
Abstract
Background:
The increased contamination of illicit drugs with fentanyl in the United States drug market has contributed to escalating mortality from drug overdose. Leisure and hospitality service industry workers are encountering opioid-triggered overdoses in their workplaces, such as restaurants and bars. Consequently, this increases the need for overdose education and naloxone distribution (OEND) training, which has been limited. We aimed to describe the experiences among service industry workers encountering an overdose in their workplace.
Methods:
We conducted in-depth qualitative interviews with service industry workers in Little Five Points (L5P), Atlanta, between October 2019 and April 2020 and triangulated methods with participant observations and fieldwork. Purposive criterion sampling methods were applied to recruit from different establishments in the L5P commercial district, which comprised restaurants, bars, retail shops, and theaters. After an initial seed sample was identified by engaging key stakeholders during fieldwork (business owners, managers, and the business association), a snowball sample followed for a final sample of N = 15. To contextualize the local population of harm reduction workers, people who use drugs and/or obtain safer drug consumption supplies in L5P (sterile syringes, safer using kits, naloxone), and service industry workers and their customers in L5P, the first author volunteered with an Atlanta syringe services program from October 2019 to April 2020. The first author conducted participant observations during the syringe exchange program and field notes were taken during observation (44 hours). This engagement ensured a rich, thick description. We used a pragmatic approach to thematic data analysis for this study. Data were analyzed iteratively and inductively from interviews and observations. Two independent researchers reviewed transcripts to identify passages in the data related to the question of interest. The passages were contextualized within the full data set independently to understand the relationships in developing a theory of what was commonly occurring across participants’ experiences, and these relationships led to emerging salient themes regarding encountering an opioid overdose at work.
Results:
One salient theme related to overdose response emerged with the service industry workers included fear of negative consequences of overdose response, specifically, fear of disease transmission from artifacts of drug use and overdose response, including the spread of blood-borne disease, violence, and exposure to unintentional overdose. When discussing drug use, participants’ beliefs about the potential for personal danger from drug use artifacts (syringes and discarded drugs) and violence were identified as barriers to opioid overdose responses.
Conclusions/Implications for Occupational Health Practice:
Our findings provide valuable insights for tailoring OEND training for service industry workers to confront fears associated with opioid overdose response in their places of work to decrease mortality from the opioid epidemic. Harm reduction approaches need to be sensitive to the places in which overdose occurs and who the overdose responder is likely to be, which requires appropriately tailoring OEND training for service industry workers.
Background
The opioid epidemic is a significant public health concern in the United States. In 2021, more than 100,000 Americans died of drug overdose—of which 70% were opioid-related (Centers for Disease Control and Prevention [CDC], 2021). Introducing fentanyl to the illicit drug supply in the United States has contributed to a surge in mortality from opioid overdose (Lockwood et al., 2021). Illicit drugs contaminated with fentanyl include stimulants such as cocaine, methamphetamines, and illicitly manufactured pills (Ciccarone, 2021).
Consumption of these drugs puts people who are opioid naïve at increased risk of an opioid-induced overdose (Hughto et al., 2022). To combat the increasing mortality, standing orders for the opioid antagonist, naloxone, have been implemented in all 50 U.S. states (Herbert et al., 2020; Razaghizad et al., 2021). Naloxone, which is now available without a prescription (Davis, 2020), was found to be crucial in preventing opioid fatalities in an umbrella review of systematic reviews that included studies conducted in the United States, Portugal, and the United Kingdom (Razaghizad et al., 2021). Healthcare providers (Jawa et al., 2020), pharmacists (Palmer et al., 2017), first responders (Crocker et al., 2019), healthcare professional students (Bachyrycz et al., 2019; Halmo et al., 2021; Hargraves et al., 2019), law enforcement (Dahlem et al., 2017), people who use drugs (Piper et al., 2008), and their friends and families (Taylor et al., 2019) have been targeted for overdose education and naloxone distribution (OEND) training. However, the widespread opioid epidemic continues to affect communities—and laypeople are more likely than ever to encounter an opioid overdose in public settings where they could be potential first responders.
In urban settings, overdoses are more likely to occur in public settings, including restaurants, bars, and parked cars (Allen et al., 2020; Treitler et al., 2022). Service industry workers employed in these settings are uniquely positioned to reduce preventable deaths by opioid-related overdose (Febres-Cordero & Smith, 2022 ). There are 16.7 million leisure and hospitality workers in the service-providing industry, including those employed in food services such as restaurants and bars (U.S. Bureau of Labour Statistics, 2021, 2022). These workers are well-positioned to be the first people to respond to opioid overdoses.
Little research has been done to inform how service industry workers who encounter an overdose in community settings perceive overdose in public spaces (Allen et al., 2020; Febres-Cordero & Smith, 2022 ; Wolfson-Stofko et al., 2018). This study aimed to describe the experiences of service industry workers who encountered an overdose in their place of work. These insights are invaluable when tailoring OEND training for service industry workers in communities to respond to opioid overdoses to decrease mortality from the opioid epidemic.
Methods
We conducted in-depth qualitative interviews with service industry workers (N = 15) in Little Five Points, Atlanta, and triangulated methods with participant observations and fieldwork recorded in field notes.
In the commercial district of Little Five Points (L5P), Atlanta, the Little Five Points Pharmacy, in collaboration with the Georgia Department of Public Health (GDPH), the Atlanta Harm Reduction Coalition (AHRC), and Georgia Overdose Prevention, distributed more than 1,000 units of naloxone for free to residents and community members, including service workers in L5P from 2014 (year standing orders were implemented in Georgia) to 2020 at The Little Five Points Pharmacy, during syringe exchange in Little Five Points, and at OEND training in restaurants and bars, throughout the commercial district conducted by a public health nurse and the local pharmacist (Febres-Cordero, Sherman, et al., 2021; Febres-Cordero & Smith, 2022; Georgia Pharmacy Foundation, 2020).
Purposive criterion sampling methods (van Manen, 2007) were applied to recruit from different establishments in the L5P commercial district, which comprised restaurants, bars, retail shops, and theaters. One question identified participants, “Have you encountered an overdose while working in Little Five Points?” During fieldwork, the PI asked workers in Little Five Points this one question. Anyone who affirmed working at businesses in L5P was considered a service industry worker. Inclusion criteria were (a) encountered an overdose at work in any establishment in L5P and (b) were over 18 years of age. After the PI identified an initial seed sample by engaging key stakeholders during fieldwork (business owners, managers, and the business association), a snowball sample followed (Patton, 2002) for a final sample of N = 15. Participants recruited in the snowball sample were told by seed participants that the PI was recruiting people who had encountered an overdose while working in Little Five Points. The seed participants shared the PI’s contact information with potential participants. When potential participants contacted the PI, they were screened for inclusion in the study.
Data Collection
To contextualize the local population of harm reduction workers, people who use drugs and/or obtain safer drug consumption supplies in L5P (sterile syringes, safer using kits, naloxone), and service industry workers and their customers in L5P, the first author volunteered with an Atlanta syringe services program from October 2019 to April 2020. The first author conducted participant observations during the syringe exchange program (SSP) (Fetterman, 1998; Hammersley, 1995; Spradley, 1980), and field notes were taken when observing the SSP (44 hours). This engagement ensured a rich, thick description (Merriam, 2009). Thick description aims to provide not only individual interview data but also a detailed description of the setting and participants to contextualize cultural and social relationships, allowing for the possibility of transferability to similar settings (Merriam, 2009).
Open-ended, individual interviews (Maxwell, 1996; Neergaard et al., 2009; Sandelowski, 2000, 2010) were conducted by the first author at a place and time of the participants’ choice. Data collection occurred between October 2019 and April 2020. The first author used a semi-structured, open-ended interview guide during individual interviews. The interview guide included 13 questions, with the primary question being: Can you tell me the story of your most memorable experience of encountering an overdose in L5P? Interviews lasted 50 minutes on average. Participants were compensated for their time with a 30-dollar gift card to a local grocery store.
The demographic form also asked participants to describe any other information that would be useful to gain a better understanding of them as individuals. This data and data from interviews informed the narrative participants’ descriptions (Table 1).
Narrative Description of the Participants’ Demographic Characteristics
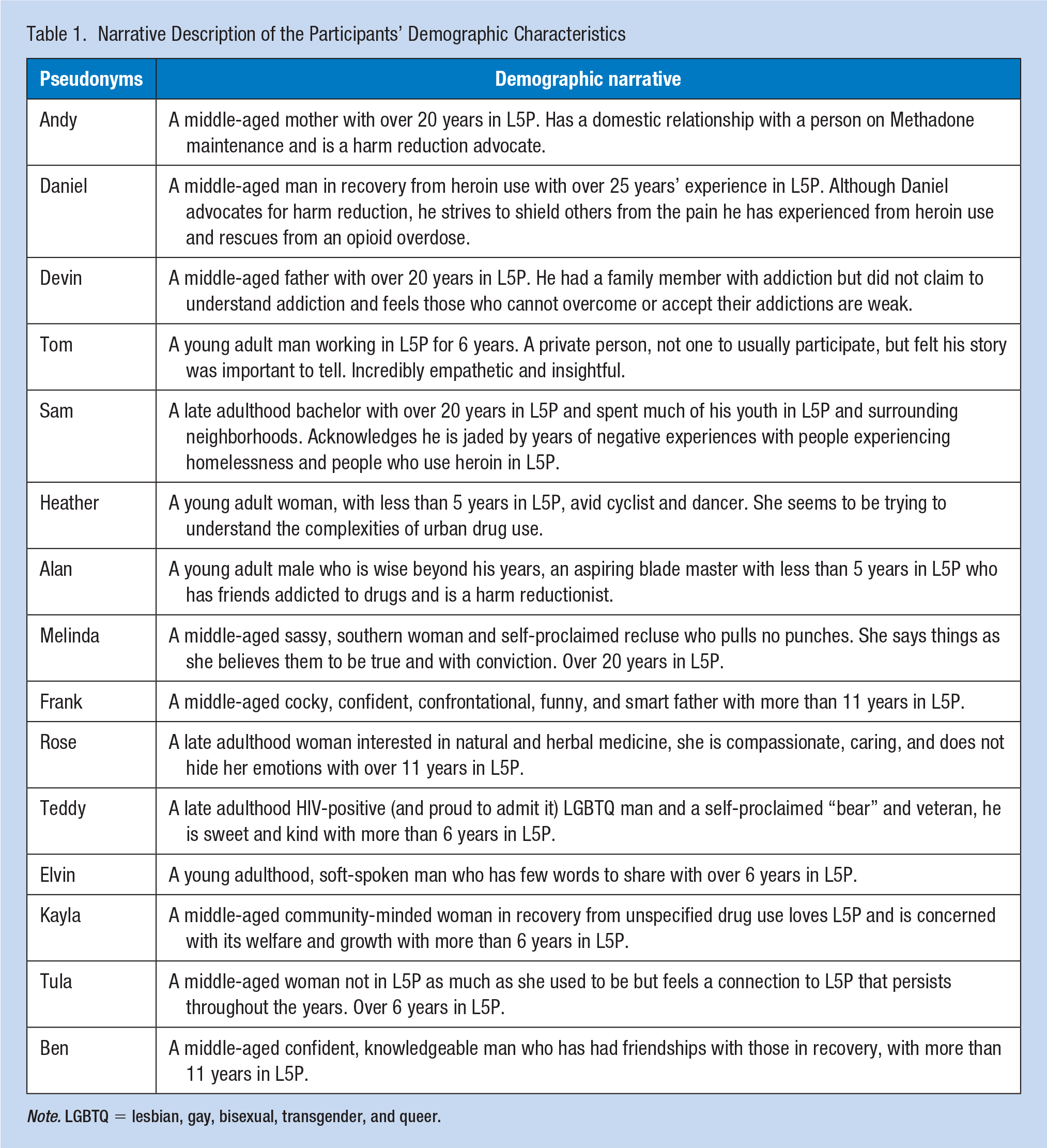
Note. LGBTQ = lesbian, gay, bisexual, transgender, and queer.
The Emory University Institutional Review Board (IRB) approved all data collection protocols (IRB00115738). Informed verbal consent was obtained to minimize the possibility of participant identification.
Data Analysis
We used a pragmatic approach to thematic data analysis for this study (Neergaard et al., 2009). Data were analyzed iteratively and inductively from interviews and observations. Observation and field notes were taken during and after individual interviews and during and after participant observations and fieldwork in L5P with pen and paper and then were transcribed to word processing software by the first author until data saturation was achieved. Two independent researchers reviewed transcripts to identify passages in the data related to the question of interest. The passages were contextualized within the full data set independently to understand the relationships in developing a theory of what was commonly occurring across participants’ experiences, and these relationships led to emerging salient themes regarding encountering an opioid overdose at work (Maxwell, 1996).
Anonymization
Pseudonyms have replaced the names of the service industry workers who shared their experiences to protect their privacy (Table 1). We present text (data) taken from interview transcripts or observational field notes, and phrases such as “so,” “like,” and “you know” and repetitions have been deleted. We made every effort to maintain the intended tone.
Results
Participant Characteristics
The study participants (n = 15) were predominately White (93%) and male (60%), with a mean age of 43 years (range, 19–66 years). Most had some college education or were college graduates (80%) and worked in the L5P for 5 years or more (87%). Many in this sample acknowledged having intimate knowledge of drug and opioid use through personal friends, family, or work exposures (93%). During the interviews, more than half indicated that they had lived near L5P in the past or present.
Fear of Negative Consequences of Overdose Response
One salient theme related to overdose response emerged with the service industry workers included fear of negative consequences of overdose response, specifically fear of disease transmission from artifacts of drug use and overdose response, including the spread of blood-borne disease, violence, and exposure to unintentional overdose. When discussing drug use, participants’ beliefs about the potential for personal danger from drug use artifacts (syringes and discarded drugs) were identified as barriers to opioid overdose responses. Syringes were the most common artifacts of drug use in L5P. Discovered by service industry workers or recalled in neighborhood folklore, participants noted artifacts revealing that injection drug use had occurred in the area. Many fears were revealed when speaking about artifacts. Fears and stigma were coupled in many of these instances when recalling found artifacts.
Disease Transmission
Two service industry workers shared stories of collecting discarded syringes and neighbors coming to complain that they found discarded needles on their properties in the surrounding residential neighborhoods. At the root of the conversation about discarded syringes was a fear of disease transmission. “Kayla” shared, “But we’ve definitely found needles and that kind of thing. And that’s all around Little Five Points. I’ll see needles just walking around, which is really scary.” “Kayla” had worked in L5P for more than 6 years and was an active participant in community events. Just the sight of used syringes created fear for her.
In our study, no one reported being personally stuck with a used needle. Still, there was one story of a needlestick injury while taking out the daily garbage that resonated with the participant who shared this information leaving him to consider syringe disposal boxes for the business, “I think it’s a great idea (syringe disposal boxes) because we’ve had an experience where an employee got nicked with a needle in the garbage.” “Sam” had an employee who was stuck by a syringe. This experience left him open to the idea of having a sharps container in the business bathroom. However, the other 14 participants did not agree. When asked if they thought syringe disposal boxes would be of benefit in their workplace restrooms, all participants, except
The syringe used for injecting drugs may be one of U.S. history’s most stigmatized pieces of paraphernalia. People fear the syringe used for injecting drugs. These fears continue to act as a barrier not only to overdose rescue but to harm reduction efforts. Although the participants spoke of seeing and finding discarded syringes, the PI joined the business association on a neighborhood clean-up day and was able to find only one discarded syringe. We found by contextualizing the data in a historical context, these fears may be conflated due to the severe historical stigma surrounding the syringe for drug use. Fears surrounding syringes were only one of many involving the transmission of disease.
Rescue Breathing
Participants had differing attitudes about and willingness to perform rescue breathing. While 13 participants did not hesitate to say they would provide rescue breathing, if necessary, two participants believed that people who overdose from opioid use are unworthy of rescue breathing and infected with diseases that may be transmitted through rescue breathing. “Devin” shared again, acknowledging his socially undesirable views as “asshole tendencies”: . . . and that’s where my asshole tendencies come in . . . I literally would stand over them and watch them die before giving them mouth to mouth. Because I don’t know what diseases they might have. I have more to lose in life at that moment than they do. And I’m not going to risk myself to save someone who, unfortunately, I see as weak.
“Devin” was not afraid to make socially undesirable comments. He called these his “asshole tendencies.” It is important that people like “Devin” are included in studies such as this one, as these are the fears that must be addressed to make people ready to respond to an overdose in a public setting. The use of rescue breathing as an overdose response strategy is challenging, as it is a practice that requires substantial time expenditure to teach adequately and opportunities for hands-on training. However, the four participants interviewed during COVID-19 still acknowledged the importance of providing rescue breathing, even during a pandemic. In addition to fears of disease transmission, participants also feared unintentional overdose from unintended drug exposure.
Unintentional Overdose: Fentanyl and Found Drugs
People do not know what drugs they may encounter when rescuing someone from an overdose. Fears of fentanyl were identified among participants of the study and people encountered during syringe service observations. Interviewees stated the belief in the danger of unintentional overdose from contact with drug residue by providing interventions that require close physical contact with someone who is overdosing or from drugs left behind after an overdose. “Frank” recalls. “He had left it in the restroom, like a sack of dope. We just flushed it immediately. I just made a biohazard scene of the trash can.” “Frank” found drugs after an overdose rescue and disposed of the drugs in the only way that felt safe at that moment and then proceeded to remove the trash can with the assumption that other dangerous paraphernalia may have been left on the scene as well. People in L5P are aware of the danger of fentanyl as they have personal experience with the drug.
Many interviewed for this study had lost someone or knew of someone who died from a heroin overdose or overdose where fentanyl was later found in other drugs (namely cocaine). Following data collection and analysis, a young man who frequented L5P died of a drug-related death rumored throughout L5P from cocaine laced with fentanyl. Another concern voiced by participants of syringe exchange and participants of the study was the fear of perceived violence of people who use drugs, especially after naloxone administration, another barrier to response to an overdose.
Fear of Perceived Violence
Four of the 15 participants assumed that people who use drugs are violent. The fear of violence by those who use drugs is a barrier to opioid overdose rescue and a clear sign of stigma. Nonetheless, participants reported fear of violence frequently during interviews and needed to be addressed to confront stereotypes of people who use drugs. Participants’ inability to judge whether someone has violent tendencies also supports how the possibility of violence keeps people from intervening with those they may consider at risk for an overdose. “Kayla” exemplified this point of view, “I didn’t have proof. But it was my gut. Like, I knew. The guy he was talking to looked like he was on heroin and was slow drinking. And who knows how dangerous that particular person is?” “Kayla” was cautious when encountering someone she suspected of using heroin. Her caution came from a place of fear of people who use drugs. The people who work in L5P are aware of the many dangers of the urban milieu. For the people who work in the area, there is a need to be street-smart. The belief that these threats are linked to people who use drugs demonstrates the persistence of stereotypes about the violent drug user.
Discussion
International researchers from Canada, the United Kingdom, and Australia have identified that encountering people who have overdosed in public spaces is not a new phenomenon and that there is a need for safer consumption environments (Dovey et al., 2001; Parkin & Coomber, 2011; Rhodes et al., 2006, 2007); however, with the current opioid epidemic and its increasing reach into communities, new knowledge is needed to understand how we can support those who may become “default” first responders. This study identified one salient theme to responding to opioid overdoses, fear of negative consequences from rescuing someone experiencing an overdose. Below, we discuss ways to address this prominent barrier and note implications for future intervention to facilitate opioid overdose rescue in service industry settings.
It is estimated that around 2,000 individuals acquire a needlestick injury in the United States from improperly disposed of needles in public spaces (Jason, 2013). However, community-acquired needlesticks are considered relatively rare, with an associated annual rate of 0.7 per 100,000 U.S. citizens (Jason, 2013). As seen in among our sample, there is an increasing concern of needlestick injuries despite the evidence to the contrary. Interventions such as syringe service programs and overdose prevention sites establish safe places where people who inject drugs can dispose of used syringes, decreasing improper syringe disposal (Levine et al., 2019). There are many areas across the United States where no such services exist to facilitate proper syringe disposal. One way to address this challenge is placing syringe disposal boxes in neighborhoods where injection drug use is known to occur. One community where syringe disposal boxes were set up showed them to be a promising solution to address the problem of improper syringe disposal (Roth et al., 2021). However, as our results have shown, there are still many barriers to overcome when advocating for syringe disposal boxes, namely deconstructing the myth that providing such a service would enable and welcome drug use in neighborhoods and business restrooms. Thus, no syringe disposal boxes exist in L5P.
As seen in our results, laypeople commonly report fear of transmission of communicable diseases and regurgitation of bodily fluids as a barrier to rescue breathing in response to witnessing an opioid overdose (Dezfulian et al., 2021). The COVID-19 pandemic contributed to this fear. One strategy to increase willingness to engage in rescue breathing in the face of an opioid overdose is using barrier devices or masks that reduce or prevent direct contact between the respondent and the person experiencing an overdose (Dezfulian et al., 2021). In addition, the rise in fentanyl-related overdoses has led to reports of fear of overdose among emergency responders (Persaud & Jennings, 2020).
Participants of this study voiced concerns surrounding unintentional overdose from fentanyl exposure. While some first responders report overdoses caused by fentanyl, all such reports have been refuted by medical experts (Feldman & Weston, 2022). In addition, the American College of Medical Toxicology, the American Academy of Clinical Toxicology, and the National Occupational Safety and Health have all asserted that fentanyl overdose from incidental skin contact is impossible (CDC, 2020; Moss et al., 2018). Despite this, 80% of first respondents surveyed in New York reported believing that “briefly touching fentanyl could be deadly” (Persaud & Jennings, 2020), and such beliefs may influence first responders’ willingness to engage in rescue breathing and other lifesaving activities (Winograd et al., 2020). Dissemination of medically accurate information on fentanyl contact among first responders and those who might respond to an overdose is necessary (Feldman & Weston, 2022; Winograd et al., 2020). Many programs in the United States provide safe disposal of prescription opioids/other controlled substances (Foy, 2020; Rural Health Information Hub, n.d.; US Department of Justice (USDJ, n.d.). These allow individuals and community members to return unused pharmaceutical medications responsibly and safely.
This study has several limitations that need to be considered before more comprehensive policy or intervention suggestions can be made. First, the study took place in a unique commercial district in Atlanta, GA, and may not be generalizable to all commercial districts and service industry workers. The study participants were White, and therefore, future research with service industry workers should seek to recruit a diverse sample. Before beginning the study, we were cognizant of the possibility of social desirability bias (the desire to give the socially acceptable answer) as a threat to this study’s validity (Bergen & Labonte, 2019).A precursor to the interview guide questions was added to decrease the effect of this concern—“there is no right or wrong answer, please speak freely” (Bergen & Labonte, 2019). In addition, our sample consisted of service industry workers that responded to an overdose. By interviewing only people who respond to opioid overdose with a rescue response, we have not captured all the service industry workers’ perspectives in L5P. This extended inquiry would be necessary before planning any intervention.
Implications for Occupational Health Nursing Practice
When developing overdose response training for service industry workers, public health nurses should consider education on existing resources and laws and ways to dispel myths about people who use drugs (Febres-Cordero & Smith, 2022; Febres-Cordero, Smith, et al., 2021). When training service industry workers in OEND, a rapid landscape analysis is recommended to understand the unique culture and subcultures of the service industry workers that require training to address the stigma surrounding opioid use and injecting drug use within their specific community. Resources and laws of note include “never using drugs alone” (Never Use Alone, 2022), harm reduction strategies, and hotlines for people who need someone to provide non-judgmental care in case of an overdose. Domestic and international research has identified a need for increased education to dispel the stigma around safe injection sites, community syringe disposal, and other harm reduction strategies (Des Jarlais et al., 2011; Turner et al., 2011). Harm reduction approaches need to be sensitive to the spaces in which overdose occurs and who the overdose responder is likely to be, which requires appropriately tailoring OEND training for service industry workers who may not know the benefits of harm reduction. Finally, people fear fentanyl; they know how deadly it is and how it has ravaged the community (Park et al., 2019). Fears must be addressed when training service industry workers in OEND. Although these fears may not be grounded in scientific evidence, they act as a barrier to an overdose response. These claims must be discussed when training service industry workers, even if unfounded.
Applying Research to Occupational Health Practice
Service industry workers can potentially decrease mortality from opioid overdoses in commercial settings when they are properly trained to do so. Service industry workers are the default frontline first responders and must have access to high-quality training that addresses their unique cultures and points of view. By addressing fears of rescuing people from an opioid overdose in a commercial setting with scientific evidence, we can equip these workers with the skills needed to identify and intervene in opioid overdoses while creating conversations that confront the many stigmas associated with opioid use.
Footnotes
Acknowledgements
The authors thank the service industry workers who participated in this study, The Little Five Points (L5P) Business Association, Julie Odom (L5P photographer), representatives of the Atlanta Harm Reduction Coalition (AHRC)—Dr. Mojgan Zare, Executive Director of AHRC; Ms. Mona Bennett, AHRC Ambassador; and Netline Lindsay, AHRC outreach specialist. They thank harm reduction advocates across Atlanta, GA: AHRC, the Elizabeth Foundation, the Georgia Department of Public Health, Georgia Overdose Prevention, Maxine Wright of AZIZ, and Dr. Hannah L. Cooper, Department of Behavioral, Social and Health Education Sciences, Rollins School of Public Health, Emory University. They also thank those who use drugs and utilize harm reduction services in Atlanta, GA, and “Digger” of Little Five Points. The content is solely the responsibility of the authors.
Author Contributions
SF-C: conception and design, analysis and interpretation of data, and draft and revision.
KS: conception and design, analysis and interpretation of data, and revision.
LMT: conception, design, and revision.
UAK: conception, design, and revision.
OSC: analysis of qualitative data.
ADFS: critical revision.
AKW: draft and revision.
All authors read and approved the final manuscript.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data are not publicly available because they contain information that could compromise research participant privacy/consent.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work has been partially funded by the Nell Hodgson Woodruff School of Nursing Postdoctoral Fellowship
Ethical Approval
The Emory Institutional Review Board (IRB) approved all data collection protocols (IRB00115738). Informed verbal consent was obtained to minimize the possibility of participant identification.