
Abstract
Promoting the use of hearing protection devices (HPDs) can prevent noise-induced hearing loss (NIHL) among workers who are exposed to excessive noise. In the present study, the authors examine factors that may explain HPD use among industrial workers from 15 manufacturing plants in Thailand. Participants consisted of 268 randomly selected workers exposed to harmful noise levels for which routine HPD use was required. Logistic regression analysis of study variables revealed the most powerful predictors of HPD use were perceived hearing status (b = 0.66, p < .001) and interpersonal factors (i.e., role modeling and interpersonal support; b = 0.20, p < .001). Together, these variables correctly classified 63.4% of the cases. These findings have implications for interventions aimed at motivating workers to use HPDs regularly.
Noise-induced hearing loss (NIHL) is an occupational health problem in many countries (World Health Organization [WHO], 2004). In the United States, approximately 30 million workers are occupationally exposed to hazardous noise. Since 2004, the Bureau of Labor Statistics (BLS) has reported nearly 125,000 workers have suffered from hearing loss, and in 2009 alone, BLS reported more than 21,000 hearing loss cases (Occupational Safety and Health Administration [OSHA], 2016b).
Thai workers are also affected by this serious occupational problem. In 2014, the Thai Bureau of Occupational and Environmental Diseases (2014) reported 44,026 NIHL cases (74.29/100,000 workers). Noise-induced hearing loss is irreversible and progressive with continued exposure to excessive noise (Sataloff & Sataloff, 2006). In the United States, an estimated US$242 million is spent annually on workers’ compensation for hearing loss disabilities (OSHA, 2016a). Hearing loss may negatively influence workers’ quality of life and work life through impaired communication and diminished ability to communicate on the job (Dalton et al., 2003; Morata et al., 2005). According to the authors of one study (Choi et al., 2005), workers who had fair or poor hearing were nearly twice as likely as those workers without hearing loss to experience injuries.
Although engineering controls (e.g., redesigning equipment to eliminate noise sources and constructing barriers to prevent noise from affecting workers) and administrative controls (e.g., changing employees’ work schedules to prevent noise exposures) are preferred methods to reduce noise exposure (Centers for Disease Control and Prevention [CDC], 2014). However, these techniques may be impractical, costly, or scientifically impossible to implement in given work settings. Hearing protection devices (HPDs; e.g., earmuffs and plugs) are acceptable when engineering or administrative controls are not feasible to prevent hearing loss (OSHA, 2016b). To effectively prevent NIHL, HPDs must be used regularly, preferably all the time, when exposed to excessive noise (National Institute for Occupational Safety and Health [NIOSH], 1998). Studies in developed countries (i.e., the United States) determined that noise-exposed workers used HPDs only 14% to 49% of the time HPDs were required (Hong, 2005; Lusk, Kerr, & Kauffman, 1998; Seixas, Ren, Neitzel, Camp, & Yost, 2001).
Similarly, in Thailand, a literature review revealed that only 28.9% to 33.1% of noise-exposed workers in a food canning factory and lumber mills used HPDs every time they were exposed to hazardous noise (Tantranont, 2004; Tonchumporn, Chanprasit, & Songknam, 2008). The reported studies stressed the necessity of promoting HPD use among these vulnerable workers. To develop an effective intervention to increase HPD use, it is necessary to understand factors that influence this specific health behavior.
Researchers have reported a wide variety of factors affecting the use of HPDs. Lusk and colleagues conducted studies with factory workers (Kerr, Lusk, & Ronis, 2002; Lusk, Ronis, Kerr, & Atwood, 1994), construction workers (Lusk, Ronis, & Hogan, 1997), and farmers (McCullagh, Lusk, & Ronis, 2002) using Pender’s health promotion model (HPM) as a conceptual framework. Lusk et al. (1994) found that 50% of the variance in HPD use among workers in an automobile transmission plant was explained by perceived self-efficacy, perceived barriers, perceived benefits, job category, health competence, and situational factors. In another study by Lusk et al. (1997), 50% of the variance in HPD use among construction workers was explained by perceived value of use, barriers to use, self-efficacy for use, interpersonal modeling, and noise exposure. Kerr et al. (2002) found that perceived benefits minus barriers, definition of health, perceived health status, and hearing protection requirements had significant direct paths to the use of HPDs, and these together explained 50% of the variance in HPD use among Mexican American workers in three garment factories. McCullagh et al. (2002) found that interpersonal support, situational influences, and perceived barriers to HPD use explained 78% of the variance in HPD use among farmers.
Based on previous studies, Lusk and colleagues derived the predictors of use of hearing protection model (PUHPM) from the HPM (Hong, Lusk, & Ronis, 2005). In the PUHPM, the predictors of HPD use were divided into two categories: modifying factors (e.g., demographic factors, interpersonal influences, and situational factors) and cognitive-perceptual factors (e.g., benefits, barriers, and self-efficacy). This model was evaluated in three studies. Hong et al. (2005) found that 12% of the variance in HPD use among Black workers was explained by gender, noise level, and perceived benefits and barriers, whereas 36% of the variance in HPD use among White workers was explained by years working at a plant, noise level, perceived hearing, social norms, social modeling, interpersonal support, supervisor climate, perceived benefits, and perceived barriers. Raymond, Hong, Lusk, and Ronis (2006) found that 20% of the variance in HPD use among Hispanic workers was explained by age, noise level, and perceived benefits, whereas 37% of the variance in HPD use among non-Hispanic workers was explained by age, noise level, social norms, social modeling, interpersonal support, supervisor climate, and perceived benefits and barriers. Unfortunately, all these studies were conducted in the United States.
Only a few Thai studies were found in the literature. These studies showed that the most common factors that predicted HPD use were perceived susceptibility and severity of NIHL (Chaloemvipaht, 1998; Prechaworawet, 1992), perceived benefit, perceived self-efficacy, and the accessibility and availability of HPDs (Tonchumporn, 2008). Unfortunately, many potentially salient factors were not included in these studies. The purpose of the present study was to identify significant factors associated with the use of HPDS by Thai industrial workers.
Theoretical Framework
This study used the PUHPM (Hong et al., 2005) as the theoretical framework. The PUHPM was derived from the HPM and based on the results of previous studies of construction and factory workers (Lusk et al., 1997; Lusk et al., 1994). As presented in Figure 1, predictors of health-related behaviors were divided into two categories: modifying factors and cognitive-perceptual factors. Modifying factors included demographic/experiential factors, interpersonal influences, and situational factors. Cognitive-perceptual factors included benefits, barriers, and self-efficacy. Because the literature revealed that perceived susceptibility and severity of NIHL could predict the use of HPDs among Thai workers, these factors were added to the model for this study. As presented in Figure 1, all factors were found to have direct effects on the use of HPDs. The modifying factors also had an additional indirect effect on the use of HPDs, exerting influence through cognitive-perceptual factors.
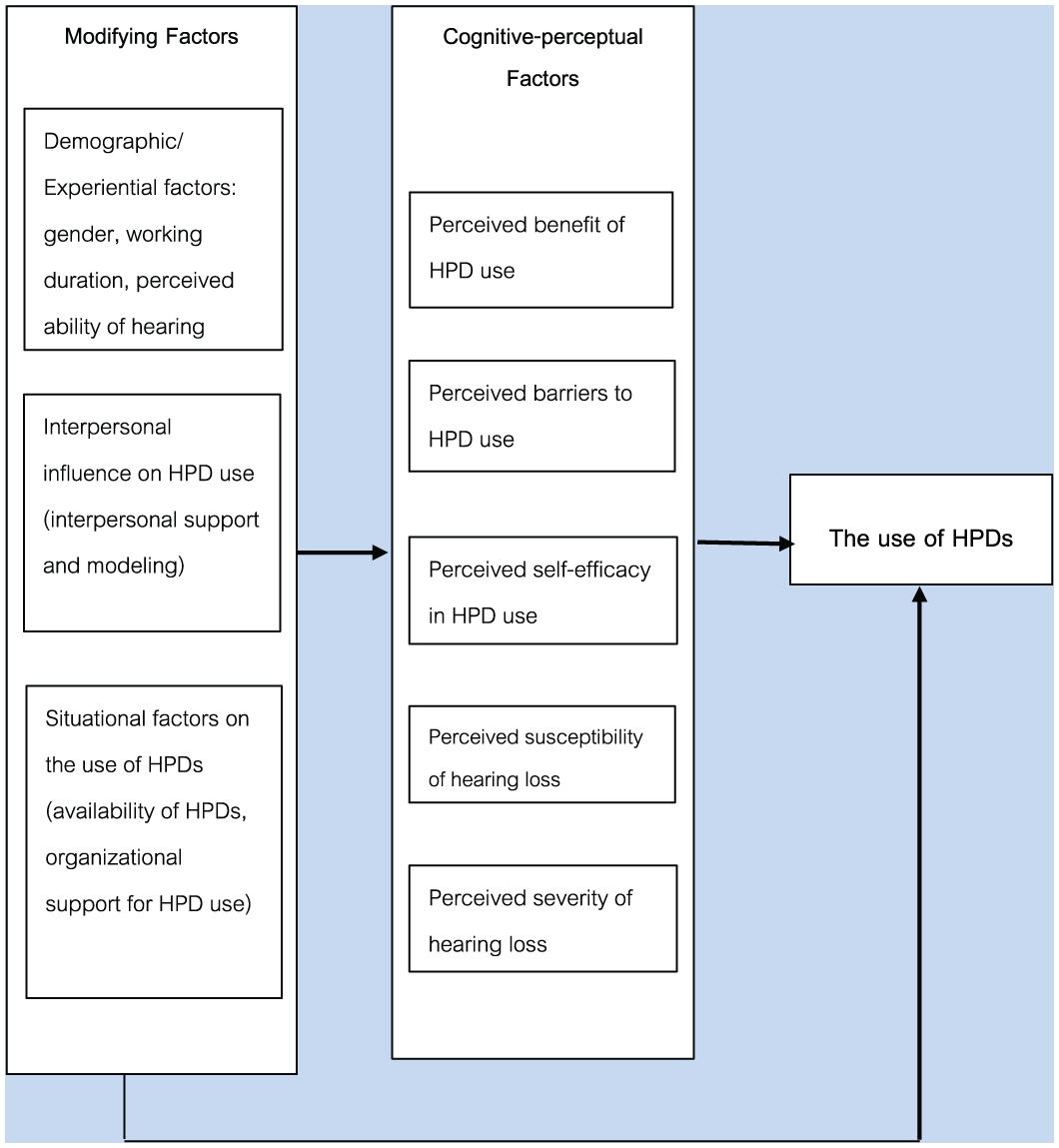
Predictors of industrial workers’ use of hearing protection model.
Research Design and Method
This study was approved by the Research Ethics Committee, Faculty of Nursing, Chiang Mai University in Chiang Mai, Thailand. Because noise levels of 80 dBA and above pose a hazard to workers (NIOSH, 1998), 15 manufacturing plants (i.e., two rib smoked sheet plants, five beverage plants, three frozen food manufacturing plants, a power plant, a palm oil manufacturing plant, a wood furniture factory, a plastic bottles plant, and an asphalt plant in Tharongchang district, Surajthanee Province) known to have noise levels above 80 dBA were selected for this study. After securing permission from the factories’ owners or managers, workers employed in high noise departments of manufacturing plants were recruited for the study. Inclusion criteria included workers who were (a) currently exposed to noise levels higher than 80 dB (A) over an 8-hour period, (b) able to read and write Thai, and (c) willing to participate in this study. A total of 850 workers were eligible for the study. A minimal number of 268 workers were randomly selected to participate from these factories.
Data Collection
Questionnaires were distributed directly to workers by a researcher, safety officer, or personnel resource staff member in study factories. Along with the questionnaire, the participants were provided study details and informed about study methods that were used to protect their privacy. The workers were also asked to sign consent forms and complete the survey individually after work. A token gift was given to the workers who returned their questionnaires.
Instruments
Demographic data were collected using single-item measures for gender, work duration, and self-reported perception of hearing status. Workers’ perceptions of their hearing were measured by responding to the question, “How good do you think your hearing is?” using a four-point Likert-type scale: 1 = excellent, 2 = good, 3 = fair, 4 = poor.
The use of HPDs was measured using a self-reported percentage of time (0%-100%) HPDs were used at work. Using HPDs was defined as wearing earplugs or earmuffs.
The instruments to measure study variables specific to HPD use in this study were derived from instruments developed for previous studies (Tantranont, 2009; Tantranont, Suthakorn, & Wisutthananon, 2013). A Likert-type scale, ranging from strongly agree to strongly disagree, was chosen for response.
Perceived Benefits of Hearing Protection scale was developed to measure concepts such as “preventing abnormal hearing” and “preventing noise annoyance.” Cronbach’s alpha for the original scale was .86 (Tantranont, 2009). Alpha coefficient for the revised scale was .83 (Tantranont et al., 2013). Examples of items to measure the benefits of HPD use included the following: “Using earplugs can prevent difficulty in hearing caused by loud noise” and “Using earplugs makes the worker happy when working because there is no disturbing noise.”
Perceived Barriers to Hearing Protection scale included two dimensions: personal discomfort and interference with communication. Alpha coefficient for the original scale was .92 (Tantranont, 2009), and for the revision scale was .88. Examples of items measuring perceived barriers are as follows: “Your ears hurt when using earplugs,” “You feel there is air pressure in your ears when using earplugs,” and “Using earplugs blocks the hearing of colleagues’ voices when they call me.”
Perceived self-efficacy in HPD use was measured by a scale developed to measure perceptions of workers’ capabilities to use HPDs correctly and manage barrier HPD use. Alpha coefficient for the scale in a previous study was .83 (Tantranont et al., 2011). Examples of items related to self-efficacy are as follows: “You can wear HPDs correctly” and “You can wear HPDs all the time during exposure to loud noise, even when you feel irritation in your ears.”
Perceived susceptibility to hearing loss was measured by two items: “You are at risk of NIHL” and “You are more at risk of NIHL than workers who are not exposed to loud noise.” Alpha coefficient for this scale was .89 (Tantranont et al., 2011).
Perceived severity of hearing loss included the perception of capability to use HPDs correctly and manage barriers to HPD use. Alpha coefficient for this scale was .89 (Tantranont et al., 2011). Examples of items related to severity of hearing loss included the following: “Hearing loss is irreversible” and “Hearing loss results in difficulty with communication.”
To measure interpersonal influences, a range of statements about social network and social support systems from primary groups in the workplace setting (i.e., coworkers and supervisors) that affect workers’ use of hearing protection were used. Alpha coefficient for the original scale was .90 (Tantranont, 2009), and for the revision scale was .88 (Tantranont et al., 2011). Examples of items related to interpersonal influences include, “Coworkers use earplugs every time when working in loud-noise areas” and “Supervisors regularly tell workers to use earplugs.”
Situational influences measures revealed the formal and informal organizational policies and functions that support or do not support workers’ use of hearing protection. Alpha coefficient for the original scale was .94 (Tantranont, 2009), and for the revision scale was .90 (Tantranont et al., 2011). Examples of items related to situational influences included the following: “The factory requires that workers use earplugs every time when working in loud-noise areas” and “Every worker who is working in loud-noise areas receives earplugs.” The scales, number of items, mean scores, and Cronbach’s alpha coefficients for these samples are listed in Table 1.
Scales, Number of Items, Mean Scores, and Cronbach’s Alpha Coefficients (n = 11)
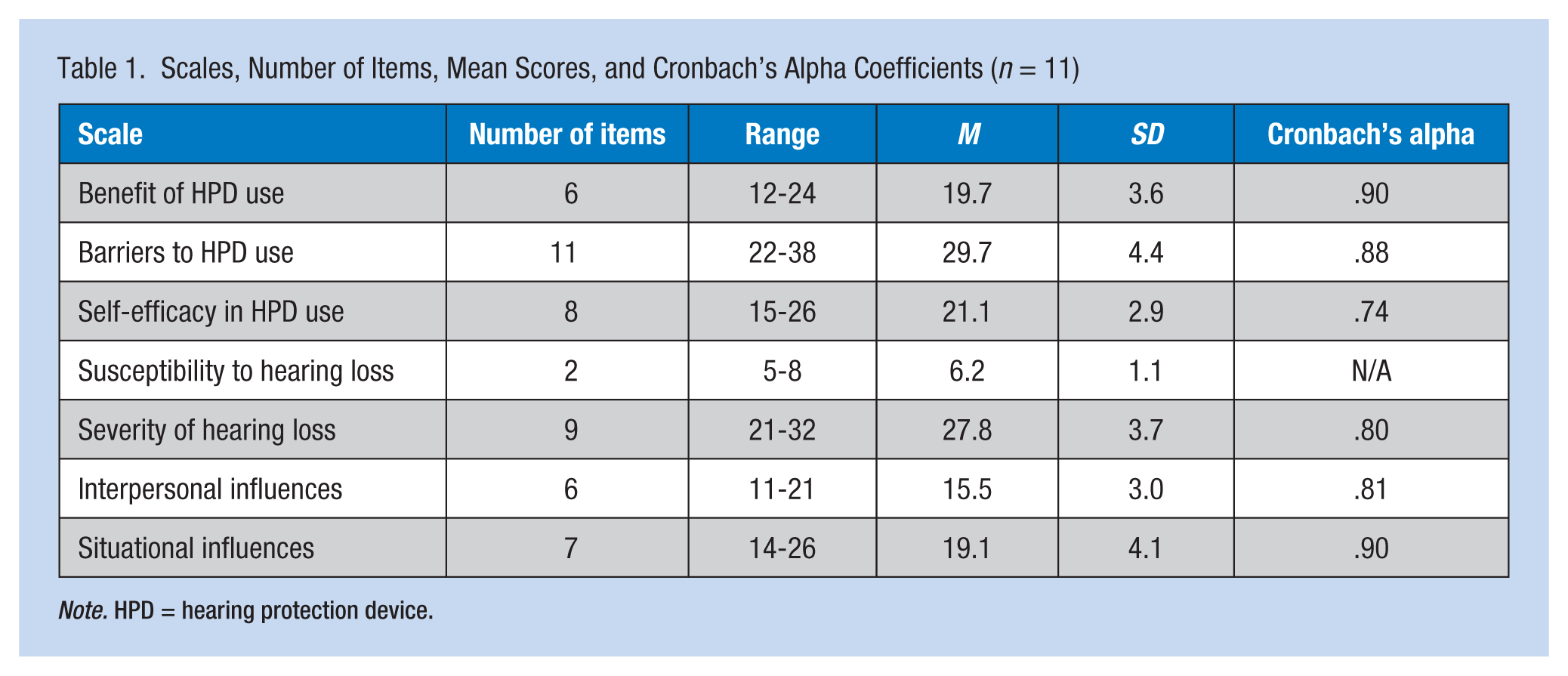
Note. HPD = hearing protection device.
Data Analyses
Demographic characteristics were analyzed using descriptive statistics. Because the distribution of the dependent variable violated assumptions for multiple regression, logistic regression was used. Percentage of HPD use was dichotomized into nonuse (<90%, coded zero) and ever-use (≥90%, coded 1).
Results
The average age of participants was 35.4 years (SD = 8.3 years), and mean years of experience in their factories was 7.3 years (SD = 7.0 years). Male and female participants were 54.9% and 45.1% of the sample, respectively. The majority of participants reported their hearing was good (67.2%). On average, participants reported use of HPDs 77.9% of the time they were exposed to loud noise (SD = 29.4). A majority of participants (90.7%) reported that they used earplugs (85.2%) and earmuffs (14.8%). Results are displayed in Table 2.
Logistic Regression for HPD Use
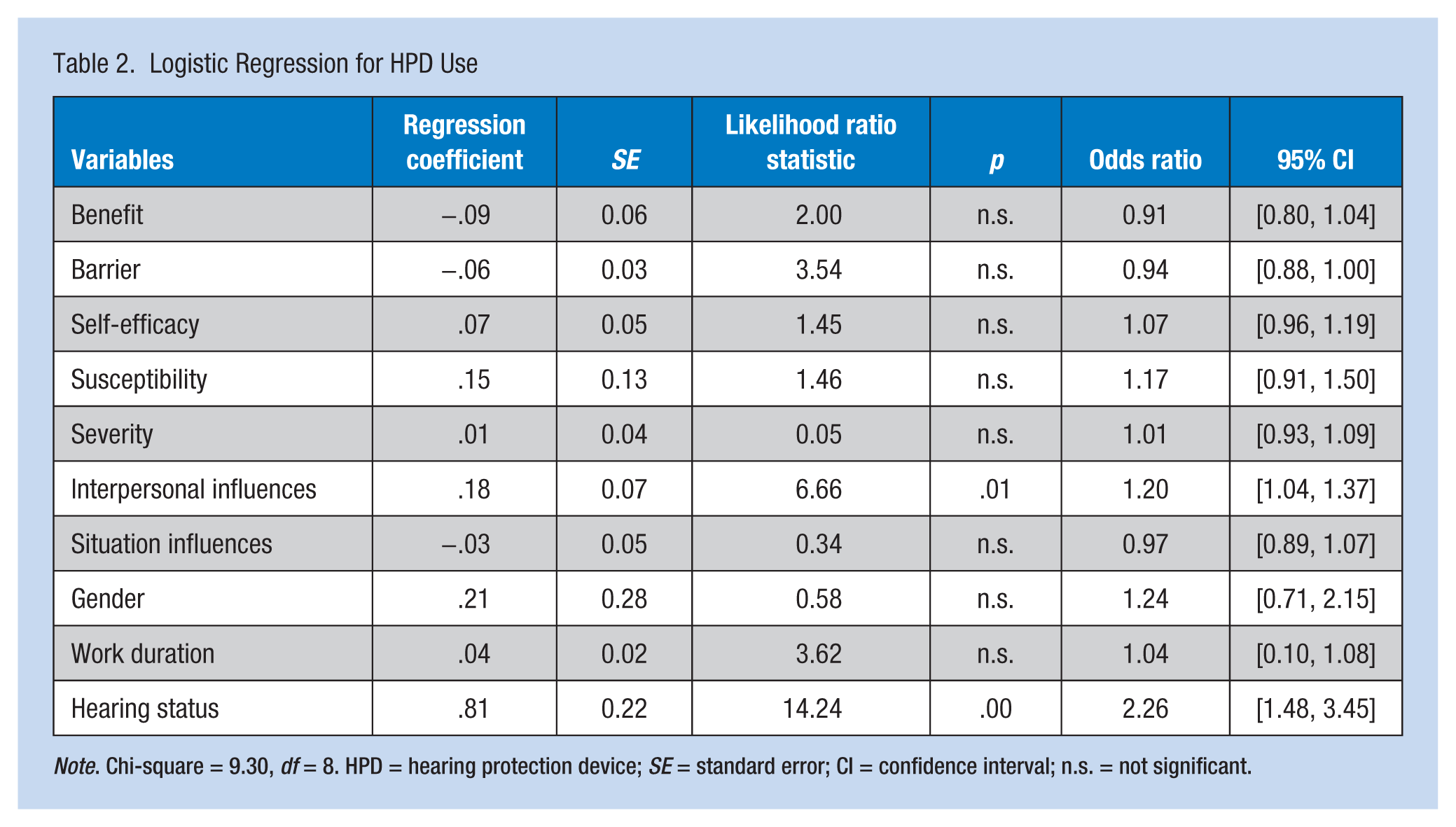
Note. Chi-square = 9.30, df = 8. HPD = hearing protection device; SE = standard error; CI = confidence interval; n.s. = not significant.
The overall goodness-of-fit model was 320.8. Logistic regression analysis revealed that perceived hearing status (b = 0.81, p < .001) and internal influences (b = 0.18, p < .025) statistically correlated with use of HPDs. As can be seen in Table 3, overall, the model correctly classified 70.1% of the cases. Almost 80% of users and 58% of nonusers were accurately classified.
Classification by Model of Predicted and Self-Reported Use of HPDs
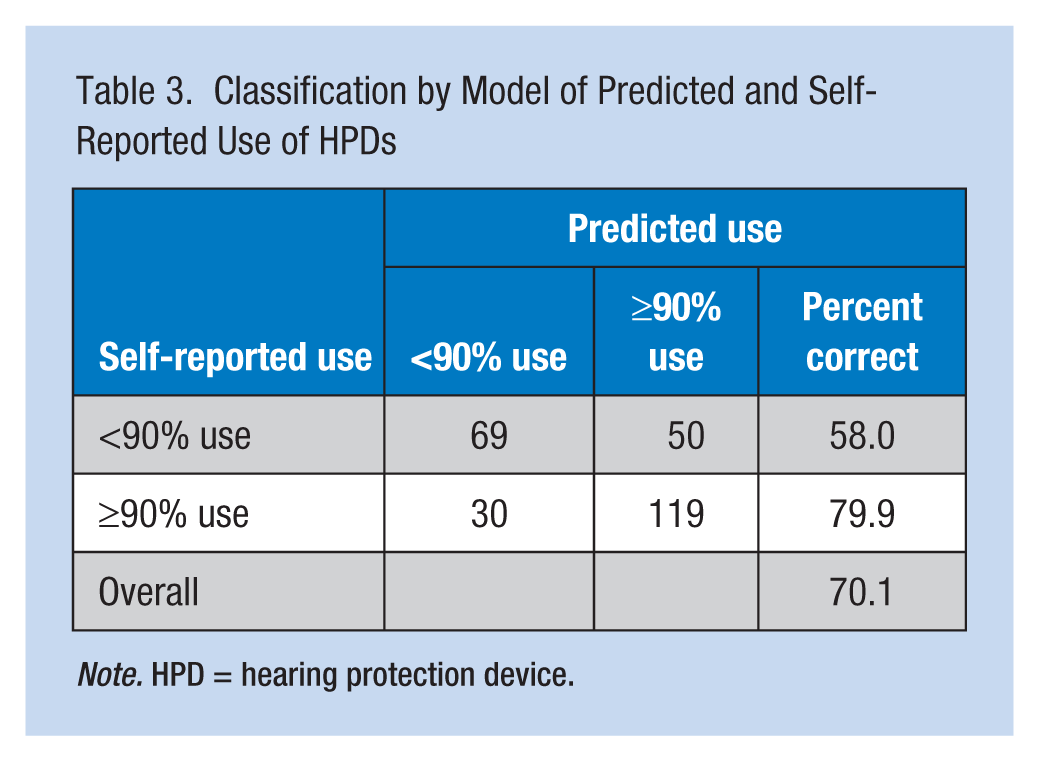
Note. HPD = hearing protection device.
In an effort to reach a parsimonious model, post hoc model revision was investigated. Only significant factors, perceived hearing status and internal influences, were included in the model. As shown in Table 4, goodness-of-fit model was 335.4. Perceived hearing status (b = 0.66, p < .001) and internal influences (b = 0.20, p < .001) were significantly correlated with the use of HPDs. The overall model correctly classified 63.4% of the cases. The percentage of users accurately classified was 78.5%, and the percentage of nonusers accurately classified was 44.5%.
Logistic Regression of Selected Model Variables on HPD Use
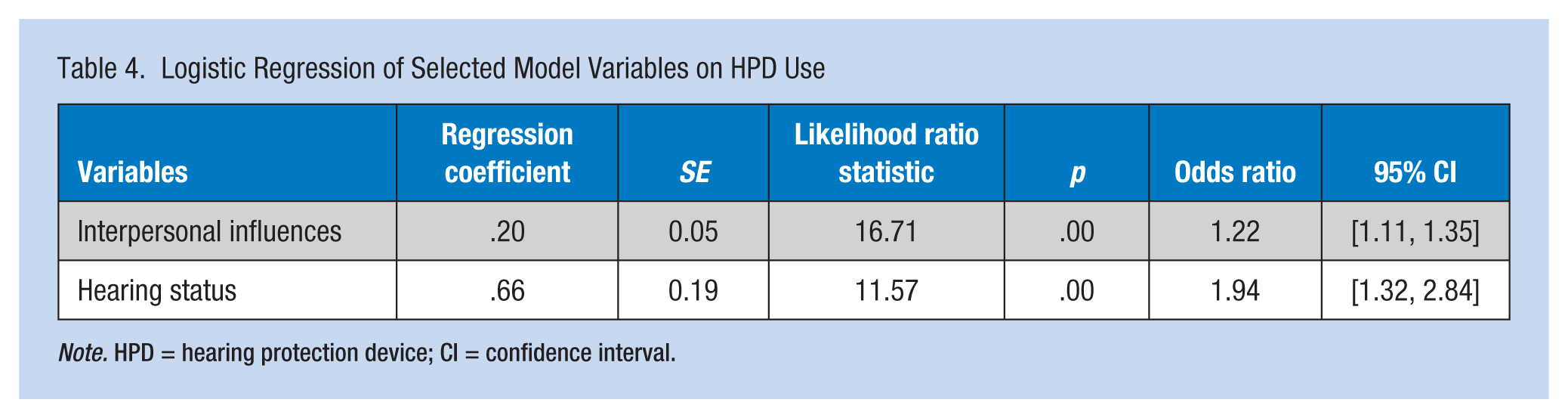
Note. HPD = hearing protection device; CI = confidence interval.
Discussion
This study emphasized that the PUHPM could be used to predict the use of HPDs among noise-exposed Thai workers. Study results have shown that overall the model correctly classified 70.1% of the cases. The percentage of users accurately classified was 79.9%, and the percentage of nonusers accurately classified was 58%. These percentages were higher than the previous study, which found that the PUHPM explained 12% of the variance in HPD use among Black workers and 36% of the variance in HPD use among White workers (Hong et al., 2005). Raymond et al. (2006) found that the PUHPM explained 20% of the variance in HPD use among Hispanic workers and 37% of the variance in HPD use among non-Hispanic workers.
This study revealed significant factors affecting industrial workers’ use of HPDs. Perceived hearing status and interpersonal influences were found to be significantly related to the use of HPDs among this group of workers; together, these variables correctly predicted HPD use in 63.4% of the cases. Perceived hearing status was the strongest predictor of HPD use (OR = 1.94, 95% CI = [1.32, 2.84]); workers who perceived their hearing status as good were more likely to use HPDs. This result is new because no study was found in the literature that correlated the use of hearing protection with perceived hearing status. The results from this study were similar to previous studies of other occupational groups, namely, that “interpersonal influences” were a significant factor in predicting HPD use. Lusk et al. (1997) found that interpersonal influence—interpersonal norms, interpersonal support, and interpersonal modeling of HPD use (i.e., how much workers believe others use HPDs when exposed to noise, especially their supervisors and coworkers with whom workers spend the most time)—was the strongest predictor of HPD use among construction workers (r = .45, p < .05). Similarly, McCullagh et al. (2002) found that interpersonal support was a significant predictor of HPD use among farmers (b = 1.93, p < .005). With regard to other previous studies, interpersonal influences could predict the use of HPDs among White workers (r = .19, p < .001; Hong et al., 2005), and firefighters (β = 18.55, p < .001; Hong et al., 2013). For this particular sample, the strong interpersonal influence on HPD use may reflect a unique work culture that highly values observational learning and encouragement from others, especially coworkers and supervisors.
Interestingly, the other strong factors (i.e., perceived benefits, perceived barriers, and self-efficacy in the use of HPDs) did not predict HPD use among the workers in this study. Different characteristics of the samples and the instruments used might have affected the results. This study should be carefully generalized because the participants were employed only in factories located in the Tharongchang district, Surajthanee Province of Thailand, and the findings may not apply to workers in other areas of Thailand or other global workplaces.
Implications for Occupational Health Nurses
This study revealed predicting factors influencing HPD use among Thai workers. These factors included workers’ perceptions about hearing status and interpersonal factors incuding social network and social support systems from primary groups in the workplace setting (i.e., coworkers and supervisors). Further research is needed to develop a comprehensive program to promote Thai workers’ use of HPDs. Occupational health nurses can perform audiometric tests and inform workers’ about their hearing status. The findings demonstrate the need for more than individual change strategies. At the interpersonal level, occupational and environmental health nurses should assist workers to create a support or self-help group to promote workers’ use of HPDs. For example, they might choose workers who are wearing HPDs consistently to be leaders who can support and encourage their coworkers to use HPDs. Occupational and environmental health nurses might also consider using “train the trainer” strategies to promote hearing protection use among noise-exposed workers.
Applying Research to Practice
The Predictors of workers’ Use of Hearing Protection Model (PUHPM) could be used to predict hearing protection device (HPD) use among noise-exposed Thai workers. Significant factors included workers’ perceptions of their hearing status and interpersonal influences (modeling and support from coworkers and supervisors); together, these variables correctly predicted HPD use in 63.4% of the cases. Instead of focusing only on personal factors, occupational and environmental health nurses can develop comprehensive interventions targeting the individual and interpersonal levels of influence to promote the use of hearing protection.
Footnotes
Acknowledgements
The authors are thankful for the study participants. The authors also acknowledge Dr. Mary K. Salazar, Department of Psychosocial and Community Health, University of Washington School of Nursing for her suggestions to improve this article.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research funding was provided by CMU Junior Research Fellowship Program, Chiang Mai University.
Author Biographies
Kunlayanee Tantranont is Assistant Professor, Faculty of Nursing, Chiang Mai University, Chiang Mai, Thailand.
Nuntanat Codchanak is an Occupational Health Nurse, Tharongchang Hospital, Surajthanee, Thailand.