
Abstract
Background: Mitigating bloodborne pathogen exposure (BBPE) risk among healthcare workers is a major focus of hospital-based occupational health programs. The COVID-19 pandemic has placed added demands on occupational health services for healthcare workers. Its impact on BBPE incidence is unreported. Methods: As part of quality improvement efforts, we examined BBPE case incidence at two affiliated health centers during a 24-month period, 12 months preceding and following the COVID-19 pandemic onset. We used Year 1 to Year 2 change in incidence at the larger health center as the referent value to generate predicted incidence rates at the study health center. We tested the ratio of observed to predicted values at the study health center as a Poisson variable to its expectation. We defined a BBPE consistent with the Occupational Safety and Health Administration (OSHA) Bloodborne Pathogens Standard. Results: The BBPE case incidence at Health Center One (HC1), totaled 46 cases in Year 1, increasing 19% to 55 cases in Year 2. The cumulative incidence at Health Center Two (HC2), the referent facility, was 664 cases in Year 1, declining 24% to 503 in Year 2. The ratio of 55 events at HC1 to the expected incidence of 35, based on the experience at HC2, was 1.6 (p < .05). Discussion/Applications to Practice: The incidence of BBPE events at HC1 paradoxically increased during the COVID-19 pandemic, contrasting to the expected decrease that we observed at HC2. These data suggest that during times of increased stress to employee healthcare delivery from an infectious disease outbreak, the burden of ongoing practice demands may increase.
Keywords
Background
Mitigating bloodborne pathogen exposure (BBPE) risk among healthcare workers is a major programmatic focus of hospital-based occupational health programs. The ultimate goal of such programs is to mitigate the risk of transmission from patient to healthcare workers of human immunodeficiency virus (HIV), hepatitis C virus (HCV), and hepatitis B virus (HBV). The COVID-19 pandemic has placed considerable added demands on employee occupational health services for healthcare workers, superimposed on ongoing BBPE response needs. We hypothesized, however, that the incidence of BBPE events would decrease in the midst of a concomitant rise in COVID-19 cases because of fewer elective procedures, a reduction in other non-COVID-19 in person clinical encounters, and the increased usage of healthcare services via telehealth. We tested whether this hypothesis was supported by observation through analysis of BBPE case incidence at two affiliated healthcare centers over the 12 months preceding the COVID-19 pandemic and comparing this with the 12 months following the onset of the pandemic.
Methods
Study Sites and Observation Period
We defined BBPEs consistent with the Occupational Safety and Health Administration (OSHA) 2001 Bloodborne Pathogens Standard (BPS) as “a specific eye, mouth, other mucous membrane, nonintact skin, or parenteral contact with blood or other potentially infectious materials that results from the performance of an employee’s duties” (OSHA, 1910.1030). This pertains to whether the case required first aid or not, as mandated in the OSHA Recordkeeping Standard (OSHA 1904). Furthermore, cases were considered for inclusion regardless of the source patients’ status and the healthcare workers’ employment status (i.e., salaried employee or other status, such as trainee). Each health center’s BBPE database, which forms the basis of their Sharps’ Injury Logs, was reviewed for case identification and data collection.
HC1, the study center, is a Veterans Affairs Healthcare System encompassing outpatient clinics and home care services forming a network at multiple sites and inpatient wards and emergency services at a single site. HC2 served as the referent facility in this analysis. It is a large tertiary care university center in the same geographic region and with which HC1 has an academic affiliation. The BBPE hotline services at both HC1 and HC2 organize and coordinate their services similarly. We studied case incidence over the same 24-month period at both sites: the 12 months immediately preceding the COVID-19 pandemic, from March 2019 through February 2020 (Study Year 1), and the 12 months that followed (Study Year 2, March 2020 through February 2021), the latter subsuming the bulk of the pandemic period prior to effective immunization, a period which also includes the initial shelter-in-place orders for the region.
Applications to Professional Practice
Occupational health professionals during times of pandemics, as in other periods, should expect and plan for increased work injuries and illnesses due to additional stressors. Best practices may include the following:
Continuing data collection for BBPEs and other occupational health services to identify and evaluate trends.
Understanding results of such evaluations can be useful to determine prevention measures that need to be developed or enhanced.
Collaborating with colleagues in your geographic region can support this process to identify trends that may be similar or dissimilar. Practices can then be shared for purposes of quality and service improvement.
Considering resilience and supporting resources to offer healthcare workers during such times to lessen the adverse medical and psychological outcomes of stress and burnout.
Furthering research related to the COVID-19 pandemic and its effects on work injuries and illnesses.
Data Sources and Case Definition
As noted preciously, we identified BBPE cases through the telephone hotline databases from HC1 and HC2 covering the study period of interest. We reviewed each hotline call logged to ensure it pertained to a BBPE exposure (whether via splash, needlestick, bite, cut, or other relevant mechanism, as defined previously) and not some other query unrelated to a BBPE event (in particular, COVID-19 questions in the second half of the study period misdirected to this hotline from either health center). We did not, however, exclude cases for which ultimately it was concluded that the BBPE scenario did involve a substantive risk, for example, contact to intact skin or a stick from an unused needle. We created a separate database for the purposes of this analysis cleansed of personal identifiers. The core variables retained in this file were month and year of the reported case and location of the exposure (HC1 or HC2).
Statistical Analysis
We tallied the call incidence at each site by month and study period. Within HC1 and HC2, respectively, we calculated the ratio of monthly BBPE cases reported in Study Year 2 to Study Year 1, as well as the ratio for the sum of the entire 12-month periods. Thus, the study and referent health centers each yielded 12 monthly incidence values and one summary measure for the two study years. We assessed the differences between the number of ratios that were less than 1.0 (reflecting a decrease in Year 2 relative to Year 1) at HC1 versus HC2 using Fisher’s exact test. We tested whether the incidence ratios within the study site (HC1) of Study Year 2 to Study Year 1 differed statistically from unity (1.0), month by month and summed over the 12-month period, based on an observed Poisson variable to its expectation and assuming that the baseline year was the expected frequency. We carried out a further analysis using the ratio of Study Year 2 to Study Year 1 at HC2 as the expected proportional change in incidence for HC1. For this analysis, we calculated the expected number for HC1 over Year 2 by multiplying the HC2 ratio times the actual observed number of events in HC1 in Year 1. For example, if the incidence at HC2 decreased from a baseline month in Study Year 1 with a ratio 0.8 and the incidence at HC1 was 10 cases in that month in Study Year 2, the expectation would be reduced to only eight cases (0.8 × 10). We tested this expected incidence in a new set of ratios of observed to expected counts. We tested differences in the ratios of all observed to expected values based on the Poisson distribution. We did not correct for multiple comparisons. We specifically limit the term “expected” throughout this report to refer only to expected in the sense of the Poisson analyses described.
As part of ongoing quality control activities that did not include a formal consent process, we analyzed data we had collected as a part of ongoing clinical activities to examine the incidence of BBPE events at two affiliated healthcare centers using similar telephone hotline notification and follow-up protocols. The report was reviewed at the lead institution and deemed a nonresearch activity.
Results
The BBPE case incidence at HC1 totaled 46 cases in Study Year 1, increasing 19% to 55 cases in Study Year 2. The cumulative incidence at HC2, the referent facility, was 664 cases in Study Year 1 declining 24% to 503 in Study Year 2. The incidence of BBPE calls by site and by study month and year is presented in Figure 1. The incidence of BBPE cases at HC1 increased or stayed the same in seven out of the 12 months during Study Year 2 compared with Study Year 1. In contrast, the incidence of BBPE cases at HC2 decreased in 10 out of the 12 months during the same period.
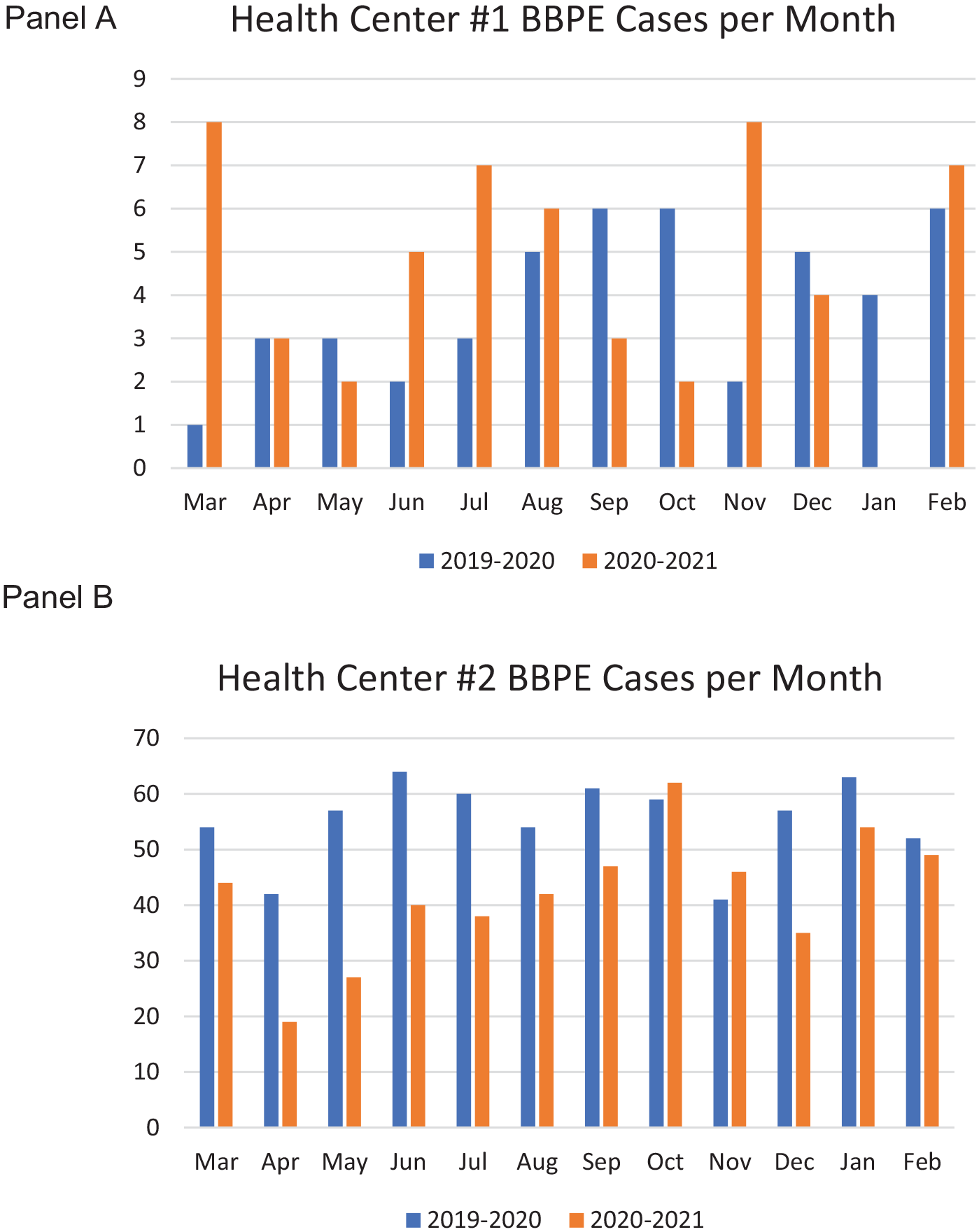
Panel A. Bloodborne pathogen exposure (BBPE) cases at Health Center 1, March through February 2019–2020 and 2020–2021. Panel B. Bloodborne pathogen exposure (BBPE) cases at Health Center 2, March through February 2019–2020 and 2020–2021.
The incidence rate ratios of Study Year 2 to Study Year 1 are illustrated in Figure 2. This shows that the ratios at HC2 were less than or close to a value of 1.0 with a dominant pattern of a decrease. The values at HC1, in contrast, fluctuated over time but the majority were above the ratios observed for HC2. The difference in the proportion of decreased months for HC1 (5 of 12, 42%) was half that of HC2 (10 of 12 months, 84%) but this difference was not statistically significant (p = .089, Fisher’s exact test).
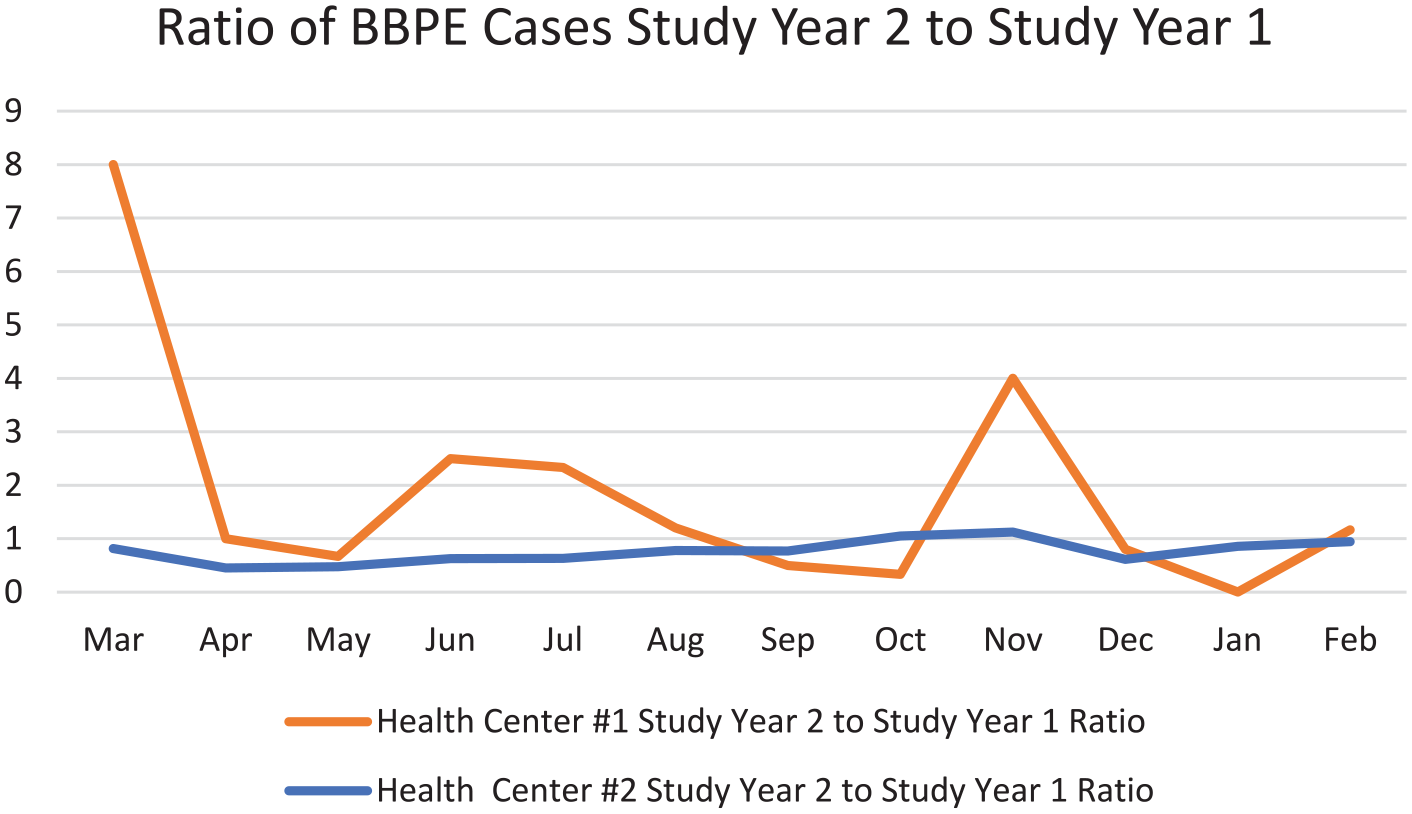
Ratio of bloodborne pathogen cases from Study Year 2 (March–February 2020–2021) to Study Year 1 (March–February 2019–2020) at each of the two Health Centers studied.
The composite annual and monthly observed BBPE case incidence for HC1 shown in Table 1 also presents two ratios of observed to previous or expected incidence. Ratio 1 is that of the incidence for HC1 in Year 2 to Year 1, the baseline pre-COVID-19 year. Ratio 2 is that of the incidence in Year 2 to the value expected based on the proportional change at HC2 in Year 2. Overall, the 55 cases in Year 2, as a ratio to the 46 from the baseline year, yield a value of 1.1, which is statistically nonsignificant. The ratio of 55 to the expected incidence of 35 (1.6) is statistically significant. Four of 12 months also had significant increased ratios to the expected values. For none of the months for which there was a ratio of less than 1.0 was that decline statistically significant.
Bloodborne Pathogen Exposure Cases at Study Health Center 1, and Expected Incidence Based on Referent Health Center 2
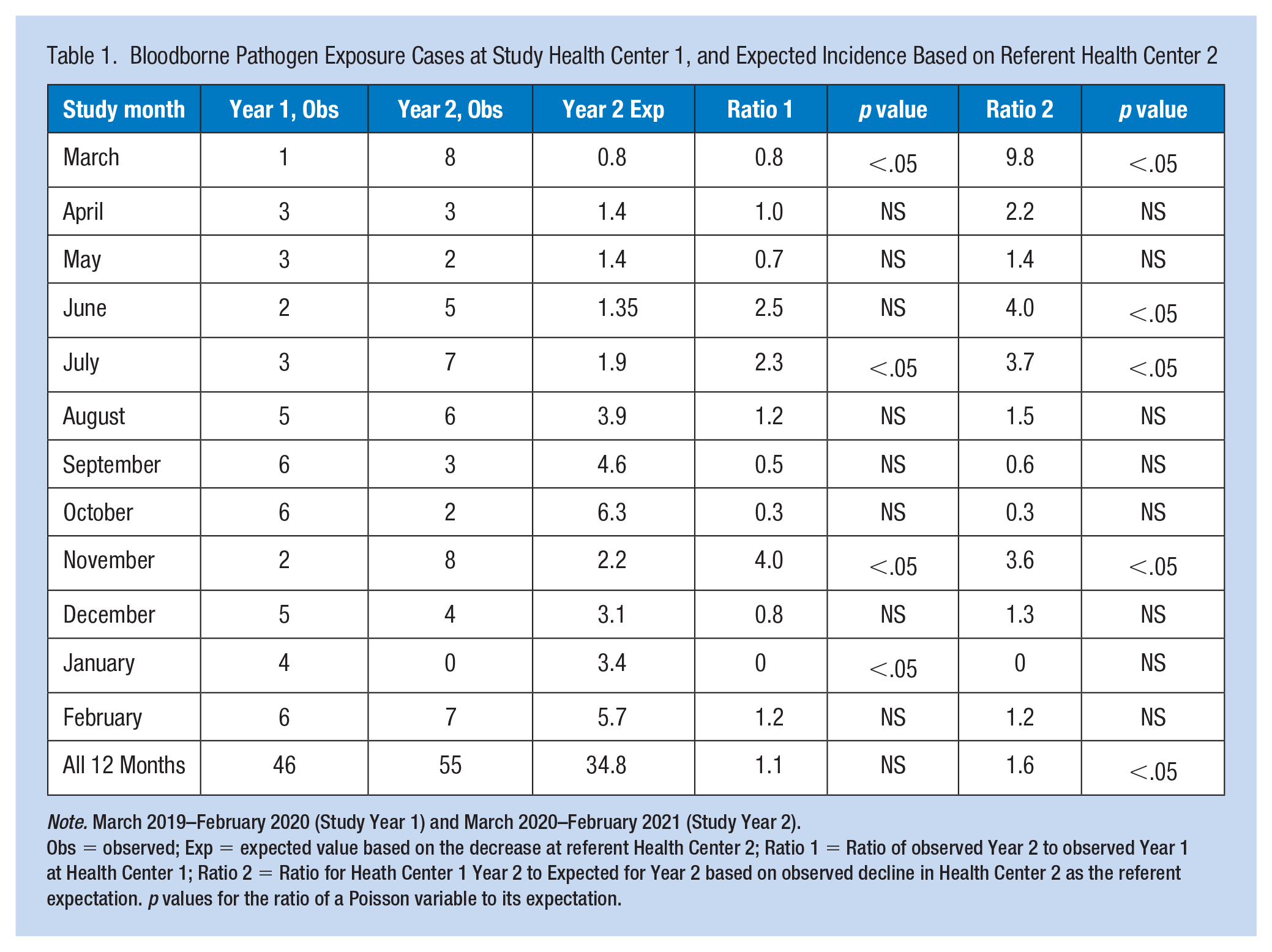
Note. March 2019–February 2020 (Study Year 1) and March 2020–February 2021 (Study Year 2).
Obs = observed; Exp = expected value based on the decrease at referent Health Center 2; Ratio 1 = Ratio of observed Year 2 to observed Year 1 at Health Center 1; Ratio 2 = Ratio for Heath Center 1 Year 2 to Expected for Year 2 based on observed decline in Health Center 2 as the referent expectation. p values for the ratio of a Poisson variable to its expectation.
Discussion
We observed an increase in BBPE incidence at HC1 during the first 12 months of the COVID-19 pandemic compared with the previous interval that we did not hypothesize we would observe. This increase was manifested both in absolute terms and, more dramatically, juxtaposed with the referent HC2, which had a consistent decline in reported BBPE incidence over the period in question.
A study from a single medical center in Turkey with approximately 4,000 healthcare workers analyzed its experience with needlestick or sharps injuries reported for 2019 compared with 2021 (Diktas et al., 2021). During 2019, there were 112 reported needlestick or sharps injury events (27.7 per 1,000 workers) compared with 82 reported events (21.4 per 1,000 workers) in 2021, a decrease that was not statistically significant (p = .09). Of interest, there were 14 events among 295 medical interns in 2019, with no reports among a reduced workforce of 143 interns in 2020. A study that indirectly addressed bloodborne pathogen risk analyzed compliance with safe disposal of sharps at a single hospital in the United Kingdom based on 100 sharps containers audited in November 2019 (pre-COVID-19) and 125 audited in July 2020 during the pandemic (Hussain et al., 2020). Overfilling was noted with 56% of sharps containers in the first survey and only 17% in the second, which the authors interpreted as improved safety compliance in response to an educational training effort.
The EPINet Sharps Injury and Blood and Body Fluid Exposure Surveillance Research Group and the Massachusetts Sharps Injury Surveillance System (MSISS), which are from geographic areas beyond California, may also prove to be useful data sources for future analyses of the impact of COVID-19 on BBPEs among healthcare workers, given previous publications based on these systems (International Safety Center (EPINet), 2020; Massachusetts Department of Public Health, 2021).
The study of risk factors for BBPE, in general, has focused predominantly on safety training and the adoption of safety devices, neither of which changed at either site between Study Years 1 and 2. A systematic review of needlestick injuries among healthcare workers did identify that “workload” was a risk factor for a BBPE (Lee et al., 2017). On that basis, increased workload during the COVID-19 pandemic might account for an increased BBPE incidence. Increased workload among nursing staff as a result of the COVID-19 pandemic has been well-documented. For example, a study of intensive care unit nurses at six hospitals in the Netherlands quantified higher patient loads and Nursing Activities Scores in the COVID-19 period (Hoogendoorn et al., 2021). Perhaps as relevant, a single study reported that increased self-perceived stress was a risk factor for needlestick, sharps, and mucous membrane BBPE among nurses (Mehrdad et al., 2014). Perceived stress among healthcare workers has emerged as a major issue in dealing with the COVID-19 pandemic (Kuo et al., 2020) and increased stress has also been quantified physiologically (Rajcani et al., 2021).
Other studies of nurses found that night shift work was a risk factor for sharps and needlestick injury (d’Ettorre, 2017; d’Ettorre et al., 2020; Ferrario et al., 2021). We have no evidence, however, that the pattern of night shift work changed at either HC1 or HC2 during the COVID-19 pandemic. Another study, among internal medicine residents as opposed to nurses, found that fatigue was a prospective risk factor for motor vehicle injury but not BBPE, although the low personal accomplishment domain of burnout was related to BBPE (West et al., 2012). The general injury literature does support the hypothesis that a holistic construct of a multifactorial “safety climate” was associated with workplace injury risk. Research has not been reported, however, on changes to the safety climate overall among healthcare workers during the COVID-19 pandemic, although factors of distress and resilience came into play (Hines et al., 2021).
The requirements promulgated by OSHA subsume other factors that are relevant to BBPE mitigation, such as the use of engineering controls (sharps with safety devices), work practice controls (e.g., handwashing, labeling of contaminated containers, no recapping of needles), safe sharps disposal devices, personal protective equipment (e.g., gloves, goggles, face shields, gowns), utilization of “universal precautions” (i.e., treating all blood and body fluids as infectious for bloodborne pathogens), and training on all of these elements. Although we did not carry out an institutional-level analysis of these factors as might have mediated a temporal relationship to the COVID-19 pandemic, handwashing and personal protective equipment use should have increased at both the health centers studied.
This was a retrospective analysis whose limitations should be kept in view to better contextualize its findings. We do not have data providing direct insights into factors underlying the possible phenomenon of an increase in reported BBPE events during the COVID-19 pandemic as experienced by HC1. Our observational analysis of data collected relatively recently over the first 12 months of the COVID-19 pandemic experience had the advantage of timeliness in addressing a knowledge gap. However, the disadvantage existed of not having available the extensive set of variables that might be present in more extended, future studies. We analyzed data from only two health centers. Both were located in the same geographic area. Therefore, the findings may not be generalizable to other areas of the United States, especially those that experienced higher or lower COVID-19 rates during Study Year 2. In addition, in California where this study was based, the California OSHA has promulgated its own standards related to both BBPE and COVID-19 worker protection, both of which are applicable to the employees in HC2. In other states, and in Veterans Affairs facilities in California, Federal OSHA standards apply. Transportability of the findings outside the United States is likely to be even more limited. We have no data on perceived stress or workloads that may have differed between the two health centers.
Our presumption that HC2, even though larger, was an appropriate “referent” for comparison and thus serving as the basis for expected values in the Poisson analyses may be incorrect. We did not use any other data set to provide an alternative source of an “expected” incidence against which to test. We assumed that reported BBPEs reflected the true incidence of such events without temporal trends depressing or inflating the proportion of true events that were reported between the two study years. We lacked data on systematic under reporting of such incidents at both centers, even if stable over time. We also had not taken into account differences that may exist between the two health centers in such attributes as employee demographics, COVID-19 case incidence per capita, safety climate, training, or healthcare provider to patient ratios. We have no reason to suspect, however, that any differences changed systematically and divergently over the study period.
Our statistical analysis did not account for the variability inherent in the smaller observed numbers at HC1. The relatively low incidence, however, did preclude analyses stratified by subgroups of hospital employees by work areas, for example, among operating room or emergency department personnel, or by professionals such as nurses or physicians. Our COVID-19 pandemic study period did not include a substantial period of COVID-19 vaccination administration, which had been cited specifically as a potentially important source of healthcare worker needlestick injury (Persaud & Mitchell, 2021). Finally, we did not include “near misses” from which additional insights might have been garnered.
In summary, we report the observation of increased BBPE incidence reported at a single health center coincident with the first 12 months of the COVID-19 pandemic. If this observation is confirmed by others, it would suggest that BBPE incidence may reflect a collateral adverse manifestation of the general stress on health systems connected with the COVID-19 pandemic or may be related to other specific factors not studied in this analysis.
Applications for Professional Practice
Organizations and occupational health professionals, during times of pandemic, should expect and plan for a potential increase in work injuries or illnesses not directly related to the pathogen at hand. This may add an additional stressor to a healthcare system already operating under considerable strain. This may be true in the face of natural disasters such as hurricanes or earthquakes. Efforts to continue standard operations and data collection for BBPE and to provide other core occupational health services are important, especially during times of crisis. This is all the more true when the crisis is likely to place particular demands on existing employee health services, as COVID-19 unquestionably has done. Our data suggest that even in the midst of an ongoing pandemic, data can be utilized to identify and evaluate trends, informing practice. Such evaluation can identify prevention measures that should be developed or enhanced, respond to changing employee health staffing needs, or revise standing protocols, to cite a few examples. Collaborating with colleagues within a single geographic region and across regions also can support programmatic evaluation and improvement processes through identifying temporal trends that may be similar or dissimilar. Practices can then be shared for purposes of quality and service improvement. Another interesting consideration is that of resilience and supporting resources to offer healthcare workers during such times to lessen the adverse medical and psychological outcomes of stress and burnout. Further research related to the COVID-19 pandemic and its effects on work injuries and illnesses, specifically BBPEs would be useful.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project was supported in part by the National Institute for Occupational Safety and Health (NIOSH; T42OH008429) and Health Resources and Services Administration (HRSA; D33HP31668) training grants. The statements, findings, conclusions, views, and opinions contained and expressed herein are not necessarily those of University of California, San Francisco, or any of its affiliated or subsidiary entities or the Veterans Affairs Healthcare System.
Ethical Approval
As part of a Quality Improvement effort, this report was reviewed by the appropriate Designated Official at the SFVAHCS and found to be exempted, non-research.
Author Biographies
Matthew Kiok, MD MPH, is a recent graduate of the University of California San Francisco (UCSF) Occupational and Environmental Residency Program who led the quality improvement project upon which this report is based while on a rotation at the San Francisco VA Healthcare System (SFVAHCS) Employee Occupational Health Service (EOHS).
Sandeep Guntur, MD MPH, is acting medical chief of the San Francisco VA Healthcare System (SFVAHCS) Employee Occupational Health Service (EOHS) and assistant medical chief for the Compensation and Pension Program. He is also an associate professor at the University California, San Francisco (UCSF) School of Medicine (SOM)
Paul D. Blanc, MD MSPH, is chief of the Division of Occupational and Environmental Medicine at UCSF, where he is professor of Medicine and holds the endowed chair in Occupational Medicine.
Olga Lozato, RN, is a nurse within the Occupational Health Service (OHS) at UCSF. Her clinical duties include work with its bloodborne pathogen program.
Grace Domingo, RN, is a nurse within the Occupational Health Service (OHS) at UCSF. Her clinical duties include work with its bloodborne pathogen program.
Robert Kosnik, MD, DIH, is the medical director of the OHS at UCSF and clinical professor of Medicine at UCSF.
Chika E. Ugbaja, DNP-PMHN, FNP-APRN, is a nurse practitioner at the SFVAHCS EOHS.
Noreen Chan, FNP-APRN, is a nurse practitioner at the SFVAHCS EOHS.
Alan Ramos, ANP-APRN, is a nurse practitioner at the SFVAHCS EOHS.
Sandra Domeracki, MSN, FNP-APRN, FAAOHN, is a nurse practitioner at the SFVAHCS EOHS and associate professor at UCSF School of Nursing, Occupational and Environmental Health Nursing Program. Is also a fellow with AAOHN and active member for several years.