
Abstract
Background
Workplace wellness programs (WWP) offer physiological and psychological benefits to employees and financial and productivity benefits to employers. However, the COVID-19 pandemic has prevented in-person sessions and has required WWP’s to transition to online platforms. The purpose of this brief report was to assess the preliminary feasibility, acceptability, and efficacy of a mobile version of the Bruin Health Improvement Program (BHIP mobile) WWP.
Methods
Participants virtually attended (i.e., via Zoom) twice weekly physical activity sessions and a once weekly nutrition seminar for 10-weeks with the option of a 30-minute one-on-one consultation with a registered dietician. Demographics, anthropometric indices, stress, muscular endurance, and aerobic fitness were assessed at baseline and follow-up. All analyses were conducted in SPSS v. 27.
Results
Twenty-seven participants (96% female) enrolled and 13 (100% female) completed the 10-week program. There were significant reductions in bodyweight (p < .01) and body mass index (p < .02) but not stress (p > .05), and significant increases in muscular endurance (p < .01) but not aerobic fitness (p > .05). Overall, BHIP mobile appears to be acceptable to participants but logistical concerns such as inconsistent internet connection was noted as potential downfalls.
Conclusions/Applications to Practice
Improvements in health outcome among completers of a mobile WWP were promising. Completer feedback highlighted program strengths as the flexibility and comfort of attending exercise sessions and nutrition classes from home. Future versions of the program will allocate resources to improve completion and expand appeal for men and women.
Background
The World Health Organization (WHO, 2021) considers workplace wellness programs (WWP) important to both physiological and psychological health of employees while having both financial and productivity benefits to employers. Although WWP’s have shown preliminary efficacy (Burn et al., 2019; Emerson et al., 2017; Prieske et al., 2019; Rezai et al., 2020), the COVID-19 pandemic and associated social distancing orders required that some non-essential employees work from home (Guan et al., 2020). These orders presented a significant challenge to WWP’s that have participants attend their sessions in fitness centers with their peers. Thus, to continually offer exercise and nutrition classes to interested and motivated employees, some WWP’s developed and executed alternative modes of dissemination.
There has been a significant amount of research on the use of mobile technology (mHealth) to help facilitate health and wellness interventions (Arigo et al., 2019). As a subset of electronic health (eHealth) interventions that include internet-based interventions, video games, and other interventions using the computer, mHealth interventions take advantage of the ubiquitous nature of cell phones, and by extension, smartphone applications and text messaging services as a delivery mechanism (Lindhiem et al., 2015). Among others, some of the advantages of mHealth are that it can avoid many of the barriers to on-site interventions. For example, mHealth interventions can be completed anytime and anywhere at participants’ convenience, and can reach many more individuals at a given time (Arigo et al., 2019). In addition, mHealth can avoid logistical challenges such as transportation, child care (if applicable), and the cost of building the infrastructure needed to support an exercise program (i.e., fitness center) (Lindhiem et al., 2015). However, the biggest advantage mHealth has over traditional in-person WWP, particularly during the pandemic, is that it allows employees to work out alone eliminating the risk of COVID-19 acquisition and transmission.
The Bruin Health Improvement Program (BHIP) is a WWP for employees at the University of California, Los Angeles (UCLA) (“UCLAREC FITWELL Program,” n.d.). BHIP offers twice weekly exercise and once weekly group nutrition classes for 12-weeks. The aim of BHIP is to reduce cardiovascular disease risk factors (e.g., reduce obesity, increase cardiorespiratory fitness) and to improve mental well-being. Previous evaluations of BHIP have shown reductions in bodyweight, body mass index, and waist-to-hip ratio (Rezai et al., 2020) as well as significant reductions in stress and improvements in social satisfaction, self-efficacy and quality of life (Emerson et al., 2017). Cost-benefit analyses of BHIP have also estimated that employee weight loss can reduce annual medical care costs to employers by ~$2,200 USD per employee per year (Rezai et al., 2020).
The COVID-19 pandemic and its associated social distancing guidelines resulted in an immediate transition from in-person BHIP to a virtual iteration (BHIP mobile) with all assessments and classes moved to the online platform. BHIP mobile was developed and implemented in 2020 and the purpose of this brief report was to assess its preliminary feasibility, acceptability, and efficacy.
Methods
Data for this study were collected from UCLA faculty and staff who enrolled in BHIP mobile for 10-weeks between July 2020 and September 2020. BHIP mobile was offered in lieu of the traditional in-person program to help employees engage in regular exercise and nutrition classes while maintaining social distancing guidelines. Roughly 33,000 emails were sent via a campus-wide listserv giving all employees an equal opportunity to participate; however, we aimed to recruit a maximum of 30 participants. In total, 26 interested participants completed an online application and were chosen at random from the 63 who expressed interest for enrollment. A second email was sent to congratulate participants who were selected. This email included a set of instructions to complete several baseline questionnaires (online through Survey Monkey) and convenient times to set up their physical assessment sessions via Zoom.
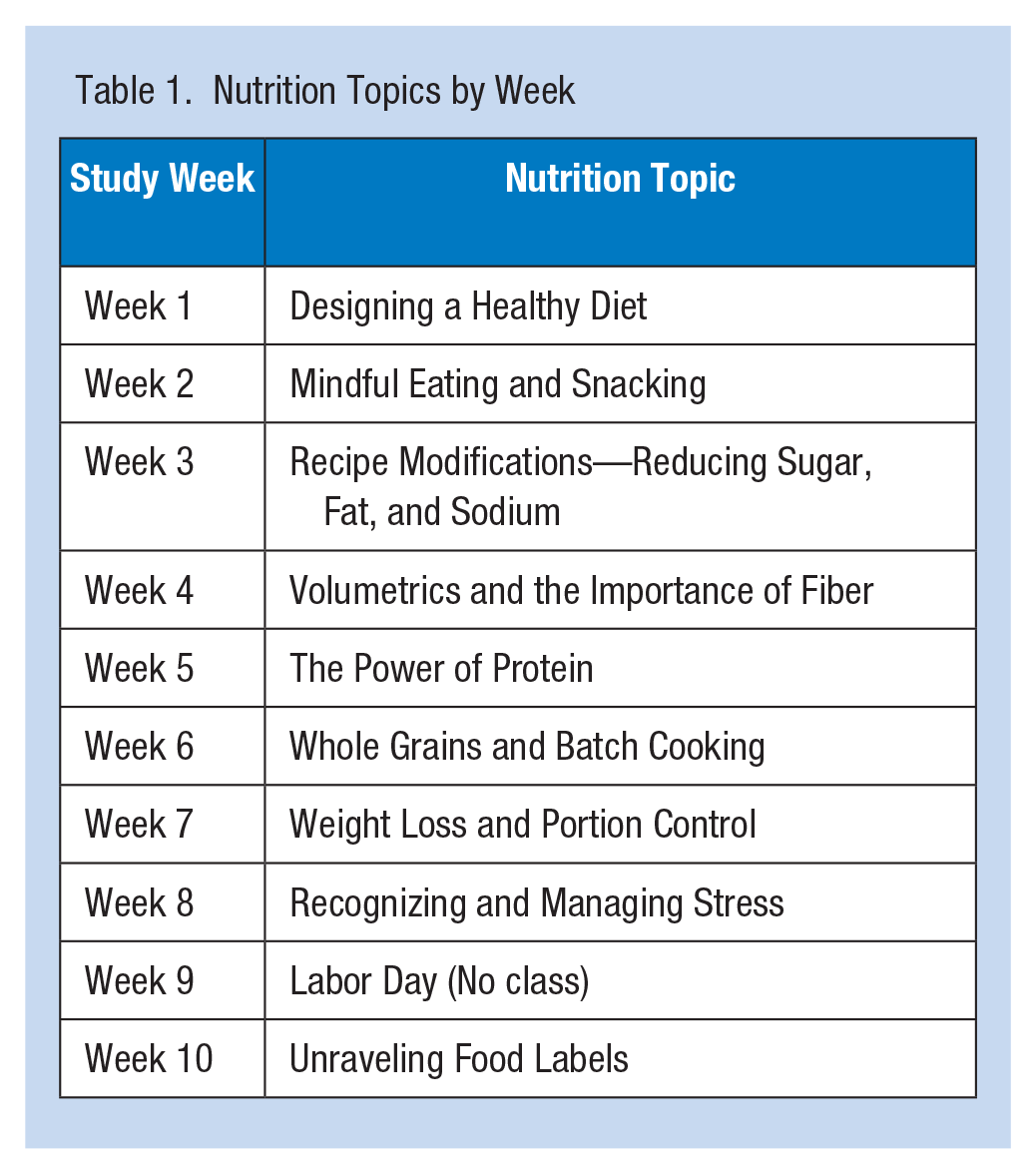
The weekly exercise sessions (and pre- and post-physical assessments) were led by certified UCLA fitness trainers and focused on building muscular endurance and aerobic fitness. The nutrition class curriculum covered a new topic each week and is detailed in Table 1. Participants were also offered one, one-on-one, 30-minute consultation with the registered dietician via Zoom over the 10 weeks. Although previous in-person iterations of BHIP were 12 weeks, concerns regarding participant engagement in a virtual setting led to the first round of BHIP mobile being offered for six weeks, with the option to continue. All participants requested an extension so four weeks were added for a total of 10 weeks. Demographics, anthropometric indices, stress, physical activity status, and fitness were assessed. Given the sudden change in the dissemination strategy, we assessed program acceptability by inquiring with open-ended questions about participant experiences with the Zoom classes, the overall virtual experience, and aspects of the program that they liked and disliked.
Nutrition Topics by Week
Baseline characteristics were analyzed using descriptive statistics including mean and standard deviations. Pre-to-post changes in study outcomes were analyzed using paired samples t-tests, but only those with actual observations at both baseline and follow-up were included. All analyses were performed in SPSS v. 27.
Data were collected with the limited intent of evaluating and improving an existing program. Approval was obtained from the university Institutional Review Board (IRB) for a prior study and the current study analyzed the de-identified data. Based on the IRB’s policy on secondary analysis using de-identified data, no additional approval was required.
Results
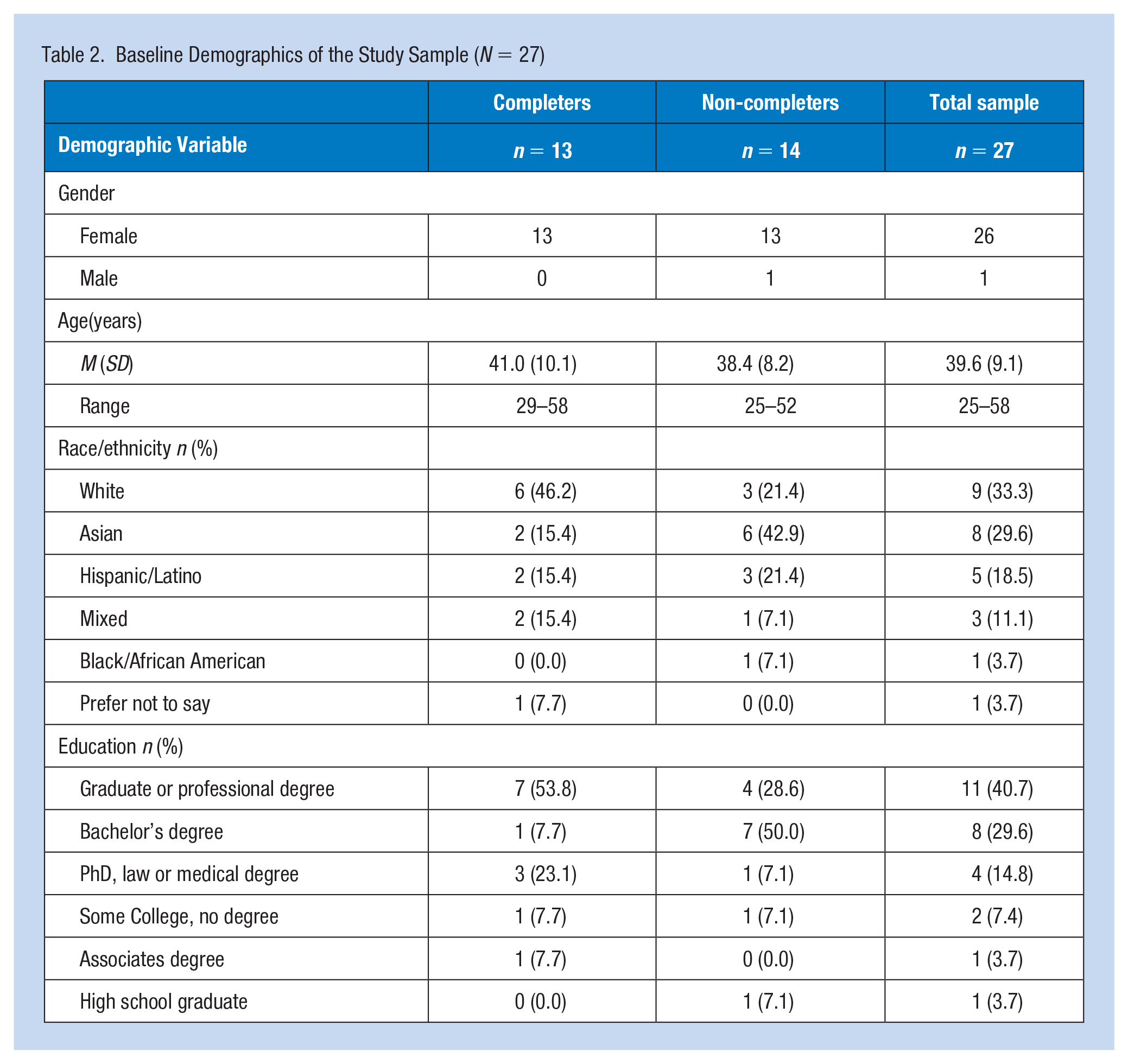
Twenty-six females and one male were enrolled in BHIP mobile. The average age of the sample at baseline was 39.6 (SD = 9.1) years. The majority of participants (85.1%) had a bachelor’s degree or higher (Table 2). In addition, the average body weight, height, and mass index of the sample at baseline were 198.9 (SD = 42.5) pounds, 64.4 (SD = 2.5) inches, and 33.4 (SD = 7.2). Most participants (51.9%) were not regularly active (Table 3).
Baseline Demographics of the Study Sample (N = 27)
Baseline Anthropomorphic Measurements, Self-Reported Physical Activity Status and Past Week Exercise Capabilities (n = 27)
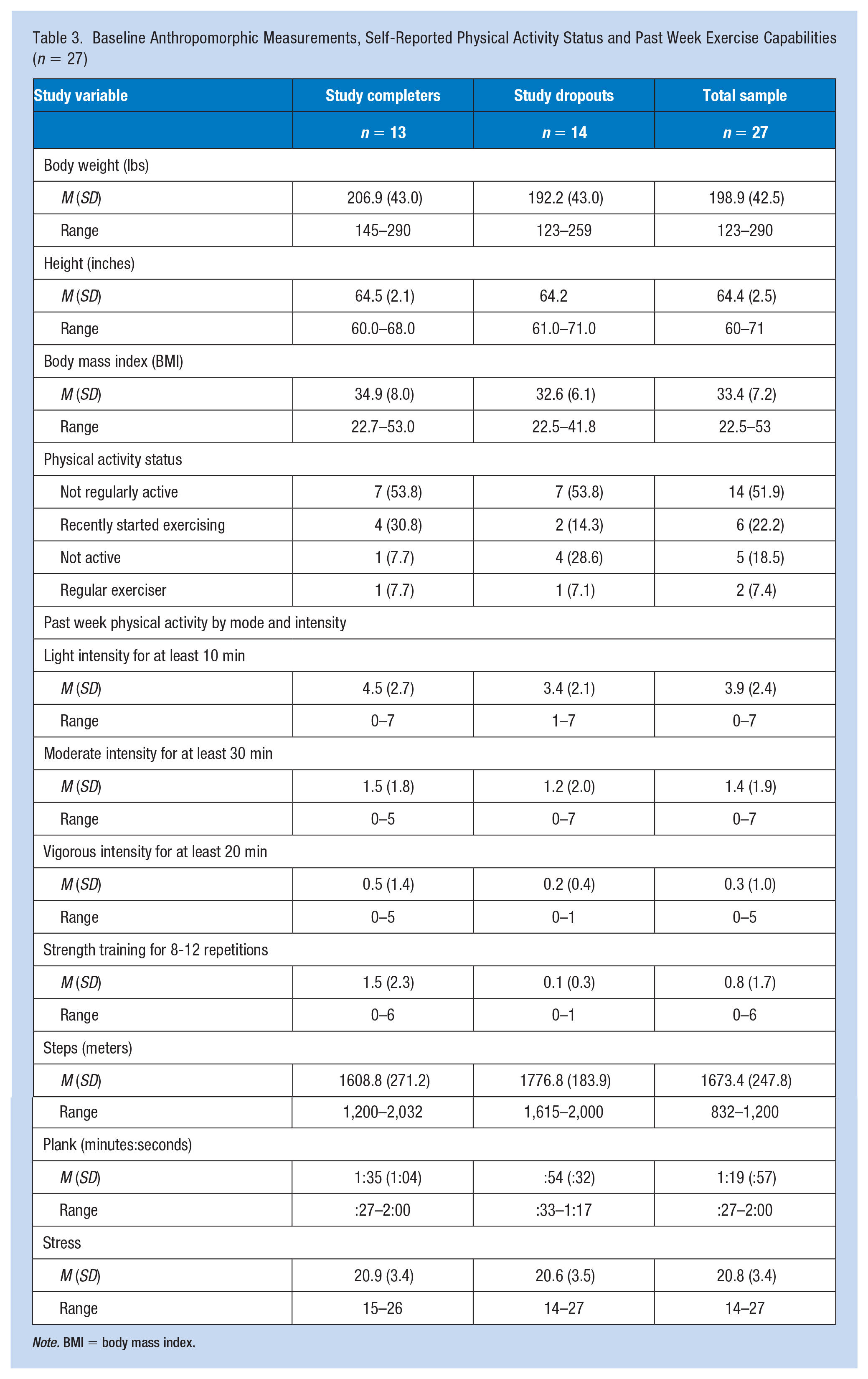
Note. BMI = body mass index.
Only half (n = 13) of the participants completed the full program and as such, we explored potential differences between completers and non-completers at baseline; however, no significant differences emerged. Among program completers (n = 13), there were significant reductions in body weight from baseline to follow-up (mean difference = 5.9 lbs.) 95% confidence interval (CI) = [1.93, 9.92], t(12) = 3.23, p < .01 and body mass index from baseline (mean difference = .85) 95% CI (0.15 to 1.54), t(12) = 2.65, p = .02. Maximum time in a plank pose also significantly increased from baseline to follow-up (mean difference = 1:29); 95% CI [-1.38, -0.41], t(6) = 4.50, p < .01. Participants also ran an additional 148.5 (SD = 319.3) meters in 15 min; however, this change did not reach statistical significance (p = .27). There were also no significant changes in stress (p > .05).
Study completers considered BHIP mobile to be acceptable and beneficial to help them reach their health and wellness goals. Some participants (n = 2) would have preferred to meet in person but overall, they indicated that they enjoyed the virtual interactions with coaches and nutrition specialists. Increased flexibility, a decrease in travel time to get to the fitness center, and the ability to work out alone (to avoid feeling embarrassed or negatively judged by others) were noted as positives of BHIP mobile but logistical concerns such as inconsistent internet connection and difficult placing the camera in a good position were also noted as challenges.
Discussion
The COVID-19 pandemic and its associated social distancing guidelines have presented many challenges to in-person health and wellness interventions, including those targeting the workplace. BHIP mobile tested a mobile version of the in-person BHIP framework and was developed to comply with government orders associated with the pandemic. Health outcome improvements among completers were promising, particularly as they relate to reductions in markers of cardiovascular disease (i.e., bodyweight and bodyfat %) and improvements in muscular endurance. However, unlike the findings from previous in-person versions of BHIP (Emerson et al., 2017), we observed no significant reductions in stress which was possibly a result of the COVID-19 pandemic increasing stress beyond pre-pandemic levels (Fofana et al., 2020). Furthermore, most participants found BHIP mobile to be acceptable and enjoyable, particularly its flexibility and improved level of comfort.
Despite all the benefits of mHealth interventions one notable limitation can include not being able to ask questions or express concerns in real-time. With this in mind, a significant strength of BHIP mobile was that fitness and nutrition sessions were live. Thus, participants had the ability to stop the instructor to ask questions about technique for certain exercises, modifications to exercises or cooking techniques that may have been too difficult, or about substitutions for ingredients that may not be enjoyable and/or available. A limitation to this method, however, was that sessions were not asynchronous, meaning that participants could not login and complete sessions at any time.
Another strength of BHIP mobile was the flexibility and comfort of attending exercise sessions and nutrition classes at home. One of the positive comments about BHIP mobile made by participants was the increased level of comfort performing exercises alone (and not in front of their peers) to avoid negative judgment. This is a common barrier to exercise participation among those with social physique anxiety (SantaBarbara et al., 2017) and may highlight another strength of BHIP mobile (and other WWPs) moving forward. Specifically, having an mHealth option as an alternative to in-person sessions may have a greater reach by attracting those who would not join such a program if an mHealth option were not offered. However, it would be important for the instructor to be able to constantly monitor exercise technique to reduce the risk for injury. Finally, a strength of the nutrition classes was that they could be viewed from participant’s kitchen which could be more meaningful because the lessons and recipes could be immediately applied.
Despite these strengths there were limitations worth mentioning. First, the high level of attrition and low level of participation (among men, specifically) in relation to the total number of UCLA faculty and staff was notable. Low levels of enrollment and retention were common in WWPs in general, and among men more specifically (Hunter & Brandner, 2019; Hunter et al., 2019; Rounds & Harvey, 2019). However, it is also possible that the low engagement was a result of daily stressors associated with the pandemic, as many UCLA employees may have focused more on keeping their families safe or navigating how to transition their typical in-person job responsibilities online instead of initiating an exercise program. Another possible reason for the low engagement was that BHIP only recruited those individuals who were currently sedentary and at least 40 lbs. overweight. Still, the 13 participants who did complete the program attended 86% of the classes (26/30) and the level of attrition and retention of the one male completer was similar to previous in-person versions of BHIP (Rezai et al., 2020). Some solutions to these limitations could include increasing the number of check-ins via free text messaging applications by study staff to increase program compliance. Another possible solution could include adding a social support component (e.g., a buddy system) which has been shown to increase engagement in health-based programs (Arigo et al., 2019). Finally, given that the ideal male body image is commonly portrayed as muscular and lean (Lefkowich et al., 2017), advertising future WWPs as an opportunity to increase muscle mass while also losing bodyfat may encourage more men to join.
A second limitation of BHIP mobile was the significant reduction in the selection of certain exercises and equipment that could be used, particularly as it relates to strength training. However, household items such as milk cartons and food bags could be used as external resistance in lieu of traditional weight room items (i.e., dumbbells). Future mHealth WWPs could provide resistance bands, medicine balls, and/or kettlebells to participants who prefer working out alone at home to group workouts in a fitness center. Third and finally, a limitation of BHIP mobile was that muscular (e.g., one repetition maximum) and aerobic (e.g., VO2max) fitness assessments were limited and instead relied heavily on bodyweight exercises, such as pushups.
Conclusion
The implications of BHIP mobile include its flexibility and increased comfort of working out alone at home. Thus, this alternative mode of dissemination (i.e., mHealth) may attract more employees who were (or are) disinterested in participating in the more traditional in-person offerings of a WWP. In addition, we observed reductions in bodyweight and body mass index as well as improvements in muscular fitness which suggests that even a virtual program without any traditional exercise equipment (i.e., dumbbells) can be an effective way to improve employee health. However, given the low rates of engagement particularly among men, future research will need to allocate resources to improve recruitment, delivery, and usability. In addition, more work is needed to determine if similar results can be achieved in those with varying levels of education and from different racial groups. These WWP improvements may ultimately increase program reach and attract more employees for participation.
Applications to Professional Practice
WWPs offer physiological and psychological benefits to employees and financial and productivity benefits to employers. However, the COVID-19 pandemic has forced WWPs to transition to online platforms to accommodate stay-at-home orders. Assessing the preliminary feasibility, efficacy, and acceptability of a mobile WWP sheds light on whether virtual programs can be as effective in improving employee health as in-person programs. Results demonstrate that virtual wellness programs, such as the BHIP mobile, appear to be an effective strategy to improve muscular endurance and reduce markers of cardiovascular disease, such as body weight and bodyfat percentage. Significant strengths of the program are the flexibility and comfort of attending exercise sessions and nutrition classes at home.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following funding for research, authorship and/or publication of this article: The research BHIP was funded by UCLA Worker’s Compensation/Rate Additive. The research study was unfunded. None of the authors received funds or financial assistance from UCLA Worker’s Compensation/Rate Additive or any other source. The study was conducted independently from Worker’s Compensation/Rate Additive. Dr. SantaBarbara’s time was supported by the National Institute of Mental Health [T32MH109205].
Ethical Approval
Data were collected with the limited intent of evaluating and improving an existing program. Approval was obtained from the university Institutional Review Board (IRB) for a prior study and the current study is analyzing the de-identified data. Based on the IRB’s policy on secondary analysis using de-identified data, no additional approval was required.
Data were collected with the limited intent of evaluating and improving an existing program. All data have been deidentified, therefore it did not require approval from the university institutional review board (IRB).
Author Biographies
Dr. SantaBarbara is a T32 postdoctoral fellow in the Department of Psychiatry and Biobehavioral Sciences within the Semel Institute of Neuroscience and behavior at UCLA. Dr.SantaBarbara is primarily interested in developing and implementing sustainable and scalable exercise interventions to treat and prevent chronic illness.
Roxana Rezai, MPH is a doctoral student in the Department of Epidemiology at UCLA’s Fielding School of Public Health. Roxana has worked in the field of behavioral health research examining health disparities and risk for HIV among minority populations. She is particularly interested in how social media and other new technologies can be used as tools for engagement, recruitment, data collection, and health promotion.
Elisa Terry UCLA Recreation Associate Director of Fitness & WellnessCertified Strength & Conditioning Specialist (CSCS) by the National Strength & Conditioning Association (NSCA). Elisa developed and manages the Bruin Health Improvement Program; hires, trains, and supervises all coaches and program staff; and coaches several classes.
Kelly Shedd is the Wellness Program Analyst for the UCI Health system. She helps coordinate, promote, and implement employee wellness programs and services for all clinical staff. Kelly also serves as part of the UC wide Diabetes Prevention Program Coordinating Center, and is the co-chair of the UC wide Wellness Managers Committee.
W. Scott Comulada, DrPH, is the director for the UCLA Semel Institute Center for Community Health and a professor-in-residence in the UCLA Department of Psychiatry and Biobehavioral Sciences with a secondary appointment in the Department of Health Policy and Management. He has a background in statistics and has research interests to develop and evaluate digital health interventions.