
Abstract
Background:
Flagging is a standardized way to communicate the risk of patient violence to workers. We add to the limited body of research on flagging by describing hospitals’ approaches to and challenges with flagging patients with a history of violent behavior.
Methods:
We used a qualitative case study approach of hospitals in Ontario, Canada and their patient flagging practices. Key informants and our advisory committee identified 11 hospitals to invite to participate. Hospitals assisted in recruiting frontline clinical and allied health workers and managers to an interview or focus group. A document analysis of hospitals’ flagging policies and related documents was conducted. Thematic analysis was used to analyze interview and focus group data.
Findings:
Five hospitals participated. Of the five hospitals, four had a flagging policy where frontline clinical workers (n = 58), frontline allied health workers (n = 31), and managers (n = 42) participated in an interview (n = 43) or focus group (n = 15). Participants described three challenges: patient stigmatization, patient privacy, and gaps in policy and procedures.
Conclusion/Application to practice:
Flagging patients with a history of violent behavior is one intervention that hospitals use to keep workers safe. While violence prevention was important to study participants, a number of factors can affect implementation of a flagging policy. Study findings suggest that hospital leadership should mitigate patient stigmatization (real and perceived) and perception of patient rights infringement by educating all managers and frontline workers on the purpose of flagging and the relationship between occupational health and safety and privacy regulations. Leadership should also actively involve frontline workers who are the most knowledgeable about how policies work in practice.
Background
Violence toward health care workers is a global crisis (World Health Organization, 2021) with psychological, emotional, and career consequences (Brophy et al., 2018; Rosenthal et al., 2018). Hospital workers experience some of the highest rates of patient violence (Hango & Moyser, 2018; Liu et al., 2019, U.S. Bureau of Labor Statistics, 2020). Despite research on the prevalence of violence in health care and its deleterious impact on workers, health care leaders remain challenged to prevent and mitigate patient violence (Gates et al., 2011; Havaei et al., 2020; Lanctôt & Guay, 2014; Phillips, 2016).
One approach to preventing and managing the incidence of violence is by flagging, which is a system of communicating safety-related concerns like a patient’s history of violent behavior (HOVB) to workers who may encounter the patient (Public Services Health & Safety Association [PSHSA], 2017a). The purpose of flagging patients who have an HOVB is to alert those with a need to know of the potential for risky behaviors. It is not to identify specific diagnoses or to label patients (Nova Scotia Health Research Foundation [NSHRF], 2017; PSHSA, 2017a).
Flagging involves sharing information using visual and/or electronic flags. These flags draw workers’ attention to the risk so that they can protect themselves and others, and implement safety protocols and behavior care plans. Flags are grouped under two categories: medical-record flags and visual flags (PSHSA, 2017a) both of which can be either electronic or paper-based. Electronic flags can be active or passive. Active flags are pop-ups on the computer screen. They require the worker to acknowledge seeing the flag before their work flow can continue. Passive flags are always visible in a prominent place on the electronic medical-record computer screen and do not require the worker to acknowledge them. In paper-based medical records, flags are often color-coded and used in conjunction with other flags such as a symbol on a “face-sheet” at the front of the chart. Other examples of paper-based flags include pull-tab sheets that extend past the top edge of the chart or an adhesive dot on the spine of the chart. Additional visual cues are built into the care environment for quick recognition of risk. They include wristbands of a specific color; symbols on signage placed above the patient’s bed, door, or assignment boards; and on mobility aids (PSHSA, 2017a).
In Ontario, Canada, employers are required under the Occupational Health and Safety Act (OHSA, 1990) to take every precaution reasonable in the circumstances to protect workers against hazards such as workplace violence. Bill 168 (2009), “An Act to Amend the Occupational Health and Safety Act With Respect to Violence and Harassment in the Workplace and Other Matters,” imposed new obligations. One obligation is that the employer provides to a worker information including personal information related to a risk of workplace violence from a person with an HOVB if (a) the worker can be expected to encounter this person in his or her work and (b) the risk of workplace violence is likely to expose the worker to physical injury. The flagging program is one way a hospital can operationalize this legal obligation and is a common approach to workplace violence prevention (WVP) in health care (Kling et al., 2011).
Drummond et al. (1989) conducted the first known study of flagging patient violence risk in U.S. Veterans Health Administration (VHA) hospitals. The authors found a 92% mean decline in violent incidents 1 year after the flagging intervention was implemented compared with 1 year prior to patients being flagged. Unlike Drummond et al., Kling et al. (2011) found that although violent incidents decreased during the implementation period of an Alert System intervention (including flagging practices), they increased after the implementation period ended. The authors speculated that the return to pre-implementation rates (and higher) may have been due to intervention sustainability issues or increased reporting due to heightened program awareness. Paterson et al. (2019) found a decrease in flag-related incidents for 61% of patients, but an increase in incidents for 28% of patients, and no change in number of incidents for 11% of others. The authors discussed that the flags have some value as a communication mechanism and that the reduction in incidents may have been because of other reasons such as improved mental health due to hospitalization. Despite the question of how effective flagging is on rates of violence, research shows that flagging heightens health care workers’ vigilance of the potential for danger (Burkoski et al., 2019; Paterson et al., 2019). This awareness may lead workers to proactively seek and implement preventive safety precautions such as requesting immediate security presence.
The purpose of this study was to describe hospitals’ approach to flagging patients with an HOVB and the challenges related to flagging. We focused on stigmatization, patient privacy, and policy and procedural gaps. This study was part of a qualitative multiple-case study (Stake, 2005) to examine hospitals’ measures to prevent workplace violence. In the main study (Kosny et al., 2018), flagging was one of several interventions that hospitals implemented as part of their WVP programming and efforts to comply with the OHSA (1990).
Methods
This was a qualitative multiple-case study of five hospitals’ flagging practices and challenges. The University of Toronto Research Ethics Board and four of the five hospitals which had their own research ethics board approved the study protocol.
Sampling and Recruitment
Expert sampling was used to recruit eight external key informants. They included senior policy makers and senior leaders from health and safety associations, unions, and training organizations. We also recruited a mix of high-performing and low-performing hospitals based on measures that assessed their WVP implementation in Ontario, Canada. This approach is aligned with maximum variation sampling which allowed us to describe themes or outcomes that cut across organizational variation (Patton, 2015). High-performing hospitals (a) proactively invested in workplace violence strategies prior to the effective date of the new requirements under the OHSA; (b) observed declines in incidents of workplace violence following investments; or (c) adopted strategies beyond basic requirements of the legislation. Low-performing hospitals (a) received orders from the Ministry of Labour, Training and Skills Development related to requirements for WVP that were previously unmet; (b) had elevated incidents of violence for over a year, including claims associated with workplace violence; or (c) invested in improvements but struggled to bring down incidents of workplace violence. To reach our target sample of hospitals, the key informants and our advisory committee identified six high-performing and five low-performing hospitals, and suggested we have a representation of small-, medium-, and large-sized hospitals in rural, suburban, and urban geographical areas. Hospitals were contacted by the principal investigator and/or research manager by calling or emailing an administrator or director of occupational health and safety. Once contact was established, phone meetings were conducted with the hospital’s liaison to discuss the study and finalize the data collection plan. The hospital liaisons recruited (a) management representatives (herein: managers) responsible for leading and overseeing WVP initiatives, and (b) frontline clinical and allied health workers who could provide insights into how WVP policies and programs were operating in practice. This included workers on committees such as the Joint Health and Safety Committee (JHSC), a committee of management representatives and unionized workers who meet regularly to deal with health and safety issues, Code White committee (managed violent incidents in progress), or WVP committee where present. In three hospitals, hospital liaisons recruited mainly JHSC, Code White, or WVP committee members to participate in focus groups (FGs).
Frontline workers and managers were invited to participate in an FG and a one-on-one interview, respectively. Frontline workers were provided the option to participate in an interview if unable to attend or felt uncomfortable participating in an FG. Focus groups with members of the same committee (e.g., JHSC) contained both frontline workers and managers. We aimed to conduct five to eight interviews with managers and three FGs per hospital with six to eight frontline workers in each. Participants were offered a CAN $25 gift card honorarium as a token of appreciation. Hospitals were also offered a worker replacement fund of CAN $55/hour per participant although none took up this offer.
Data Collection
External key informants were interviewed between May and August 2016 before hospital data collection. Interviews were 60 minutes and audio-recorded with consent. A semi-structured interview guide was developed by the research team with input from our advisory committee. Interview questions addressed key informants’ perspectives on the design and development of workplace violence legislation and implementation supports and challenges. Sample questions included the following: Considering violence in hospitals, what are the most pressing issues that need to be addressed from your perspective? What do hospitals struggle with the most and why?
Next, we conducted interviews and FGs with managers and frontline workers, respectively, between October 2016 and May 2017. Interviews were in person or via telephone (30–60 minutes); FGs were in person (60–90 minutes). Semi-structured interview and FG guides were developed by the research team with input from our advisory committee. All participants consented to participate and being audio-recorded; recordings were transcribed verbatim. A sample interview question is as follows: How are frontline workers informed about patients who have a potential for violence or who have been violent in the past? We asked FG participants questions about components of their WVP program including flagging, for example: How are workers informed about patients with a history of violence? Which frontline workers have access to flagging information? Are there any challenges related to flagging?
In addition, we requested written flagging policies, evaluation reports, training materials, and committee documents from each hospital. We examined the documents to analyze the extent to which the hospitals were adhering to their WVP policies after analyzing the key informant, interview, and FG data.
Data Analysis
Thematic analysis was used which involved organizing content systematically and identifying, analyzing, and reporting themes (Braun & Clarke, 2006). Inductive and deductive coding approaches were used. The research team read a sample of transcripts and established a preliminary list of codes. The content assigned to codes was reviewed, and a coding manual was developed. Transcripts were coded by one researcher and then sent to a second researcher to add additional codes or to identify and discuss sections that may have been miscoded. Coding was not blinded because it was important for our research team to know when there were discrepancies in coding. When the first and the second coders disagreed with the way data were coded, this was an opportunity to discuss and refine the code. It also ensured that coders were “using” codes in the same way, meaning that the entire team had a shared understanding of what the code meant and how it applied to our data. Data assigned to each thematic code were reviewed to facilitate a within-case and cross-case analysis noting patterns and contradictions. The focus was not strictly about prevalence but whether the theme captured key insights about the data in relation to the research question (Braun & Clarke, 2006). Transcripts were entered into NVivo (Version 10) for data storage and coding.
Results
Eight external key informants and the study advisory committee identified 11 high-performing and low-performing hospitals in the province of Ontario. Eight hospitals were invited to participate, and five agreed to participate. Two hospitals declined without giving a reason, and one did not respond to our invitation. The two hospitals that declined were both small—one in a rural area and the other in a suburban area. The non-responsive hospital was medium in size in a rural area. The three hospitals from the original list of 11 were not contacted because we reached our target sample size.
The number of participants and type of employee group per site are listed in Table 1. Hospitals represented a mix of urban (n = 2), suburban (n = 2), and rural (n = 1) high-performing (n = 3) and low-performing (n = 2) hospitals, ranging from 40 to 1,000 beds. One hospital did not have a flagging policy and was excluded from the analysis. Across the four hospitals with a flagging policy, 58 frontline clinical workers, 31 frontline allied health workers, and 42 managers participated for a total of 131 participants. We conducted 43 interviews and 15 FGs with 88 participants.
Number of Interview and Focus Group Participants Among Study Hospitals (n = 4) and Hospital Workers (n = 131)
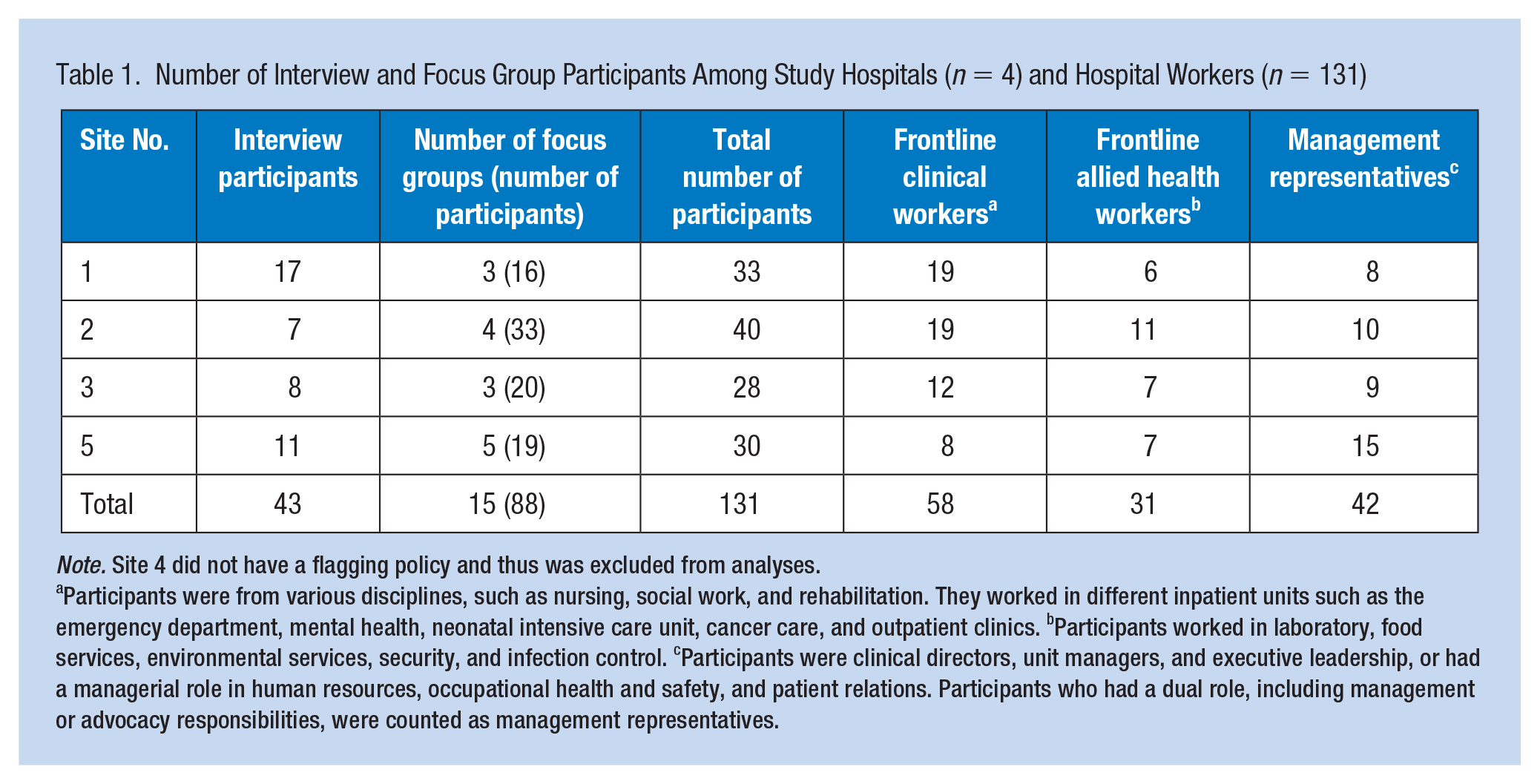
Note. Site 4 did not have a flagging policy and thus was excluded from analyses.
Participants were from various disciplines, such as nursing, social work, and rehabilitation. They worked in different inpatient units such as the emergency department, mental health, neonatal intensive care unit, cancer care, and outpatient clinics. bParticipants worked in laboratory, food services, environmental services, security, and infection control. cParticipants were clinical directors, unit managers, and executive leadership, or had a managerial role in human resources, occupational health and safety, and patient relations. Participants who had a dual role, including management or advocacy responsibilities, were counted as management representatives.
Three hospitals had a fully operational flagging policy and one hospital was pilot testing their flagging policy during the study. The general perspective of frontline workers and managers across hospitals was that flagging was an important practice to forewarn workers of a risk of violence. Methods to communicate varied but included a combination of symbols, colors, signage, wristbands, face sheets on charts, and electronic alerts. Verbal communication was a common approach which was not necessarily formalized in policy. Rather, workers and managers verbally shared violence-related information during usual practices such as during shift change or team huddles.
Table 2 illustrates the main components of hospitals’ flagging policy. Hospitals varied in their flagging approach. For instance, in medium-sized hospitals, clinicians had the authority to initiate flags, whereas in the large hospitals, managers had the authority. Policies also addressed worker responsibilities, whether or not security personnel are involved, flag types, flag duration, and the process to inform patients about their flagged status in their medical record. Hospitals relied on visual alerts such as signage and wristbands to communicate risk of violence to workers who do not have access to patient medical records (e.g., dietary aides, housekeeping staff). Qualitative data revealed three major challenges when flagging patients with an HOVB: patient stigmatization, patient privacy, and gaps in policy and procedures.
Characteristics of Study Hospitals (n = 4) and Their Flagging Policy Components
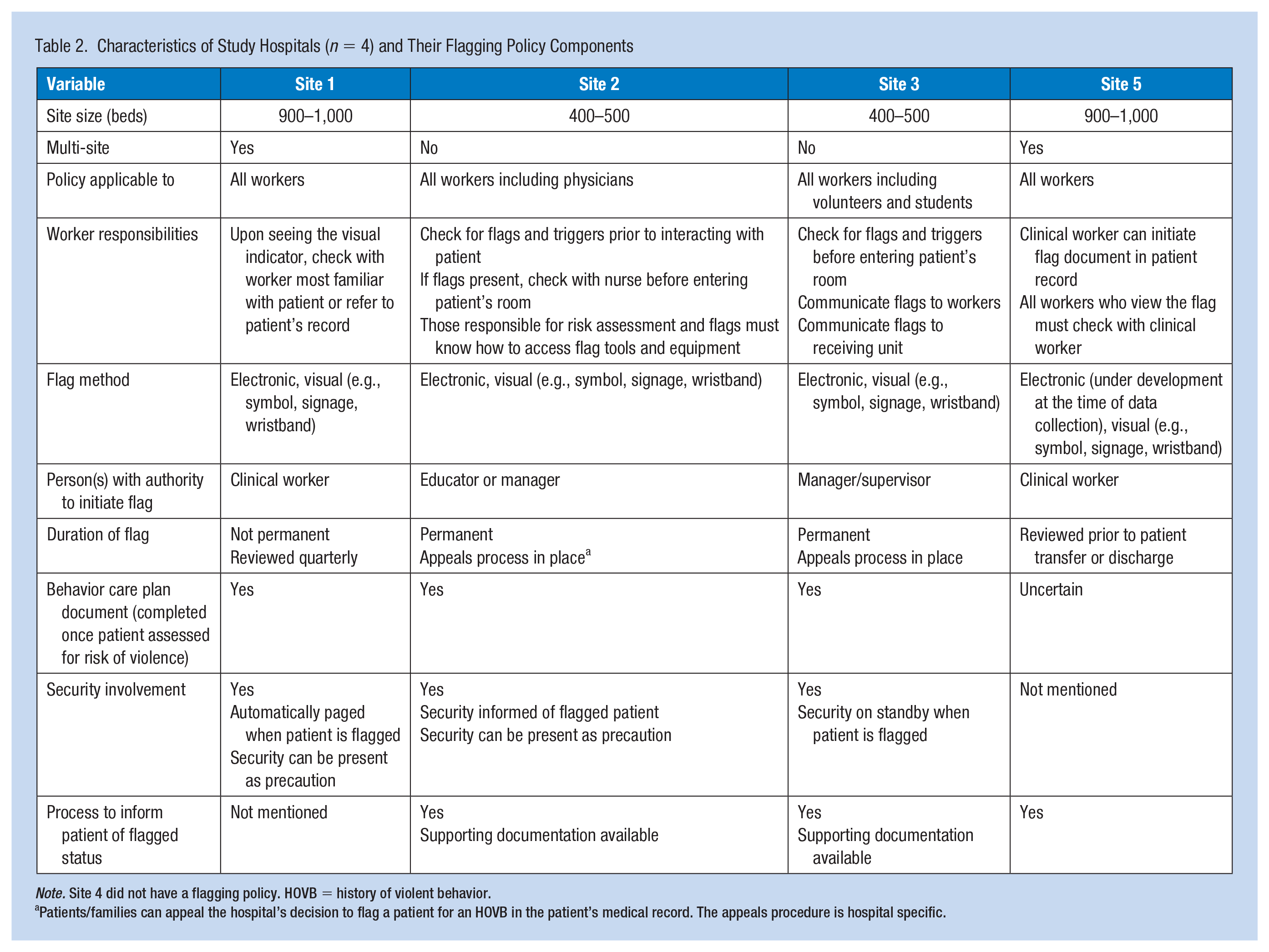
Note. Site 4 did not have a flagging policy. HOVB = history of violent behavior.
Patients/families can appeal the hospital’s decision to flag a patient for an HOVB in the patient’s medical record. The appeals procedure is hospital specific.
Patient Stigmatization
Some frontline workers and managers were concerned that flagging patients with an HOVB is stigmatizing. Participants feared that flagged patients would not receive quality care. Participants were particularly concerned about patients who exhibited violent behavior due to their medical condition (e.g., mental health illness or dementia) or what participants perceived as “one-off” situations, such as anesthesia-induced disorientation post-surgery. For example, frontline workers discussed situations when patients are refused admission to long-term care homes due to the flagged status in their medical record. Pressures to discharge patients to make beds available for incoming patients prompted some workers to omit violent behaviors from transfer of care forms.
Both frontline workers and managers in mental health were concerned about flagging patients who, according to participants, were already stigmatized because of their medical condition. It was explained that flagging as a communication process is not clinically beneficial as many mental health patients have an HOVB. If all of these patients are flagged, the flags would become meaningless, and workers would ignore them. A mental health program director speculated on the repercussions of flagging mental health patients.
I think it [flagging] is enormously stigmatizing. For an illness that the symptoms make people do things that they wouldn’t normally do, to flag them in that way I think is doubly stigmatizing . . . I think that flagging is dangerous because I think people are going to get hurt . . .
On the contrary, frontline workers were frustrated about the hospital’s differential approach to mental health patients with an HOVB. Focus group participants pointed out that the hospital’s effort to not stigmatize mental health patients is in fact stigmatizing them by treating them differently than other patients. One FG participant explained, . . . if you have a violence prevention program for everybody and then you’re saying we’re not going to do this for mental health, it’s actually the hospital’s mental health program who is stigmatizing those mental health patients . . . putting their own worker at much greater risk.
Patient Privacy and Worker Safety
Some frontline workers and managers perceived efforts to protect worker safety by flagging patients with an HOVB conflicted with patients’ right to privacy. Particularly among participants not involved in policy development or committee work, confusion existed about which act, the OHSA (1990) or the Personal Health Information Protection Act (PHIPA, 2004), takes precedence specific to the disclosure of personal information of patients with an HOVB. This perceived legislative conflict sometimes left participants uncertain about the kind of information that could be shared and with whom.
Several frontline workers believed that their hospital focused on patient privacy to the exclusion of worker safety. One nurse who was badly injured by a patient several years prior to the study remained in legal conflict with her employer over return-to-work accommodations. From the nurse’s perspective, the original conflict was centered on her employer’s stance that patient privacy is more important than worker safety. She explained, In Bill 168 it’s very clear. It’s very clear. There’s a clause even in PHIPA, and they [management] said no. They are hiding behind PHIPA. I’ve been off work . . . because they were saying PHIPA trumps your safety.
An external key informant who worked for a union echoed the nurse’s claim that some employers focus more on patient privacy than worker safety. On the contrary, one director believed that the pendulum has swung too far toward worker safety: “I think the shift is a little too heavy towards protecting the worker and a little too light in meeting the needs of the patients.”
Some patients voice their displeasure with being flagged. One director shared that flagged patients feel singled out and feared being treated differently when required to wear a different wristband, for example. However, some participants did not let the protests prevent them from implementing flagging policy and procedures. The same director discussed the hospital’s continued efforts to find the right balance between patient privacy and worker safety, and emphasized that flags are not to label patients but to communicate with workers that a risk of violence exists.
Gaps in Flagging Policy and Procedures
Several gaps in the flagging policy and procedures across hospitals were noted. Participants were concerned about the permanence of flags in patient medical records, the lack of flag gradation, lack of information flow between clinical and allied health workers and between locations (within or between hospitals), lagged flag initiation, and incompatible inpatient and outpatient technology systems. For example, frontline participants revealed that information about patients’ HOVB was commonly omitted from transfer of care forms whether the transfer was between units or facilities. Allied health workers discussed the difficulty with locating a patient’s nurse from whom to seek instructions on how or whether to encounter a flagged patient, as directed by signage. In addition, both frontline workers and managers took issue with the same flags being applied to a patient who had been verbally aggressive and to a patient who had physically assaulted and injured a worker. They were concerned that a “one flag for all” approach would overestimate the risk in some instances and underestimate it in others.
Hospitals experienced delays communicating about flagged patients due to system lags or procedures that delayed decision making. At one hospital, alerts were received hours after being entered into their electronic system. At another hospital where only managers had the authority to initiate flags, workers initiated temporary flags when incidents occurred during the evening or weekends for managers to review and authorize when back to work.
The policy to permanently flag a patient with an HOVB in their medical record was a contentious issue, resulting in non-compliance of some workers. In two hospitals, a flag remained on a patient’s record even if the patient had visited the hospital numerous times since the initial flag without incident. One director talked about frontline workers’ issue with flagging permanency: If patients are identified as violent or with a history of violence, they’re flagged permanently. You could have somebody who is upset about the loss of a child and swears, and somebody who lashes out with a weapon and hurts somebody, or kills somebody even, and they’re flagged in the same way. There’s no gradation. That’s the biggest problem, I think. What ends up happening is it doesn’t work for workers, so they sort of pick and choose how to apply it.
Discussion
Flagging is a standardized way to communicate the risk of violence to workers to protect their safety. In Ontario, Canada, employers are required under the OHSA (1990) to take every precaution reasonable in the circumstances to protect workers against hazards such as workplace violence. Bill 168 (2009) imposes new obligations with respect to workplace violence. One such obligation is that the employer provides information to workers, including personal information related to a risk of workplace violence from persons with an HOVB if workers can be expected to encounter these persons in their work and the risk of workplace violence is likely to expose workers to physical injury. The flagging system is a hospital’s operationalization of their legal obligations.
In this article, we describe four Ontario hospitals’ approach to and challenges with flagging patients with an HOVB. It is important to emphasize that the challenges were not with the practice of flagging. Rather, both employees and managers reported fears of patient stigmatization, training needs regarding occupational health and safety and privacy legislations, and policy and procedural gaps affecting the success of implementing a flagging program.
Four of the five hospitals had a formal flagging policy and procedures, and in general, participants expressed positive views about flagging similar to other studies (e.g., Burkoski et al., 2019; Paterson et al., 2019). One hospital did not meet our criteria for inclusion because they did not have a flagging policy at all, despite legislation requiring measures and procedures to communicate personal information about a person’s HOVB.
In our study, fear of stigmatizing patients by flagging them for an HOVB was present in frontline workers and managers. Examples of participants themselves stigmatizing patients were not provided. However, participants discussed stigma occurring when hospitals attempt to transfer flagged patients to another health care facility and are subsequently denied admission due to their flagged status. Anticipating this response, workers withhold HOVB information from receiving facilities to ensure discharge, inevitably creating an unsafe situation unbeknown to other health care providers. This system-level stigma may be due to hospitals’ lack of resources and infrastructure to adequately care for patients with increased behavioral needs. The deaths of two long-term care resident patients and injury to a third resident patient in 2001 by a resident patient with an HOVB toward his family demonstrate the significant impact of withholding information. The family doctor intentionally withheld the information on the admission application to the long-term care home, believing the disclosure to be a breach of confidentiality (Priest, 2004).
Limited literature exists on the impact of flagging patients with an HOVB on health care workers’ subsequent behaviors; however, it is an acknowledged concern (Andress et al., 2018; “‘Flagging’ Disruptive Patients Reduces Violence: Portland VA Program Cut Incidents by 92%,” 2002; Loftus et al., 2019; NSHRF, 2017; Wyatt et al., 2016). Hospitals across Ontario, Canada, are considering stigma in the planning stages of their WVP and flagging programming. For instance, a consortium of seven hospitals, The Joint Centres for Transformative Healthcare Innovation (referred as The Joint Centres), use purple on their visual flags (e.g., wristbands, signage) to alert workers to the necessary precautions without revealing personal information that may result in stigmatization (Andress et al., 2018). During a Toronto, Ontario, hospital’s development of their aggressive behavior risk program (Loftus et al., 2018, 2019), the project lead stressed that stigma was proactively addressed by including a patient advisor from their inpatient psychiatry unit and a representative from their human rights and health equity department in their working group (C. Loftus personal communication, November 20, 2020).
We found that despite understanding the rationale behind flagging, workers and managers were concerned that flagging practices jeopardize patient rights to privacy. The hesitance may be rooted in a lack of understanding legislations. The Ontario Public Service Employees Union (OPSEU, n.d.) states that employers frequently cite the PHIPA as a reason not to comply with Bill 168 (2009), Section 32.0.5(3), which requires employers to provide workers with information about persons with an HOVB. However, the OHSA (1990) states that it prevails over other legislation (s 2(2), 1990) and the PHIPA states that it prevails unless another Act (like the OHSA) states otherwise (s 7(2), 2004).
In addition, some patients/families feel singled out when required to wear a specific wristband, fearing differential treatment. Similarly, NSHRF (2017) found that patient’s right to privacy, which they referred to as confidentiality, was a concern mentioned by key informants. Several solutions were provided by informants, including sharing only what is needed to take appropriate action, sharing information on a need-to-know basis, and ensuring patient confidentiality by allowing only certain roles access to patient records and audit this process. One informant discussed that the use of a specific color on wristbands does not breach confidentiality as several colors are used for a variety of alerts (e.g., allergies, risk of falling), and the significance of the colors is not widely known beyond staff. In our study, two hospitals had handouts for patients/families about patient/family violence and aggression and the hospital’s expectation of appropriate behavior. However, participants did not discuss whether these resources effectively increase patient awareness or whether they are regularly shared with patients who pose a risk of violence.
Similar to other studies (e.g., Burkoski et al., 2019; Paterson et al., 2019), we found several gaps in flagging policy and procedures. Some gaps were particularly frustrating that, according to one manager, led workers to not comply with the policy. In our study, a common practice to communicate with allied health workers was the use of visual alerts such as signage posted with instructions to speak with the patient’s nurse. On paper, this procedure is feasible. But implementing it often resulted in workers not being able to locate a clinician to provide instructions. We also found that in hospitals where management were the only persons authorized to initiate a flag resulted in significant lagged flag initiation, even days, when incidents occurred on weekends. Based on Paterson et al.’s (2019) finding that the health care team found it challenging when only the medical heads had authority to initiate flags, the authors recommended that other members of the health care team have authority to initiate flags. This process contributes to greater safety protection by sharing risk information in real time.
Our study has some limitations. We relied heavily on hospitals to recruit participants; therefore, participants’ views of their hospital’s flagging program may have been biased by the hospitals’ control over our access to participants. As a result, we may not have heard from all staff who were interested in participating in the study. For instance, at one site, we were not permitted to speak with any non-JHSC frontline workers. It also led to situations of managers and frontline workers attending the same FG where some individuals may have been reluctant to share their perspectives (rectified later by separating managers and frontline workers into different FGs). Also, hospital participation was voluntary. Likely, participating hospitals were more interested and invested in WVP than those that chose not to participate.
Implications for Occupational Health Practice
Hospital leadership has the opportunity to prevent violent incidents or mitigate serious injuries to workers during violent incidents by addressing the challenges related to flagging found in this study. Given stigma’s multi-level nature (Rao et al., 2019), it is not surprising that fears of patient stigmatization exist across workers and managers, patients/families, and health care organizations. To help dispel stigma, hospital leadership should commit to educating and training (with refreshers) managers and workers at all organizational levels on stigma, the purpose of flagging, and directly relevant legislations. In addition, leadership might collaborate with other organizations to reduce stigma by developing processes and tools (e.g., transfer of care forms with sections to indicate behavior history) to standardize and streamline communication related to patient violence. The Joint Centres in Toronto, for example, have partnered to share innovations to improve the quality of care, including joint WVP efforts (Andress et al., 2018).
Authoritative bodies such as Ontario’s Ministry of Labour, Training and Skills Development can contribute to eliminating the confusion over flagging and patient privacy by issuing a clear public statement about the relationship among legislations. The PSHSA (2017b) developed a fact sheet with a labor and employment law firm about communicating patient risk of violence without compromising obligations to protect patient privacy. More of these plain-language documents are needed with effective dissemination.
It is critically important that frontline clinical and allied health workers have an active role in flagging policy and procedure development to streamline the process and increase compliance (Paterson et al., 2019). Frontline workers are most knowledgeable about their unit/department’s nuanced activities that may be important to procedure feasibility. Involving frontline workers will help hospitals develop streamlined processes, including the important element of real-time information sharing. For instance, hospital leadership might engage nurses in developing flag initiation guidelines and corresponding safety measures that appropriately reflect level of risk or gradation. If leadership does not address frontline worker concerns, hospitals will continue to experience policy implementation challenges which have been found to contribute to additional worker-level stressors that can affect job performance, satisfaction, and cognitive strain (Baethge & Rigotti, 2013).
It is important to keep in mind that flagging is not a stand-alone activity but an important element of a comprehensive WVP program (e.g., Andress et al., 2018; Burkoski et al., 2019; Drummond et al., 1989; Hutton et al., 2018; Kling et al., 2011; Loftus et al., 2019; McPhaul & Lipscomb, 2004; Paterson et al., 2019; Wyatt et al., 2016). Moreover, flagging, along with other WVP interventions, is linked to the utmost goal which is to provide patients with appropriate care. Reaching this goal may be best met when worker safety is approached in tandem with patient safety. It is not misguided to consider the safety of workers first, as ultimately patient safety depends on worker safety. If workers are or feel unsafe, they cannot provide quality patient care (OPSEU, n.d.).
Conclusion
Flagging is one strategy used by hospitals to communicate to workers about patients with an HOVB. By addressing the challenges discussed in this article, hospital leadership will contribute to the safety of their workers, patients and their families, and others in the hospital environment. Flagging alone cannot keep workers safe. Rather, flagging practices are an essential element of a comprehensive WVP program in which leadership must be committed to.
Applying Research to Occupational Health Practice
Flagging patients with a history of violent behavior is one approach used by four hospitals in Ontario, Canada. By sharing violence-related information with workers, workers are able to keep themselves and others safe by being more vigilant and implementing safety protocols and behavior care plans. Despite the overall sentiment among frontline worker and management participants, three main issues challenge the effectiveness of a flagging program: patient stigmatization, patient privacy in relation to worker safety, and gaps in policy and procedures. Hospital leadership and occupational health and safety staff should focus on repeated education and training for workers and managers at all organizational levels on the purpose of flagging, stigma, and the relationship among the occupational health and safety and privacy legislations. Involving frontline clinical and allied health workers will help to develop directly relevant and feasible practices which may contribute to workers’ compliance and ultimately their safety.
Footnotes
Acknowledgements
We thank our advisory committee for their help with hospital recruitment. Thank you to the participants in the study.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided by the Ontario Ministry of Labour, now called the Ontario Ministry of Labour, Training and Skills Development.
Author Biographies
Era Mae Ferron, PhD, RN, has a PhD in nursing from the Lawrence S. Bloomberg Faculty of Nursing at the University of Toronto and worked at the Institute for Work & Health as a research associate.
Agnieszka Kosny, PhD, has a doctorate in public health from the University of Toronto and worked at the Institute for Work & Health as a scientist.
Sabrina Tonima, MHE, has a master’s degree in health evaluation from the University of Waterloo. At present, she is a Knowledge Transfer & Exchange Associate at the Institute for Work & Health.