
Abstract
One of the great problems of caregivers and health professionals in recent times has been the so-called compassion fatigue and its association with burnout syndrome. Another pole of compassion has been described in terms of compassion satisfaction. Both propositions could be problematic in the caregiving setting. This is an analytical reflective article that through an apparent aporia tries to problematize and propose a theoretical synthesis that allows to denote compassion as a virtue in Aristotelian terms. To this end, it resorts to etymologies, translations and mainly to the classical theoretical references regarding compassion fatigue, compassion satisfaction and, of course, Aristotelian ethics. This is a theoretical bet that leaves open the discussion regarding the dichotomies compassion fatigue and compassion satisfaction; apathy and hyperpathy; and proposes to rethink compassion as a virtue, a reasoned middle ground, contextualized in the framework of care between two possible excesses.
Introduction
There are numerous publications today on issues such as moral distress, 1 burnout, 2 and compassion fatigue. 3 It is precisely this latter term that seems to be somewhat problematic because it has a blaming perspective on compassion and ultimately on care. Other authors have proposed compassion satisfaction as a guiding horizon to resolve this problem, but it may still be insufficient to denote what is meant when we talk about compassion, especially when using pleonasms or redundancies such as compassionate care, and on the other hand oxymorons or nonsensical expressions, such as uncompassionate care or dehumanized care. 4 These adjectives about care can be problematic and confusing, some questions around it have arisen especially because of the increasing technification of life, the loss or transvaluation of values and, therefore, transformations of health services and the practice of health professionals. However, they have been described as problematic because they do not denote the essence of the problem, since adjectives are used to modify the essence of concepts such as care, human and compassion. What is the ontological essence of care? What does it mean to humanize care? Are we humans’ beings with virtues and vices or only virtuous ones? Can care exist without compassion?
Background
Previous theoretical developments on problematic adjectives in the framework of care can be expanded in “the deconstruction of humanization: towards the dignity of health care”: “Talking about humanization can be a term that denotes egocentrism as a human characteristic, since it confers to the human category a superlative benevolent character, nowadays everything from dogs and cats to health and education are humanized, what is different in humanizing a dog and humanizing health or education? Are pets or health really being conferred human characteristics? When we talk about humanizing animals, we refer to assigning characteristics and activities to animals that do not have them, do not need them and therefore can be counterproductive, for example, a costume party for dogs, sharing the table and the same food with pets, overloading them with decorative objects or exceeding hygiene measures. Now, when allusion is made to humanizing a dehumanized health, in the sense of the loss of humanistic values, the commercialization and technification (they are human activities) of health are intimately linked to the human, it is necessary to assume that the human implies perfectibility and not perfection, that the exchange, the technical and of course some defects or anti-values, such as selfishness, cruelty, greed, among others, are human.” 5
The notion of compassion, in the context of the discussion of moral sentiments in the West, has gone through several stages. Greek philosophy, represented by Aristotle, focused on benevolence and altruism, but did not yet develop the concept of compassion as we recognize it today. The great religious traditions recognized and cultivated compassion as a central part of their ethics, especially in relation to the condition of human frailty and suffering. In Eastern philosophical traditions, compassion is part of the cardinal virtues of Taoism (compassion, moderation and humility) and the Four Sublime States (or Divine Abodes) of Buddhism (loving-kindness, compassion, altruistic joy and equanimity). 6 The 18th century marked an important transition through the work of philosophers such as Adam Smith, the Earl of Shaftesbury and Francis Hutcheson, who attempted to balance reason and emotion in ethics. 7 In the context of empiricism, enlightenment, and utilitarianism, according to Macintyre, the notion of compassion, for Smith and Hume, is no more than a “philosophical fiction” to bridge the gap between universal and particular reasons that motivate human behavior. 8
The influence of Immanuel Kant privileged reason rather than emotion as the basis for moral 7 deliberation, challenging, for example, what some authors call “Scottish sentimentalism,” represented by authors such as David Hume (who defines compassion as the common passion that allows us to share the feelings of others) 8 or the physician and ethicist John Gregory, 9 defender of the notion of sympathy in the doctor-patient relationship. Some critics, such as Arthur Schopenhauer, argued that Kant had abandoned the heart of morality by ignoring compassion. 7 In this sense, Kantian ethics defines two modes of compassion: proximal compassion characterized as a form of emotional contagion that interferes with our ability to make rational decisions, while distal compassion is active and based on reason, and constitutes a fundamental element in Kant’s explanation of the duties of virtue. 10
Denoting dichotomies or apparent conflicts to refer to issue’s factors related as significant as burnout, compassion, compassion fatigue, objectification of the subject, and the loss of warmth in attention can be complex, especially because attention is diverted from what is truly important. We are language, language constructs the reality of phenomena, hence logical, etymological, and conceptual analysis is of radical importance for addressing bioethical problems. Therefore, pseudo-conflicts generate false tensions or dichotomies, which somehow become aporias, that is, sterile contradictions that do not allow us to reach either a Hegelian synthesis that resolves the tensions, or a convergence of principles in the sense of Maliandi. 11
Compassion has been of interest to bioethics, according to Washburn 12 ethics is concerned with human constants such as finitude, compassion, suffering and solidarity. The bioethical response is first and foremost a compassionate response that recognizes in the other a suffering subject, a face in Levinas’ sense and not just a simple face. Defining or conceiving compassion as a feeling, a passion, a virtue, a commandment, a moral weakness, a form of covert selfishness, a feminine attitude (as Spinoza saw it), denotes practice with respect to compassion and thus allows us to problematize conflicting adjectivations and substantivations such as compassion fatigue and compassion satisfaction, all within the framework of bioethics and care.
Methodology
This is an article with a theoretical critical approach that problematizes terms such as compassion, empathy, sympathy, compassion fatigue, and compassion satisfaction. It uses etymological tools to delve into the meaning and relationship of terms, but also philosophical proposals within the framework of ethics and bioethics. In this case, the authors include Aristotle and his work Ethics to Nicomachean, Heidegger 13 and the concept of Sorge as care and concern, and contemporary references that have developed theoretical propositions regarding care and compassion. The theoretical objective initially is to problematize or in the sense of Maliandi 14 thematize an apparent pseudo-conflict inherently unresolved between compassion satisfaction and compassion fatigue, both related to the field of care, a field in which the essence of care and nursing discipline seems to be undermined; ignoring the usual extrinsic historical and social triggers related to this false conflict. In the second instance, there is a propositional aporia, that is, to transcend the contradiction to denote compassion as a virtue within the framework of care.
Etymological analysis of compassion, empathy, sympathy, care, and nurse
Etymologically, compassion comes from the Latin word “cumpassio,” which is composed of the prefix “cum,” which refers to convergence, meeting, together, that is, to alterity and disposition, giving rise to synonyms such as company, companion, and community; the word “passio,” “to feel,” which in turn comes from the Latin verb “patior,” meaning “to suffer or endure.” 15 But in Greek could be replaced by “Παθο” passion in the classical Aristotelian sense; finally, the last grapheme of compassion is the suffix “-sion,” which denotes action and effect. In this sense, two possible etymological definitions of compassion could be conceived; the first of them compassion as the action and effect of accompanying the other in their pain or suffering; secondly, accompanying the other in their passions (whether positive or negative). For now, in a preliminary way, I venture to outline a general construction of compassion as a challenge to become one with and for the other, in which the limits of the individual must be transcended, recognizing that every other is another like me and not a mere abstraction; therefore, compassion implies recognizing, understanding, accompanying, being present and willing with and for the other.
Compassion implies a paradoxical communion with the other and an overcoming of conventional moral distances. As Kearney 16 states, “compassion represents an appropriate way of being ‘close’ to pain.” Compassion has as its object of understanding suffering, injustice, and moral failure. 7 Unlike sympathy and pity, compassion involves an unequivocal intrapersonal identification with the other, but also recognizes their otherness. 17 In Murdoch’s terms, 18 and from the perspective of the sovereignty of the good and the ethics of love, compassion represents a purified form of eros that transcends the selfish illusion of human desire, as an imaginative attention that treasures the other in the justice of his or her own reality. “It is in the capacity to love, that is to see, that the liberation of the soul from fantasy consists of. The freedom which is a proper human goal is the freedom from fantasy, that is the realism of compassion.” 18
Sympathy and empathy, although very similar to compassion, require some clarification of differences. Empathy comes from the Greek “Παθεûv,” epathon, meaning “to feel,” and the inseparable prefix “εv,” which means inside. In this way, it is a feeling that enters into the other, penetrating with him, to some extent, putting oneself in the other’s shoes, 19 so it has been criticized in the sense that no matter how much one tries to assume someone else’s pain or passion as one’s own, it seems somewhat utopian. 20 Sympathy comes from the Greek “συμπάθεια” (sympátheia), broken down into the prefix “syn-” (συν), which means “together” or “with,” the noun “pathos” (πάθος), which means “suffering” or “experience,” and the suffix “-ia” (-ία), which was used to form abstract nouns and denotes a quality or state. It means a community of feelings, but the semantic derivation has turned it into an affective inclination between people, generally spontaneous and mutual; and today, a person is called sympathetic if they have a “way of being and character that make them attractive and pleasing to others.” 21 The separation between terms can be problematic but given the connotative use of language regarding sympathetic people as a reaction to the other’s pain, not necessarily recognizing oneself and the other as vulnerable beings, sympathy at least seems to be at a lower scale of compassion and empathy in the use of the term.
The separation between terms can be problematic; but given the connotative use of language regarding sympathetic people as a reaction to the pain of the other, not necessarily recognizing self and other as vulnerable beings; sympathy at least, in the use of the term seems to be on a lower scale of compassion and empathy. Some authors, Stevens y Woodruff,
22
propose an explanatory model from empathy to compassion (Empathy to Compassion-EtoC). The model assumes that the process from empathy, to sympathy, to compassion is marked by a dynamic shift of attentional resources between egocentric (other as self) and allocentric (other as other) representations, in which the observer represents the other as the self, or the other as the other, then oscillates rapidly between these two representational states through sympathy and compassion. The authors’ proposal shows how in empathy there is a turning towards the other that exceeds reasonable limits, while in sympathy an egocentric approach is maintained and finally in compassion with an allostatic approach it seems to respond appropriately to the suffering of the other, as can be seen in Figure 1. Empathy to compassion-EtoC model. Taken from: Stevens, L., and Woodruff, C. C. (Eds.). (2018). The neuroscience of empathy, compassion, and self-compassion. Elsevier/Academic Press.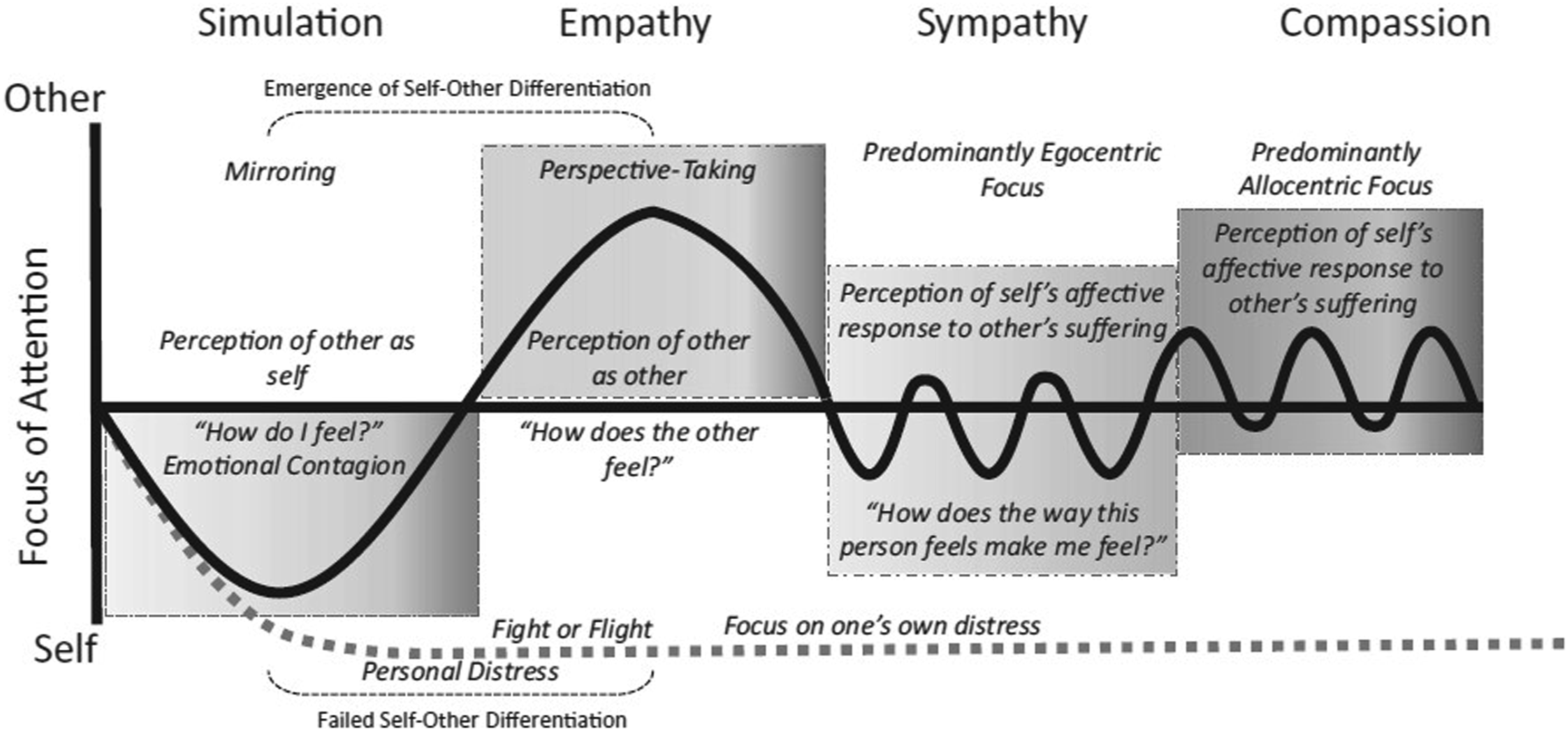
Sympathy has been a fertile concept in philosophy, authors such as Hume and Smith made theoretical contributions to the concept. According to Hume, “no quality of human nature is more remarkable, either in itself or in its consequences, than the inclination we possess to sympathize with others and to receive by communication their inclinations and feelings even though they may be different or contrary to our own.” 23 In this way it could be described that sympathy is a passion that generates affections, as a kind of emotional contagion that makes action possible, “a jovial aspect produces a sensitive complacency and serenity in my spirit; in the same way, an irritated or sad aspect fills me with a sudden discouragement.” 23 Therefore, it seems that sympathy seems to fall short in the contextual framework of care, it does not allow us to respond to the suffering face of the other.
Nurse, in the case of the Spanish term (noun enfermera, o), comes from the Latin word infirmus, where the prefix “in” means negation or lack, “firmus” means firmness, and the suffix “ero” means occupation or profession. 15 In Latin, the term “infirmitas” was used in a context of being weak but not sick, weak constitution or of gender or weak state (women and children); while the term used to qualify the disease was “morbus-i.” In other words, a nurse is someone who takes care of those who have lost their firmness or who are weak, they are an actor who helps another person regain their solidity, and a profession that solidifies the other. In the English language, the word nurse has its origins from the French word “nocerice” and the Latin “nûtrio, is, ire” which means to feed, nourish or rear; 24 hence many caring practices are associated with feeding or rearing another, represented in everyday expressions such as “he is very well-fed, that's because he has been taken care of very well.” In this sense, the concepts of nursing in Spanish and nursing in English, although they share roots in the sense of helping others, are not completely homologous. It is worth noting that no concept can encompass the heterogeneity of social practices, especially one as complex as nursing. However, as historical representations and descriptions of a phenomenological social reality, they can help us understand the changes in social and historical dynamics.
The word “care” (cuidado as a noun in spanish) in its etymological sense (One of the various meanings that can be analyzed) “refers to the action of caring and comes from the Latin word cogitatus” (reflection, thought, reflective interest that one puts into something). The verb cogitare is composed of “co,” joint action, and agitare (set in motion) a frequentative of agere (move forward, advance, move). 15 Care is then a joint action that is characterized by a reflective, reasoned, and dialogical interest to help and accompany another who is vulnerable. It is somewhat striking the etymological relationship between care and thought reason, which allows us to transcend some conceptions of care not associated with reason in the practical sense. At this point It is necessary to mention that the theoretical development around the concept of care is vast, authors of the stature of Heidegger have analyzed care in an ontological sense, that is, as a characteristic of being in the world, which Heidegger calls Sorge, openness, and concern. Since caring primarily involves thinking, knowing the reality of the other, being open to the other, it is a reflective act to mobilize or act for another who needs and demands it. 25
In this sense, a triple etymological relationship can be spoken of between care, nursing, and compassion. However, if care is essentially compassionate and compassion is required to care, describing care without compassion or lack of compassion in care associated with terms such as humanization of care and dehumanization of care can be problematic expressions. There is no caring without compassion. Asserting that this exists implies erasing the essence of care and blurring it, which is a contradiction. On the other hand, adjectivizing it with the word humanization is bizarre. In humans, there are impulses of life and death, we can be selfish and petty. Likewise, the dehumanization of care, at least in the sense of lack of compassion, does not represent intentionality and tends to be confusing. What quality of the human needs to be added to care to speak of humanized care? Perhaps it could simply be spoken of as care, if it is understood that compassion is its essence. Instead of resorting to literary figures, pleonasms, and oxymorons, the factors that make care essentially what it is, a compassionate act, could be described.
From the dichotomy of compassion fatigue and compassion satisfaction to compassion as a virtue
Burnout, understood as a syndrome of professional exhaustion, has a theoretical and literary development prior to compassion fatigue, as can be shown in the theoretical development of Freudenberger in 1974 26 and, Maslach and Jackson in 1981. 27 Years later, other authors 28 described vicarious traumatization as that transformation in the internal experience of a psychotherapist that arises as a result of empathic engagement with the traumatic material of clients. Subsequently, Figley 29 described compassion fatigue as the suffering or stress caused by an effect of compassion as the natural behaviors and emotions that arise from the knowledge of a traumatic event experienced by a significant person, that is, the stress resulting from helping or wanting to help a traumatized person. This same author maintains that “Compassion fatigue is identical to secondary traumatic stress disorder (STSD) and is the equivalent of PTSD.” 29
Regarding compassion satisfaction, while from a theoretical standpoint, certain antecedents can be outlined from philosophy in Nietzsche in the sense of will power as a creator of vital meaning, that is, an invitation to transcend the compassion inherited from suffering and Christian guilt. “To me you have too cruel eyes, and you look lasciviously at those who suffer. Has your voluptuousness only disguised itself, and is that what you call compassion?” 30 This philosopher suggests a sumptuousness that is masked in the compassionate gesture. It is only in the 21st century that the concept of compassion satisfaction is coined in contrast to compassion fatigue, feeling that it is a pleasure to help others through one's work, and that pleasure motivates one to continue participating with diligence in compassionate relationships.31,32
Problematic adjectives then return if we consider Freud's pleasure principle; on certain occasions, we must act moved by the pleasure that we find in sympathizing with others, while in other situations, perhaps to safeguard the psychic structure, we should distance ourselves from compassion because it causes displeasure or pain. On the other hand, it is problematic to describe compassion as a tiring act; although anything that requires energy or libidinal expenditure in Freud's sense could tire a person both physically and mentally, which poses an axiological problem between two antithetical values; this could be counterproductive within the framework of care. It could be that compassion is not a sine qua non condition for physical and emotional fatigue, but that certain social, work-related, historical, and moral and economic recognition factors play a much more determining role in physical and emotional exhaustion. 2
Now, what if we do not contemplate compassion as a value that can have its counterpart, nor as a passion that moves us between the instincts of Freud’s pleasure principle, but rather we reconfigure compassion as an Aristotelian virtue, although Aristotle per se never conceived it as such. According to the Stagirite, passions are “appetite, anger, fear, courage, envy, joy, love, hate, desire, jealousy, compassion, and everything that is accompanied by pleasure or pain.” The faculties are those capacities by virtue of which we say that we are affected by these passions, for example, that by which we can become angry, sad, or compassionate, while the modes of being, that by virtue of which we behave well or badly regarding passions.” 33 It should be clarified that virtues are not passions; passions move us, while virtues dispose us. According to Aristotle, virtues are not faculties either; we are not good or bad because of the capacity to feel passions. Virtues are the way of being that tends to the relative mean point regarding us, the concrete situation, and the due reason; they are equidistant between two extremes (vices), one by excess and the other by deficiency. 33
Compassion as a virtue is in the middle ground between a hyperpathy that exhausts and fatigues to such an extent that it can lead to an apathy that makes it impossible to act and constitutes the other extreme; satisfaction by compassion will have to be decided what is the end of it; if the end is pleasure, although more praiseworthy than apathy or hyperpathy; it can lead to apathy when it stops finding pleasure, or tend to hyperpathy by the condition of insatiability or displacement of the object of desire; if pleasure comes during the process not as an end but as something added, it is then a compassion that is satisfied in itself and not in desire, hence it can be a virtue in the framework of care; finally compassion fatigue may be a consequence of hyperpatia, or of other social, historical or relational factors that exceed compassion, but above all compassion as a virtue will not fatigue, it cannot be a pathology, much less the precursor of professional burnout in the framework of care. These relationships can be represented in Figure 2. The virtue of compassion: the middle ground between hyperpathy and apathy. Author’s construction through Draw.io.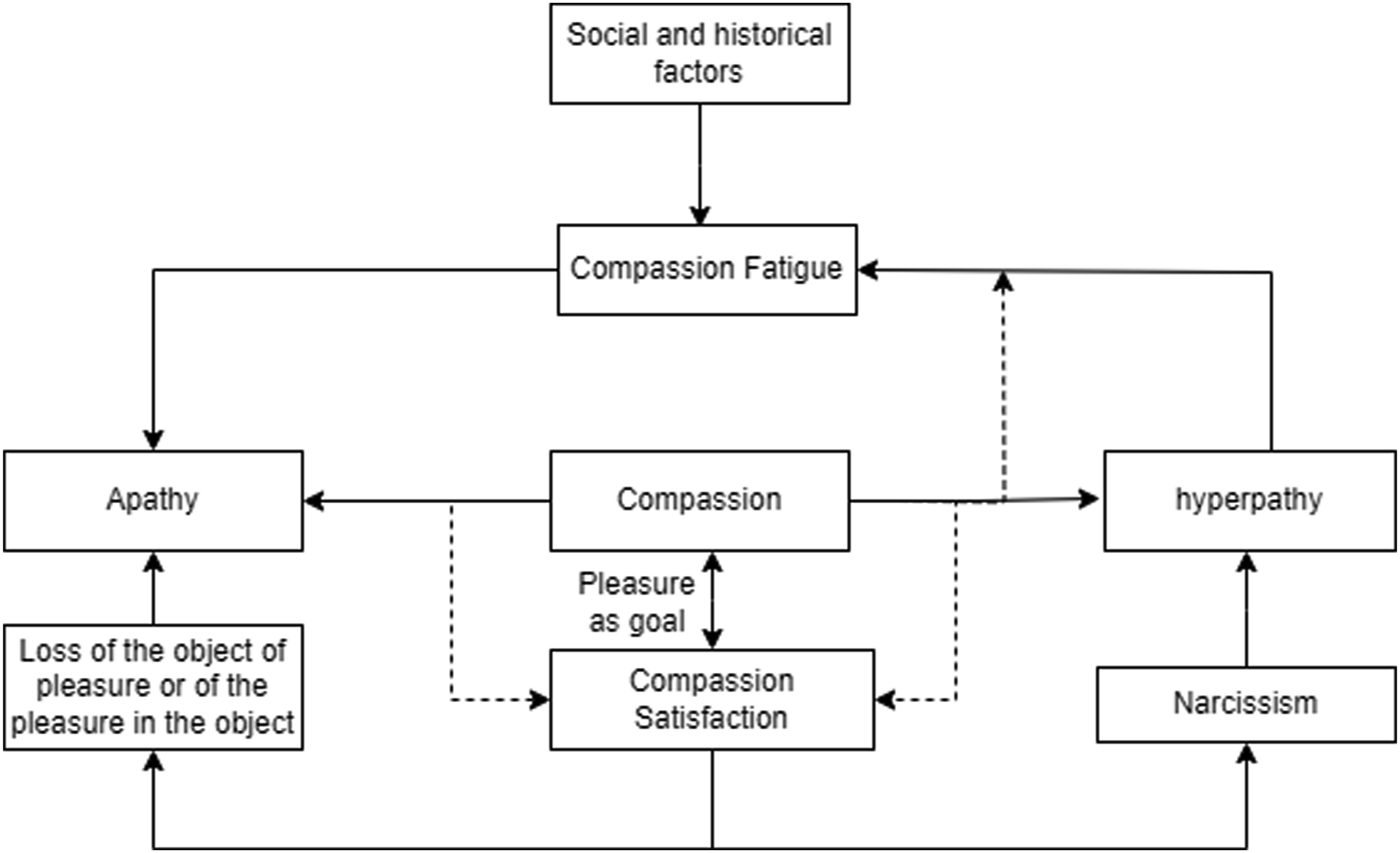
In this sense, the bet is, on the one hand, to depathologize compassion (compassion fatigue), and on the other hand, to avoid compassionate narcissism, to put compassion as a virtue, as the essence of care at the center of the discussion. To do so, it is necessary to delve a little further into Aristotelian ethics. According to Aristotle, the dianoetic virtues (wisdom, intelligence, and prudence) originate and grow mainly through teaching; therefore, they require experience and time. Ethical virtues (liberality, moderation, justice, friendship, among others), on the other hand, come from the will and can be acquired or strengthened by habit and custom. Naturally, man is not virtuous because learning and habit are required. Moreover, something that exists naturally could not be transformed by custom. This is exemplified by the author through the following statement: “practicing justice makes us just; practicing moderation, moderate, and practicing manhood, manly.” 33 At this point, two important clarifications must be made: by practicing compassion, we become compassionate, and it is necessary to train and educate in compassion. Otherwise, prudence and reason would suffice to control it as a mere passion.
In such a way that compassion can be an end in itself, of course a path to eudaimonia, but it cannot become a narcissistic vice that seeks pleasure, nor a sacrifice that consumes the psychic, physical, spiritual, and social apparatus of caregivers. In this sense, compassion is proposed as an Aristotelian ethical virtue that could be the right middle ground between compassion fatigue and compassion satisfaction. For this, it requires the other intellectual virtues and a syncretism between mathesis (learning) and askhesis (exercise), because virtuous men act and live consciously according to virtue.
According to Pellegrino, 34 “compassion is a virtue because it is a habitual disposition to act in a certain way, a way that facilitates and enriches the telos or purpose of any human act we perform.” In this case, it is the act of caring for someone. Compassion is the character trait that shapes the cognitive aspect of caring to suit the unique situation of each person or suffering being. According to this same author, 34 compassion is a mixture of affections, words, gestures, languages, silences, listening, emotions, but as a virtue in the classical sense it has a moral and an intellectual component. In this sense, for the cognitive bet of the virtue of compassion, according to Pellegrino, 34 a certain epoche is paradoxically required, a suspension of attachment, of the affective component, a kind of retreat that allows not to completely blur the limits of the self in order to respond for the other, with the other and from the other in search of the solidification and lessening of suffering. “As a virtue, compassion also aspires to a means. If a caregiver identifies too much in suffering with the other person, “he or she may lose the objectivity essential for the more accurate assessment of what is wrong, what can be done, and what must be done to meet those needs [...]. Co-suffering, too, has the danger of such close identification with the patient's suffering that the professional may unconsciously impose his or her values on the other.” 34 Therefore, compassion as a virtue has vices by excess or defect that should be avoided.
The secularization of morality and the search for an alternative basis for ethics after the withdrawal of religious influence demands a new rationale regarding the cultivation of moral sentiments, given that there is no universal taxonomy and that there are differences in the way terms such as “compassion,” “empathy,” and “sympathy” are used, as well as in the way various moral situations are interpreted. 7 In the context of health care, the notion of compassion persists as a significant virtue, so its precision is also relevant. 35 Some authors even propose, not only its philosophical or psychological characterization, but its measurement. 36
Taking up some of Schopenhauer’s theoretical contributions may be valuable for further developments regarding the topic of compassion in the context of nursing care, but also as an ontological bet in a world that requires compassionate caregivers of ecobionts and holobionts. In some sections, Schopenhauer proposed as a presupposition of compassion an identification that the barriers of individuality that separate beings are mere appearances and that behind them lies an essential identity of all those beings. Therefore, for those privileged enough that the other is no longer a “non-self” but “again oneself,” and the pleasure and pain of others become a motive for their desire of equal or greater relevance than their own, they have discovered “the ultimate secret of life”: that evil and malice, suffering and hatred, victim and perpetrator, are the same, even when they appear different in representation, compassion is born, the source of all moral actions and the only possible foundation of morality. 37
Conclusion
Talking about compassion satisfaction could be problematic as it seems to distort the essence of care, the other. But accepting terms like compassion fatigue in the context of an ethics of care may also seem bizarre, as it seems to be playing a heuristic that is not played on the side of compassion, or ultimately of care that does not lose its essence. A critical review of concepts does not necessarily solve questions; on the contrary, it leaves a deliberative landscape characteristic of bioethics.
Regarding exact knowledge, such as the axioms of mathematics, there is no deliberative process because they cannot be otherwise. But regarding compassion as a virtue or as a passion, a discussion is necessary in the context of care and ethics, since deliberation is not about ends, but about the means that lead to the ends. Because once the end is determined, it is investigated, analyzed, and discussed which means are possible to achieve it in the best possible way. Bioethics is above all a field of knowledge and practice turned to the ethos and to life, it is a compassionate commitment, it is a recognition that favors rapprochement, it is a questioning that arises from the other and implies a response, a response that transcends the limits of the self, this response implies reasoning in the sense of cogito cogitare, to accompany from the finitude and welcome the other in his suffering, trying to solidify it by caressing it without grabbing it. A commitment to the virtue of compassion may be the path to a reasoned, reasonable and ontological practice of compassion, consequently, so will be the care, if compassion fatigues or satisfies, will care fall into compassionate narcissism or will it wear out until it ceases to be what it is?
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article is part of the development of the doctoral thesis, as a project funded by the Ministry of Science and Technology of Colombia, administered by the Autonomous University of Bucaramanga and El Bosque University. In addition, the authors will receive co-financing support from Remington University Corporation and El Bosque University for publication and editing expenses.