
Abstract
Background
Mental health professionals caring for the veteran population are at increased risk for compassion fatigue, burnout, and secondary traumatic stress based on the nature of their work. While mental health professionals may experience positive outcomes from providing compassionate care to veterans, compassion fatigue can lead to instability of the workforce.
Methods
A pilot employee wellness program was implemented over a 9-week period, offering a different wellness module weekly during the employee lunch hour. Demographic data were collected pre-program, and mental health employees were surveyed pre- and post-program using an intent to stay scale and the Professional Quality of Life Scale version 5 (ProQOL-5) to measure compassion satisfaction, burn out, and secondary traumatic stress.
Findings
Pre-program participants (N = 42) reported significant differences in intent to stay in their current position for the next year compared to the post-program group (N = 15). Pre-program participants reported no intent to leave their current position, apply for internal or external positions, or retire in the following year. However, post-program participants reported intent to leave their current positions, apply to internal or external positions, or retire. Pre- and post-program compassion satisfaction scores increased and burnout and secondary traumatic stress scores decreased; these scores were not significantly different between groups.
Conclusions/Application to Practice
While no significant differences were found between ProQOL-5 subscale scores, the change in participants’ scores may indicate some change, potentially as a result of the intervention. This pilot program offered a creative solution to organizations with limited resources to combat occupation-related compassion fatigue.
Background
Following conflicts in the Middle East, there have been increased veteran enrollment in the U.S. Department of Veterans Affairs (VA; Newell & MacNeil, 2011), with a subsequent increased utilization of mental health care provided by VA employees. Post-traumatic stress disorder (PTSD) is a mental health condition triggered by a terrifying event, either experiencing or witnessing it, and PTSD affects between 11% and 20% of the 1.8 million U.S. military veterans who have served since 2001 (VA, 2014).
Mental health care professionals working with the veteran population are at increased risk for compassion fatigue, burnout, and secondary traumatic stress (Cetrano et al., 2017). Compassion fatigue is defined as the negative emotional and psychological effects resulting from experiencing the distress or suffering of others (Figley, 1995; Stamm, 1997). Burnout, a component of compassion fatigue, is defined as emotional exhaustion, depersonalization, and reduced personal accomplishment (Baum, 2016; Newell & MacNeil, 2011). Although Figley (1995) stated secondary traumatic stress is also a component of compassion fatigue, it is linked specifically to symptoms of re-experiencing, intrusive thoughts, and avoidance after exposure to others’ traumatic experiences (Shoji et al., 2015). One positive outcome resulting from working with those who have experienced trauma is compassion satisfaction, which is defined as the positive emotional and psychological effects a person derives from helping others (Sacco et al., 2015; Stamm, 2010). Compassion satisfaction is marked by pleasure and purpose that results from working in a helping profession.
When looking at factors affecting employee’s professional quality of life (ProQOL), both the positive and negative aspects warrant consideration (Stamm, 2010). The Compassion Satisfaction-Compassion Fatigue Model explores how positive aspects of work contribute to compassion satisfaction and compassion fatigue. In this model, three environments contribute to symptoms of compassion satisfaction and compassion fatigue: the work environment, the client/person helped environment, and the personal environment. Stamm (2010) suggests that negative feelings can be overcome by positive feelings and vice versa; healthcare workers can exhibit symptoms of compassion fatigue and concurrently experience compassion satisfaction as a result of helping others (Stamm, 2010).
While studies including nurses and social workers make up the main body of ProQOL research, all professionals have been found to be at risk. Acker (2011) found that out of 460 mental health care providers, 56% reported high levels of emotional exhaustion, a component of burnout, and 50% considered quitting their job. Furthermore, workers in government-funded jobs had higher levels of emotional exhaustion than non-government employees (Acker, 2011). Shoji et al. (2015) found that high burnout was a predictor of secondary traumatic stress in U.S. military mental health care professionals. Finally, higher emotional exhaustion scores have been found in female VA clinicians and administrators relative to their male counterparts (Newell & MacNeil, 2011). Newell and MacNeil (2011) attributed these findings to patients’ expectations for female staff to provide emotional support, which could increase the risk of emotional exhaustion.
Radley and Figley (2007) theorized that when energy from compassion fatigue is handled differently, it can impact compassion satisfaction in a positive way. To increase self-care behaviors, Flarity et al. (2013) and Weidlich and Ugarriza (2015) used employee education programs to prevent and treat compassion fatigue with demonstrated positive outcomes. Expressive writing, guided imagery, yoga, mindfulness, and music therapy have been shown to reduce compassion fatigue and to increase or sustain compassion satisfaction (Gregory, 2015; Henry, 2014; Hilliard, 2006; Kiley et al., 2018).
Compassion fatigue can contribute to instability of the healthcare workforce, ultimately leading to staff turnover (Kim et al., 1996). Staff turnover results not only in loss of revenue but also poor continuity of patient care (Brandt et al., 2016; University of New Mexico, 2016). The cost to replace registered nurses and social workers is between US$52,000 and US$85,000 per worker, while the cost to replace a psychiatrist is closer to US$500,000 (American Federation of State, County & Municipal Employees, 2019; Barrett & Greene, 2016; Cagliostro, 2020; HealtheCareers, 2012). Often, when organizations experience high turnover, positions are left unfilled. Specifically, the VA reported 40,456 vacancies out of 375,953 full-time positions in 2018 (Office of Public and Intergovernmental Affairs, 2018). A lack of qualified employees, non-competitive salaries, and high staff turnover were found to be reasons for vacancies in VA facilities, according to the VA Office of Investigator General (OIG; U.S. Department of Veterans Affairs, 2018). The OIG defines a staffing shortage as having positions that are difficult to fill with a severe shortage of candidates; however, nursing was not included in the published results (U.S. Department of Veterans Affairs, 2018). Contrary to the OIG results, Salyers et al. (2013) compared compassion fatigue in VA staff to staff in other healthcare systems and reported institutional resources, including better pay and job security, contributed to lower levels of compassion fatigue in VA staff. Garcia et al. (2014) studied VA mental health clinicians providing evidence-based PTSD care; almost half reported feeling exhausted and cynical in their work. It was suggested that mental health employees may experience higher levels of burnout when they have less control over their work. Moreover, 32% of the employees reported that they were “somewhat likely” or “likely” to leave their current position (Garcia et al., 2014). Currently, there are gaps in the literature relating to how VA organizational factors influence compassion fatigue.
There were two questions this pilot program sought to answer: (a) Were employees in mental health services and community-based mental health programs experiencing compassion fatigue? and (b) Would an employee wellness program have an effect on compassion fatigue, compassion satisfaction, and intent to stay? The aim of this pilot program was to determine what effect a voluntary employee wellness pilot program would have on occupation-related compassion fatigue and compassion satisfaction levels in mental health services and community-based mental health program employees at three VA locations in New York State.
Methods
In November 2019 through February 2020, we conducted a wellness pilot program at three VA locations in New York State. An interdisciplinary sample of healthcare workers was drawn from the VA mental health clinic and mental health community care departments at these locations. The wellness program included weekly seminars that workers were welcome to participate in. We obtained measures from workers before and after the intervention period for purposes of examining the effect of wellness activities on compassion fatigue, compassion satisfaction, and intent to stay in their current position.
The inclusion criterion for this pilot program was employment in the mental health clinic or mental health community care departments in three VA locations in New York. Staff included medical support assistants, social services assistants, licensed practical nurses, registered nurses, social workers, psychologists, nurse practitioners, psychiatrists, licensed mental health counselors, addiction therapists, peer support specialist, and vocational therapists. Employees were recruited for this pilot program through email via the employee listserv. All of these employees at the three locations were invited to participate in the employee wellness program and were asked to complete a survey via an emailed link. When participants clicked on the survey link, they first reviewed the consent form and, if they were interested, selected “agree” to proceed with the survey.
The employee wellness program was implemented over a 9-week period with one 30- to 45-minute module offered each week. Sessions were offered via televideo for employees who were unable to attend in person, with the exception of yoga. Employees, who were experts in each content area, were approached and voluntarily agreed to lead the modules. The modules included nutrition, sleep hygiene, therapeutic use of music, mindfulness, guided imagery, therapeutic journaling, yoga, Tai Chi, and basic movement. Weekly emails were sent to employees describing the module being offered with an employee Wellness Toolkit. The Wellness Toolkit was a list of phone/computer applications that employees could access for self-initiated wellness activities related to the modules. Formal attendance was not taken for the modules; instead, the number of attendees for each module was recorded.
Data Collection
All surveys were completed online using Qualtrics and an electronic description of the program accompanied the survey. Participants were instructed to click on “I agree” to consent and move forward with the survey. No identifiable information was collected during the course of this project.
A pre-program survey was administered prior to launching the pilot program that included demographic questions and questions related to wellness and their intent to stay. Information regarding intent to stay in the current position, internal or external change of position, and retirement within the next year was collected using a 5-point Likert-type scale (1 = strongly disagree to 5 = strongly agree). Compassion fatigue and compassion satisfaction data were collected using the ProQOL scale version 5 (ProQOL 5). This was a 30-item tool with three subscales (compassion satisfaction, burnout, and secondary traumatic stress) with demonstrated construct validity (Stamm, 2010). Reliability had been established for the ProQOL-5 subscales, with the published Cronbach’s alpha noted to be .88 for compassion satisfaction, .75 for burnout, and .81 for secondary traumatic stress (Stamm, 2010). For each of these variables, scores of 22 or less indicated low levels, scores 23 to 41 indicated average levels, and scores 42 and higher indicated high levels (Stamm, 2010).
The post-program survey included the intent to stay questions, the ProQOL 5, and questions regarding program attendance and program evaluation. After conclusion of the pilot program, the post-program survey was sent via email to all eligible employees, regardless of participation in the modules. The survey was open for 2 weeks with two additional reminder emails distributed prior to the closing date.
All participation was voluntary and anonymous. Institutional Review Boards of the Syracuse VA Medical Center and St. John Fisher College approved this project.
Data Analysis
Data were analyzed using SPSS 26. Descriptive statistics were performed for demographic variables, pre-program wellness information, attendance, post-program wellness information, and ProQOL 5 data. Inferential analysis included a comparison of mean intent to stay and ProQOL 5 scores pre-program and post-program using independent-samples t tests.
Findings
For the pre-program survey, 54 participants accessed the survey and provided consent; 12 were dropped from the analysis due to missing data. Post-program, 21 accessed the survey and provided consent, and seven were dropped from the analysis due to missing data. The final sample included 42 participants pre-program and 15 participants post-program (n = 57) (Table 1). Participants were more likely to be female (64%), have a master’s or doctoral degree (69%), to have been employed with the organization for 10 to 15 years (36%), and to have taken 2 or more sick days in the previous 2 months (38%). Pre-program, 31% of employees reported not participating in any wellness activities, though 38% reported exercising for 1 to 4 hours a week. Post-program, 47% of participants reported attending one wellness module; 40% of modules were attended via televideo. When asked to evaluate the pilot program, participants reported the module content was the aspect they enjoyed the most (53%) and reported that the time constraints of the program were what they disliked the most (40%). Less than half of the participants (40%) accessed the Wellness Toolkit, with MyFitnessPal™ (22%) being the most frequently used. Participants reported they would like to see yoga (64%) and mindfulness (64%) offered again. Participants reported an interest in relaxation, art therapy, massage, active movement-cardio, and financial planning in the future. Mean scores were calculated for the intent to stay questions for both the pre- and post-program groups (Table 1). The pre-program participants reported they intended to stay in their current position in the next year (M = 1.7), disagreed that they would be applying for internal positions (M = 3.5), and strongly disagreed that they planned to leave the VA (M = 4.4) or retire (M = 4.6). Post-program participants reported they did not intend to stay in their current positions (M = 4.5), agreed that they planned to apply for internal positions (M = 2.4), planned to leave the VA (M = 1.5), or planned to retire (M = 1.2) in the following year.
Pre- and Post-Intervention Intent to Stay and ProQOL-5 Data
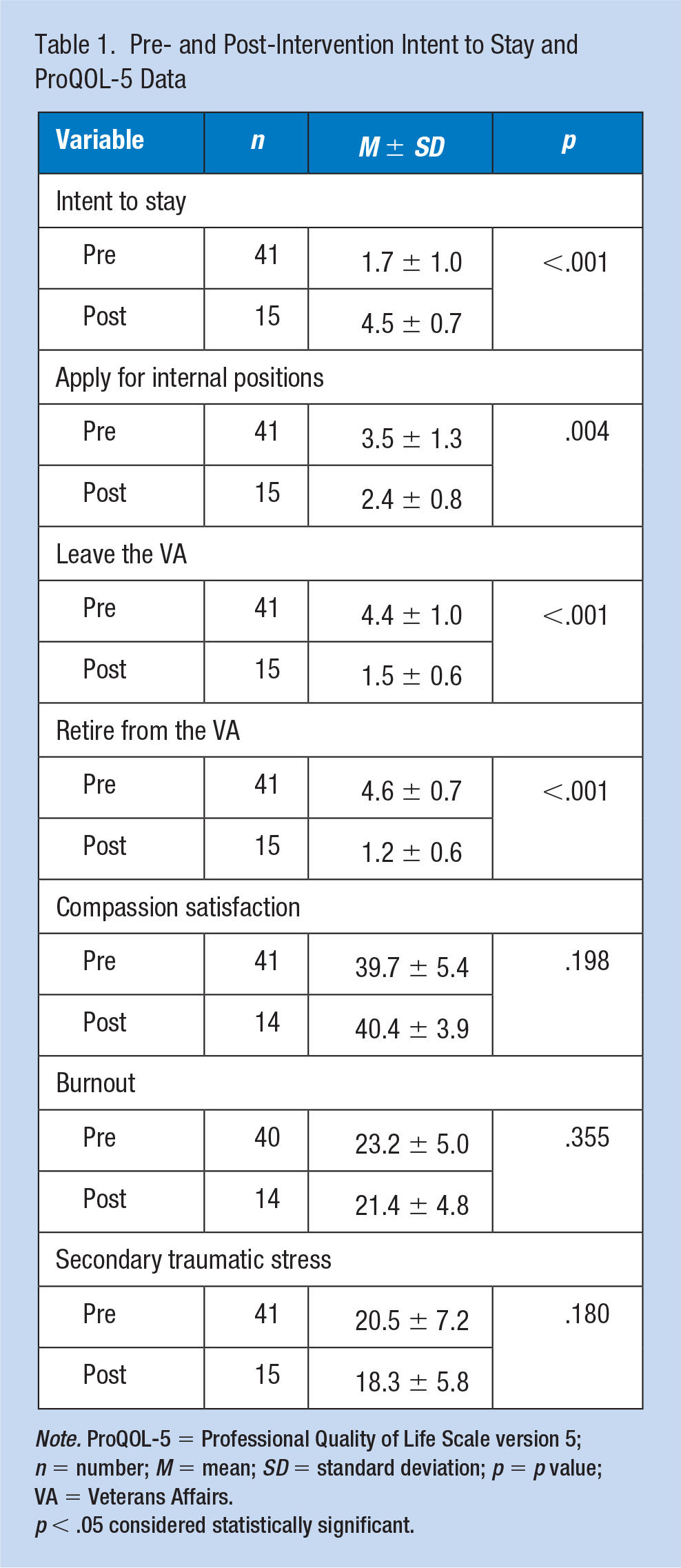
Note. ProQOL-5 = Professional Quality of Life Scale version 5; n = number; M = mean; SD = standard deviation; p = p value; VA = Veterans Affairs.
p < .05 considered statistically significant.
Participants pre-program and post-program had similar scores for compassion satisfaction, burnout, and secondary traumatic stress (Table 1). Both pre- and post-intervention, participants reported average compassion satisfaction scores (M = 39.7 and M = 40.4, respectively). Participants had average pre-program burnout scores (M = 23.2) and low post-program scores (M = 21.4), indicating participants post-program reported less burnout. Similarly, participants pre- and post-program reported low secondary traumatic stress subscale scores (M = 20.6 and M = 18.3, respectively).
Discussion
The main purpose of this project was to determine the effects an employee wellness program had on compassion fatigue and compassion satisfaction for mental health service employees. Unfortunately, it was impossible to match participants pre- and post-intervention, and the risk of committing a type I error was high due to unequal pre- and post-program sample sizes (Rusticus & Lovato, 2014). Therefore, the data needed to be interpreted with caution. The difference in mean ProQOL 5 scores between groups did not reach statistical significance. However, the participants’ mean compassion satisfaction scores increased and mean burnout and secondary traumatic stress scores decreased, indicating some change, potentially as a result of this program.
Pre-program, participants indicted they did not intend to leave their current positions, apply for internal positions, leave the VA, or retire in the following year. Interestingly, post-program participants intended to leave their current position, but they agreed/strongly agreed with either a position change within the VA, outside of the VA, or to retire. It was difficult to explain the intent to stay results; however, these findings may be a result of self-selection and differences in sample size pre- and post-program.
This pilot program did not examine differences in ProQOL 5 scores based on demographic factors, due to a small sample size and the risk of identifying participants based on the data. Furthermore, differences in occupational expectations may have played a role in participants’ perception of compassion satisfaction, burnout, secondary traumatic stress, and intent to stay (Yanchus et al., 2016) and should be investigated in future work.
This pilot project had several limitations. First, there were technologic issues that resulted in an inability for some employees to engage in the Basic Body Movement, Tai Chi, and Therapeutic use of Music modules; this had a direct impact on the number of module participants and potentially decreased the post-program sample size. Second, one of the locations experienced substantial turnover prior to and during program implementation. This potentially played a role in the number of employees who attended modules and participated in the post-survey. Third, prior to project implementation, the three VA sites involved started a separate VA-run employee wellness program that was launched concurrently with this program. The program offered similar services in the evenings after clinic hours. It was possible that employees chose to participate in this program, the VA-run program, or both, which may have confounded results. As the VA-run program was launched after this pilot project was approved, it was impossible to examine the effects of both programs.
Conclusion
Creativity was necessary in organizations with limited resources for employee wellness. Utilizing employees trained in various wellness interventions to provide modules was a cost-effective way to implement a wellness program. Offering wellness activities during the unpaid lunch hour also opens the possibility for employees to participate in wellness activities without sacrificing time after their workday ends.
It was not possible to match pre- and post-program ProQOL or intent to stay data to determine the effectiveness of the pilot program. The pilot program tested the feasibility of implementing a wellness program, and this program could be applied to a larger sample in the future. While this pilot program focused on mental health employees, all employees at the VA could potentially benefit from increased wellness services.
Applications to Professional Practice
An employee wellness pilot program was implemented utilizing employees to provide wellness services for mental health staff. ProQOL-5 and intent to stay data were collected pre-and post-program. Pre-program, participants indicted they did not intend to leave their current positions, apply for internal positions, leave the VA, or retire in the following year. Interestingly, post-program, participants intended to leave their current position, indicating either a position change within the VA, outside of the VA, or to retire. A comparison of pre- and post-program ProQOL-5 scores did not reach significance. However, the participants’ mean compassion satisfaction scores increased and mean burnout and secondary traumatic stress scores decreased, potentially as a result of this program. With limited resources for employee wellness, organizations may have to look at creative ways to support employees. Utilizing employees, who are trained in various wellness interventions, to offer programs was a cost-effective way to implement a wellness program.
Footnotes
Acknowledgements
I would like to thank Dr. Tara Sacco (St. John Fisher College), my DNP project advisor, for assisting with project development, data analysis, and manuscript editing and Dr. John Kirchgessner (St. John Fisher College), DNP Program Coordinator, for assisting with project development and manuscript editing. I would also like to thank Jennifer Funderburke (project PI), Jennie Tapio (research assistant), Kevin Whittaker (project clinical mentor), and Erek Biddle, Victoria Bridges, Leslie Charles, Joseph Kostecki, Danielle Lutz, Kevilyn O’Connor, Janice, Putrino, Sara Matteson-Rusby, and Nicole Quataert from the Department of Veterans Affairs for leading the wellness modules.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biography
Michelle L. Van Kirk, DNP, RN, PMHNP, is a behavioral health RN with the Department of Veterans Affairs. She recently finished her Doctor of Nursing Practice Degree at St. John Fisher College and is certified as a Psychiatric-Mental Health Nurse Practitioner.