially regarding the knee, hip, and back), herniated disks, rheumatism (such as spondylitis, gout, osteoporosis, osteoarthritis), or other severe health impairments that cause musculoskeletal pain.
The study conformed with recommendations of the Declaration of Helsinki and all requirements defined by the Swiss Society of Psychology. The ethical committee of the University of Bern approved the study proposal (Nr. 2017-08-00003). Participants were given a guarantee of confidentiality and all provided informed consent prior to their inclusion in the study. All participants filled out the registration form with information about their rights, including to stop whenever they wanted.
Data Collection
In the first week of the study, all participants answered a general questionnaire about work and well-being, in which workers were asked demographic questions about age, sex, body mass index and smoking behavior, illegitimate tasks—including unnecessary and unreasonable tasks—using the Bern Illegitimate Tasks Scale (BITS), as well as on participation in decision-making, prolonged sitting at work, maladaptive back beliefs, and lack of exercise. In addition, they reported their musculoskeletal pain on a visual analogue scale (VAS) for every working day for 5 weeks.
BITS (General Questionnaire)
The BITS (Semmer et al., 2010) assesses unnecessary and unreasonable tasks with four items each. All items start with the lead-in phrase: “Are there tasks/assignments in your daily work that make you wonder whether.” The items concerning unnecessary tasks end with statements, such as “they have to be done at all?” or “they make sense?” The items on unreasonable tasks end with statements, such as “somebody else should do them?” or “they provoke an embarrassing situation?” Participants answered these questions on a scale from 1 “never” to 5 “very often.” Semmer et al. (2015) stated an internal consistency of α = .75 for unreasonable tasks, α = .84 for unnecessary tasks, and α = .85 for the total illegitimate tasks scale and a correlation of r = .51 between the two facets unnecessary and unreasonable tasks.
We assessed prolonged sitting by asking, “How much time do you spend in a working day sitting without the possibility to stand up?” Possible answers were from 1 “not at all” to 5 “more than six hours.” This single item is from the Instrument for Stress-Related Task Analysis (ISTA) questionnaire (Semmer et al., 1999).
We assessed participation in decision-making by asking how much influence people had on decisions about their work situation. Possible answers were from 1 “I have no influence” to 5 “I strongly influence these decisions.” This single item is part of the ISTA from Semmer et al. (1999).
To examine maladaptive back beliefs, we used the Back Beliefs questionnaire (Symonds et al., 1996). Respondents are asked to indicate their agreement with nine maladaptive back belief statements (e.g., “Once you have had back trouble there will always be a weakness”) on a 7-point scale from 1 “completely disagree” to 7 “completely agree.”
We assessed lack of exercise by asking how often participants were doing sport/exercise. Possible answers were from 1 “never” to 7 “more than once a day.” Therefore, lower values indicated a greater lack of exercise.
Musculoskeletal pain was assessed on a VAS and is the outcome measure in this study. The VAS (Häfeli & Elfering, 2006) was introduced by “Throughout the day, how do you rate your personal sensations in muscles and joints (back pain, shoulder and neck pain, pain in leg muscles etc.)?” Answers to this question ranged from 0 “no pain” to 100 “worst pain imaginable.”
Data Analysis
First, we calculated the descriptive statistics (frequencies, mean, standard deviation) of work-related risk factors (unnecessary tasks, unreasonable tasks and prolonged sitting), job resources (participation in decision-making), individual risk factors (sex, smoking, exercise, body mass index and maladaptive back beliefs). and daily musculoskeletal pain.
For these analyses, daily musculoskeletal pain was regressed on risk factors in a linear multilevel regression. Our data included repeated measurements on musculoskeletal pain for five workdays over five working weeks. Thus, the data have a multilevel structure: participant demographics and information from the general questionnaire was on Level 2 and musculoskeletal pain on Level 1 (Eid et al., 2010; Woltman et al., 2012). Continuous predictor variables at the person level were centered at a grand mean. Our sample sizes on the person level (Level 2, n = 55 individuals) and day level (Level 1, n = 742 person-days) were sufficient for multilevel regression analysis (Maas & Hox, 2005). The sample size of Level 2 fit the recommended size of 50 (Maas & Hox, 2005).
We calculated three multilevel regression models to test the effects of unnecessary tasks (Model 1), unreasonable tasks (Model 2) and illegitimate tasks (Model 3) on musculoskeletal pain. We included maladaptive back beliefs, prolonged sitting, and participation in decision-making as predictor variables. Also, we controlled for group allocation of the intervention study and individual risk factors such as body mass index, age, sex, lack of exercise and smoking. Based on the discussed theoretical background, unnecessary and unreasonable tasks are potential risk factors for musculoskeletal pain, and therefore, the hypotheses are directional and the test of hypotheses is one-directional. Thus, the alpha level was set to p < .05; one-tailed and unstandardized coefficients are reported.
Results
A total of 62 of 101 (61.4%) workers participated in this study. Nineteen employees (18.81%) could not participate because of the exclusion criteria and 20 (19.80%) chose not to participate for other reasons (e.g., no time). All participants filled out the daily questionnaire in the first week of the study. Thirty-six participants filled out the daily questionnaire in the four following weeks. Because of completely missing daily reports (four participants) or the existence of only one daily report (one participant), as well as complete missing of the general questionnaire (two participants) the final sample size in this study was 55 (29 male; mean age = 41.96, SD = 14.2 years) on Level 2 of the data and with 742 daily reports on Level 1 of the nested data structure.
Forty-six (83.6%) participants did not smoke, 20 (36.4%) reported exercising/doing sports for three to seven days a week, while 35 (63.7%) reported exercising/doing sports more than once a week (Table 1).
Demographic and Work Characteristics of Office Worker Participants (N = 55)
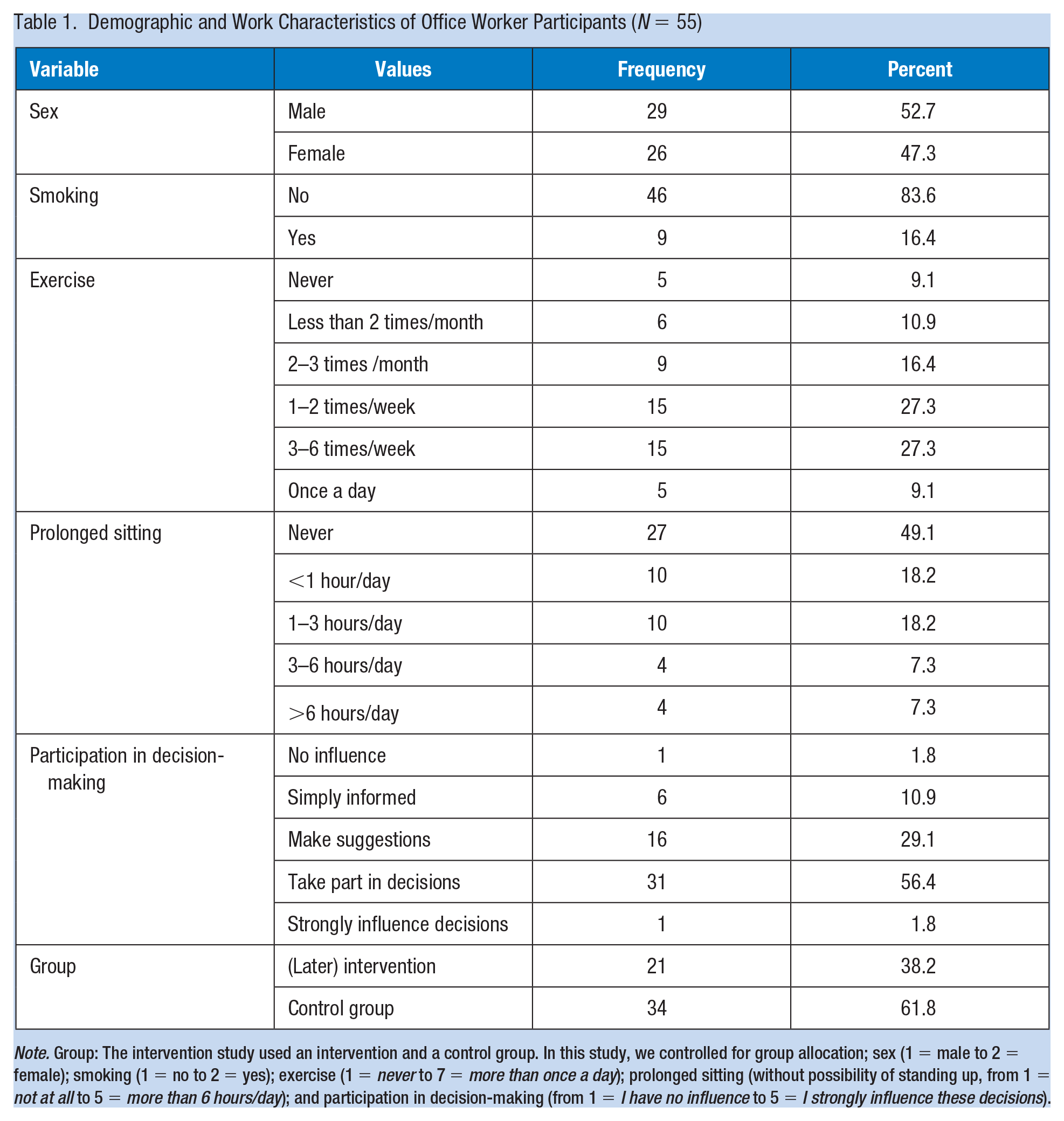
Note. Group: The intervention study used an intervention and a control group. In this study, we controlled for group allocation; sex (1 = male to 2 = female); smoking (1 = no to 2 = yes); exercise (1 = never to 7 = more than once a day); prolonged sitting (without possibility of standing up, from 1 = not at all to 5 = more than 6 hours/day); and participation in decision-making (from 1 = I have no influence to 5 = I strongly influence these decisions).
On a scale of 0 to 100, the mean level of musculoskeletal pain across 742 person-days was 10.7 (SD = 15.7, Table 2). Mean levels of unnecessary tasks (M = 2.53, SD = 0.80) were higher than mean levels of unreasonable tasks (M = 1.78, SD = 0.67). Unnecessary tasks were positively correlated with musculoskeletal pain (r = .29). Correlations between unreasonable tasks and musculoskeletal pain were slightly lower (r = .18). Prolonged sitting (without possibility of standing up) was common among the employees. Half of the sample reported that this was common while the remaining participants reported that they could, for example, use stand-up desks or alternate between sitting and standing. Musculoskeletal pain was also positively related to prolonged sitting (r = .14) while the association with participation in decision-making was unexpectedly positive (r =0.09). More intense maladaptive beliefs corresponded to more frequent daily musculoskeletal pain = (r = .18).
Measures of Pain, Unnecessary, and Unreasonable Tasks in Office Worker Participants (N = 55)
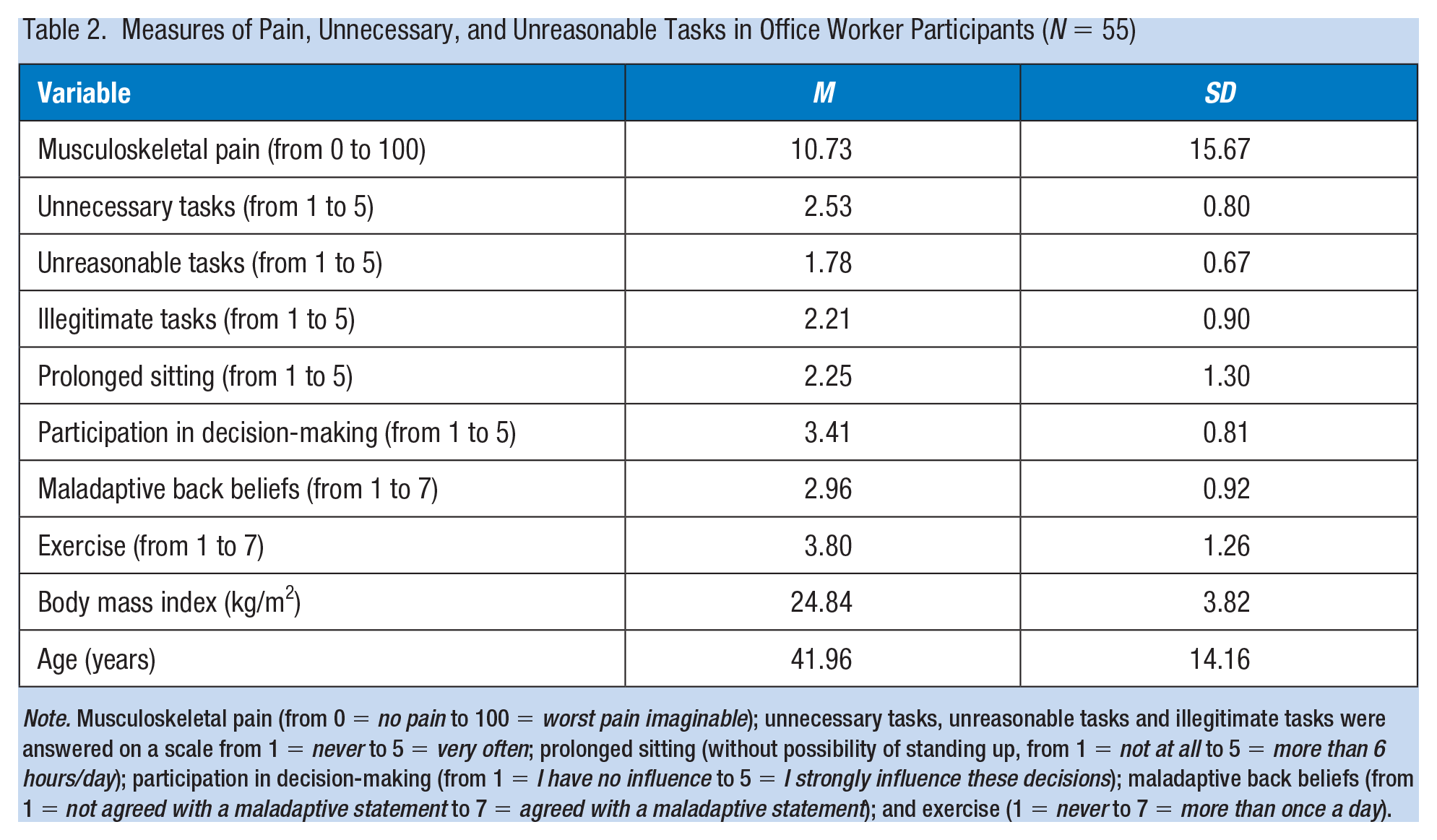
Note. Musculoskeletal pain (from 0 = no pain to 100 = worst pain imaginable); unnecessary tasks, unreasonable tasks and illegitimate tasks were answered on a scale from 1 = never to 5 = very often; prolonged sitting (without possibility of standing up, from 1 = not at all to 5 = more than 6 hours/day); participation in decision-making (from 1 = I have no influence to 5 = I strongly influence these decisions); maladaptive back beliefs (from 1 = not agreed with a maladaptive statement to 7 = agreed with a maladaptive statement); and exercise (1 = never to 7 = more than once a day).
Table 3 provides the results of three multilevel regression analyses with musculoskeletal pain as outcome. For unnecessary tasks, unreasonable tasks, and illegitimate tasks, higher body mass index and smoking were positively related to higher musculoskeletal pain while age, sex, and group membership were not related. Unnecessary tasks were a significant predictor of daily musculoskeletal pain (first model: B = 4.27, p = .006), while unreasonable tasks were not (second model: B = 3.05, p = .074). When unnecessary and unreasonable tasks were merged into a single illegitimate tasks scale, illegitimate tasks were a significant predictor of musculoskeletal pain (third model: B = 2.63, p = .045). Prolonged sitting was a significant risk factor with unnecessary tasks (first model: B = 2.06, p = .039) but did not reach significance for unreasonable tasks and illegitimate tasks. Maladaptive back beliefs were a strong risk factor for daily musculoskeletal pain with unnecessary tasks (first model: B = 3.78, p = .003), unreasonable tasks (second model: B = 3.38, p = .007), and illegitimate tasks (third model: B = 4.07, p = .003). Participation in decision-making was not a significant protective factor for musculoskeletal pain.
Regression Analysis of Daily Musculoskeletal Pain for 742 Working-Days Among Office Workers (N = 55)
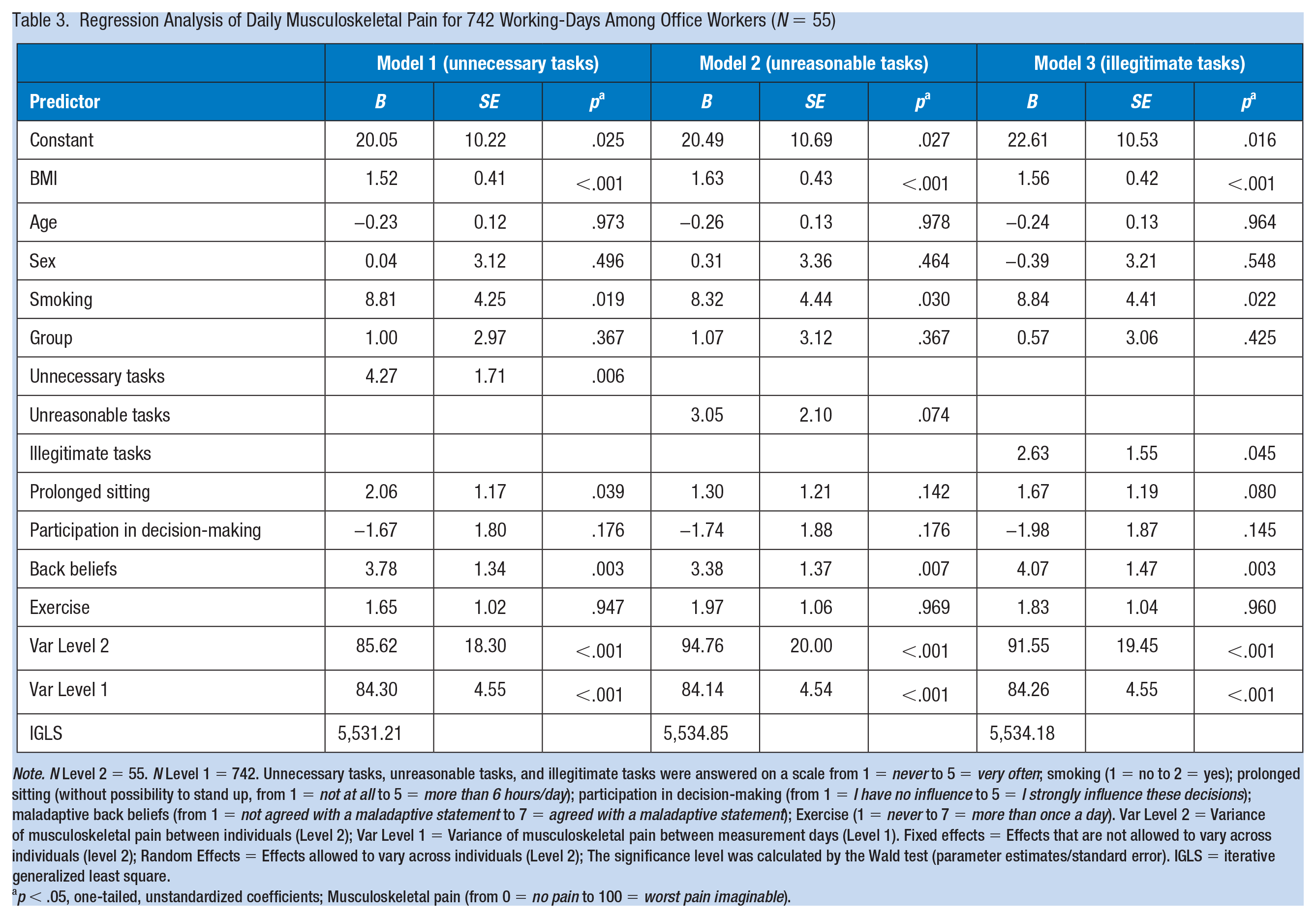
Note. N Level 2 = 55. N Level 1 = 742. Unnecessary tasks, unreasonable tasks, and illegitimate tasks were answered on a scale from 1 = never to 5 = very often; smoking (1 = no to 2 = yes); prolonged sitting (without possibility to stand up, from 1 = not at all to 5 = more than 6 hours/day); participation in decision-making (from 1 = I have no influence to 5 = I strongly influence these decisions); maladaptive back beliefs (from 1 = not agreed with a maladaptive statement to 7 = agreed with a maladaptive statement); Exercise (1 = never to 7 = more than once a day). Var Level 2 = Variance of musculoskeletal pain between individuals (Level 2); Var Level 1 = Variance of musculoskeletal pain between measurement days (Level 1). Fixed effects = Effects that are not allowed to vary across individuals (level 2); Random Effects = Effects allowed to vary across individuals (Level 2); The significance level was calculated by the Wald test (parameter estimates/standard error). IGLS = iterative generalized least square.
p < .05, one-tailed, unstandardized coefficients; Musculoskeletal pain (from 0 = no pain to 100 = worst pain imaginable).
Discussion
In this pilot study, we tested risk factors for daily musculoskeletal pain in sedentary office work and for the first time tested the new concept of illegitimate tasks as a risk factor for daily musculoskeletal pain. We confirmed the first hypothesis in finding that unnecessary tasks predicted the daily intensity of musculoskeletal pain at work, even when other known risk factors were controlled in analyses.
Interestingly, the effects of unreasonable tasks on musculoskeletal pain were not significant. This was surprising given the theoretical background of the SOS model, which postulates a potentially even greater risk to the employees’ self-worth from unreasonable than from unnecessary tasks (Semmer et al., 2007, 2019). In the prediction of daily musculoskeletal pain, unnecessary tasks had a bigger impact on musculoskeletal pain than unreasonable tasks. Small variance in unreasonable tasks might have contributed to low association with musculoskeletal pain. Unnecessary tasks were more common than unreasonable tasks in the federal administration setting and in the current sample the standard deviation of unreasonable tasks was smaller than that of unnecessary tasks.
As repeated strain results in long-lasting muscle tension (Lundberg & Melin, 2002), the higher frequency of unnecessary tasks could make them especially hazardous for musculoskeletal pain. In addition, unnecessary tasks are maybe harder to combat than unreasonable tasks, as they leave less opportunity for reappraisal, reframing, and interpretation (Fila & Eatough, 2019). In the employer’s view, the negative effects of unnecessary tasks might be easily underestimated (“Everyone needs to do unnecessary tasks from time to time . . .”). Thus, unnecessary tasks often stay unchanged even when discovered.
The risk of prolonged sitting for musculoskeletal pain somehow depended on whether unnecessary or unreasonable tasks were included in the regression model and remains inconclusive. Participation in decision-making was proposed to be a work-related protecting factor for musculoskeletal pain, but was unexpectedly found to be unrelated to musculoskeletal pain.
Maladaptive back beliefs were confirmed as a strong individual risk factor (Elfering et al., 2015). These findings suggest that occupational health promotion should focus on cognitive behavioral pain approaches (Rolli Salathé et al., 2018). Although, well-constructed self-reports can predict a wide range of outcomes with ease and efficiency (Paulhus & Vazire, 2007), future studies should also include observer data because of response bias in self-reports (Semmer et al., 2004). In addition, there are slightly different wordings for unnecessary (“which keep you wondering”) and unreasonable (“which you believe”) tasks. “Believe” might implicate a stronger attitude than “wonder” and could result in less agreeing responses for unreasonable tasks. Also, our prolonged sitting scale was not distinctive, if participants had exact three hours of prolonged sitting a day. If so, participants might have answered with 1 to 3 hours a day or with 3 to 6 hours a day. Multiple item measures are known to have better psychometric properties than single-item measures (Fisher et al., 2016). However, the VAS item to assess musculoskeletal pain has stand-alone quality in comparison with multi-item questionnaires (Hawker et al., 2011) and has been shown to be psychometrically satisfying with respect to reliability and validity within pain self-reporting measures (Häfeli & Elfering, 2006). Finally, there may be a potential bias from the study context, as the study was set originally as an intervention study. The waiting control group might have been questioning the reason for daily reports of their musculoskeletal pain, especially when they had experienced no pain. But the response rate for the daily questionnaire was 44% (742/1,650), which is comparable with Sugiura et al. (2011), who reported response rates ranging from 40.1% to 47.3% in a web-based daily questionnaire for health (WDQH).
Implications for Occupational Health Practice
Because unnecessary tasks were significant predictors of musculoskeletal pain, we advise supervisors to avoid unnecessary tasks whenever possible. When certain unnecessary tasks need to be done, we recommend that justification for the task should be explained to the employee. Work redesign that reduces unnecessary tasks can make a valuable contribution to the prevention of musculoskeletal pain in employees. In addition, we recommend a reduction in sitting time (e.g., stand-up desks) or to enhance more dynamic sitting behavior (Bontrup et al., 2019) and suggest educational and worksite training interventions for back muscle functioning and body balance (Elfering et al., 2014). Thun et al. (2018) showed that administrative tasks are often experienced as illegitimate, and found an association between administrative work and sickness presenteeism in physicians. Further studies should focus on illegitimate tasks and musculoskeletal pain among other occupations. Along with Fila and Eatough (2019), we recommend additional research to identify buffers of unnecessary tasks, because unnecessary tasks appear frequently and seem to be hard to combat.
Applying Research to Occupational Health Practice
Unnecessary tasks predicted the daily intensity of musculoskeletal pain at work, greater than other significant risk factors, such as prolonged sitting, body mass index, and maladaptive back beliefs. In the view of employers, the negative effects of unnecessary tasks might be easily underestimated (“Everyone needs to do unnecessary tasks from time to time . . .”). Thus, unnecessary tasks often stay unchanged even when discovered. Supervisors should be aware that assigning unnecessary tasks can have a negative impact on their employees’ health. Especially, the high frequency of unnecessary tasks could make them hazardous for musculoskeletal pain. It is recommended that supervisors avoid assigning unnecessary tasks whenever possible. However, sometimes unnecessary tasks just need to be done. In these instances, it is recommended that workers are provided with justification as to why the task needs to be done. Also, work redesign that reduces unnecessary tasks—for example, by improving software compatibility—can make a valuable contribution to the prevention of musculoskeletal pain in employees.
Footnotes
Authors’ Note
This study was presented at the 19th EAWOP congress, Torino, Italy, May 29 to June 01, 2019.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Yannik Faes (MSc) is a doctoral researcher in the field of work and organizational psychology. Along with other publications on work and health, this one is part of his doctoral thesis.
Achim Elfering (Prof. Dr. phil. nat.) is a professor and researcher in the field of work and organizational psychology. He has contributed a number of articles on the topic of occupational health, work stress, and work safety.