
Abstract
In Fall 2020, a female physical therapist (PT) developed mild changes in gait, infrapatellar tendon pain, and lateral patellar tracking. As a PT in good physical condition, she did not access her employer’s occupational health clinic but instead she self-treated. Two months after symptom onset and self-treatment, she was diagnosed with an intramuscular myxoma within her left vastus lateralis, the largest muscle within the quadricep. The employee was at risk of slips, trips, and falls as the mass grew. Due to the location and increasing size of the mass, the employee required surgical treatment. Healthcare workers, particularly those who provide treatment, are likely to self-treat rather than seek assistance from the occupational health professional. The employee was seen by a plastic surgeon for an unrelated medical condition which is when the myxoma was diagnosed. Further delay may have led to occupational injury associated with the balance and gait disturbances. Opportunity exists for the occupational health professional to provide a review of services, including screening for musculoskeletal changes associated with occupational injury such as those described herein. This is especially important among those healthcare workers who tend to self-treat.
Keywords
Introduction
A 52-year-old female physical therapist (PT) presented to a plastic surgery practice with back and shoulder pain and was prepared to undergo a reduction mammoplasty. The patient also complained of a relatively recent, slow growing mass on her left lateral thigh that she noticed interfered with the natural biomechanics of her walking pattern and was thus a fall risk. Changes in gait of unknown etiology threaten the health of workers as they pose the risk of slips, trips, and falls. This is especially true in this case where the worker had direct physical contact with patients throughout the work shift. Once diagnosed, an excisional biopsy was performed and histological analysis revealed an intramuscular myxoma.
Intramuscular myxomas are rare benign tumors, typically found in skeletal muscle with an incidence of 1:1,000,000 of population per year (Hashimoto et al., 1986; Yaligod & Ajoy, 2013). They are usually found in large muscle groups and are composed of fibroblasts and myxoid stroma (Nielsen et al., 1998; Yaligod & Ajoy, 2013). Intramuscular myxoma is most frequently diagnosed in females (57%) between 40 and 70 years old (Gump & Gadre, 2013). Similar to this employee, the condition often goes undiagnosed. While the etiology of intramuscular myxomas remains elusive, it is thought to be a combination of environmental and genetic factors. In fact, 36% of intramuscular myxomas contain an activating mutation in the GNAS1 gene; a gene involved in many metabolic and regulatory signaling pathways and hence mutations within this gene are frequently implicated in tumorigenesis (Walther et al., 2014).
The typical presentation is a slowly enlarging mass in 64% of patients (Petscavage-Thomas et al., 2014). The lesion is a deeply seated mass confined to skeletal muscle and without malignant potential. A painful mass will be present in 55% of patients (Gump & Gadre, 2013; Pichierri et al., 2010). Myxomas have been reported to range in diameter from 1 to 17 cm (Vattemi et al., 2020). Intramuscular myxomas can be solitary or multiple. When multiple myxomas are present, they are often associated with monostotic (single bone) or polyostotic (multiple bones) fibrous dysplasia; the combination of these conditions is known as Mazabraud syndrome (Majoor et al., 2019; Pichierri et al., 2010). Intramuscular myxomas can be located in any skeletal muscle group; however, they most commonly occur in the quadriceps (65%), hip adductors (35%), gluteus muscles (20%), gastrocnemius, and upper arm (Gump & Gadre, 2013; Pichierri et al., 2010).
A growing mass in a major muscle group has potential to increase the risks for slips, trips, and falls as the tumor grows and interferes with the function of the skeletal muscle (Menant et al., 2021). Thus, the occupational health implications of this condition and others like it are important. This case report is structured according to CAR (for CAse REports) E guidelines (Riley et al., 2017).
Patient/Worker Information
The employee was a 52-year-old female PT who typically performed numerous highly physical tasks with patients in the long-term acute care facility where she worked. Likely due to her specialized skill set as a PT, the employee noticed mild alterations with her gait; however, she was active and physically fit and able to compensate for this deteriorating situation by favoring her right (non-injured) leg, as well as via strengthening exercises and stretching. During this time, she did not contact the occupational health professional at her facility.
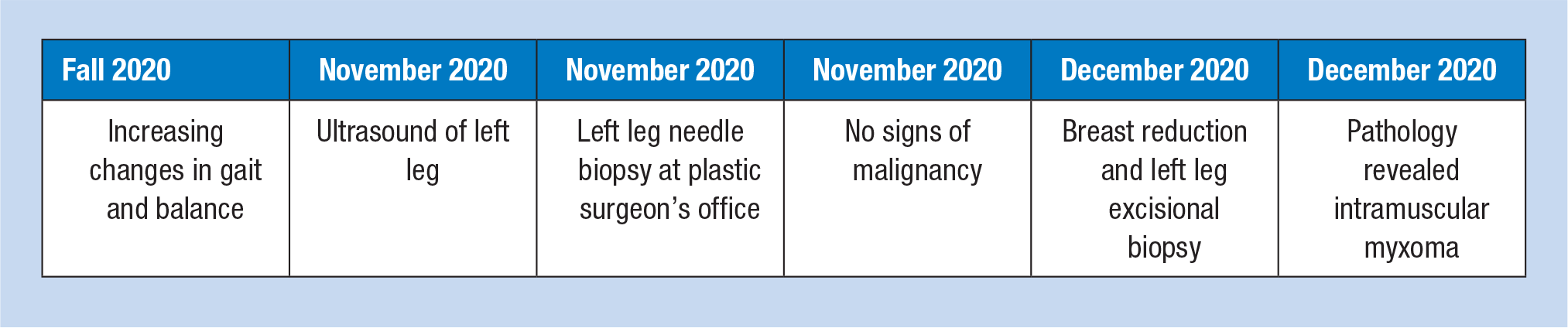
The employee recognized that she was experiencing infrapatellar tendon pain and lateral patellar tracking. At that time, she began self-treating with deep tissue kneading and massage. In fall 2020, 2 months after symptom onset, the mass was discovered by the patient after perceiving increasing changes in the biomechanics of her left leg while walking and exercising. By November 2020, changes were noticeable to the extent that she reported this as a secondary concern to her plastic surgeon when seeking an evaluation for reduction mammoplasty. The employee acquired information from her plastic surgeon about removal of the mass to prevent further gait changes.
Clinical Findings
The employee received a consultation with a plastic surgeon for a reduction mammoplasty and presented with mid-to-low back and shoulder pain. During consultation, the patient raised a secondary complaint of a recent onset of a solid round mass within her left thigh. Upon physical examination, the mass was palpable and moved along the axis of the muscle such that the mass’s relative location shifted between standing and sitting positions. The plastic surgeon recommended a needle biopsy (which could be performed by the plastic surgeon) to rule out malignancy. There is no relevant medical history or pertinent comorbidities to report.
Diagnostic Assessment
An ultrasound demonstrated a rounded hypoechoic mass with dimensions of 2.2 cm × 2.6 cm × 1.8 cm (Figure 1). A needle biopsy was preformed prior to resection under local anesthetic in the plastic surgeon’s office. A clear, viscous gel was aspirated. Histological evaluation of the specimen was limited due to the fragmented nature of the sample. Initial findings were inconclusive with possibility of benign intramuscular lipoma or a focus of fat necrosis, but more importantly ruled out malignancy.
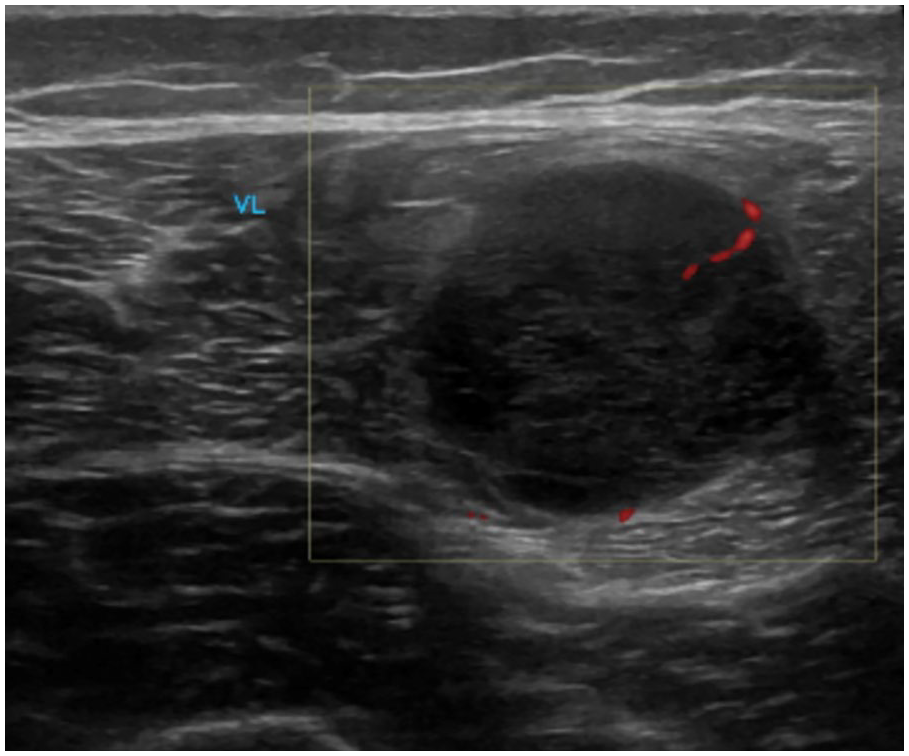
Focused ultrasound of the lateral mid left thigh revealing a 2.2 cm × 2.6 cm × 1.8 cm mass within the vastus lateralis muscle.
Therapeutic Intervention
The mass was resected by the plastic surgeon at the time of the reduction mammoplasty surgery. At the time of the resection, which was 5 weeks following the ultrasound, a 4 cm tumor was excised from within the vastus lateralis. The surgically excised mass was pearly white and appeared to be filled with a clear gelatinous material. The patient had no postoperative complications. Histological examination revealed the mass was an intramuscular myxoma. Surgical excision for intramuscular myxoma was curative.
Timeline
Discussion
It is likely that without the patient’s unique skill set and expertise as a PT this growth would have gone unnoticed until her gait was severely compromised. Intramuscular myxomas are typically found in large skeletal muscles, with the long axis of the mass aligned with the muscle fibers (Shi et al., 2020). However, they have also been found in the face and neck (Nisi et al., 2021). Intramuscular myxomas are detected more frequently in females. Intramuscular myxomas are characterized by hypocellularity, hypovascularity, and undifferentiated stellate cells (Luna et al., 2005; Nielsen et al., 1998; Shi et al., 2020). Due to their rarity, intramuscular myxomas are difficult to diagnose and final diagnosis can only be made with histological verification. In fact, both the nature of the ultrasound and the characteristics of the needle aspirate in this case coincide with other intramuscular myxoma in the literature (Yang et al., 2016). However, due to their rarity, these characteristics were not recognized by the radiologist, pathologist, or plastic surgeon. Furthermore, intramuscular myxomas, soft tissue perineuriomas, and low-grade fibromyxoid sarcomas have significant cytomorphological overlap and thus can be difficult to distinguish from needle biopsy evaluations (Yang et al., 2016). This case is consistent with the literature and provides an additional report and information on how these tumors may interfere with the biomechanics of the skeletal muscle. While changes in gait can be due to many other conditions ranging from neurological disorders to osteoarthritis, any change in gait increases the risk for trips and falls (Pirker & Katzenschlager, 2017). Furthermore, as intramuscular myxomas are not limited to the lower extremities, it is possible that tumors within other muscle groups, such as those in the upper arms, may also incur occupational health risks. For example, in occupations that require physical demands such as heavy lifting, a mass within the upper arm may hinder the natural biomechanics, interfere with balance, and lead to occupational injury. This case points to the need for occupation health nurses to engage in proactive conversations about their role to employees. It has been long established that medical professionals tend to self-treat, so the need for occupation health nurses to engage in proactive outreach is especially true for those who work with medical professionals. Workers who recognize gait and balance issues must be aware and feel comfortable accessing the occupation health nurse who may perform basic screening and referral, if necessary.
Worker Perspective
I began to notice lateral patellar tracking and infrapatellar tendon pain in Fall of 2020. I initially assumed that I could stretch and rest to ameliorate the situation, but I quickly realized that wasn’t the case. I then began to integrate massage and deep tissue kneading into my self-treatment regimen. I became concerned when my gait began to mildly change and [I] palpated a mass within my left thigh. I was already seeing a plastic surgeon for a reduction mammoplasty, so I thought I would probe at getting this mass excised too.
Informed Consent
The authors gained consent from the patient prior to writing this case report.
Conclusion
Changes in gait with unknown etiology are important to consider. Although many of these changes are due to osteoarthritis or neurological causes, changes in biomechanics of unknown etiology have the potential to be tumors within muscles. This case provides insight on how masses of unknown origin can cause gait changes. The patient noticed the change in her gait before any harmful incidents, but this case demonstrates that changes in gait with unknown etiology have the potential to be tumors. Excision of the tumor corrected these gait changes and therefore reduced the likelihood of trips or falls. Complete excision of myxomas carries an extremely low chance of tumor recurrence (Yaligod & Ajoy, 2013).
More importantly, within the context of occupational health and safety, alterations in biomechanics and gait may increase the risk of trips and falls (Gauchard et al., 2001; Menant et al., 2021). This patient, due to her specialized training as a PT, noticed these changes before an accident occurred. Real-life scenarios such as this reinforce the value the occupational health professional could have had in earlier intervention as a result of occupational screening associated with gait and balance changes. Barriers to occupational health and safety include a worker’s tendency to self-treat. Increasing awareness of the role of the occupational health nurse, which includes a discussion of self-treating musculoskeletal injuries/disorders, may best serve workers as they better recognize the value of the occupation health nurse and the occupational health program.
Continued Education Questions
Which of the following organ systems are involved in fall risks? Nervous System Muscular System Visual System All the above
Which of the following could provide explanation for a changed gait? Parkinson’s Disease Osteoarthritis Skeletal Muscle Tumors All the above
Gait changes, regardless of the etiology, may lead to the following reportable occupational injury. Generalized pain Slips, trips, or falls Changes in footwear Mood swings
Based on the article, which statement is thought to describe healthcare professionals who develop health issues that may impact occupational injury? There is a tendency to self-treat Delayed care There is no difference between employees regardless of healthcare background Both a. and b. are correct
Intramuscular myxoma is a rare disorder that is detected more frequently in females and is characterized by: Recurrence irrespective of intervention Hypocellularity, hypovascularity, and undifferentiated stellate cells Increasing limb weakness Systemic vascular damage
This article highlights an example of an opportunity for occupation health professionals to Encourage screening and employee health activities among employees Engage in interdisciplinary outreach among healthcare providers who serve employees Encourage medical professionals to self-treat Both a. and b. are correct
A myxoma is a noncancerous tumor that arises from connective tissue. The work-up for these tumors may include: Physical examination Ultrasound Biopsy All of the Above
The treatment of choice for myxomas is: Surgical excision Radiation therapy Chemotherapy Massage therapy
A patient presents to their family doctor, physical therapist, or occupational therapist with a change in gait. The healthcare professional should explore the following options with the patient: A recent injury (Trauma) Acute localized muscle strain (Stress) New skin or muscle tumors (Tumor) All of the above
When a patient presents to any healthcare professional, an acute change in their gait should be addressed by: Discussing the issue with the patient to procure additional information Ignoring the issue, since it does not pertain to the healthcare professional’s interest Immediate referral to a specialist, with no further inquiry or investigation by the initial healthcare professional Downplaying the acute issue as not important, as it will probably go away with time
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Madison A. Clements, BA, completed her undergraduate degree in neuroscience at the University of Colorado, Boulder. She is currently applying to medical school, with aspirations of melding a career of excellent patient care and public policy.
Susan Gallagher, PhD, MSN, MA, is associate editor for professional practice at Workplace Health & Safety. Her areas of professional interest are bariatrics, safe patient handling and mobility, skin and wound care, and policy ethics.
Glenn E. Herrmann is in private practice Plastic Surgery in Lafayette Colorado. As a Colorado native, he completed his initial undergraduate and medical training at the University of Colorado, and subsequently his advanced training at the University of Florida and the University of Illinois at Chicago. Outside of the office and operating room, Dr. Herrmann enjoys hiking, biking, skiing, entrepreneurialism, and time with his family.