
Abstract
Background:
Violent workplace deaths among health care workers (HCWs) remain understudied in the extant literature despite the potential for serious long-term implications for staff and patient safety. This descriptive study summarized the number and types of HCWs who experienced violent deaths while at work, including the location in which the fatal injury occurred.
Methods:
Cases were identified from the Centers for Disease Control and Prevention’s National Violent Death Reporting System between 2003 and 2016. Coded variables included type of HCW injured, type of facility, and location within the facility and perpetrator type among homicides. Frequencies were calculated using Excel.
Findings:
Among 61 HCW deaths, 32 (52%) were suicides and 21 (34%) were homicides; eight (13%) were of undetermined intent. The occupations of victims included physicians (28%), followed by nurses (21%), administration/support operations (21%), security and support services (16%), and therapists and technicians (13%). Most deaths occurred in hospitals (46%) and nonresidential treatment services (20%). Within facility, locations included offices/clinics (20%) and wards/units (18%). Among homicide perpetrators, both Type II (perpetrator was client/patient/family member) and Type IV (personal relationship to perpetrator) were equally common (33%).
Conclusion/ Applications to Practice:
Suicide was more common than homicide among HCW fatal injuries. Workplace violence prevention programs may want to consider both types of injuries. Although fatal HCW injuries are rare, planning for all types of violent deaths could help minimize consequences for staff, patients, and visitors.
Keywords
Background
Health care settings are seen as places of healing and safe refuge in communities, yet they face a rising and disproportionate share of workplace violence incidents (Occupational Safety and Health Administration [OSHA], 2015). The OSHA guidelines for preventing workplace violence for health care and social service workers defines workplace violence as “any act or threat of physical violence, harassment, intimidation, or other threatening disruptive behavior that occurs at the work site” (OSHA, 2016). Workplace violence can manifest in numerous forms including verbal abuse, physical threats, physical assaults, and homicide (Pompeii et al., 2013). It can affect and involve employees, clients, customers, and visitors (OSHA, 2016).
There is growing recognition that workers who feel unsafe in their work environment are less able to provide safe patient care (The Joint Commission, 2018; Perlo et al., 2017). Exposure to violence can cause stress, distraction, and greater possibility of errors in decision-making among health care workers (HCWs; National Quality Forum, 2020; Udoji et al., 2019).
Most violence related HCW injuries come from physical assaults perpetrated by patients and visitors (Phillips, 2016; Pompeii et al., 2013). Moreover, data from the Bureau of Labor Statistics (BLS) indicate that workplace violence (including violence by persons, animals, and self-inflicted injuries) is the leading cause of fatal occupational injury among hospital workers (BLS, 2019).
Violent deaths, including homicides, suicides, and deaths due to law enforcement intervention (e.g., security officer shootings), are the most dramatic examples of workplace violence. Any violent death, especially those in public areas such as emergency departments, may cause lasting trauma for many, including colleagues, patients, and visitors who observe and respond to the incident as well as those who have to deal with the aftermath and remediate the environment (Sabbath et al., 2018).
The need for additional research on the epidemiology and strategies to prevent health care workplace violence has been well documented (Arnetz et al., 2015; Bromley & Painter, 2019; Phillips, 2016). While researchers have focused on specific disciplines such as physicians or nurses (Davidson et al., 2018; Udoji et al., 2019), only a few studies have included all types of HCWs within the organization (Hoffman, 2019; Pompeii et al., 2015).
No studies, to our knowledge, have specifically examined workplace-related violent deaths among HCWs. The purpose of this study was to describe the number and types of HCWs experiencing violent deaths in their workplaces and the location within the facility in which the fatal injury occurred using the national reporting system developed and managed by the Centers for Disease Control and Prevention (CDC).
Methods
The data source for this study was a CDC-restricted access data set known as the National Violent Death Reporting System (NVDRS; CDC, 2019). The NVDRS, which began in 2003, is a population-based, active surveillance system designed to obtain a complete census of violent deaths within a participating state. Each participating state collects information on its own deaths from death certificates, medical examiner/coroner files, and law enforcement records and submits information through their health departments (or their bona fide agents). Reported cases comprise violent deaths from suicide, homicide, and law enforcement intervention (e.g., individual is killed by law enforcement acting in the line of duty).
Our data set included all available incidents from states reporting during the time frame 2003 to 2016; however, states were not required to submit data to the NVDRS and the number of states reporting varied over time, with a range of seven to 32 states reporting over this time period. Two variables were used to identify cases: (a) the location of injury was a hospital or medical facility and (b) the injury occurred to the victim while at work. We initially included only cases for which injured at work was coded as “yes.” However, after review of the narrative for cases in which the field “injured at work” was blank, missing, or Unable to Determine (UTD), we identified additional cases by reviewing occupation text fields. This allowed us to include retired HCWs, and those fatally injured in a health care organization who may not have been on duty at the time. A complete list of variables used in this project is provided in Supplemental Table 1.
For this study, we created four new variables: (a) type of HCW, (b) type of health care facility in which injury occurred, (c) location of injury within the health care facility, and (d) perpetrator type among homicides. Categories for these four variables were derived in part from the BLS Standard Occupational Classification System (BLS, 2019), OSHA Guidelines (2016), and Howard (1996). All codes were assigned by consensus during team meetings to promote consistency and accuracy. Use of this public health–related data set on decedents is not considered human subjects research; therefore, human subjects approval was waived.
Data Analysis
Microsoft Excel™ was used for filtering data and calculating frequencies and correlation coefficients. Due to initial concerns about low numbers of included cases, we sought cases that may have been incorrectly classified (false negatives) on the two key variables. To look for cases that might have been missed, we created a separate data set (n = 6,121) in which the two variables were coded as not applicable, unknown, or blank and we reviewed every 100th row. During this process, no additional eligible cases were found. Also, in accordance with NVDRS data sharing agreement requirements for protecting anonymity, findings were grouped and nonzero frequencies of less than five cases were suppressed (CDC, 2017).
Results
Overall, our data set comprised 270,886 unique incidents reported to NVDRS, with 278,183 deaths and 6,101 incidents with more than one victim. Across all industries, the number of incidents in which the victim was injured at work was 3,477 (1.3%), with 3,576 (1.3%) deaths (data not shown). Separately, the total number of incidents in which the location of injury was a hospital or medical facility (regardless of worker status) was 1,207 (0.5%), with 1,234 deaths (0.4%). When filtering for cases in which the HCW was injured at work and the location of injury was a hospital or medical facility, 61 HCW deaths were identified.
The number of states submitting data steadily increased from seven in 2003 to 32 in 2016 (Table 1). Between the years 2003 and 2015, the number of reported cases of HCW deaths injured at work per year was only moderately correlated with the number of states submitting data (Pearson r = .48, p = .10) suggesting that the increase in the number of cases is not directly proportional to the increase in the number of states submitting data. Among reporting states, 12 (38%) did not report any HCW deaths within health care facilities. The most HCW deaths from any single state across the time period was 9. When adjusted for the number of states enrolled, the mean number of deaths reported per year was 0.24 (SD = 0.10 and median = 0.25).
National Violent Death Reporting System State Participation and Reported Number of Deaths Among HCW Who Were Injured at Work
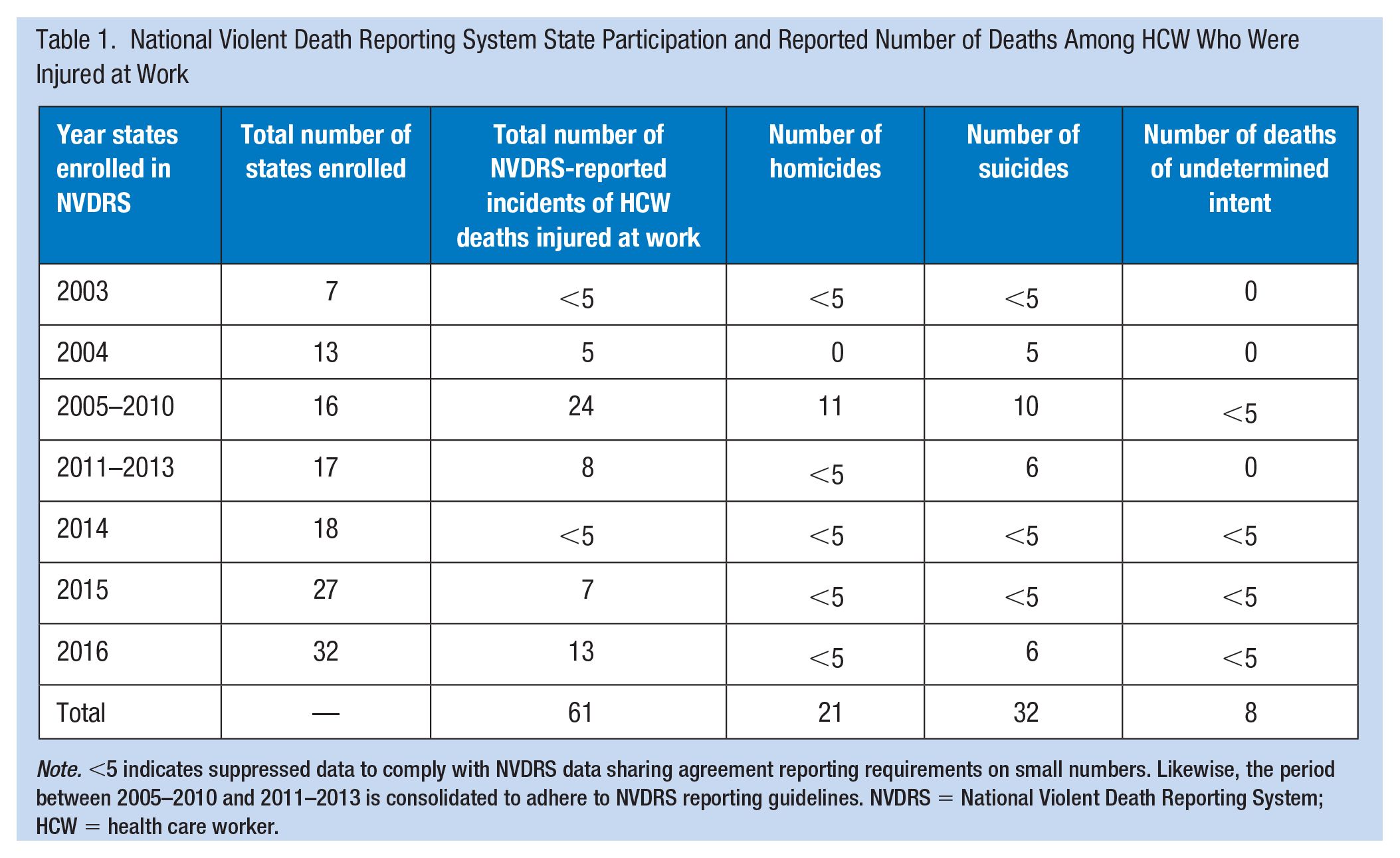
Note. <5 indicates suppressed data to comply with NVDRS data sharing agreement reporting requirements on small numbers. Likewise, the period between 2005–2010 and 2011–2013 is consolidated to adhere to NVDRS reporting guidelines. NVDRS = National Violent Death Reporting System; HCW = health care worker.
Among the 61 HCW deaths, 32 (52%) were suicides and 21 (34%) were homicides; eight (13%) were of undetermined intent and none were law enforcement related. The occupations of victims were frequently physicians (n = 17; 28%), nurses (n = 13; 21%), administration and support operations and other categories (n = 13; 21%), security and environmental services staff (n = 10; 16%), and therapists and technicians (n = 8; 13%; Table 2). Compared with other HCWs, physicians died more frequently from suicide than homicide.
Occupation of Health Care Worker That Experienced a Violent Death as Reported to the NVDRS: 2003 to 2016
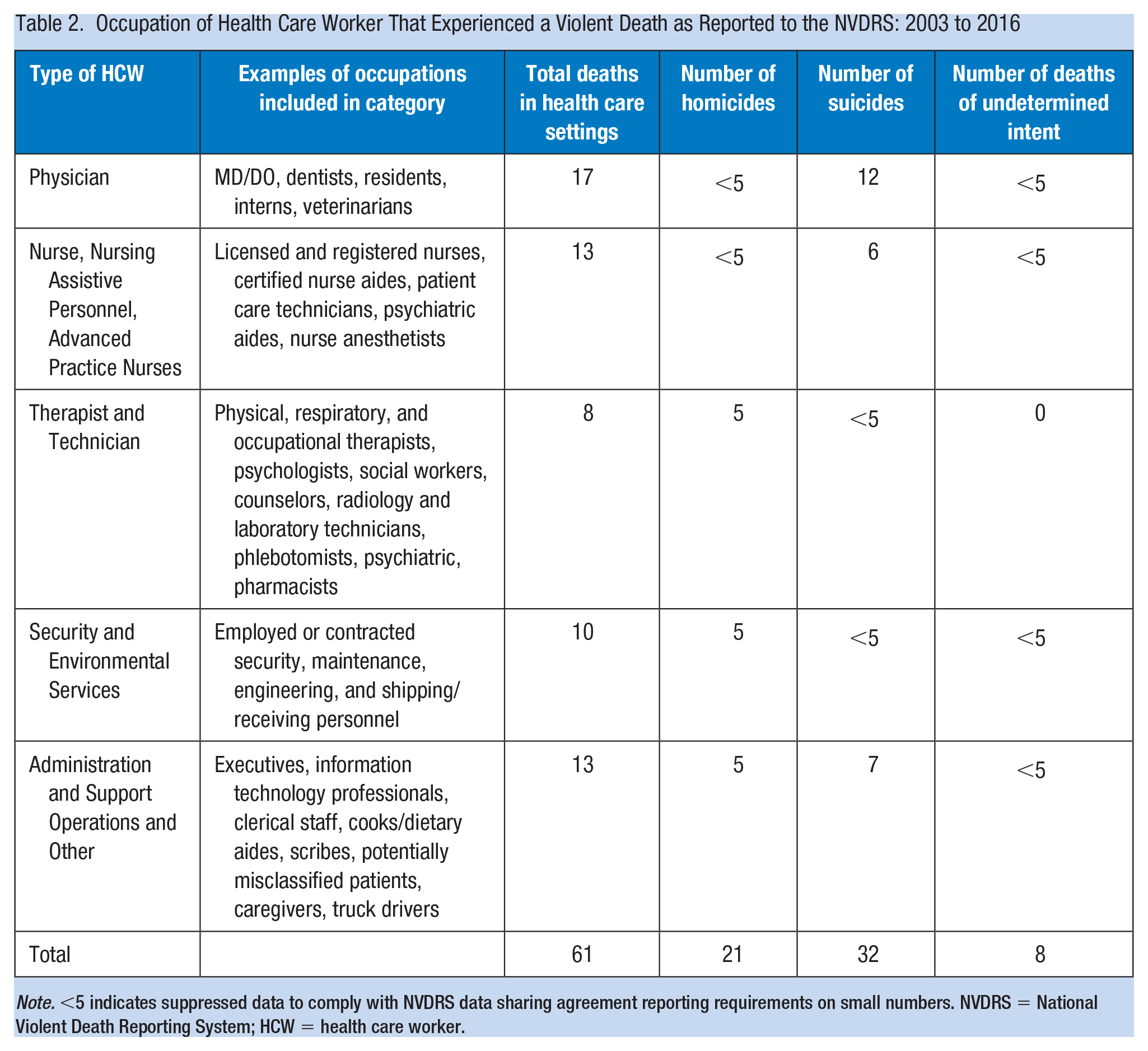
Note. <5 indicates suppressed data to comply with NVDRS data sharing agreement reporting requirements on small numbers. NVDRS = National Violent Death Reporting System; HCW = health care worker.
The most frequent health care setting where the fatal injury occurred was hospitals (n = 28; 46%), followed by nonresidential treatment services such as clinics (n = 12; 20%), unable to determine (n = 9; 15%), and residential treatment (n = 7; 11%) (Table 3). Within the health care facility, frequently occurring locations were offices or clinics (n = 12; 20%), wards or units (n = 11; 18%), other/unable to determine (n = 11; 18%), restrooms (n = 8; 13%), outside or garage (n = 7; 11%), and common areas (n = 6; 10%). There were no reported cases in the settings of field work (e.g., home health care) or emergency departments. Furthermore, within settings, there were more homicides than suicides in hospitals and more suicides than homicides in nonresidential treatment.
Location of Injury and Comparison of Type of Violent Death Among Health care Workers Within the Health Care Setting: Data From the NVDRS (2003–2016)
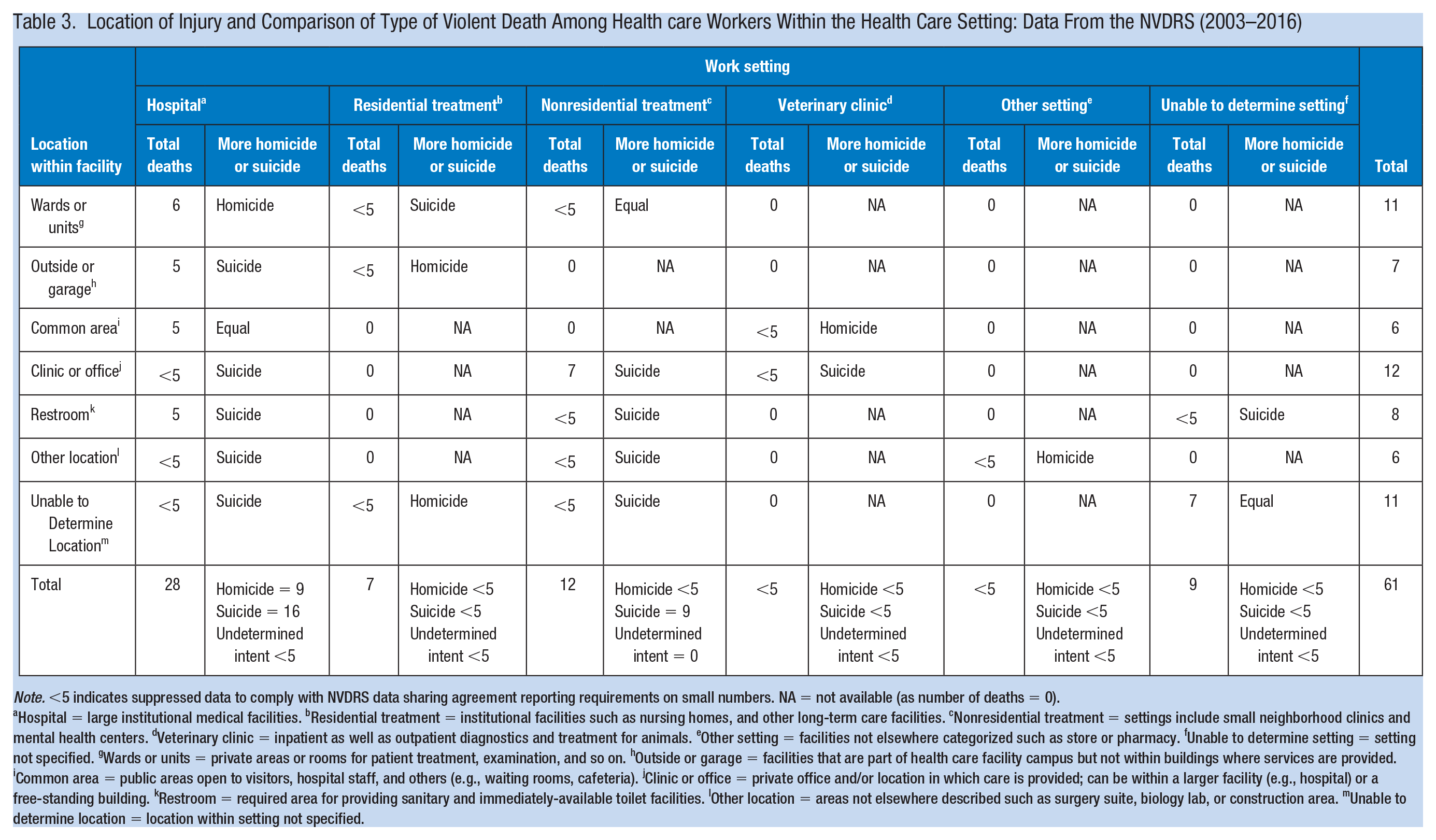
Note. <5 indicates suppressed data to comply with NVDRS data sharing agreement reporting requirements on small numbers. NA = not available (as number of deaths = 0).
Hospital = large institutional medical facilities. bResidential treatment = institutional facilities such as nursing homes, and other long-term care facilities. cNonresidential treatment = settings include small neighborhood clinics and mental health centers. dVeterinary clinic = inpatient as well as outpatient diagnostics and treatment for animals. eOther setting = facilities not elsewhere categorized such as store or pharmacy. fUnable to determine setting = setting not specified. gWards or units = private areas or rooms for patient treatment, examination, and so on. hOutside or garage = facilities that are part of health care facility campus but not within buildings where services are provided. iCommon area = public areas open to visitors, hospital staff, and others (e.g., waiting rooms, cafeteria). jClinic or office = private office and/or location in which care is provided; can be within a larger facility (e.g., hospital) or a free-standing building. kRestroom = required area for providing sanitary and immediately-available toilet facilities. lOther location = areas not elsewhere described such as surgery suite, biology lab, or construction area. mUnable to determine location = location within setting not specified.
Among the 21 homicides, the most frequent types of perpetrators, as classified by Howard (1996), were Type II (perpetrator is a client or patient, family member, or visitor at the workplace) and Type IV (perpetrator has a personal relationship to employee outside of workplace) with (n = 7; 33%) for each, followed by unable to determine (n = 4; 19%). Two perpetrators (9%) were Type III (perpetrator is a current or former employee of the workplace), and one (4%) was Type I (criminal intent; perpetrator has no legitimate relationship to the business or its employees).
Discussion
This descriptive analysis sought to characterize the number and types of HCWs experiencing violent deaths in their workplaces and the location within which the fatal injury occurred among deaths reported to the NVDRS.
In contrast to sensational news accounts, the number of HCWs fatally injured at work by homicide was smaller than anticipated. While this could be interpreted as good news, it is important to consider the data source. The relatively small number of cases in our data set may be attributed to the fact that most states were not submitting data to NVDRS at the time. For example, in 2014, although the NVDRS had been operational for 11 years, only 18 states were submitting data in that year. Nevertheless, an important strength of using this data set is its standardized coding definitions and detailed narratives (Nazarov et al., 2019). NVDRS has been used to study suicides among physicians, veterinarians, and hospital inpatients (Gold et al., 2013; Williams et al., 2018; Witte et al., 2019). Recent efforts to support enrollment and data submission for all states will overcome this limitation in the years ahead (Krisberg, 2018).
The finding of more suicides than homicides is consistent with NVDRS data that indicate that in 2017 more than 47,000 people died by suicide, whereas 19,500 people were victims of homicide (CDC, 2019). Similarly, that physicians and dentists had more violent deaths than other health care occupations has been previously identified (Gold et al., 2013; Ji et al., 2020; Kalmoe et al., 2019; McGill University Office for Science and Society, 2021). Previous studies that examined perpetrators across all types of workplace violence (including assaults) have found Type II (patients and customers) to overwhelmingly be the most frequent (Phillips, 2016; Pompeii et al., 2013). However, among fatal workplace injuries (homicides only), we found there were equal proportions of perpetrators who were customers (Type II) and perpetrators with a personal relationship (Type IV), a key contribution of this study given the paucity of extant literature on Type IV violence in health care.
This preliminary study has several limitations. Conclusions should not be generalized to U.S. HCWs or facility types as we did not have the sample to estimate incidence rates or adjust for confounding factors, nor did we consider comparison with any international reporting systems. Besides the number of states enrolled, another possible reason for the small number of cases is underreporting. For example, according to 2016 Census of Fatal Occupational Injuries (CFOI) BLS data, there were 24 violence-related fatal occupational injuries among HCWs (10 among health diagnosing and treating professionals including physicians and nurses, seven among health technologists and technicians, and seven among nursing, psychiatric, and home health aides; BLS, 2019). Compared with this national estimate, we found 16 deaths reported in 2016 from 32 states, which suggests that our numbers may be only slightly undercounted. It is also possible that cases were missed due to the search strategy and one or more cases identified as HCWs actually had a non-health care occupation (e.g., truck driver).
This study identified several gaps in need of future research. As mentioned in the results section, the large difference between the 1,200 or more reported violent deaths in health care settings and the number of HCW deaths suggests that many deaths may have occurred among patients and/or visitors, although these groups are not easily identified from NVDRS. Future research should examine the characteristics and reasons for all homicides and suicides in health care settings to develop effective prevention strategies. Also, research is needed on the accuracy and completeness of NVDRS data in comparison with other sources such as BLS CFOI data. Furthermore, this analysis should be redone after all states were enrolled in the data submission system to get a more comprehensive and current estimate of fatal workplace violence events in health care settings.
Using NVDRS data, this descriptive study summarized the number and types of HCWs experiencing violent deaths in their workplaces and the location within which the death occurred. Our analysis found that the number of suicides that occurred within health care facilities exceeded the number of homicides among HCWs. Workplace violence prevention programs may want to consider both types of injuries. Although rare, planning for all types of violent deaths should help minimize consequences for staff, patients, and visitors. Prevention of all violent deaths will improve the safety and well-being of HCWs, patients, and visitors within the health care setting.
Implications for Occupational Health Practice
The practical implications for health care workplace violence prevention programs include the recognition that violent deaths from suicide can, and perhaps should, be considered a form of workplace violence, although suicide is rarely addressed in guidance for workplace violence prevention programs and instead is usually considered in relation to employee assistance programs. Although specific strategies for prevention of suicide and homicide will vary, health care organizations should recognize and prepare for the impact of both on staff and patients.
As mentioned previously, most workplace violence events in health care are not fatal; thus, these data reflect the worst-case scenario. Although in this study fatal events were not frequent, health care organizations may also want to plan for violent deaths and related events that can occur in public areas such as hospital lobbies or emergency department waiting rooms. Adequate preparation, including consideration of security, communication, and support services for observers and secondary victims, helps to ensure a timely and appropriate response and minimize long-term sequelae (NQF, 2020; OSHA 2016).
Application of Research
This study addresses a gap in the literature on violent workplace deaths among health care workers (HCWs). Workplace violence in health care settings is an occupational hazard that has serious implications for employee health and safety and the delivery of quality health care. Although assaults from patients are the most frequently reported injury, little is known about violent workplace deaths in health care settings. Using data from the Centers for Disease Control and Prevention’s (CDC) National Violent Death Reporting System, this study summarizes the number and types of HCWs experiencing violent deaths in their workplaces and the location within which the death occurred. Our findings reveal that suicide was more common than homicide, pointing to a need to consider workplace violence prevention policies and interventions that address the risk of both homicide and suicide among HCWs. Prevention of all violent deaths will improve the safety and well-being of HCWs, patients, and visitors within the health care setting.
Supplemental Material
sj-pdf-1-whs-10.1177_21650799211003824 – Supplemental material for Health Care Worker Violent Deaths in the Workplace: A Summary of Cases From the National Violent Death Reporting System
Supplemental material, sj-pdf-1-whs-10.1177_21650799211003824 for Health Care Worker Violent Deaths in the Workplace: A Summary of Cases From the National Violent Death Reporting System by Barbara I. Braun, Hasina Hafiz, Shweta Singh and Mushira M. Khan in Workplace Health & Safety
Footnotes
Acknowledgements
The authors thank Tasha Mearday for editorial assistance and Scott Williams, PsyD, for the thoughtful review.
Disclaimer
The National Violent Death Reporting System (NVDRS) is administered by the Centers for Disease Control and Prevention (CDC) by participating NVDRS states. The findings and conclusions of this study are those of the authors alone and do not necessarily represent the official position of the CDC or of participating NVDRS states.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
Barbara I. Braun is associate director, Health Services Research in the Division of Healthcare Quality Evaluation at The Joint Commission.
Hasina Hafiz is a research associate in the Department of Research at The Joint Commission.
Shweta Singh is a clinical data analyst in the Department of Quality Measurement at The Joint Commission.
Mushira M. Khan is a research associate in the Department of Research, Division of Healthcare and Quality Evaluation at The Joint Commission.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.