
Abstract
Introduction
Compassion fatigue (CF) is defined as an adverse effect of helping individuals who have experienced traumatic events or who suffer from pain (Yu et al., 2016). Sorenson et al. (2016) defined CF as a condition characterized by a gradual reduction of compassion shown to patients over time. CF is also a critical concept for health institutions because it is associated with nurse retention and turnover, patient safety, and patient satisfaction (Jang et al., 2016).
As part of the healthcare team, oncology and dialysis nurses often spend the most time with patients and their families. Oncology nurses provide long-term care to patients and families, develop close relationships, and are exposed to patients’ pain and suffering (Austin et al., 2017). Consequently, oncology nurses are considered a group at most risk for CF and burnout (BO) (Jang et al., 2016). Dialysis nurses also provide care for the same patient over long periods of time, with dialysis sessions often lasting four hours per day, three days a week, and have to deal with the complex situations and emotions that chronic disease and treatment bring to the patient and family (Cao & Chen, 2021). These nurses often partake in difficult conversations, sharing bad news, and experiencing patient deaths, and thus may feel emotionally exhausted. Mendes (2017) stated that health professionals who provide care for patients with chronic kidney disease should also first accept that they may face the risk of CF due to their profession.
Background & purpose
CF is a culmination of secondary traumatic stress (STS) and BO (Stamm, 2005). BO stressors are related to the work environment and workloads, whereas STS is associated with direct exposure to traumatic situations. Although their symptomatology is similar, they often appear together (Turgoose & Maddox, 2017). Compassion satisfaction (CS), which is a concept that can balance the risk of CF and BO and reduce their harmful effects, is defined as the psychological reward of caring for others (Stamm, 2005). Duarte and Pinto-Gouveia (2017) found that about 25% of oncology nurses experienced high levels of BO and STS while Ja and Hyunjoo (2017) reported that 27.9% of oncology nurses experienced high levels of STS and 35% showed high levels of BO. A study that addressed the CF levels of nurses working as liver and kidney transplant coordinators reported moderate levels of CF (Kim, 2003). Wang et al. (2022) found that hemodialysis nurses had high levels of CF. Similarly, the literature shows that nurses working in the dialysis unit may experience BO because they are highly exposed to intensive and long-term interaction with patients requiring complex technological care (Hayes & Bonner, 2010). A recent multi-center study in China found that the burnout level of hemodialysis nurses in the Northeastern and Western regions of China was relatively high, and the associated factors related burnout was ordered as working atmosphere, night shift, relationships with colleagues, number of children, marital status, and specialist nurse training (Guo et al., 2021).
The purpose of this investigation was to add to the existing literature on this topic through a comprehensive analysis of CF, BO, and CS in a combined population of oncology and dialysis nurses. The study aimed to compare the levels of CF, BO, and CS of nurses working in oncology-hematology and dialysis services and to determine the predictors of each outcome.
Methods and procedures
Study design
This study used a descriptive and correlational design to compare the CF, BO, and CS levels of oncology-hematology with those of dialysis nurses following the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for reporting observational studies (von Elm et al., 2014).
Participants and setting
The research was conducted with 278 nurses from the oncology-hematology inpatient services, outpatient chemotherapy units, and bone marrow transplant (BMT) units as well as dialysis nurses of 4 private, 3 public, and 3 university hospitals having comprehensive oncology and dialysis treatment centers in Istanbul, Turkey. In Turkey, dialysis and oncology treatments are carried out in private, public and university hospitals. Istanbul encompasses 18.7% of Turkey’s population and since it has a good representativeness (Turkish Statistical Institute, 2022). Participants from all 3 hospital types in Istanbul were included to ensure sampling diversity. The hospital settings were selected purposively. A total of 298 nurses work in these hospitals. Because 15 nurses were not volunteered to participate and 5 nurses’ data were missing, total 20 nurses were not included in the study. The study was completed with 278 nurses.
Participants were enrolled using a convenience sampling technique from hospitals. The minimum required sample size was 250 (G-Power 3.1.3; Faul et al., 2007) to maintain a power level of .80, an effect size of .15 (medium), and a significance level (alpha) of .05 for multiple regression analysis. A convenience sample of 278 nurses was included in the study. Inclusion criteria included the nurses working in inpatient oncology-hematology, outpatient chemotherapy, BMT, and dialysis units and who gave voluntary informed consent to participate. Nurses having any current or previous psychiatric disorder and/or treatment and/or those working in pediatric oncology-hematology and dialysis units were excluded from the study.
Instruments
Personal information form
A personal information form was created by researchers after an examination of the existing literature (Hayes et al., 2015; Ja & Hyunjoo, 2017; Yu et al., 2016) and included 14 questions about sociodemographics, occupational information (such as willingness to work in the current unit, voluntary career choice etc.), working conditions, and the level of received social support.
Professional quality of life-IV (ProQOL)
Developed by Stamm and adapted to Turkish by Yeşil et al., the ProQOL is a self-reporting instrument consisting of 30 items and three subscales: CF, CS, and BO. The scale has no total score; each subscale is evaluated separately, and items 1, 4, 15, 17, and 29 should be reversed scored during the evaluation. The evaluation process of items was based on a six-digit chart ranging from “never” (0) to “very often” (5). In the Turkish adaptation, the Cronbach's alpha reliability coefficients were found to be 0.83, 0.62, and 0.81 for CF, BO, and CS, respectively (Yeşil et al., 2010). There was no cut-off point in the validity and reliability study of the Turkish version. However, Stamm stated in their evaluation performed with high- and low-range groups of 25% that scores above 17 indicate high CF levels while scores below 8 indicate low. Scores below 18 indicate low BO levels while scores above 27 indicate high, and scores above 42 indicate high CS levels while those below 33 indicate low (Stamm, 2005). Permission was given for the instrument.
Data collection
Prior to data collection, ethics approval was obtained from xxx university (No: 2018.342.IRB3.241), and permission to conduct the study was obtained from hospital administrators, after which data was collected from November 2018 to April 2019. The investigators, consisting of a nurse educator and an assistant professor, conducted individual, face-to-face interviews using questionnaires as a guide. Questionnaires were completed in the hospital in a quiet environment without interruptions. The questionnaires took approximately ten minutes for each participant to complete. The participants did not receive any gifts or monetary compensation.
Ethical considerations
Research committee ethical approval was received from Koç University Ethical Board of Social Sciences Research on 29 November 2018 (No: 2018.342.IRB3.241). Institutional permissions and verbal and written informed consent of the nurses were obtained before the study.
Statistical analysis
SPSS 26.0 software package was used to analyze the data. Before employing parametric statistical techniques, the Shapiro–Wilk test was used to ensure the data were distributed normally. Descriptive statistics were calculated for sample characteristics and the mean scores of CF, BO, and CS. A series of Pearson r correlation, t test, and one-way analysis of variance (ANOVA) were used to examine the associations between demographics, work-related characteristics, and the level of CF, BO, and CS.
CF, BO, CS scores were considered to be outcome variables which were explained by the independent factors. In the preliminary step, variables were checked for the assumptions of parametric statistical testing by the visual analyses of distribution plots, skewness, and kurtosis values as well as Shapiro–Wilks tests. Based on our univariate analysis, we conducted multiple stepwise linear regression analyses to reveal the predictors of CF, BO, and CS that contributed to three different models. Independent variables with p-values less than 0.20 in univariate analysis were used in the multiple stepwise linear regression analysis to improve the parsimony of the resulting regression model (Tabachnick & Fidell, 2015). Data met the assumptions of multiple linear regression analysis (multicollinearity, multivariate outliers, and multivariate normality [linear relationship, homoscedasticity, normal distribution of residuals]). We used adjusted R-square (R2) to compare across the models and explain the total variance. The α level was set at .05 for statistical significance.
Results
Participant characteristics
The sociodemographic and work environment characteristics of the nurses are shown in Table 1.
Nursing population demographics and ProQOL subscales scores (N: 278).
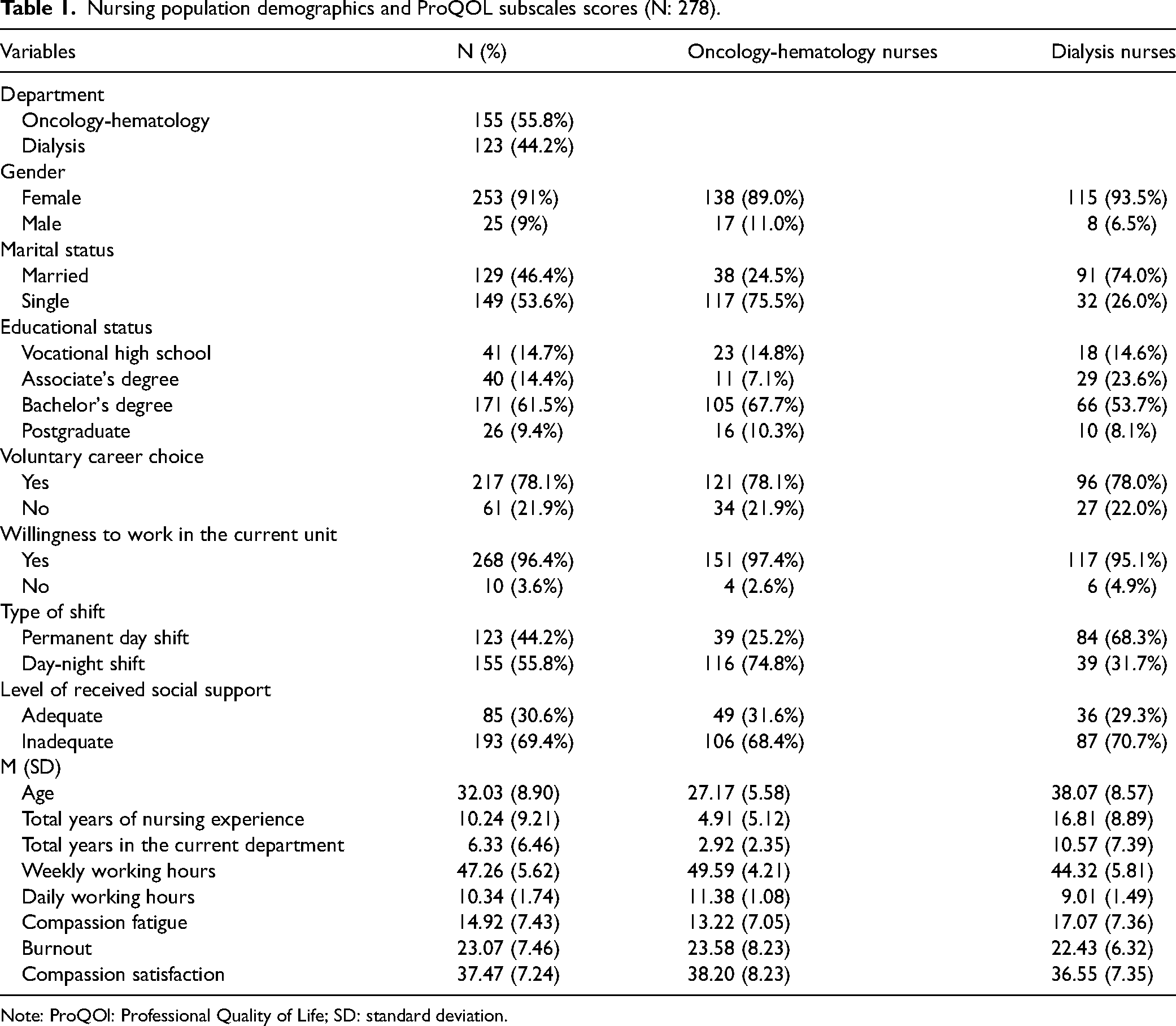
Note: ProQOl: Professional Quality of Life; SD: standard deviation.
Comparing the ProQOL-IV subscale scores of dialysis nurses with oncology-hematology nurses
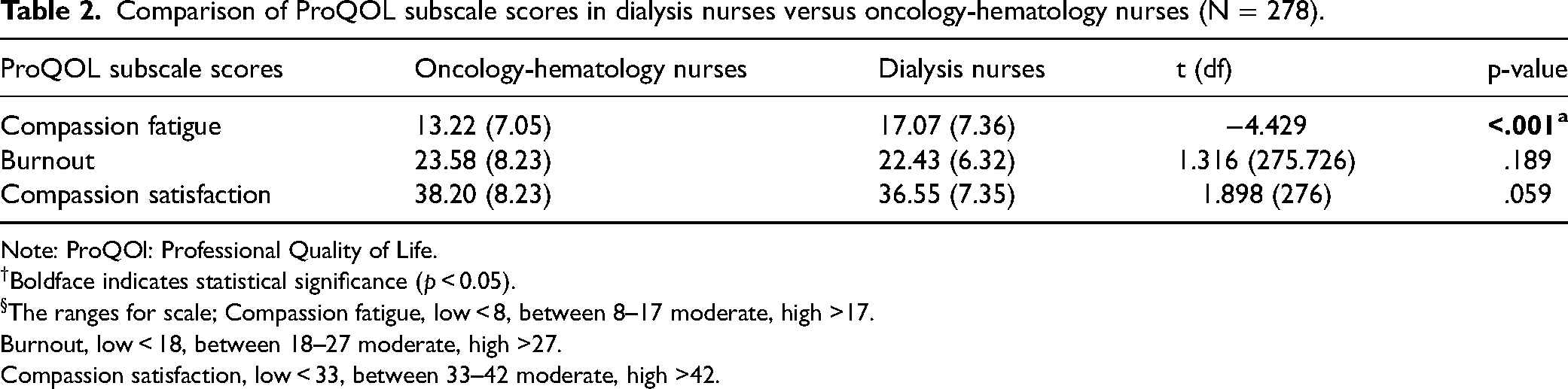
The CF, BO, and CS scores of the nurses are shown separately in Table 2. A sub-analysis comparing the oncology-hematology nurses with the dialysis nurses revealed that the CF scores of dialysis nurses were significantly higher than those of oncology nurses (17.07 ± 7.36 and 13.22 ± 7.05, respectively; p < .001; t = −4.429; see Table 2).
Comparison of ProQOL subscale scores in dialysis nurses versus oncology-hematology nurses (N = 278).
Note: ProQOl: Professional Quality of Life.
Boldface indicates statistical significance (p < 0.05).
The ranges for scale; Compassion fatigue, low < 8, between 8–17 moderate, high >17.
Burnout, low < 18, between 18–27 moderate, high >27.
Compassion satisfaction, low < 33, between 33–42 moderate, high >42.
Preliminary univariate analyses
The total number of years of nursing experience was significantly negatively correlated with BO (r = −.118, p = .05). On the contrary, there were positive correlations between daily and weekly working hours and BO (r = .163, p = .006, r = .181, p = .002, respectively).
There were no significant correlations between independent variables and CF and CS. Independent-samples test results showed that willingness to work in the current unit and the level of received social support were significant factors for CF, BO, and CS (p < .005). There were differences in the level of CF according to gender (t = 2.395, p = .017) and department (t = −4.429, p < .001). For CS, there was a difference according to whether or not the participants chose the nursing career willingly (t = 2.420, p < .001).
Multiple linear stepwise regression analyses with CF, BO, and CS
Multiple regression analysis reported three variables as independent predictors of CF: (1) willingness to work in the current unit, (2) department (dialysis or oncology-hematology), and (3) level of received social support. The model overall explained 9% of the variance in CF scores (F = 10.86, p < .001, adjusted R2 = 0.098; see Table 3). The multivariate analysis showed that working in the dialysis unit (β = 0.244, p < 0.001), an insufficient level of received social support (β = 0.171, p = 0.003), and unwillingness to work in the current unit (β = 0.121, p = 0.037) were associated with higher levels of CF (see Table 3).
Summary of multiple stepwise linear regression for variables contributing to CF, BO, and CS of nurses (n = 278).
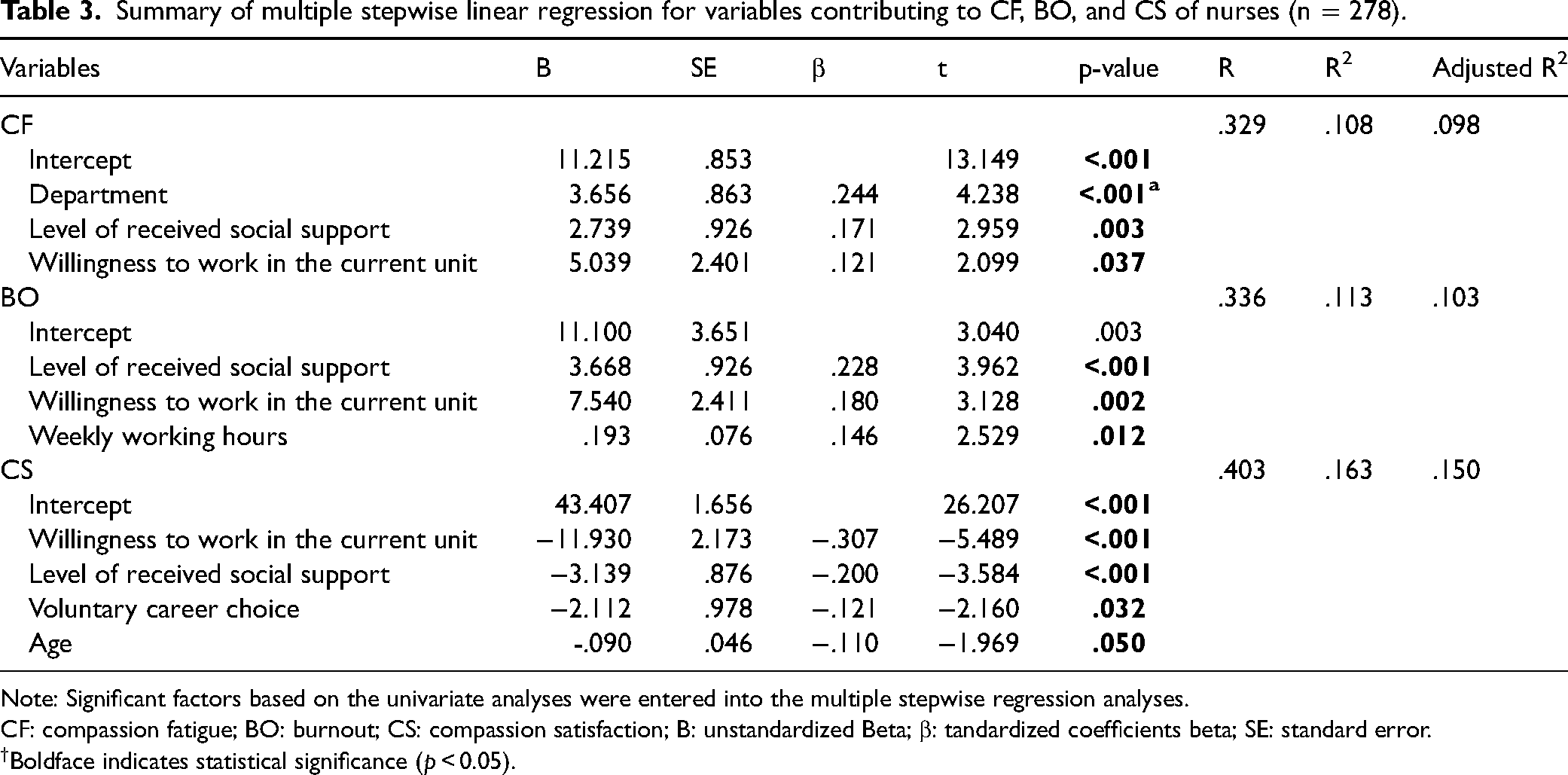
Note: Significant factors based on the univariate analyses were entered into the multiple stepwise regression analyses.
CF: compassion fatigue; BO: burnout; CS: compassion satisfaction; B: unstandardized Beta; β: tandardized coefficients beta; SE: standard error.
Boldface indicates statistical significance (p < 0.05).
Multiple regression analysis reported three variables as independent predictors of BO: (1) number of weekly working hours, (2) willingness to work in the current unit, and (3) level of received social support. The overall model explained 10% of the variance in BO scores (F = 11.41, p < .001, adjusted R2 = 0.103). The multivariate analysis showed that an insufficient level of received social support (β = 0.228, p < .001) and unwilling to work in the current unit (β = 0.180, p = 0.002) were associated with a higher level of BO. One additional working hour per week led to a 0.14 point increase in BO mean scores (β = 0.146, p = 0.012; see Table 3).
Multiple regression analysis reported four variables as independent predictors of CS: (1) willingness to work in the current unit, (2) level of received social support, (3) voluntary career choice, and (4) age. The model overall explained 15% of the variance in CS scores (F = 13.10 p < .001, adjusted R2 = 0.150). The multivariate analysis showed that unwillingness to work in the current unit (β = −0.307, p < .001), an insufficient level of received social support (β = −0.200, p < .001), and involuntary choice of career (β = −0.121, p = 0.032) were associated with a lower degree of CS. A one-unit increase in the age variable led to a 0.11 point decrease in CS mean scores (β = −0.110, p = 0.050; see Table 3).
Discussion
This study examined the levels of CF, BO, and CS and their associated factors among nurses working in oncology and dialysis units and important and remarkable findings were obtained. Although previous studies have examined levels of CF, BO, and CS in nursing populations, this is the first study, to our knowledge, that has considered department-specific comparisons in addition to the impact of sociodemographic and work environment factors on overall professional quality of life.
The level of BO and CS of nurses working in the oncology and dialysis units was moderate. However, while oncology nurses had moderate levels of CF, those of the dialysis nurses were found to be at the highest levels. In the literature, some studies have indicated that oncology nurses have both moderate (Wells-English et al., 2019; Yu et al., 2016) and high levels (Duarte & Pinto-Gouveia, 2017; Jang et al., 2016) of BO and CF. In the study by Karkar et al. (2015), 32% of dialysis nurses were found to experience high levels of BO, while 59.8% experienced low levels of emotional BO in a study by Ayraler et al. (2011). Similarly, Wang et al. (2022) found that hemodialysis nurses had high levels of CF. On the other hand, it may be considered a remarkable finding that contributes to the literature since there is limited study examining the CF levels of dialysis nurses, which in the present study were significantly high compared to those of the oncology nurses. Kotzabassaki and Parissopoulos (2003) reviewed that dialysis nurses mentioned the risk of CF being exceptionally high for those placed in a position to care for the same patients repeatedly or for those who find themselves dealing with complex patients frequently. The reason for this may be that dialysis patients do not like to change caregivers because they trust being treated by nurses who know their condition and with whom they have developed a bond — understandably, they like to see the same person again and again (Albayrak Okçin & Usta Yeşilbakan, 2020). However, this can be difficult for the caregiver. In this context, many dialysis nurses provide care for patients and their families on a longer-term basis. Naturally, a dialysis nurse who sees a patient a few times a week for years will be somewhat emotionally invested in their patient's care and his or her individual situation (Kotzabassaki & Parissopoulos, 2003). In a study by Hooper et al. (2010) evaluating the CF levels in nurses working in different specialties reported that CF levels of nurses working in the oncology unit for 14 years or more were significantly higher than those working in other branches. Therefore, long-term patient exposure is known to increase the risk of CF (Kotzabassaki & Parissopoulos, 2003). In our study, dialysis nurses had more experience than oncology nurses (4.91 ± 5.12 and 2.92 ± 2.35, respectively) both in the profession (16.81 ± 8.89) and the dialysis unit (10.57 ± 7.39). Karakoc et al. (2016) stated that 67.6% of dialysis nurses in their study worked in dialysis clinics for more than ten years, while Hayes et al.'s (2015) study indicated 47% worked over ten years and 25% over 15 years. Similarly in our study, dialysis nurses showed high levels of CF, more than the oncology nurses, and this may be explained by the fact that dialysis nurses provide care for people with chronic diseases for a more extended period of time.
Our study determined that CF levels of nurses who indicated that the level of support they received was sufficient were lower than others who stated that the support they received was not sufficient. In a study by Yu et al., which also examined the determinants of CF in oncology nurses, it was determined that social support, especially institutional support, was an essential factor in reducing CF and BO among health professionals (Yu et al., 2016). Similarly, Aycock and Boyle noted that support resources were effective in oncology nurses’ ability to cope with CF (Aycock & Boyle, 2009). In the literature, there was no study evaluating the determinants of CF in dialysis nurses. However, as in other specialties, the determinants of BO were defined as inadequate social support, inadequate top management support, inadequate transportation support, especially in dialysis sessions that started very early in the day, limitations of career planning, private sector holding 63.58% of dialysis practices in the country, and inadequate support such as day care (Kapucu, 2017; Süleymanlar et al., 2020). The relationship of these factors with the concept of CF in dialysis nurses may be discussed in further studies. However, although these variables (willingness to work in the current unit, the department, and the level of received social support) are associated with CF in our study, they only explained a small portion of the variance (9%). This finding may suggest that variables describing CF in future studies should continue to be examined in more detail. Cavanagh et al. (2020) also published a meta-analysis study in which they examined the prevalence of CF and associated factors among healthcare professionals. They stated that it was still unclear which sociodemographic characteristics were associated with CF and recommended that the root causes and specific determinants of CF should be examined in further studies (Cavanagh et al., 2020).
According to the model analysis results for CS and BO; it has been found that those who worked willingly in the department and considered the level of support they receive as adequate had higher levels of CS and lower levels of BO. Studies in the literature show that the positive work environment involving social support among oncology nurses increases CS in health professionals while reducing BO (Kelly & Lefton, 2017; Montross-Thomas et al., 2016; Wu et al., 2016). Similarly, Flynn et al. (2009) stated that dialysis nurses who rated their practice environments as least supportive were more than four times more likely to be burned out than register nurses who rated their practice environment as highly supportive. Vahey et al. (2004) found that factors associated with BO and job dissatisfaction included characteristics of the work environment, such as administrative support, nurse-physician relationships, and support services. The literature states that working long hours was one reason that both oncology and dialysis nurses experienced high levels of BO (Karkar et al., 2015; Potter et al., 2010). In this context, it may be concluded that the results of our study are compatible with the literature.
Our study determined that the levels of CF and BO of the nurses working willingly in the department were low, while they also had high levels of CS. This finding is considered a clue to nurse managers in allowing nurses the opportunity to work in the department they wanted. A study by Friese et al. (2016), conducted with oncology nurses, determined that those with high levels of job satisfaction had decreased intentions to quit their jobs. In a study by Arıkan et al. (2007), which examined BO and job satisfaction in dialysis nurses, reported that those who had chosen nursing willingly because they admired it had significantly higher job satisfaction and lower emotional exhaustion scores than those who had chosen it because they believed they would find a job more quickly after graduation. Karakoc et al. (2016) stated that 40% of nurses worked in the dialysis unit voluntarily, about one-third worked in this field due to managerial obligations, and those who became a dialysis nurse not by choice were characterized by a higher depersonalization score which represents a motivational, interpersonal distancing dimension of burnout. The fact that nurses working in a dialysis unit having higher levels of CF despite being qualified and willing to work in the department reveals the necessity of a better understanding of CF and requires a more comprehensive evaluation and awareness. Also, according to the results of our study, it is essential to ask and evaluate the preferences of nurses who have already been working in oncology and dialysis units or those who will be working there.
Some studies in the literature show that CS increases with age among health professionals (Harker et al., 2016; Sacco et al., 2015). Another study conducted with hemodialysis nurses also found that older nurses had higher levels of satisfaction (Hayes et al., 2015; Karakoc et al., 2016). Similarly, Duarte and Pinto-Gouveia (2017) conducted a study with oncology nurses and found that younger nurses had lower levels of CS than older nurses. However, it was determined in our study that CS decreased as nurses’ ages increased. In the study by Ling et al. (2020) stated that a level of working experience of at least 6 to 10 years was leading to higher nurse burnout. In our study, since the burnout level of nurses may be lower or their enthusiasm towards the profession may be higher at the beginning of the profession, their CS levels may also have been found to be higher. In addition, in our study, model analysis results created for BO and CS were found to explain only a small portion of the variance. It is recommended that further studies be conducted to examine the determinants of both BO and CS.
Limitations
There are some limitations to this research. Firstly, the collected study data are based solely on the nurses’ self-reporting. Secondly, we used a convenience sample of hospitals and nurses, which may not adequately represent the population by being a nonprobability sampling method. Moreover, a small portion of the variance in each model was explained by the determined predictors, indicating that other factors remain to be explored. Finally, the cross-sectional study did not assess the changes in the respondents’ professional quality of life over time.
Implications for clinical practice
The findings relate to the research indicated that oncology and dialysis nurses who work with chronic patients over a long period of time are at a high risk of CF and BO. In this respect, the results of this study have implications in two aspects. First, nursing educators should promote relevant on-duty training for oncology and dialysis nurses and raise their awareness of the possible negative influences (CF, BO) of working with patients. Second, nursing administrators should provide adequate support and design targeted interventions for nurses. Providing institutional support and providing nurses with the opportunity to prefer the department they like will improve their quality of work life.
Conclusion
The level of BO and CS of nurses working in the oncology and dialysis units was moderate, and there is no difference between them. However, dialysis nurses were found to have higher levels of CF than oncology nurses. It is essential to organize programs to evaluate, monitor, and prevent CF among health professionals engaged in chronic disease management such as dialysis-oncology. The results of this study may be considered a guide to nurse managers in monitoring nurses for signs of CF and the necessity of planning prevention programs. In addition, our study revealed the importance and necessity of institutional support to reduce the level of CF among nurses. Since it is the first study to evaluate the levels and determinants of CF, BO, and CS in dialysis nurses, it is recommended that further studies be conducted on the subject with a larger sample.
Footnotes
Abbreviations
Acknowledgements
The authors would like to thank all nurses who participated in this study for their valuable contributions. This study was presented as an oral in the Third International Clinical Nursing Research Congress online conference, Istanbul, 08–11 December 2020.
Author's note
Tuğba Pehlivan Sarıbudak, PhD, RN, is also affiliated at Istanbul Arel University, Faculty of Health Sciences, Cevizlibağ Health Campus, Istanbul, Turkey.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.