
Abstract
Background: Few studies have reported associations between occupational exposure to tannery chemicals with breathing difficulty and skin diseases and none have been conducted in Bangladesh. The aim of this study was to investigate the associations of health complaints with types of work and length of employment among tannery workers in Bangladesh, where occupational health and safety regulations are less restricted compared with the developed world. Methods: One hundred sixty-seven (n = 167) workers from 10 tanneries were interviewed using a questionnaire adapted from the European Community Respiratory Health Survey (ECRHS) and the Tasmanian Longitudinal Health Study (TAHS) to collect information on occupational exposures and health outcomes. Workers’ length of employment was examined, as well as their areas of work including beamhouse, wet finishing, dry finishing, and miscellaneous. Univariate and multivariate logistic regressions were performed to investigate potential associations while controlling for confounders. Results: Length of employment was positively associated with breathing difficulty (odds ratio [OR]: 1.32, 95% confidence interval [CI]:1.07–1.64). Workers involved in the wet finishing (OR: 11.75, 95% CI: 2.12–65.10) and dry finishing (OR: 13.38, 95% CI: 1.00–181.70) had higher odds of breathing difficulty; while, working in the beamhouse was associated with an increased risk of developing skin diseases (OR: 4.36, 95% CI: 1.10–17.32). Conclusion/Application to Practice: Length of employment and types of work were associated with increased risk of health complaints, including breathing difficulty and skin disease among tannery workers. Stronger regulations with regular enforcement, regular health surveillance, and worker and employer education are necessary for reducing these exposures and improving the health outcomes of the tannery workers.
Background
Leather is used in a range of consumer goods, including footwear, apparel, furniture, and other leather products. The global value of exports exceeds US$100 billion for hides, skins, leather, and leather products (The United Nations Industrial Development Organization, 2010); developing countries share about 45.8% of the global value of exports (Mascianà, 2015). Occupational health and safety (OHS) practices in most developing countries do not meet the standards that are generally in place in more developed countries which often also have stronger regulations. Developing countries generally have limited OHS programs as well as limited or underdeveloped and under enforced laws and regulations than those in the developed countries (Febriana et al., 2012a; International Labour Organization, 2011; Rantanen et al., 2004). High unemployment, low labor costs, lack of regulation, and weak enforcement of safety and environmental regulations make poorer countries very profitable for business ventures (Febriana et al., 2012b). In Bangladesh, the leather industry has a significant role in the national economy (Azom et al., 2012; Paul et al., 2013; Tinni et al., 2014). In 2017, the leather industry accounted for 0.35% of the total gross domestic product (GDP) in Bangladesh and for 3.54% of the annual export of US$1.2 billion (Razzaque et al., 2018). Currently, Bangladesh has 313 tanneries, of which 90% are established in the Hazaribagh area, which is situated within the center of the capital city, Dhaka and the bank of river Buriganga (Akhtar & Shimul, 2015; Biswas & Rahman, 2013). During the peak season 1 , Peak season starts after Eid-ul-Fitr and Eid-ul-Azha (the biggest Islamic festival) approximately 12,000 to 15,000 laborers work daily and discharge 7.7 million liters of liquid waste and 98 metric tons of solid waste every day (Azom et al., 2012; Yoshinaga et al., 2018). Although the tannery industries are essential to the export-oriented economy in Bangladesh, the lack of basic environmental protection measures contributes to serious threats to environmental sustainability and public health (Bhowmik, 2012). The local community, civil society, environmental activists, international rights groups, and buyers consistently advocate that the government ensure environment-friendly leather processing and occupational safety in the leather tannery industries (Bhowmik, 2012). In response, 106 tanneries have been moved in attempt to revitalize the environment and the river Buriganga (Rashedul, 2018).
The Tanning Process
The tanning process mainly consists of four steps including beamhouse operation, wet finishing, dry finishing, and packing as recommended by the European Commission (Black et al., 2013; Buljan & Kral, 2019; Sathiyamoorthy et al., 2013). There is a considerable variation in steps between tanneries, depending on the type of leather being produced. There is also significant variation in the scale and types of tanning facilities between developed and developing countries (Stellman, 1998). Tanneries in developed countries like the United States, Australia, and Europe are highly mechanized and use closed automatic systems and many chemicals (Black et al., 2013; Buljan & Kral, 2019), whereas in developing countries like Bangladesh, Pakistan, Afghanistan even India still uses mostly manual work and natural tanning substances with techniques remaining unchanged over a long period (Hashmi et al., 2017; Kesarwani et al., 2015; Öry et al., 1997a).
In the beamhouse, the raw hides are stretched on bamboo frames, by pegs or by spreading on the ground in the mild sun. Beamhouse operation workers are exposed to various dusts and chemical agents during preparatory operations such as soaking, liming, fleshing, deliming, bating, and pickling (Black et al., 2013; Buljan & Kral, 2019). Tanning involves the application of chrome (III) compounds or various barks in the case of vegetable tanning (Sathiyamoorthy et al., 2013). Wet finishing includes splitting, shaving, waxing, and oiling (Black et al., 2013; Buljan & Kral, 2019). Workers do not have direct contact with water or chemicals in this stage; however, they may experience exposure to oil products and chemicals while processing wet hides as well as in the dry finishing stage as drying, shaving, buffing, pressing, padding, and spraying (Black et al., 2013; Buljan & Kral, 2019). Exposure to dust particles generated from leather and paint during operating machinery and spraying are the specific hazards in this stage (Öry et al., 1997a). Finally, several workers perform duties as packers, sweepers, carriers, and mixers of chemicals which are considered “miscellaneous.” The workers in this group have the chance for multiple co-exposures as they move from one section to other during their daily work, and their duties may change from time to time. They carry raw hides and skins and mix chemicals with bare hands.
Occupational Health Concerns
Chemical waste from tanneries’ effluents contain chromate and bichromate salts, aniline, butyl acetate, ethanol, benzene, toluene, calcium salts, chlorine, surfactants salts, sodium sulfide, sulphuric acid, organic matters, toxic or poisonous substance, and dyes (Azom et al., 2012; Rastogi et al., 2008). Approximately 40 different types of chemicals are used in the tanning process, while only 20% of the chemicals are absorbed by the leather, and the remaining 80% is released as waste (Azom et al., 2012; Islam et al., 2014). Tannery workers are exposed to many hazardous materials and processes during the tanning of hides and skins. Chemicals used in the tanning process have been reported as potential irritants and sensitizers to the workers (Febriana et al., 2012a; Hedberg et al., 2018; Kolomaznik et al., 2008; Syed et al., 2010). In addition, infection is a constant hazard to the workers because of exposure to a high concentration of pathogens in the raw materials (Işsever et al., 2007; Skóra et al., 2014). A case-control study from Kenya reported a higher prevalence of dermatological symptoms (20%) compared with a control group due to higher level of chromium exposure among tannery workers (Were et al., 2014). A cross-sectional study in India reported that leather tannery workers frequently complained of low-back pain (61%), asthma (38%), dermatitis (31%), and chronic bronchitis (14%) in the 12 months prior of the survey (Skóra et al., 2014). The prevalence of asthma among tannery workers was estimated at 5.3% in Pakistan (Shahzad et al., 2006), 3% in Istanbul (Işsever et al., 2007), and 20% in Sudan (Mohamed & Musa, 2017), whereas it varied from 2.2% to 38% among the leather tannery workers in India in older studies (Chandrasekaran et al., 2014; Öry et al., 1997b; Shukla et al., 1991). Most of the studies to date reported that occupational exposure to chromium (organic form or protein bound-form) of the tannery workers increases the risk of dermatitis, ulcers, and respiratory illness (Azom et al., 2012; Febriana et al., 2012a; Hedberg et al., 2018; Islam et al., 2014; Işsever et al., 2007; Rastogi et al., 2008; Skóra et al., 2014; Syed et al., 2010; Yoshinaga et al., 2018).
Tanneries in the Hazaribagh area of Dhaka district have been identified as one of the leading causes of environmental pollution in Dhaka city (Muralidhar et al., 2017; Yoshinaga et al., 2018). A cross-sectional study on the health of 276 tannery workers reported the prevalence of diarrhea (71.7%), blood pressure (52.2%), asthma (49.9%), and skin disease (73.9%) among the tannery workers (Mahamudul Hasan et al., 2016). The Society for Environment and Human Development (SEHD) of Bangladesh conducted a survey on the health of 179 tannery workers from six tanneries and reported that 58% of tannery workers suffered from gastrointestinal problems, 31% from dermatological diseases, 12% from hypertension, and 19% from jaundice (Akhtar & Shimul, 2015). Despite the results from multiple surveys, very few studies have reported the association between specific occupational exposure and health complaints in leather tannery workers. No comprehensive occupational disease registry, ongoing health monitoring, health surveillance, and risk assessment activities have been implemented for the tannery industries in Bangladesh where the sociodemographic and housing conditions in tannery workers are different from other countries. In Bangladesh, the tannery workers mostly inhabit the slum area where poor living conditions further influences their health status, whereas the studies from other developing countries did not mention housing and living conditions (Febriana et al., 2012a; Shahzad et al., 2006). In addition, no study has been conducted in Bangladesh to investigate the association between occupational exposures and health complaints among tannery workers. Therefore, we aimed to investigate the association between length of employment and types of work and health complaints among the tannery workers in Dhaka, Bangladesh. This study will provide new information for occupational health practitioners and policymakers in settings where regulations are less strict, and the economy and health care are very different from the developed world.
Methods
Study Area, Population, and Data Collection
This cross-sectional study was conducted in a cluster of leather tanneries in Hazaribagh of the south-western region of Dhaka, the capital city of Bangladesh (Figure 1). This study was conducted in 10 large tanneries in the Hazaribagh area of Dhaka between May to August 2017. These tanneries were randomly selected through a lottery as representative of the study area. We collected a list of workers from the administrative departments of the 10 selected tanneries, including the number of workers and their work sections (i.e., handling from rawhide to finished leather). From this list, we randomly selected 231 full-time workers at least 16 years of age. All workers were involved in the manufacturing or processing tasks within the tannery. Workers from administrative and other departments, who were not directly involved in the manufacturing or processing tasks, were excluded. All workers were involved in leather tanning processes and had a minimum of 2 years of working experience in tannery work. The respondents were classified into ever smoker and never smoker according to their smoking status. Smoking daily or occasionally or former smokers were classified as ever smoker. Education level was grouped into illiterate (no education), primary education (up to 5 years), secondary education (6–12 years), and graduate (>12 years) education. The housing condition of the participants was classified into kacha house (traditional village house which is made of mud, wood or bamboo, straw, and dry leaves and the floor is made by soil), tin shade house (wall of this house is made by soil or brick, the floor could be soil or brick but the roof is tin), slum house (this house is typically made by various waste materials such as cardboard, tin or plastic; the wall is sometime made of tin or is just a fence where the roof is covered by tin or polythene), or a building. Monthly income was defined as respondent’s personal income from wages and overtime. The study participants were de-identified, and written consent was obtained from all the participants prior to the interview. Ethical approval was obtained from the Northern University Bangladesh human research ethics committee.
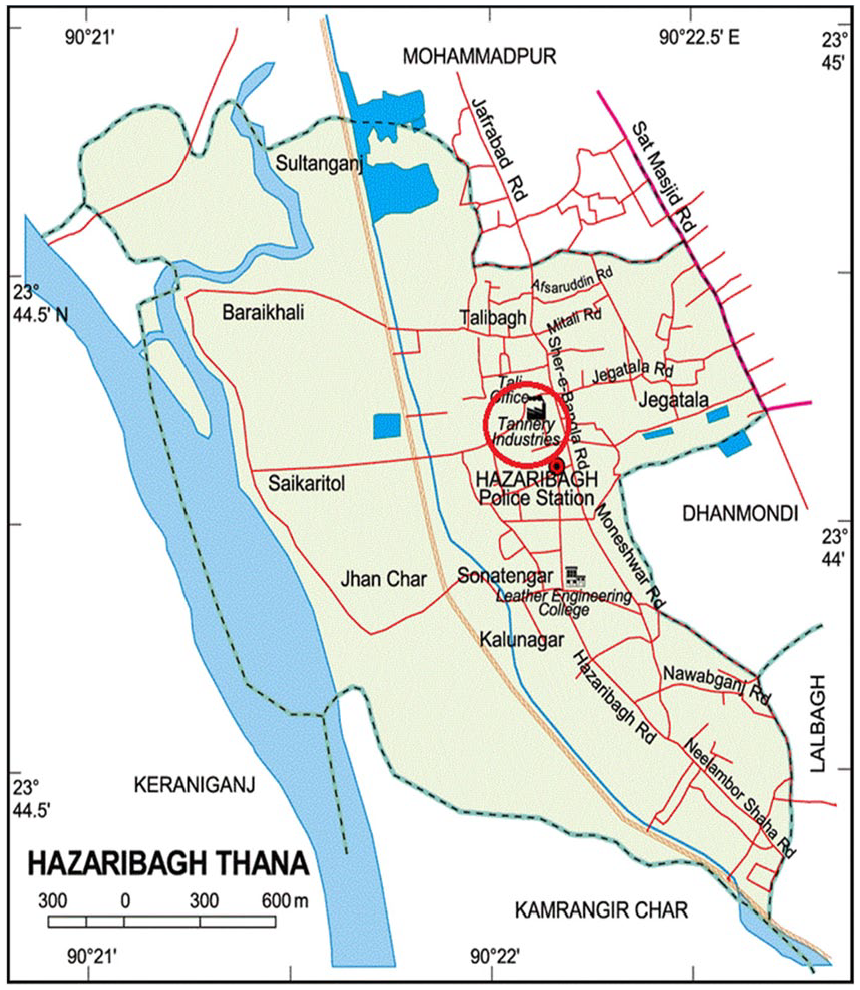
Study area in Hazaribagh Thana, Dhaka Metropolitan City, Bangladesh.
Occupational Exposure and Health-Related Questionnaires
Self-reported information was obtained from participants through face-to-face interviews. A standardized semi-structured questionnaire was used for data collection. The questions on breathing difficulty and the occupational history questions were adapted from the European Community Respiratory Health Survey (ECRHS) (Le Moual et al., 2014) and Tasmanian Longitudinal Health Study (TAHS) (Matheson et al., 2016). The information was collected on demographic characteristics, previous and current job responsibilities, history of injuries at the workplace, knowledge, and use of personal protective equipment (PPE) (including face mask, cap, apron, goggles and shields, gloves, ear plugs, respirators, and safety shoes/boots) and length of employment. The health-related questions asked the participants whether they had any known lung disease or airway disease, history of chest tightness or shortness of breath with wheezing or breathing difficulty, history of jaundice, and any kind of skin disease/itching. The questionnaire was initially developed in English and translated into local (Bengali, national language of Bangladesh) language, and the interview was conducted into the local language using a local interpreter.
Exposure Measures
Self-reported exposure variables were the length of employment and types of work in the tannery industry. The length of employment was defined as total years of work in the tannery industry, and it was collected as a continuous measure. Types of work were defined as all the workers were assigned any one of the four exposure groups that best fit their daily activities (beamhouse, wet finishing, dry finishing, and miscellaneous).
Outcome Measures
Any affirmative response to one or more of the four respiratory questions became “yes” for the “breathing difficulty” variable for the last 12 months. The four respiratory questions were (a) “Has your doctor told you that you have asthma or asthmatic conditions?” (b) “Have you ever suffered from any lung disease or airway disease?” (c) “Do you usually suffer from shortness of breath with wheezy breathing?” and (d) “Do you usually suffer from tightness of chest or difficulty of breathing? Skin disease was identified as an affirmative response to the question, “Have you ever suffered from any skin disease or itching after starting the job at tannery?” History of jaundice was defined as an affirmative response to the questions, “Do you have any history of jaundice after starting the job at tannery?” Injuries at the workplace was defined by a combination of (a) any kind of accident due to mechanical process (knife, handling mechanics, etc.) at the workplace and (b) any kind of accident due to chemical process at the workplace after starting the job at tannery. All the questions have two response options (Yes/No). When the participants answered “Yes,” they were considered or combined (breathing difficulty and injuries at the workplace) as a positive response to the respective outcomes variable.
Statistical Analysis
We used Stata statistical software for Windows, Version 14.2 (Stata Corp, College Station, Texas) for data analysis. Univariate and multivariate logistic regression models were used to investigate the association between length (years) of employment, types of work, and health complaints among the tannery workers (binary variables), in which odds ratio (OR) with 95% confidence intervals (CIs) we calculated. A two-sided p value of ≤.05 was considered to be statistically significant. In the multivariate model, we included age (continuous variable), smoking status (ever smoker/never smoker), education (illiterate, primary, secondary, and graduate), and personal income (converted into USD) as potential confounders. Confounders were selected based on prior literature review and retained in the model if inclusion changed the point estimate by ≥10%. The length (years) of employment was analyzed as a continuous variable. Types of work were classified into four categories: beamhouse, wet finishing, dry finishing, and miscellaneous which was used as a reference group for the analysis.
Results
Table 1 represents the characteristics of the study participants. Of the 231 workers invited to participate, 29 workers changed their job and moved to other tanneries during data collection, 35 declined to be interviewed, leaving 167 workers that were interviewed (response rate = 72%). As expected, most of the participants were male (96%) with a median age of 30 years. The majority of the workers completed primary (43%) or secondary (53%) schooling. The mean length of employment was 6 years, with the monthly average personal income US$125.00. Overall, 65% of the workers were working 8 to 10 hours per day, and the smoking rate was 79%. Approximately 52% of the workers were living in a tin shed house, while 34% of them were living in a slum house.
Demographic and Selected Occupational Characteristics of the Study Participants (n = 167)
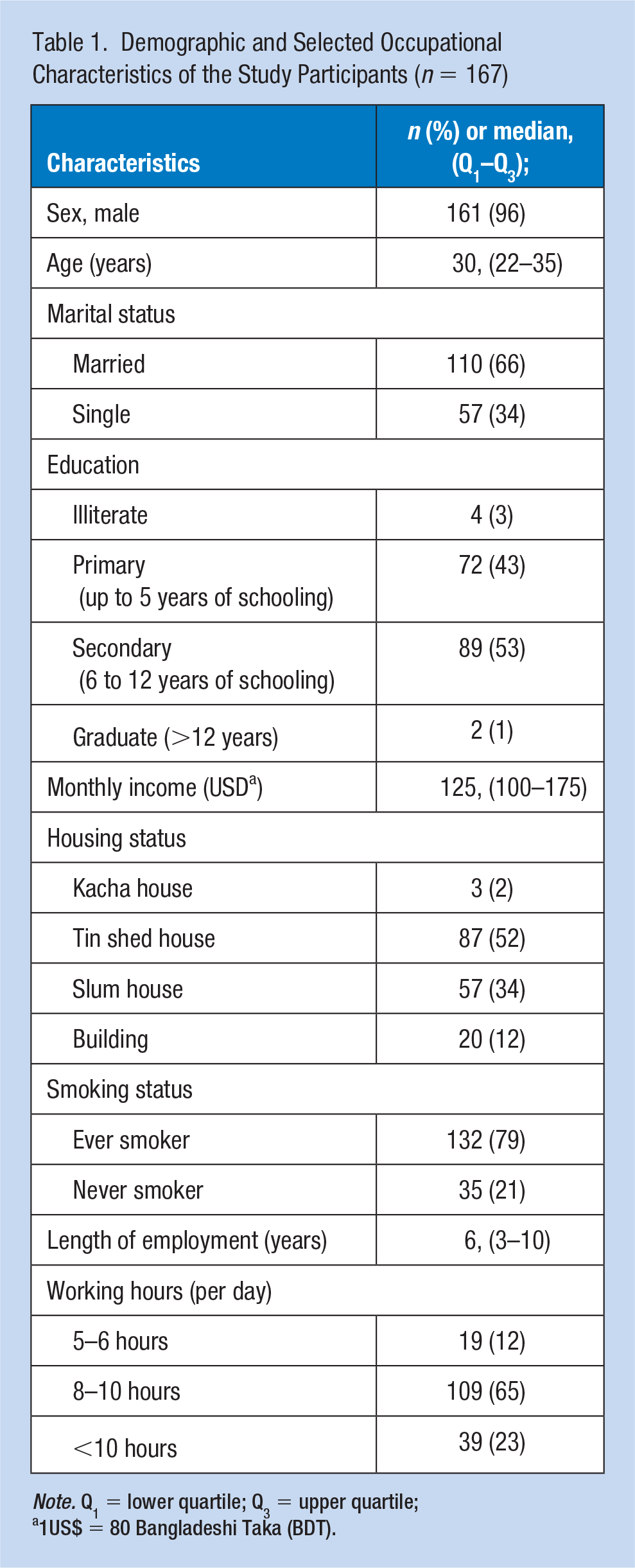
Note. Q1 = lower quartile; Q3 = upper quartile;
1US$ = 80 Bangladeshi Taka (BDT).
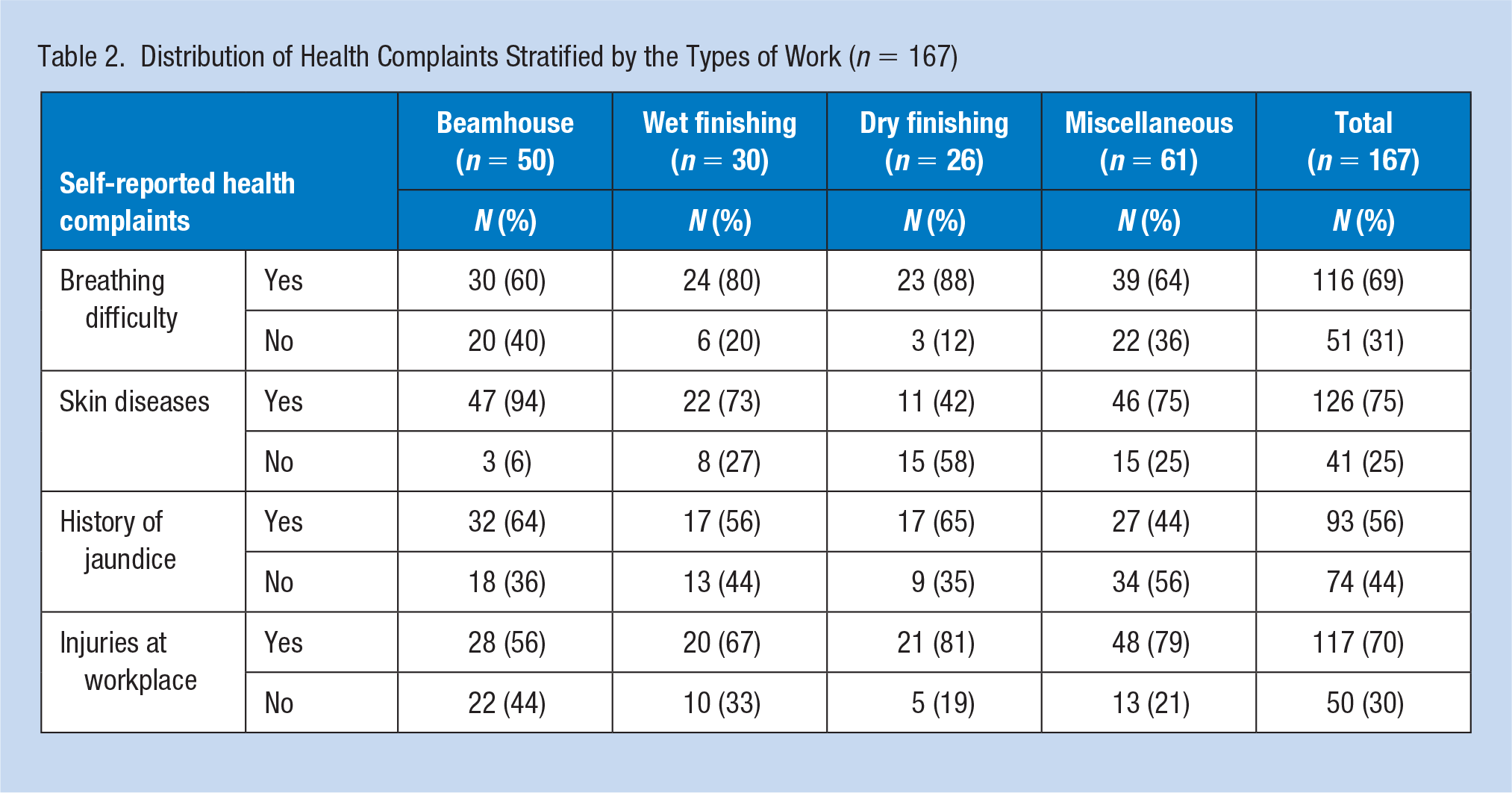
Self-reported health complaints stratified by the types of work are presented in Table 2. The proportions of complaints were similar across the four different categories of types of work. More than 80% of workers reported breathing problems in wet and dry finishing while 60% of them were in the beamhouse. About 94% of workers reported skin disease in the beamhouse and 73% in wet finishing. Almost 70% workers reported their injuries in workplace while around 80% were in dry finishing and miscellaneous group respectively.
Distribution of Health Complaints Stratified by the Types of Work (n = 167)
Both unadjusted and adjusted length of employment were significantly associated with breathing difficulty (Table 3). It was estimated that the odds of breathing difficulty increased by 32% with every 1-year increase in employment length after adjusted for confounders (OR: 1.32, 95% CI, 1.07–1.64). In addition, the unadjusted model of an injuries at the workplace was also associated with length of employment (OR: 1.10, 95% CI: 1.02–1.20) but the association slightly was attenuated when it was adjusted for confounders.
Association Between Length (Years) of Employment and Health Complaints Among the Leather Tannery Workers (n = 167)
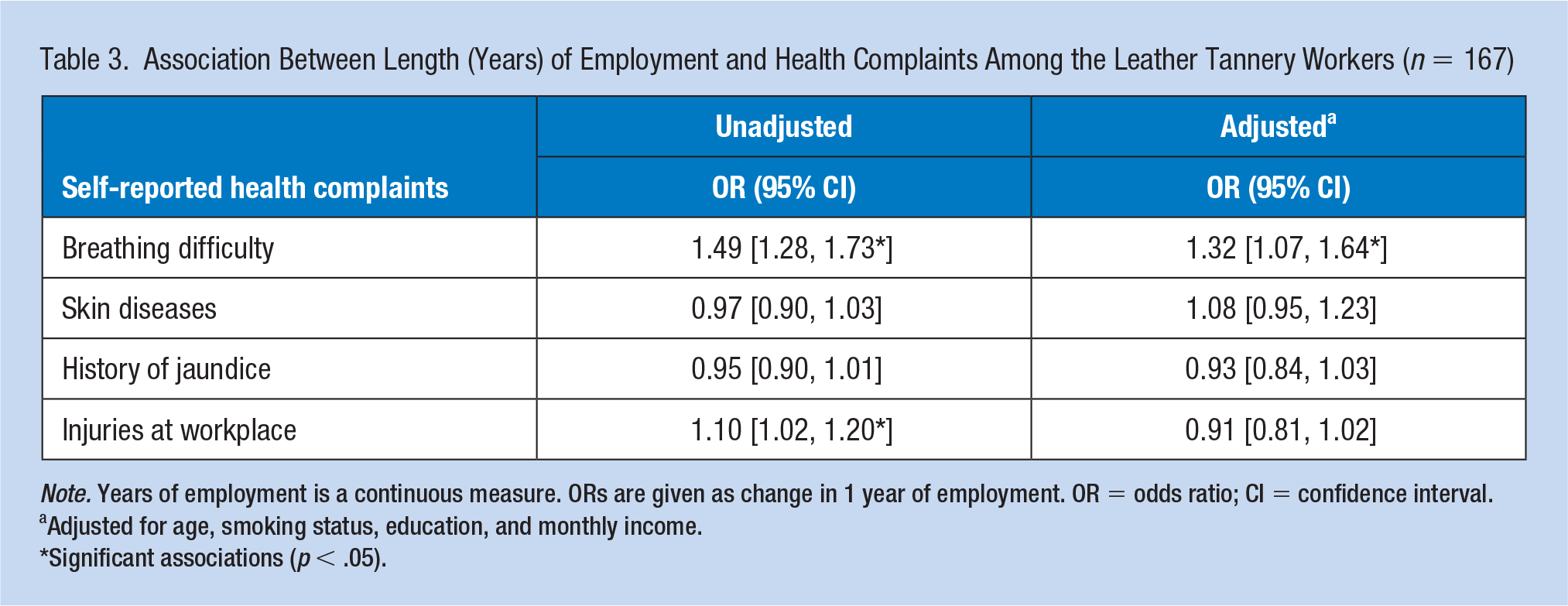
Note. Years of employment is a continuous measure. ORs are given as change in 1 year of employment. OR = odds ratio; CI = confidence interval.
Adjusted for age, smoking status, education, and monthly income.
Significant associations (p < .05).
Table 4 shows the associations between types of work and breathing difficulty and skin diseases. We found an increased risk of breathing difficulty for workers working in wet finishing (OR: 11.75, 95% CI: 2.12–65.10) in the adjusted model and in dry finishing in both unadjusted (OR: 4.32, 95% CI: 1.16–16.05) and adjusted (OR: 13.38, 95% CI: 1.00–181.70) models. We also found a significant association between beamhouse workers and skin disease in both unadjusted (OR: 5.10, 95% CI: 1.38–18.83) and adjusted (OR: 4.36, 95% CI: 1.10–17.32) models. However, workers in the dry finishing observed a negative association for skin disease in both unadjusted and adjusted models.
Association Between Types of Work and Health Complaints Among the Leather Tannery Workers (n = 167)
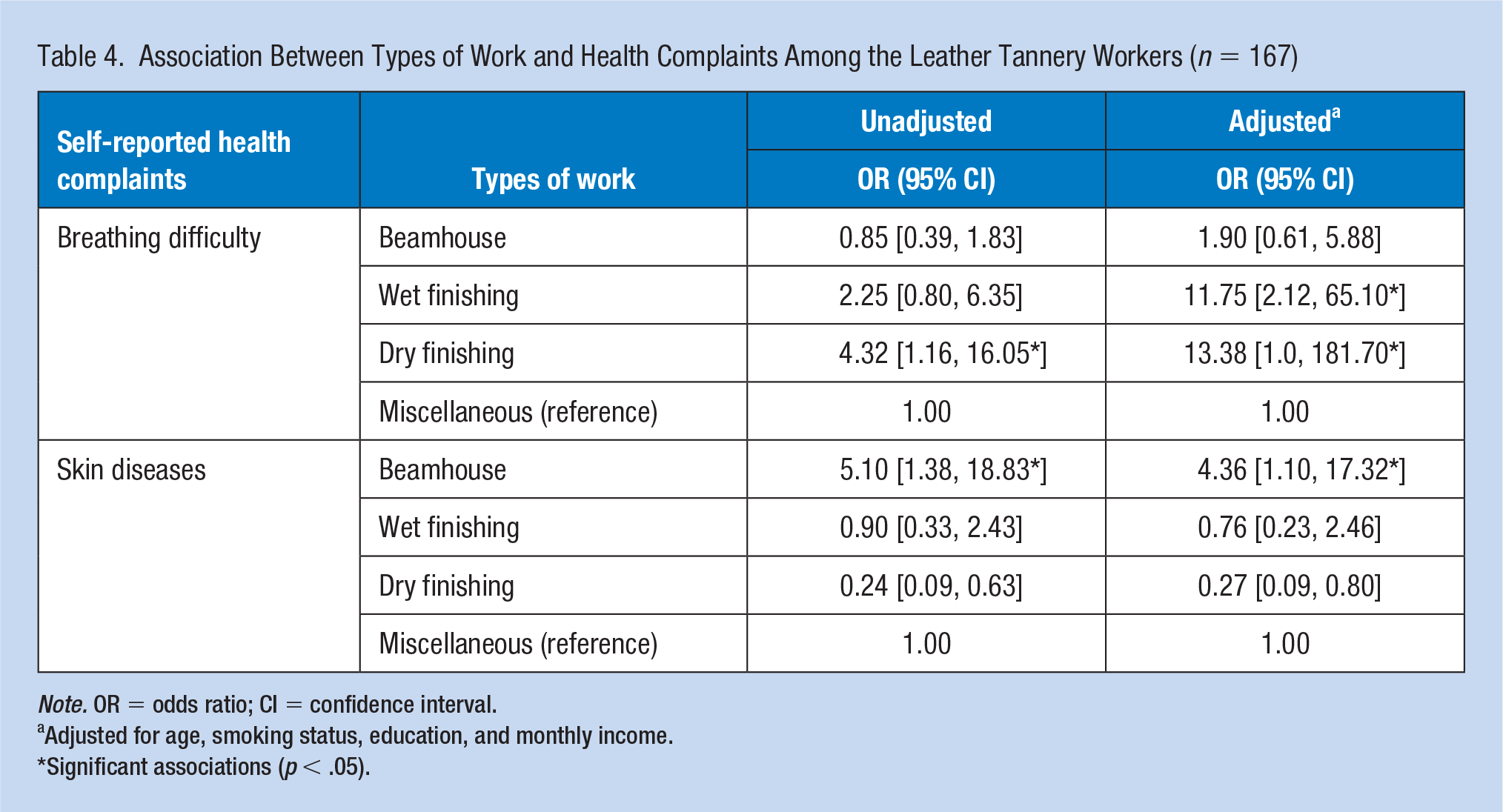
Note. OR = odds ratio; CI = confidence interval.
Adjusted for age, smoking status, education, and monthly income.
Significant associations (p < .05).
Discussion
This is the first study to our knowledge that used tannery workers length of employment and types of nonmechanized or manual tannery work to examine the association with health complaints. We found a higher prevalence of health complaints, including breathing difficulty, skin diseases, jaundice, and history of injuries at the workplace among the tannery workers. We also found that the length of employment and types of work were associated with breathing difficulty. In addition, we identified that beamhouse workers were associated with a higher prevalence of skin diseases.
This survey demonstrated high prevalence of some common health complaints among the tannery workers, including breathing difficulty (69%), skin disease (75%), history of jaundice (56%), and injuries at the workplace (70%).
We found that the length of employment was associated with breathing difficulty. There is evidence from other countries that a longer period of working in a leather tannery was associated with asthma. For example, a cross-sectional study in Ethiopia reported that >20 years of working experience had 2 times more likely to be asthmatic than those who had 1 to 5 years of working experience (Merga, 2018). In further support, a cross-sectional study in Pakistan reported that 8 years and 13 years of works in the leather tannery increased the odds of adult asthma by 2.26-fold and 3.67-fold, respectively (Shahzad et al., 2006). In addition, we also found the association between types of work and the occurrence of breathing difficulty. Tannery workers working in the wet finishing and dry finishing had an 11.75 times and 13.38 times higher risk of developing breathing difficulty, respectively, than those who were worked in miscellaneous group. None of these studies examine the effect of working in specific areas or the types of work in the tannery and the health complaints. However, a cross-sectional study in Southeast Ethiopia reported that the odds of developing respiratory symptoms was 3.37 times higher among tannery workers than unexposed workers (Dalju et al., 2019). A previous study from India also found that lifting 10 to 20 kg or >20 kg was associated with asthma (OR = 2.36 and 2.56) and chronic bronchitis (OR = 2.11 and 1.57) (Öry et al., 1997b). This difference may be due to the presence of differential misclassification caused by self-reported exposure in our study, assessment methods, sample size, and workplace health and safety cultures and practice across the countries. Alternatively, workers in the wet and dry finishing were engaged in coloring, coating, polishing, drying, and ironing which had direct contact to dust. These dusts contain heavy metals (chromium [III], copper, lead, zinc, cadmium, iron, and nickel), and prolonged exposure to metal dust are found to be linked with respiratory diseases (Sarwar et al., 2018).
We observed that types of work were associated with skin diseases, but the duration of the length of employment did not show any significant association. Our finding that working in beamhouse was associated with skin diseases has not been reported in any previous studies. The workers in the beamhouse engaged in unhairing, fleshing, soaking, trimming, picking of raw skins and hides, which generates organic particulates that may cause dermatitis (Buzea et al., 2007). On the other hand, the chemicals used in leather production change the structure of the skins and hides and may have a similar effect on the worker’s skin. Beamhouse workers who exposed to many of those chemicals for prolonged periods are at higher risk of developing occupational dermatitis (Febriana et al., 2012a). A study from India reported that exposure to chemical agents was associated with a 2.6-fold increase in the risk of skin disease among the leather tannery workers (Öry et al., 1997b). Workers in the dry finishing reported a negative association with skin diseases. It might be due to the self-reported outcomes that are more prone to recall bias.
We did not find an association between length of employment and types of work with a history of jaundice. Although 93% of participants reported a history of jaundice, this may be due to exposure to chromium in the tannery work, which may be related to hepatic impairment (Khan et al., 2013). Experiencing an injury at the workplace was also associated with length of employment, but it was attenuated after controlling the confounders. A comparison of this result with different studies is difficult because of the variations in the study design, sampling technique, and exposure assessment.
One strength of this study is that we were able to collect data from the workers who were directly handling hazardous materials in the tannery industry. We also conducted several statistical analyses adjusted for a range of confounding variables to minimize the chance of residual confounders and biases. Although the tanneries were relocated to Savar, Dhaka, after we collected our data, this study demonstrated the health consequences in the Hazaribagh area that may be applicable to the broader Hazaribagh residential community, which is situated in the center of the Capital. Furthermore, repeating this study in the new location could allow evaluation of the improvements of the new site on the workers’ health. Despite these strengths, we have several limitations, including a small samples size. We used self-reported information to assess the exposure and health status, which may be prone to recall and misclassification bias. Another possible bias in our study is selection or nonresponse bias or healthy volunteer bias caused by the participants choosing to participate in the study. Participants who self-select to participate in the study generally have better health status than those who do not. Unfortunately, we were unable to exclude this type of bias in this cross-sectional study, but we adjusted our statistical analysis for several factors to reduce the chance of recall bias. Therefore, we suggest our results should be viewed as hypothesis-generating rather than proof that these exposures are causal; hence, a replication of this study in the larger cohort with follow-up in this high-risk population is required.
Conclusion
We have demonstrated an association between length of employment and types of work with breathing difficulties and skin diseases among the tannery workers. Further research in a larger cohort is needed using more objective measures to evaluate the occupational nature of the diseases.
Implications for Occupational Health Practice
Leather tannery workers in nonmechanized tanneries are exposed to various chemicals at the workplace. Some health effects may be immediate, such as rhinitis, muscle pain, headache, jaundice, an injuries at the workplace, but others take time to develop, for example, skin disease and breathing difficulties. In Bangladesh, the Occupational Health Service is maintained by the Department of Inspection for Factories and Establishment (DIFE) under the Bangladesh Labour Act (2006) along with other existing regulations (details in online supplement). The working conditions in Bangladesh depend on the environment and workplaces where the tannery workers work but are very poor in general. This is partly due to the specific contractual situation of many tanneries. Most of the tanneries hire the workers on a contract basis where the workers are hired by a company but work within the premises of one or more “host companies.” The employer, that is, the tannery, is responsible for the health and safety of their cleaning workers but is not in control of the environment in which they work in the host company. Because tannery work comprises a wide variety of tasks, workers are potentially exposed to a wide variety of chemical, biological, physical, and psychosocial risks.
The tanneries have been relocated to improve environmental conditions; however, it remains controversial to what extent this relocation will contribute to environmental sustainability and improvement in occupational health of the tannery workers (Hoque & Clarke, 2013). There is a widespread assumption in the government circles that constructing a central Effluent Treatment Plant (ETP) in Savar will resolve the environmental and health issues related to the Hazaribagh tanneries (Human Rights Watch, 2012). However, Human Rights Watch recognized that a central ETP would do nothing to resolve most of the problems such as poor occupational health and safety conditions, hazardous child labor, and the existing industrial pollution of Hazaribagh (Human Rights Watch, 2012). They argued that without closely monitoring and regulating the tanneries in addition to rigorous enforcement of the country’s labor, and environmental laws by the government, there is no incentive for the tanneries to reduce their pollution load by adopting such measures (Human Rights Watch, 2012).
Early interventions in the form of education and training of the workers and employers, by involving public and occupational health authorities as well as worker advocates, may reduce the risk of occupational exposure. Even in the absence of adequate occupational health care facilities in the workplace, public health professionals can take steps to improve the health outcomes for the tannery workers. Greater attention should be committed to employer education, workers’ education, and primary health care. Many employers overlook the effect of prolonged chemical exposure on tannery workers in spite of requirements to monitor their health. Health education is another option to advise employers about risk in their tannery as well as the steps required to mitigate the risk. Moreover, a large proportion of workers do not use PPE during handling tannery materials or chemicals because of lack of availability of PPE or lack of awareness about PPE. Workers’ education about smoking cessation and the importance of hygiene prior to eating and leaving work as well as how PPE and work practice can reduce exposure could minimize the risk of injuries or illnesses in the tannery industry. Health monitoring in the tannery industry together with exposure control measures are required to prevent adverse health impacts.
Applying Research to Occupational Health Practice
Leather tannery workers in Bangladesh and other developing countries face a range of health and safety risks at the workplace due to exposure to hazardous materials and processes during tanning of hides and skins. Chemicals used in the tanning process are potential irritants and sensitizers to the workers. Besides that, infection is a constant hazard because manual handling of raw materials in tannery results in exposure to a high concentration of pathogens. Given the high percentage of tannery workers who reported breathing difficulties, skin diseases, jaundice, and injuries related to accidents at the workplace, safety training, and use of PPE (e.g., mask, cap, apron, goggles, gloves, gum boots) should be introduced. This will help to raise awareness of proper techniques to reduce the risk of occupational exposure at the leather tannery. Based on the results from this pilot study, we recommend changing the work tasks and regular health surveillance in this high-risk group, which could prevent further health complications in developing countries.
Supplemental Material
OSH_online_supplementary – Supplemental material for Factors Associated With Health Complaints Among Leather Tannery Workers in Bangladesh
Supplemental material, OSH_online_supplementary for Factors Associated With Health Complaints Among Leather Tannery Workers in Bangladesh by Golam Rabbani, Baki Billah, Anil Giri, Sarder M. Hossain, Ahmmad I. Ibne Mahmud, Bilkis Banu, Ulfat Ara and Sheikh M. Alif in Workplace Health & Safety
Footnotes
Acknowledgements
We acknowledged the study participants and management of the Anower Tannery (Pvt.) Ltd., Bay Tanneries Ltd., and Bengal Leather Complex Ltd. for their assistance to collect the data. We especially thank Northern University Bangladesh, Dhaka, Bangladesh for their continuous support and guidance to complete the study.
Author Contributions
All authors have contributions to the conception and design of the work, or analysis and interpretation of data for the work and drafting the article or revising it critically for important intellectual content. Finally, we approved the manuscript for publication and ensured that any questions related to the accuracy or integrity of the work were appropriately investigated and resolved.
Declaration of Conflicting Interestst
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
Golam Rabbani is a deputy director at Bangladesh Betar (radio). He is a MPH graduate from University of Melbourne and research focused on respiratory health.
Baki Billah works as a senior lecturer at the School of Public Health and Preventive Medicine of Monash University. His published articles have reached to 5000 reads and 1050 citations (as of Oct 2017), and he has received the highest cited award from the European Society of Cardiology.
Anil Giri is working as assistant professor of School of Health and Allied Sciences at Pokhara University, Nepal. His area of research is occupational health, disease epidemiology, and drug formulation.
Sarder M. Hossain is working as professor and head in the Department of Public Health, Northern University Bangladesh. His area of research focuses on nutrition, emerging diseases (communicable and noncommunicable), environmental health, maternal health, and child health.
Ahmmad I. Ibne Mahmud is currently working as CEO & technical lead at Raddron Development and Analytics. His area of research focuses on environmental health and data science.
Bilkis Banu is presently the PhD scholar in Heidelberg University, Germany, and working as assistant professor in the department of Public Health, Northern University Bangladesh. Her research expertises are in the area of noncommunicable diseases, health education, health promotion, maternal health, and child health.
Ulfat Ara is now working as lecturer in the department of Public Health, Northern University Bangladesh. Her research expertises are in the area of oral health, emerging health problems, maternal health, and child health.
Sheikh M. Alif is a postdoctoral researcher working in the fields of respiratory and occupational health. He has a strong track record of research in the fields of respiratory and occupational health, epidemiology, and biostatistics. To date, he has published 30 refereed journal articles. He is working in collaboration with European Community Respiratory Health Survery (ECRHS), and Global Burden of Disease (GBD) Chronic respiratory group based in University of Washington, USA. He is currently working in several projects including cancer and mortality in coal mine workers in Queensland, Australia and silicosis disease registry in Victoria, Australia.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.