
Abstract
Background:
Shift work is associated with long-term health risks. Workplace-based health interventions hold promise for improving or maintaining the health of shift workers; yet, the impact of workplace-based interventions on shift worker sleep duration has not been assessed. We conducted a systematic review of workplace interventions on shift worker sleep.
Methods:
We conducted searches in PubMed, Web of Knowledge, EMBASE, Scopus, and PsycINFO (n = 6,868 records) of all studies published through May 15, 2019. Eligibility criteria included the following: (a) individuals aged ≥18 years; (b) a workplace-based employee intervention; (c) an employee population comprised predominantly of shift workers (>50%); and (d) sleep duration as a study outcome.
Findings:
Twenty workplace interventions met eligibility criteria. Mean intervention duration was 125 (SD = 187) days and mean sample size was 116 employees (SD = 256) with a mean age of 36.4 years (SD = 6.5). Interventions most commonly focused on light exposure (25%) or shift timing (25%), followed by sleep hygiene (20%). Most interventions were conducted in the health care and social assistance sector (60%). Study quality on average was 64% (SD = 7%). A majority of the studies found that a workplace-based health intervention was associated with a desirable increase in 24-hour total sleep duration (55%). The overall average increase in daily employee sleep duration achieved by interventions ranged for RCT studies from 0.34 to 0.99 hours and for non-RCT studies from 0.02 to 1.15 hours.
Conclusions/Applications to Practice:
More than half of the employee health interventions, especially yoga or mindfulness interventions, resulted in a desirable increase in sleep duration. Workplaces hold promise as an avenue? for delivering programs and policies that aim to improve sleep duration among shift workers.
Background
Shift schedules, including overnight, on-call, and/or rotating shift, are a necessary part of our global 24/7 society (McMenamin, 2007). Shift work, unfortunately, is associated with numerous long-term health risks (Costa, 2010) including hypertension (Dochi et al., 2009), metabolic syndrome, diabetes (Jung et al., 2018), cardiovascular disease (Suessenbacher et al., 2011; Torquati et al., 2018), and poor skeletal muscle health (Aisbett et al., 2017). Furthermore, evidence from rigorous cohort-based nested case–control studies and population-based case–control studies have shown that shift work is associated with breast (Cordina-Duverger et al., 2018; Wegrzyn et al., 2017) and prostate cancer (Barul et al., 2019; Behrens et al., 2017). Due to this evidence, several prominent associations, including the World Health Organization and the International Agency for Research on Cancer, have concluded that shift work is a probable carcinogen (Erren et al., 2010; Ward et al., 2019). Shift work also places workers at risk for sleep deficiency, broadly characterized as insufficient sleep, sleep fragmentation (M. Härmä et al., 1998; M. I. Härmä et al., 1994), and sleep disorders, such as insomnia (Chatterjee & Ambekar, 2017) and greater severity of apnea symptoms (Verde-Tinoco et al., 2017).
Worksite-based health interventions hold promise for improving the health of workers, especially those who are high risk, such as shift workers (Papantoniou et al., 2017). Shift workers often sleep at times that conflict with the pattern of light and darkness in their environment, inducing circadian misalignment and internal desynchrony of circadian rhythms, physiology, and behavior that can compromise the duration and quality of their sleep (James et al., 2017; Morris et al., 2017). Sleep deficiency and circadian misalignment have been shown to dysregulate biological processes, and increase risk for adverse health outcomes (James et al., 2017). Compared to traditional non-shift workers, shift workers also have an increased rate of maladaptive health behaviors such as smoking, excessive eating, and poor dietary choices (Shan et al., 2018), likely furthering their higher risk of adverse sleep and health outcomes.
Sleep deficiency among workers has important workplace-related consequences. For instance, studies have identified a link between sleep disturbances and decreased work performance (due to absenteeism and decreased productivity) as well as greater health care costs (Hui & Grandner, 2015; Kessler et al., 2011). For instance, poor sleep deficiency carries an estimated economic impact of between $30 and $40 billion annually in the United States in terms of direct and indirect health care costs (Chilcott & Shapiro, 1996; Hafner et al., 2016). Also concerning, workers with sleep deficiency are more likely than workers without sleep deficiency to suffer falls, accidents, and workplace-related injuries (Ryu et al., 2017).
Several prior studies have shown that workplace-based health interventions can improve employee sleep duration, but the majority of these studies have been conducted among day workers, as opposed to shift workers (Adachi et al., 2008, 2003; Adler et al., 2017; Chen et al., 2010; Klatt et al., 2017). Workplace based health interventions focused on improving sleep among shift workers have the potential to improve the health of these workers at high risk for pressing health concerns. There is a need for more research to advance our understanding of the impact of workplace-based interventions tailored to shift workers with regard to sleep. A recent systematic review summarized sleep-related outcomes of workplace health programs among day workers (Robbins et al., 2019), and another review summarized sleep-focused workplace programs (Redeker et al., 2019). Both reviews cited the importance of health programs for shift workers as sleep is fundamentally compromised among this population. Our review addresses this important topic by summarizing workplace-based health interventions tailored to shift worker populations. Many of the studies in our review focus on shift workers such as nurses, medical residents, and other service professions including police and firefighters. We assess components such as the length of the intervention period, behavior change techniques (BCTs) utilized, and improvement in the shift workers’ sleep duration resulting from exposure to the various workplace-based health interventions. By summarizing how workplace-based employee health programs influence sleep duration among shift workers, future workplace wellness programs will be able to consider the importance incorporating evidence-based interventions to promote sufficient sleep duration for shift workers.
Methods
We conducted a systematic review of studies evaluating sleep duration as an outcome in the context of a workplace-based employee health interventions. For this reason, we identify and review articles that describe workplace employee health programs tailored to shift workers that measure sleep duration. The search adheres to the Preferred Reporting for Systematic Review Protocols (PRISMA) guidelines (Page et al., 2021). To be eligible for this systematic review, studies had to include the following: (a) individuals aged ≥18 years; (b) a workplace-based employee intervention; (c) interventions that recruited shift-workers; and (d) sleep duration as an outcome. There were no language exclusion criteria for this review. Studies were excluded if they were cross-sectional, contained sample populations of >50% day workers, did not measure sleep duration as an outcome, or was carried out with non-humans. Figure 1 displays the flow diagram of study screening according to PRISMA guidelines.
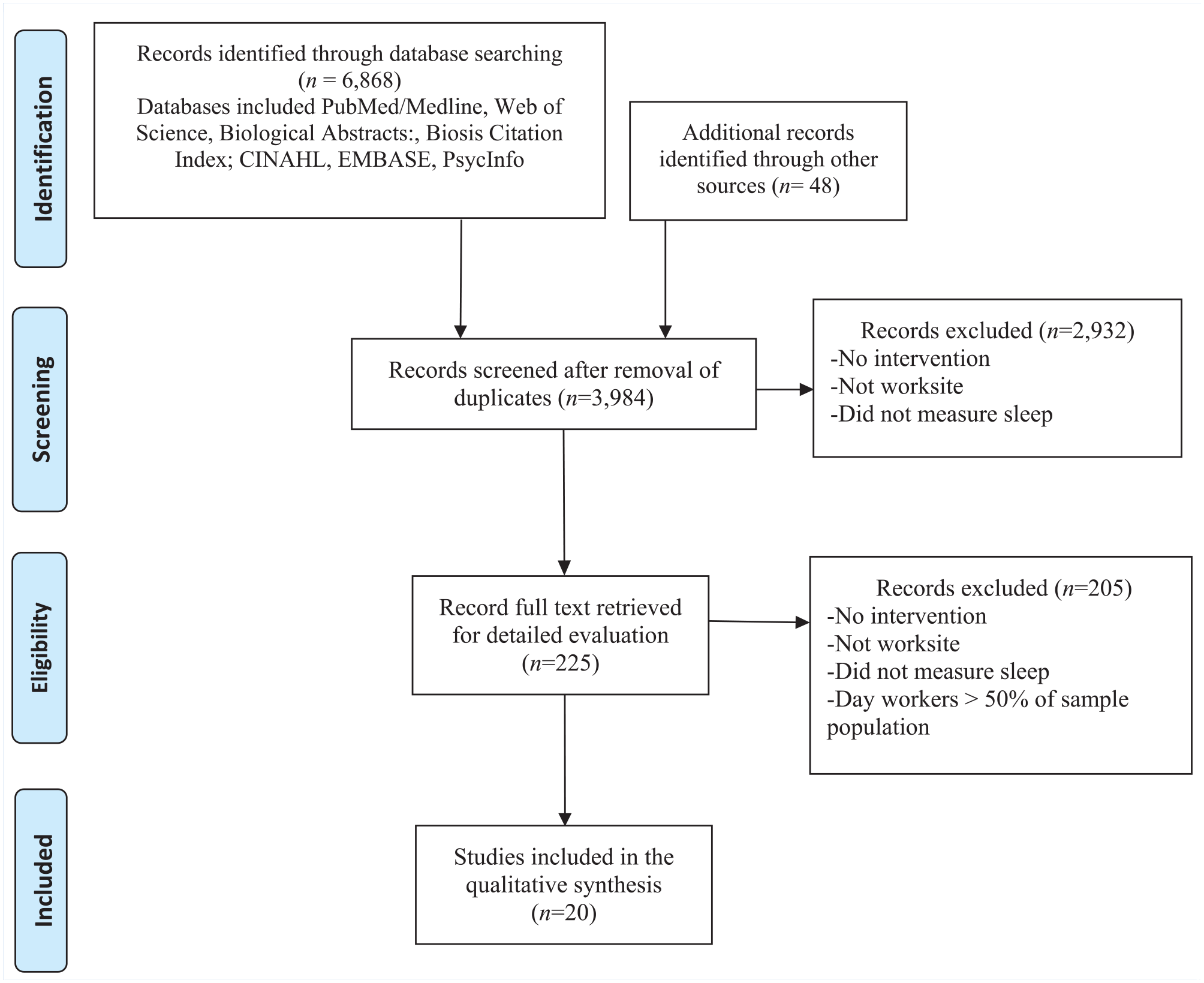
Flow diagram of study screening and selection according to PRISMA guidelines to identify studies that administered a workplace health intervention for shift workers that measured sleep.
The search strategy, shown in the Appendix, included the following databases: PubMed/Medline, Embase, Web of Science, the Cumulative Index to Nursing and Allied Health (CINAHL), PsycINFO, BIOSIS Citation Index, and the Cochrane Library. The New York Academy of Medicine Grey Literature, WorldCat’s OAISster and OpenGrey databases also provided relevant literature. In addition, a search was performed within the table of contents of the following journals: Journal of Occupational and Environmental Medicine; Sleep; International Archives of Occupational and Environmental Health; Occupational Medicine (London); Journal of Sleep Research; Occupational and Environmental Medicine; Sleep Medicine; Sleep Health; and Journal of Occupational Health. The date of the search included all published literature in press on or before November 1, 2019. From the articles that were identified as eligible, a search of the articles within their reference lists was also conducted. We used combinations of text words and thesaurus terms (i.e., work [MeSH], workplace [MeSH Terms], occupational health [MeSH Terms], occupational health [MeSH Terms], employee [All Fields], health promotion [MeSH Terms], interventions [All Fields], and sleep [MeSH Terms]). Our study included all available published literature up until November 1, 2019.
Records were identified utilizing the search strategy outlined above, then exported to EndNote X7. Three reviewers (P.U., S.K., R.R.) screened out the records based on titles and abstracts. The full texts of potentially eligible articles were retrieved and reviewed. Reference lists of these selected articles was analyzed for further eligible articles. The studies that were retrieved for detailed analysis were assessed by independent reviewers (P.U., S.K.) to ensure they satisfied the inclusion criteria. Any disagreements were resolved through consensus or discussion with the lead author (R.R.).
RevMan (version 5) was used to analyze data extracted from the full-text articles. Data were extracted into several general categories such as study design and characteristics (e.g., study design, sample size); study population demographics (e.g., age, gender, race/ethnicity); intervention characteristics (e.g., workforce population, intervention components, BCTs); intervention focus area (e.g., mindfulness, light); sleep duration assessment (i.e., actigraphy, questionnaire); and findings related to sleep duration (e.g., change in sleep duration associated with exposure to the intervention). Several of the studies measured sleep duration using the Pittsburgh Sleep Quality Index (PSQI). When available, the PSQI sub-component score for sleep duration is displayed, which measured sleep in hours. However, some authors report only the global score which is coded so that higher scores are indictive of poor sleep (Buysse et al., 1989).
The BCTs utilized in the interventions were extracted using the taxonomy of BCTs offered by Michie et al. (2011). The taxonomy of BCTs outlines a wide array of intervention components and strategies. Cluster labels for BCTs, as defined in Michie et al.’s paper, included in our review are feedback/monitoring (self-monitoring BCT), repetition/substitution (practice sessions BCT), antecedents (environmental restructuring BCT), and comparison of behavior (behavioral modeling BCT). The BCT framework was adhered to with the exception of the addition of educational seminars because there was no corollary in the taxonomy. Two reviewers assigned BCTs to each study. Responses were discussed with all co-authors.
Eligible studies were assessed for quality utilizing a modified version of the Downs and Black quality assessment checklist (Downs & Black, 1998). The domains of reporting, external validity, internal validity/bias, internal validity/confounding, and power were assessed through the Downs and Black quality assessment checklist using a 27-item scoring system. To measure quality, we used a rating scheme that determined 21 (80.8%) and higher as high quality, 11–20 (42.4%–80.8%) as moderate quality, and less than or equal to 10 as poor quality (<42.2%) (Hartling et al., 2004). Quality ratings were determined for the studies in this systematic review independently by two reviewers. Discrepancies were adjudicated through discussion until consensus with all co-authors. All studies identified in this review were of moderate-to-high quality and were included in the synthesis and interpretation of results.
Data Analysis
Our original aim was to conduct a meta-analysis of studies examining workplace interventions among shift workers and sleep duration outcomes. Due to heterogeneity of the study populations, sample sizes, sleep duration measures, and study designs this analytical approach was not possible. According to Guolo and colleagues, a random effects model without significant heterogeneity of outcomes, study designs, or populations, can detect an effect size with 40 studies, however a review of studies with heterogeneity will require over 65 studies (Guolo & Varin, 2017). The number of studies identified in our review totaled 20, therefore proceeded with a systematic review qualitatively summarizing sleep duration-related outcomes of workplace health promotion programs. A systematic review of the literature on workplace interventions and their results pertaining to employee sleep is presented. We quantitatively summarized worksite-based interventions among employee shift-worker populations, measuring employee sleep duration as an outcome. We display results of the studies included in this review by study design (RCT vs. Prospective Observational and Other). We report the range of increases in sleep duration observed by the studies included in this review. Studies were further grouped by intervention types, (i.e., exercise, mindfulness, napping, sleep hygiene, CBT-I, shift timing, and light exposure).
Results
General characteristics of the studies are shown in Table 1. Studies used one of five designs: prospective observational, single-blind intervention, RCT, prospective pilot study, and randomized prospective. Among the studies, industries where interventions were conducted included health care/social assistance (n = 12, 60% of studies) (Arora, 2007; Basner et al., 2019; Cappuccio et al., 2009; Chang et al., 2017; Fang & Li, 2015; Jensen et al., 2016; Lee et al., 2014; Rahman et al., 2013; Volpp et al., 2012), manufacturing/construction (n = 1, 5%) (Hakola & Härmä, 2001), law enforcement (n = 1, 5%) (Orth-Gomer, 1983), airlines (n = 1, 5%) (Rosekind et al., 2006), firefighting (n = 1, 5%) (Sullivan et al., 2017), transportation (n = 1, 5%) (Pylkkönen et al., 2018), and oil and gas (n = 3, 15%) (Bjorvatn et al., 1999, 2007; Thorne et al., 2010). Target populations were mostly nurses (n = 8, 40% of studies) (Chang et al., 2017; Fang & Li, 2015; M. I. Härmä et al., 1988; Jensen et al., 2016; Lee et al., 2014; Rahman et al., 2013) and medical residents (n = 4, 20%) (Arora, 2007; Basner & Dinges, 2009; Cappuccio et al., 2009; Volpp et al., 2012), with the remaining studies addressing oil rig workers (n = 3, 15%) (Bjorvatn et al., 1999, 2007; Thorne et al., 2010), factory employees (n = 1, 15%) (Hakola & Härmä, 2001), police officers (n = 1, 5%) (Orth-Gomer, 1983), airline pilots (n = 1, 5%) (Rosekind et al., 2006), firefighters (n = 1, 5%) (Sullivan et al., 2017), and long-haul truck drivers (n = 1, 5%) (Pylkkönen et al., 2018). Mean intervention duration was 126 (SD = 187) days, and ranged from 7.7 days (Rosekind et al., 2006) to 722.5 days (Arora, 2007). Mean length of follow-up was 345 (SD = 666) days.
Summary Characteristics of Interventions for Shift Workers Measuring Sleep Duration (n = 20)
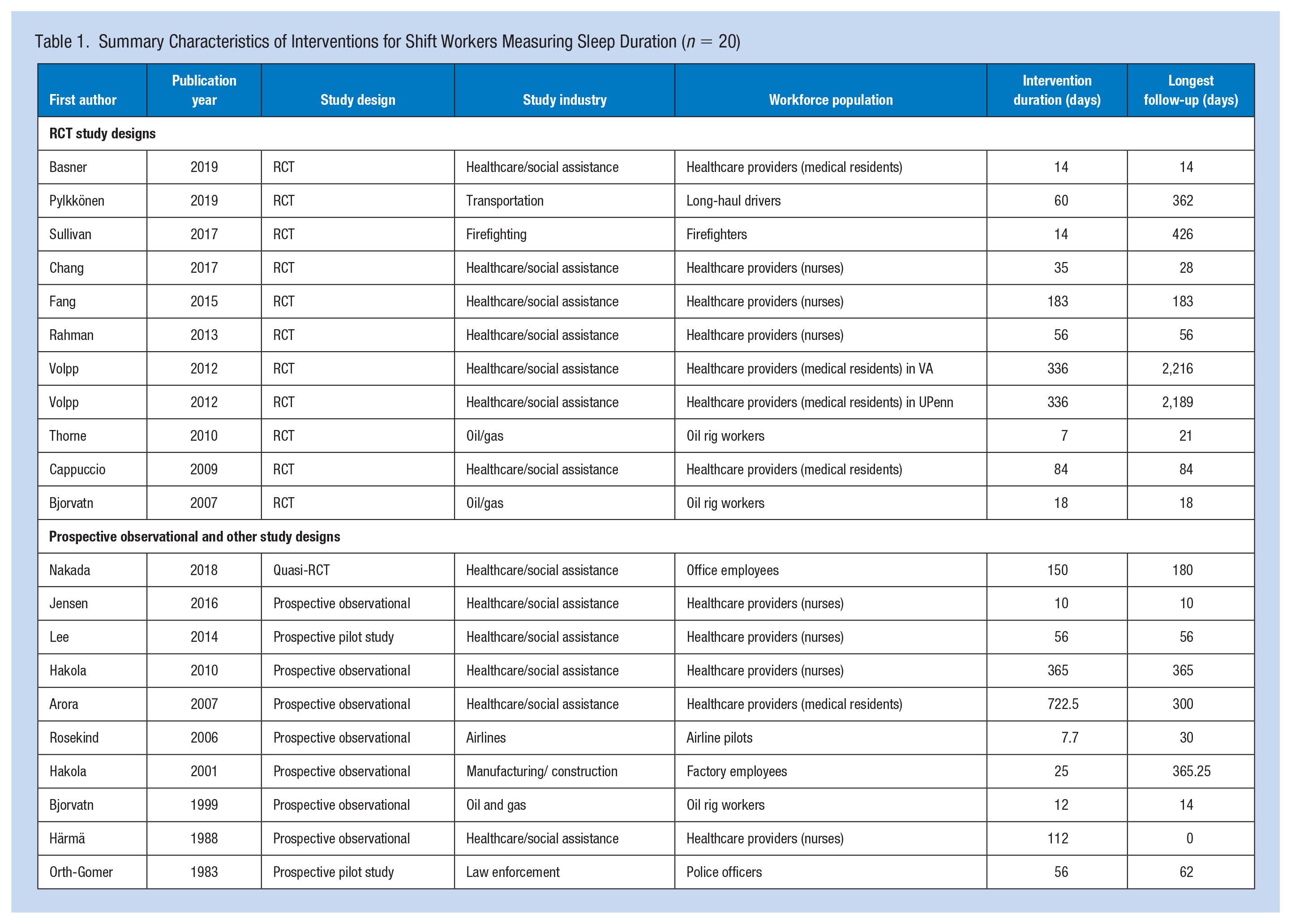
Table 2 displays characteristics of the sample populations in the selected studies. Sample size ranged from 9 (Rahman et al., 2013) to 1,189 (Sullivan et al., 2017) (M = 116 SD = 256, median = 52 participants). Regarding participants who were lost to follow-up, the studies ranged from 0 (Arora, 2007; Cappuccio et al., 2009; Chang et al., 2017; Hakola et al., 2010; Jensen et al., 2016; Rosekind et al., 2006; Orth-Gomer, 1983; Rahman et al., 2013) to 327 (Sullivan et al., 2017) participants (M = 57, SD = 241, median = 0). Participant mean age across the studies ranged from 27 (Volpp et al., 2012) to 45.5 (Lee et al., 2014) (M = 37, SD = 6.6) years. The mean proportion of males was 73% (27% female). Race/ethnicity was provided by two studies in total (Lee et al., 2014; Sullivan et al., 2017). Among those studies reporting race/ethnicity (n = 2, 11.8%), 90.2% were White (n = 1,091), 7.2% were Black/African American (n = 87), 1.0% Asian (n = 87), 0.5% were Latino/Hispanic (n = 6), and 1.2% other (n = 14). The most common geographic location was the United States (n = 7, 35%), followed by Finland (n = 4, 20%). Among the studies, the majority had a primary or secondary aim to improve sleep (n = 16, 80%).
Demographics of Shift Workers in Workplace Interventions Measuring Sleep Duration (n = 20 Studies)
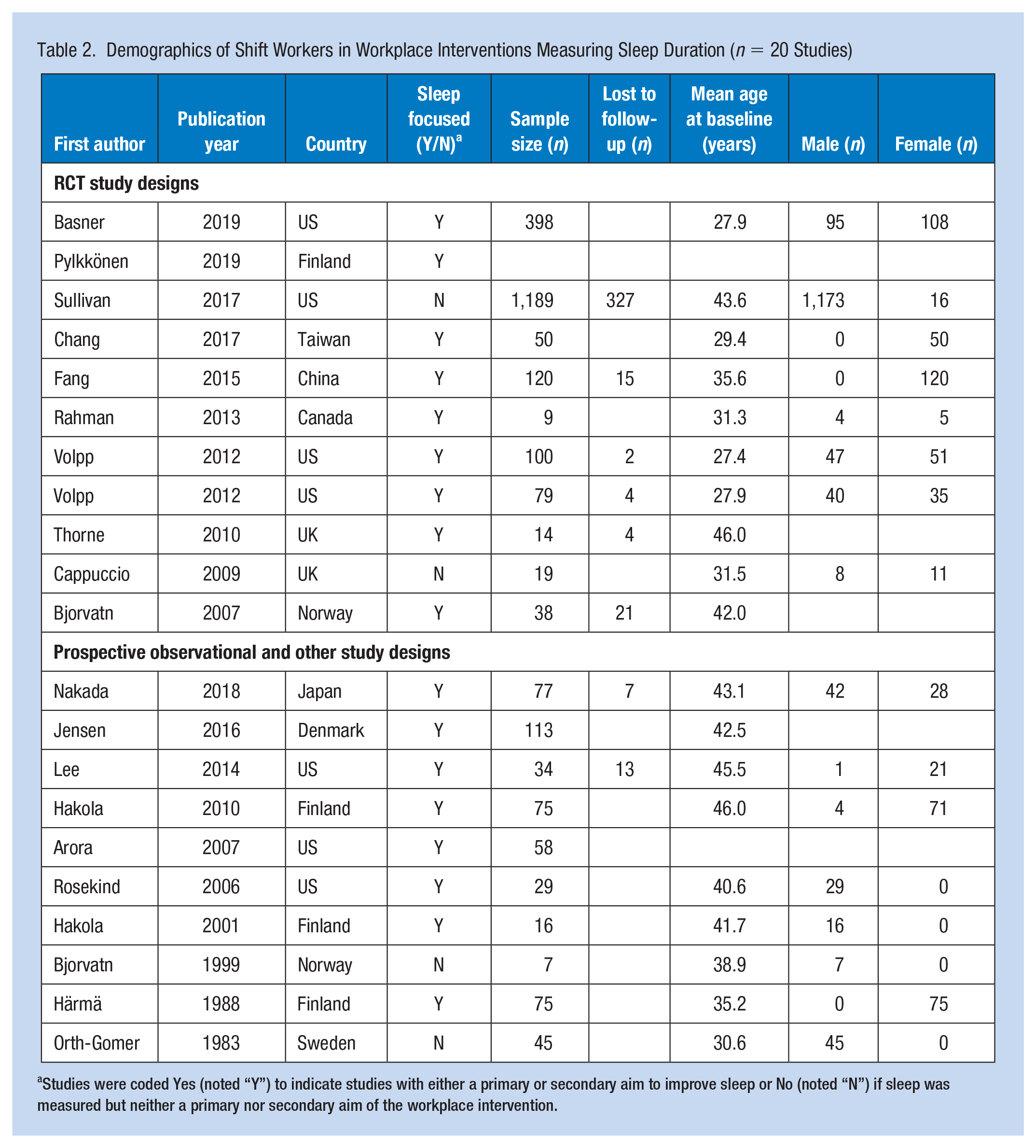
Studies were coded Yes (noted “Y”) to indicate studies with either a primary or secondary aim to improve sleep or No (noted “N”) if sleep was measured but neither a primary nor secondary aim of the workplace intervention.
Table 3 summarizes study details and intervention outcomes on employee sleep duration. The most common intervention types were light exposure (n = 5, 25%) (Bjorvatn et al., 1999, 2007; Rosekind et al., 2006; Rahman et al., 2013; Thorne et al., 2010) and shift timing (n = 5, 25%) (Cappuccio et al., 2009; Hakola & Härmä, 2001; Hakola et al., 2010; Orth-Gomer, 1983), followed by sleep hygiene (n = 4, 20%) (Arora, 2007; Nakada et al., 2018; Pylkkönen et al., 2018; Rosekind et al., 2006; Sullivan et al., 2017), mindfulness/stress reduction/yoga (n = 2, 10%) (Chang et al., 2017; Fang & Li, 2015), napping (n = 2, 10%) (Volpp et al., 2012), exercise (n = 1, 5%) (M. I. Härmä et al., 1988), and cognitive behavioral therapy for insomnia (CBT-I) (n = 1, 5%) (Lee et al., 2014). Sleep duration was most commonly assessed through actigraphy (n = 8, 42%) followed by self-report (n = 7, 37%). Regarding BCTs included in the 17 interventions, there were 7 BCTs from Michie et al.’s taxonomy (Michie et al., 2011) that were used in the interventions in this review. The most common BCTs were self-monitoring (6%), environmental restructuring (53%), and educational seminar (47%). Across the 19 interventions, 7 different BCTs were utilized; 32% interventions used 3 BCTs, 53% used 2 BCTs and 16% used 1 BCT.
Impact of Interventions for Shift Workers on Worker Sleep Behavior and Ratings of Study Quality (n = 20 Studies)
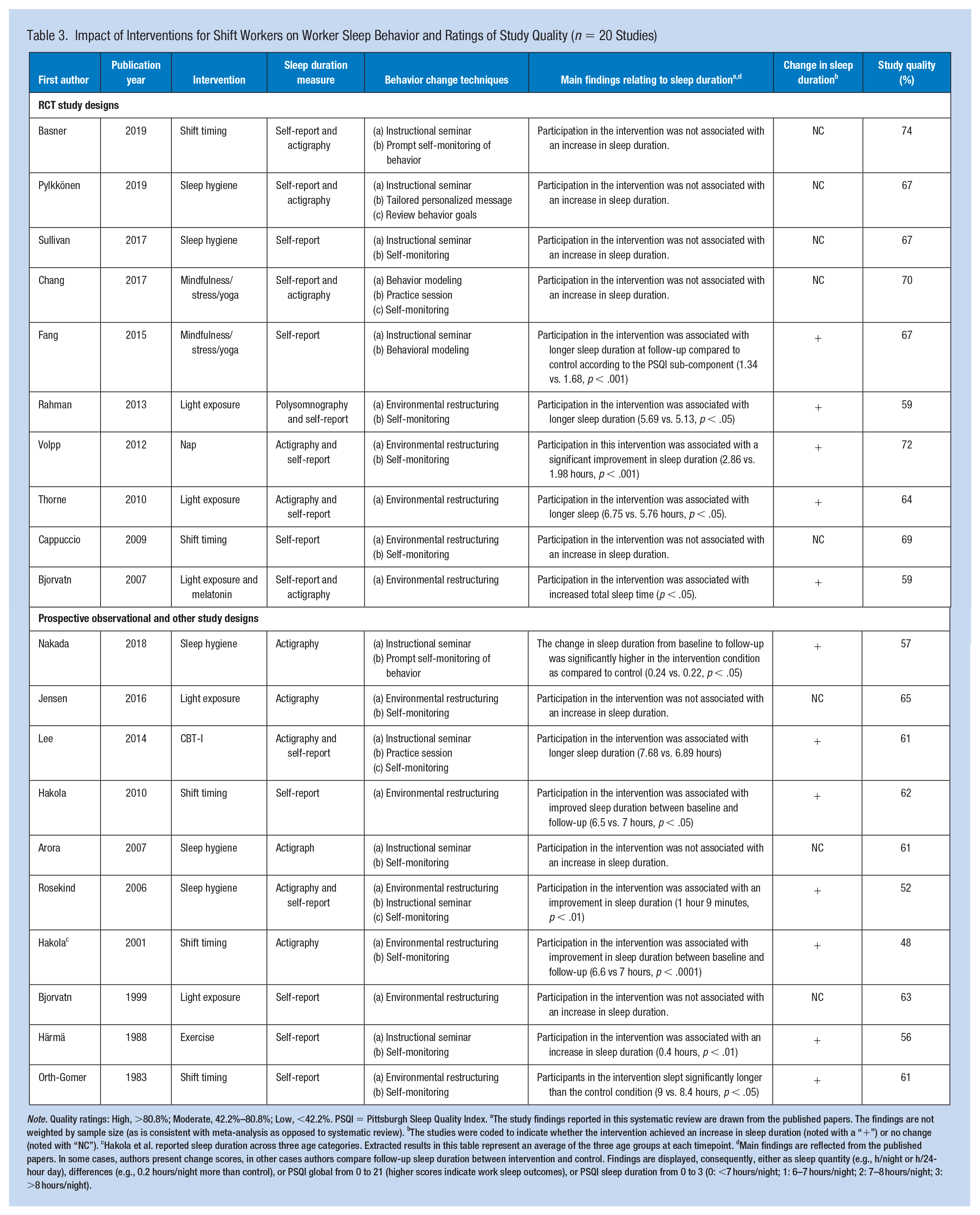
Note. Quality ratings: High, >80.8%; Moderate, 42.2%–80.8%; Low, <42.2%. PSQI = Pittsburgh Sleep Quality Index.
The study findings reported in this systematic review are drawn from the published papers. The findings are not weighted by sample size (as is consistent with meta-analysis as opposed to systematic review). bThe studies were coded to indicate whether the intervention achieved an increase in sleep duration (noted with a “+”) or no change (noted with “NC”). cHakola et al. reported sleep duration across three age categories. Extracted results in this table represent an average of the three age groups at each timepoint. dMain findings are reflected from the published papers. In some cases, authors present change scores, in other cases authors compare follow-up sleep duration between intervention and control. Findings are displayed, consequently, either as sleep quantity (e.g., h/night or h/24-hour day), differences (e.g., 0.2 hours/night more than control), or PSQI global from 0 to 21 (higher scores indicate work sleep outcomes), or PSQI sleep duration from 0 to 3 (0: <7 hours/night; 1: 6–7 hours/night; 2: 7–8 hours/night; 3: >8 hours/night).
In terms of results from the interventions on employee sleep duration, this review identified a positive result following intervention exposure on employee sleep duration in 11 studies (63.2%) (Fang & Li, 2015; Hakola & Härmä, 2001; M. I. Härmä et al., 1988; Lee et al., 2014; Nakada et al., 2018; Orth-Gomer, 1983; Rahman et al., 2013; Rosekind et al., 2006; Thorne et al., 2010; Volpp et al., 2012). A higher proportion of non-RCT studies (7 out of 10, 70%) achieved an increase in sleep duration than did RCT designs (4 out of 10 total studies, 40%). Examining results by intervention type, 60% (n = 3) of shift timing studies reported an improvement in sleep duration, 40% (n = 2) of sleep hygiene studies achieved an improvement in sleep duration, 50% of mindfulness and yoga interventions achieved an increase in sleep duration, and 80% (n = 4) of light exposure interventions achieved an improvement in sleep duration.
Regarding study quality, ratings ranged from 48.1% to 74.1%. According to Downs and Black, ≥80.8% indicates high quality, and rating between 42% and 80.8% indicates moderate quality. Study quality on average was 64% (SD = 7%), classifying most studies in the moderate quality range. Average study quality was higher among the RCT studies (66.8%, SD = 5.0%) than among the prospective observational and other study designs (58.6%, SD = 5.3%).
Discussion
We characterized the types of workplace-based interventions on shift workers that measured sleep duration. Most of the studies reported positive results of intervention exposure on employee sleep duration. Among the studies that improved sleep, increases in employee sleep duration ranged, for RCT studies, from 0.34 to 0.99 hours and, for non-RCT studies, from 0.02 to 1.15 hours. Our study results also illuminate the type of intervention that may be successful for improving sleep among shift workers, which includes interventions that aimed at addressing mindfulness and meditation. This is promising as shift work has been shown to impose significant adverse effects on sleep (James et al., 2017), and consequently, reduced workplace performance (Hui & Grandner, 2015; Kessler et al., 2011) and increased risk of accidents (Ryu et al., 2017). Another consequence of shift work and its impact on sleep hygiene due to work-related factors (work timings, light exposure, etc.) is its negative impact on health outcomes related to metabolic and gastrointestinal health, cancer, heart health, and mental health (James et al., 2017).
Interventions in this review were delivered to employees in a variety of industries, ranging from health care/social assistance to manufacturing/construction, law enforcement and firefighting. Among the employees included in the studies in this review were health care workers, airline pilots, factory employees, firefighters, oil rig workers, and police officers. Although there was a range of industries and occupations, one commonality among the occupational sectors represented in this review is the safety-critical nature of these occupations. Safety is a critical concern in these occupational groups as lapses in attention carry significant consequences in terms of motor vehicle crashes, medical errors, and other accidents. Research among medical residents shows that those working shifts of extended duration shifts are at a significantly increased risk of motor vehicle crashes (Barger et al., 2005). Also, research conducted among health care workers on shift schedules found that nearly 50% screened positive for a sleep disorder, and a positive screening result for a sleep disorder was associated with an 83% greater risk of a motor vehicle crash (Weaver et al., 2018). Given these safety concerns, it is critical that occupational health practitioners at worksites employing shift workers design programs to address sleep and fatigue, and improve sleep awareness about sleep disorders.
Average age of shift workers in this review was relatively young (37 years). Research has shown that long-term exposure to shift work carries the most pronounced risk for workers in terms of adverse health outcomes, such as cancer (Cordina-Duverger et al., 2018). On one hand, the fact that the average age of workers in this review was slightly younger could be a positive sign that worksites are intervening early with workplace sleep interventions among employees who may be new to shift schedules. On the other hand, it could be that workers who have been on shift schedules for longer periods of time may either be harder to reach, more likely to drop out of workplace interventions, or not a focus for workplace intervention designers and practitioners. Future research should endeavor to engage more workers who have had long-term exposure to shift work (e.g., 10 years or longer) and determine if these high-risk workers need a specific form of intervention that may differ from that for employees who are new to shift work.
The most common intervention types in this review were interventions addressing light exposure, shift timing, and sleep hygiene. This is not surprising because specific light exposure techniques are a well-documented means for shifting circadian phase (Czeisler et al., 1986; Rahman et al., 2017). In addition, sleep hygiene is often the first step for improving sleep health, and shift timing is a top concern for employers of shift workers. Among the studies in this review, nearly half of the sleep hygiene interventions increased sleep duration and half of the shift timing interventions elicited an increase in sleep duration. However, there is emerging consensus that sleep hygiene alone is insufficient, and instead that CBT-I techniques, such as relaxation strategies and stimulus control therapy, particularly for those with insomnia symptoms, must be considered to effect meaningful sleep health behavior change (Edinger Jack et al., 2021). In addition, the single studies that evaluated mindfulness, napping, and CBT-I, respectively, were all successful in increasing sleep duration which is significant in terms of suggesting effective workplace interventions in the future (Chang et al., 2017; Fang & Li, 2015; Lee et al., 2014; Volpp et al., 2012). The increase in employee sleep achieved by the CBT-I intervention is not surprising because CBT-I has been shown to be highly effective in a rigorous meta-analysis (Trauer et al., 2015).
More than half of the interventions that provided light exposure as a workplace-based intervention for shift workers were successful for improving sleep duration, and this intervention modality which may be an important intervention to be explored further in future work (Jensen et al., 2016; Rahman et al., 2013). A recent study shows that shift workers exposed to a bright light counter measure during their work shifts demonstrated better adaptation to night shifts as measured by the overlap in melatonin secretion with the sleep episode following the shift, and fewer cognitive deficits compared to those exposed to traditional indoor lighting (Lammers-van der Holst et al., n.d.) Therefore, it could be that the interventions that were included in our review that did not demonstrate a beneficial effect of light interventions on sleep may not have employed a light that was met the necessary threshold of bright light.
The workplace intervention approaches identified in this review vary widely in their feasibility and the intensity of resources that might be required for their successful implementation. For instance, CBT-I has been shown to be particularly effective when delivered one-on-one with a coach over a several week period (Wu et al., 2006). Therefore, delivering CBT-I in this manner may require a significant investment of employer resources, yet however, there are scalable, digital platforms that have been shown to deliver CBT-I principles effectively and at a lower cost (Espie et al., 2019). Mindfulness and meditation interventions may also benefit from widely available, low-cost digital meditation interventions, such as smartphone applications, which could be provided to employees at a relatively low cost per participant.
Overall, the findings of our review reveal the potential for workplace-based interventions to increase sleep duration among shift workers who are more likely to struggle with sleep. While the studies reviewed in this analysis did not evaluate the economic impact of improved employee health in shift workers as a result of a desirable increase in sleep duration, it is well-known that poor sleep leads to significantly elevated costs to workplaces and to society (Hafner et al., 2016). Moreover, it is possible that such costs are disproportionately higher among shift workers who are more likely to experience circadian misalignment and poor sleep hygiene. Future studies should examine the economic benefit of workplace-based interventions that are targeted at improving sleep duration in shift workers. This is particularly important, given previously published research evaluating a physical activity and nutrition workplace wellness program at a large retailer that found no significant change in objective health care utilization or cost measures as a consequence of participation in the workplace health intervention (Song & Baicker, 2019). Given the paucity of sleep-focused interventions across U.S. worksites (<10% of workplaces report such programs) (Robbins et al., 2020), yet their importance particularly for shift workers, it is possible that a comprehensive sleep enhancement program may be associated with cost savings for employers.
An important limitation of this review is that the studies identified had a high level of heterogeneity in study design, population, and intervention targets. In addition, our review identified a relatively small number of studies, and several studies included very small sample sizes (<20 employees). Therefore, although we set out with the aim of conducting a meta-analysis, doing so was not possible due to these limitations. Another limitation is that the majority of the studies included in this review investigated workplace-based interventions for employees in health care services industry, suggesting other industries and sectors that employ shift workers (i.e., law enforcement and transportation) may be lagging behind. Furthermore, several of the studies relied on self-reported sleep duration, which could result in bias or measurement error since individuals tend to overestimate their sleep duration (Jackson et al., 2018; Lauderdale et al., 2008). Thus, it is possible that there is measurement bias that inflated the outcomes of the interventions that were included in this review on employee sleep. In addition, only two of our studies characterized the study population by race and it is essential that studies in the future address more racially and ethnically diverse populations, since work environments have been shown to be differentially experienced by race/ethnicity and health interventions could impact certain populations differently (Ertel et al., 2011; Hurtado et al., 2012; Jackson et al., 2013, 2014). Although the studies included in this review were evenly split between RCT and other study designs, is a limitation that there were not more rigorous study designs, such as RCTs that evaluated workplace interventions and measured sleep. The RCT offers optimal, controlled conditions to explore the efficacy of a workplace intervention. It is possible that the pilot studies or other non-RCT studies included convenience samples and non-random allocation to interventions, which may be biased in that individuals who are perhaps already motivated to improve their health are more willing to sign up than those who may be at higher risk. Also, our study focused on sleep duration. Including other sleep outcomes, such as sleep quality, may be useful in future interventions. Additional outcomes that are direct sequalae of insufficient sleep duration or inadequate sleep quality, such as performance, accidents, or biomarker-derived measures of health, would also be fruitful areas for future interdisciplinary inquiries.
Given the potential detrimental impact of shift work on sleep, it is promising that the findings from our review suggest that sleep duration can be lengthened with evidence-based workplace interventions such as yoga or mindfulness interventions for shift workers. Future research may examine the specific mechanisms at the employee, intervention, or environmental levels that are associated with favorable changes to shift worker sleep duration. At the employee-level, future research may capture more detailed demographic factors (e.g., race/ethnicity, age, and income) as few studies in this review reported these details. At the intervention level, the BCTs identified in our study, such as environmental restructuring and instructional seminars, may be a fruitful area for future research. Specifically, research could examine which combination of BCT (e.g., environmental restructuring) and intervention target (e.g., sleep hygiene) would be most optimal for sleep duration improvement. This may be important, for it stands to reason that an intervention imparting instructional seminars as the primary BCT for an intervention designed to increase naps among shift workers may be most successful if worksites incorporated an environmental restructuring BCT, such as installing nap rooms for employees. Future research may also consider designing and evaluating multi-modal interventions, or interventions that combine multiple BCTs (e.g., environmental restructuring and instructional seminars) with multiple intervention targets (e.g., sleep hygiene and mindfulness).
Identifying the most optimal intervention dose and exposure is a ripe opportunity for future research. For instance, research could analyze intervention duration and outcome to elucidate the duration and exposure characteristics that will increase the likelihood of a successful outcome. This may be particularly useful for worksites with limited resources. At the environmental level, research may consider the workplace-related mechanisms that are associated with favorable intervention outcomes, such as the presence of leaders who support employee health. Another opportunity for future research is to examine additional outcomes of increasing shift worker sleep duration, such as improvement on cardiovascular or other desirable endpoints. This type of research should further embolden worksites employing shift workers to make worker sleep a priority. Furthermore, fewer than half of the studies included an RCT design, although these studies had higher overall quality ratings and more favorable results. Future research may consider employing these more rigorous designs where appropriate.
Another important area to study is the impact of workplace-based interventions on sleep among older shift workers due to an aging population that will be increasingly forced to work into older age. While this study only examined sleep duration, further studies could also benefit from additionally assessing sleep quality as a metric when evaluating various interventions. For future interventions, it would be beneficial to provide a deeper and broader understanding of the different types of employee shift worker populations as well as their job demands as we examine the impact of specific workplace-based health interventions.
Implications for Occupational Health Practice
This systematic review of the scientific literature provides preliminary evidence for the use of workplace-based health interventions to increase sleep duration among shift workers. These interventions focused on sleep hygiene, shift timing, CBT-I, mindfulness/stress reduction, light therapy, and napping. Since shift workers are more vulnerable to poor sleep hygiene and poor lifestyle behaviors, workplace-based health interventions that target sleep and health are important for this population. While more research is necessary, workplace productivity and health outcomes may be additional endpoints to assess for workplace health promotion programs.
More than half of the employee health interventions resulted in an increase in sleep duration, and yoga or mindfulness interventions appear to be a promising approach for improving sleep. Poor sleep among shift workers can yield significant, adverse outcomes in terms of reduced productivity and increased rates of accidents, absenteeism, and illness. The worksite holds considerable promise as a venue for delivering programs and policies that aim to improve sleep and ultimately health among shift workers.
Summary
Poor sleep among shift workers can yield significant, adverse outcomes in terms of reduced productivity and increased rates of accidents, absenteeism, and illness. The worksite holds considerable promise as a venue for delivering programs and policies that aim to improve sleep and ultimately health among shift workers.
The findings of our review reveal the potential for workplace-based interventions to increase sleep duration among shift workers who are more likely to struggle with sleep.
Nearly half of the sleep hygiene interventions increased sleep duration and half of the shift timing interventions elicited an increase in sleep duration among shift workers.
The two mindfulness studies improved sleep duration and the single studies that dealt with napping and CBT-I were all successful in increasing sleep duration in shift workers which is significant in terms of suggesting effective workplace interventions in the future.
More than half of the employee health interventions resulted in an increase in sleep duration, and yoga or mindfulness interventions appear to be a promising approach for improving sleep.
Footnotes
Appendix
Acknowledgements
The authors would like to thank Lydia Feinstein for her assistance in preparing the manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Outside of the current work, Orfeu M. Buxton discloses that he received subcontract grants to Penn State from Proactive Life LLC (formerly Mobile Sleep Technologies) doing business as SleepScape (NSF/STTR #1622766, NIH/NIA SBIR R43-AG056250, R44-AG056250), received honoraria/travel support for lectures from Boston University, Boston College, Tufts School of Dental Medicine, New York University, and Allstate, and received an honorarium for his role as the Editor-in-Chief of Sleep Health (![]() ). Outside the current work, Rebecca Robbins discloses that she has received consulting fees from SleepCycle, Denihan Hospitality, and Deep. The others have no conflicting interests to report.
). Outside the current work, Rebecca Robbins discloses that she has received consulting fees from SleepCycle, Denihan Hospitality, and Deep. The others have no conflicting interests to report.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work, in part, was funded by the Intramural Program at the NIH, National Institute of Environmental Health Sciences (Z1AES103325-01), and the National Institute of Health (K01HL150339).
Author Biographies
Rebecca Robbins is an Instructor in Medicine at Harvard Medical School and an Associate Scientist at Brigham and Women’s Hospital.
Phoenix Underwood is a medical student at the University of Maryland School of Medicine.
Chandra L. Jackson is the Earl Stadtman Investigator at National Institute of Environmental Health Sciences (NIEHS).
Giradin Jean Louis is Professor in the Department of Population Health and Professor in the Department of Psychiatry, NYU School of Medicine
Shreya Madhavaram is an internal medicine resident at MetroWest Medical Center in Framingham, Massachusetts.
Shiana Kuriakose is in the Department of Science and Technology Studies at Cornell University.
Dorice Vieira is the Associate Curator of the NYU Health Sciences Library at the NYU Grossman School of Medicine.
Orfeu M. Buxton is Elizabeth Fenton Susman Professor of Biobehavioral Health at The Pennsylvania State University.