
Abstract
Background
Falls due to postural instability are common in construction environments especially from a height. The purpose of the study was to investigate the impact of virtual reality (VR)-generated environments at different virtual heights on postural stability.
Methods
Nineteen adults were analyzed for postural stability, tested in real (No VR) environment and in three VR environments, randomly assigned, at virtual heights of 0 ft. (VR0), 40 ft. (VR40), and 120 ft. (VR120). Postural stability was quantified using center of pressure postural sway variables and analyzed using a repeated measures analysis of variance (ANOVA). Participants also completed a simulation sickness questionnaire (SSQ) before and after VR exposure and a presence questionnaire (PQ) after VR exposure.
Findings
Significant postural instability (p < .05) was identified between VR and No VR, in which increased postural instability was evident in all VR conditions compared with No VR. Scores from SSQ were within a pre–post score difference of five and the PQ score was (104.21 ± 14.03).
Conclusion/Application to Practice
Findings suggest that VR environments, regardless of virtual height, induced increased postural instability, which can be attributed to visual sensory conflicts to the postural control system created by VR exposure. Participants’ subjective responses on SSQ and PQ confirmed the feasibility of using VR to represent realistic immersions in virtual heights. However, objectively, VR could potentially lead to postural instability, stressing caution. VR can be a potential tool for providing virtual high-altitude environment exposure for fall prevention training, however, more research is needed on postural adaptation with acute and chronic exposure to VR.
Background
Falls are the leading cause of both fatal and nonfatal injuries in construction, especially from a height (Bureau of Labor Statistics [BLS], 2017). Falls can be attributed to postural instability caused by an induced loss of balance and failure to recover from the imbalance. The BLS reported that 887 fatalities in 2017 were attributed to falls, slips, and trips and a total of 227,760 cases of nonfatal workplace injuries were due to falls (falls to lower level: 47,180; same level falls: 142,770; slips/trips: 33,720) with a high incidence rate especially in construction (24,160 falls) and manufacturing (22,010 falls) (BLS, 2017). With such high fatal and nonfatal injuries reported in occupational populations, there is a need to pursue novel assessment and training methodologies to prevent falls and fall-related injuries in an ergonomic population. The dangers due to hazardous work conditions and the physical demands placed on the human body in occupational and industrial work setting increase the risk of occupational falls (Kincl et al., 2002). Moreover, assessment of postural stability serves as an indirect measure of efficacy for both physiological and biomechanical stresses placed on an individual and quantifies an overall safety status of the postural control system (Kincl et al., 2002).
Human postural stability is governed by the complex, constant feedback postural control system, which involves, the visual, vestibular, and the somatosensory/proprioceptive systems that work to maintain an upright vertical body alignment (Horak et al., 1997; Salassa & Zapala, 2009). The majority of an individual’s body mass is located in the two thirds of the upper body, thereby creating an unstable design that is in constant need of correction to maintain upright erect balance (Winter, 1995). This design is governed by a complex coordination involving the neuromuscular afferent and efferent systems producing the necessary responses to keep the center of mass (COM) within the base of support (BOS) (Horak et al., 1997). An induced loss of balance and failure to recover from the imbalance have been reported as the primary source for postural instability leading to occupational falls (Redfern & DiPasquale, 1997). Such imbalances can be due to change in visual environments when depth, distance, or height perception is inappropriate, especially as perceptual cues to height are derived from visual feedback (Salassa & Zapala, 2009; Simeonov et al., 2003).
Visual height intolerance is described as an event when the visual stimulus leads to apprehension of postural instability and falling from a height (Huppert et al., 2013). Postural instability has been reported with height elevations of 5 m (16.4 ft.; Bles et al., 1980; Salassa & Zapala, 2009) and with increasing instability up to a height of 20 m (65.6 ft.), after which the instability plateaued (Brandt et al., 1979, 1980). In addition, postural stability and overall body sway was not impacted at altitudes of 20 (65.6 ft.), 50 (164 ft.), and 100 m (328 ft.) (Bles et al., 1980; Salassa & Zapala, 2009). Subjective height imbalance was reported to be independent of up and eye gaze but dependent on eye–object distance (Brandt et al., 1980; Salassa & Zapala, 2009). Subsequently, at heights above 20 m (65.6 ft.), no differences in body sway were evident as the visual cues became saturated and postural stability in response to height, appears to be a function of the magnitude of the eye–object distance and due to the complex coordinated and constant feedback postural control systems (Salassa & Zapala, 2009).
With the increase in industrial safety awareness, virtual reality (VR) has been proven very effective for safer exposure and complex scenario investigation. VR provides an interactive and immersive three-dimensional virtual environment (VE) in which one can move around and interact with various components within the VE (Kamat et al., 2010). The advantage of using a VR system is that it can realistically simulate scenarios that are difficult to generate in the real world (Shendarkar et al., 2006). VR can provide a high sense of realism (Slater, 2003), educate and train users with specific skills (Ragan et al., 2015), and help participants adapting behaviors and performances similar to those in the real-world activities (Heydarian et al., 2015). VR application in construction safety is shown to be effective in cases such as safety training (Teizer et al., 2013), job site safety planning (Sacks et al., 2015), hazard identification (Perlman et al., 2014), and accident preventive initiatives (Guo et al., 2017). VR training has also been reported to potentially aid in minimizing falls in the workplace (Virk & McConville, 2006). However, the use of VR has been reported to have both neutral and negative effects on posture, postural stability, and the overall postural control system. The detrimental effects of VR on postural stability have been attributed to sensory conflicts between the postural control sensory systems of visual, vestibular, and somatosensory systems (Akizuki et al., 2005; Horlings et al., 2009; Robert et al., 2016). The impact of VR-generated altitude environments on postural changes have also been previously studied and found to be impacted by virtual height (Cleworth et al., 2012, 2016; Simeonov et al., 2005). However, these studies utilized a height of 3 m to 9 m maximum height and predominantly an indoor VR environment (Cleworth et al., 2012, 2016; Simeonov et al., 2005). Although it has been reported that virtual height environments can produce behavioral, psychological, physiological, and biomechanical postural stability changes (Cleworth et al., 2012, 2016; Simeonov et al., 2005), there is still a dearth of literature on the impact of virtual height environments in construction work sites, specific to being outdoors in a construction high-altitude environment.
Therefore, the purpose of this research project was to analyze the impact of an acute exposure to VR-generated construction environments at different altitudes on postural stability. The participants were exposed to three different heights VR0 (ground level height to get baseline data), VR40 (4th floor height, corresponding to 12.2 m), and VR120 (12th floor height, corresponding to 36.6 m). Based on the outcomes of the past studies (Brandt et al., 1980; Salassa & Zapala, 2009), the hypotheses were that VR40 would show increased instability compared with the VR0, and VR120 would not show further significant instability.
Methods
A total of 20 healthy adults (10 males and 10 females; age: 24.7 ± 5.6 years; height: 166.6 ± 10.8 cm; mass: 68 ± 12.1 kg) with no self-reported history of any musculoskeletal, neurological, cardiovascular, or vestibular disorders were recruited for the study. Participant’s physical fitness status was also above recreationally trained (>3–4 days/week with consistent aerobic and anaerobic training for the at least the last 3 months leading up to testing). Informed consent from the participants based on the approved protocol from Mississippi State University’s Institutional Review Board was obtained after fully explaining the protocol along with the risks and benefit involved. The work is a part of an extended VR simulation project on postural stability (Chander et al., 2019).
The experimental procedures were conducted in the Mississippi State University’s Neuromechanics Laboratory. All VEs for this study were developed using Unity and experienced with HTC Vive Pro head-mounted display (HMD; HTC America, Seattle, WA, USA). Two VEs were designed for the experiment: a lobby environment and an urban city environment (Supplemental Figure 1). The lobby environment directed participants to the next environment and/or next trial. This environment provided an opportunity to give participants instructions within the VE regarding starting trials. The closed room was used as a VR familiarization environment. Postural stability was assessed using a force platform (AMTI—Advanced Mechanical Technology, Inc., MA, USA) with the data collected at a frequency of 100 Hz.
The experimental procedures from the study are outlined in Figure 1. Each participant had one visit to the Neuromechanics lab at Mississippi State University, which included an initial familiarization session followed by the experimental testing session. All participants were briefed about the testing procedure after which they read and signed the informed consent. After initial screening for inclusion criteria using the physical activity readiness questionnaire (PAR-Q) and a simulation sickness questionnaire (SSQ), participants were provided the VR headset to get accustomed to the fit.
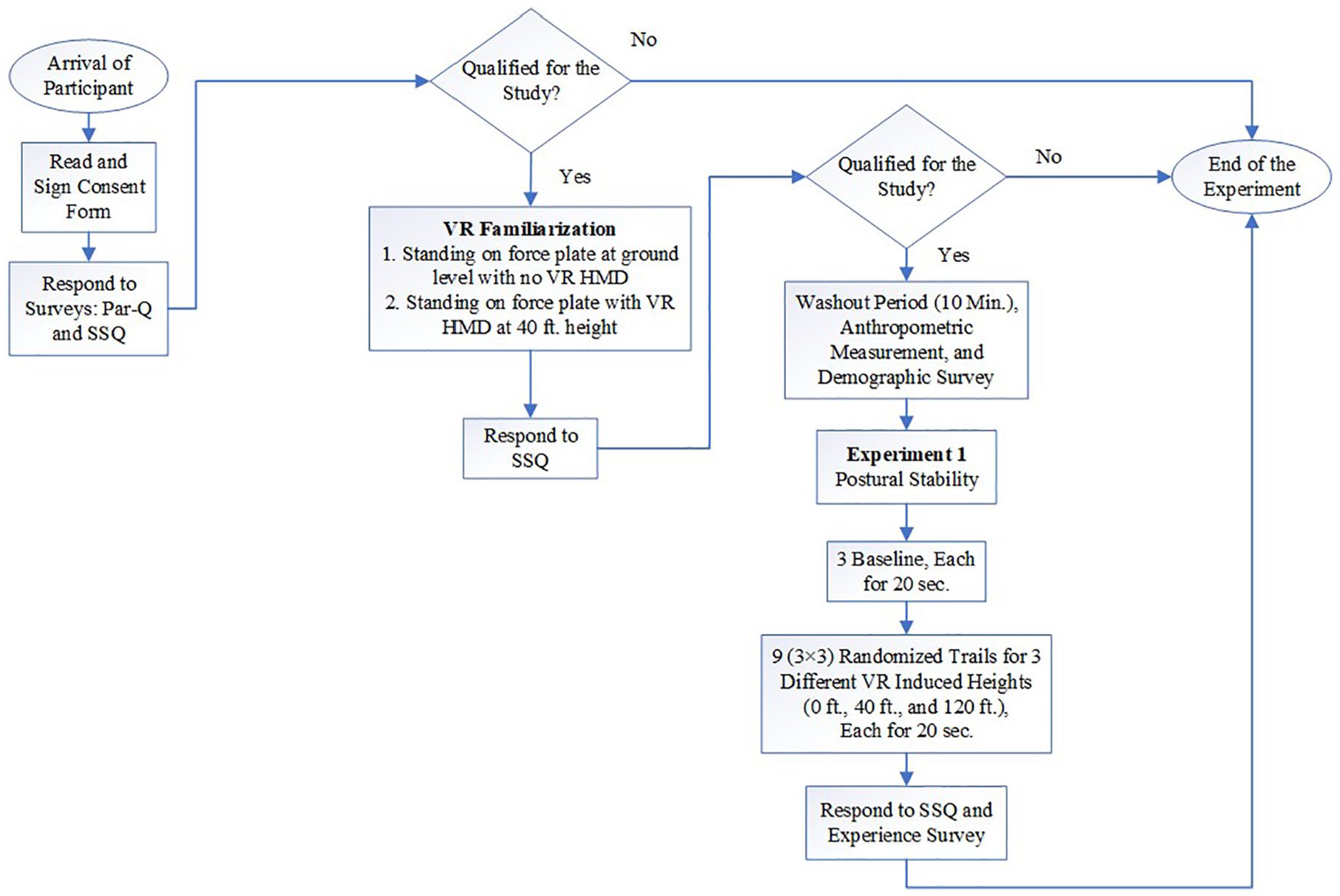
Experimental procedures from the study.
The SSQ was administered to monitor participants’ health and safety regarding their exposure to the VE. The SSQ is a 16-item questionnaire rated on a 4-point scale ranging from 0 = none, 1 = slight, 2 = moderate, and 3 = severe, based on symptoms such as general discomfort, fatigue, headache, nausea, blurred vision, dizziness, vertigo, stomach awareness, and burping, that gets classified as weighted symptoms of nausea, oculomotor, and disorientation. The total score is summed by adding symptom scores as defined by Walter et al. (2019). At any instance, if the SSQ score was equal to or greater than five, the participant was withdrawn from our study. The presence questionnaire (PQ) was used in the study to understand participants’ experience from their exposures to the virtual heights. According to Witmer and Singer (1998) of U.S. Army Research Institute for Behavioral and Social Sciences, “presence” is defined as the subjective experience of an environment, even when present in another, such as experiencing a VR-generated environment, when present physically in another environment. The PQ is a subjective perception of the environment that the individual experiences and is made of a total of 19 questions based on “involvement,” “immersion,” “visual fidelity,” and “interface quality.” The PQ has been used to assess individuals with the first exposure to VEs (Witmer & Singer, 1998). The researchers investigated participants’ subjective perception regarding the realism and quality of the VE (whether the simulated high-altitude construction site resembled the real-world settings).
During the VR familiarization, the participants were asked to stand in the closed-room environment and use their gaze to complete several tasks. These tasks involved looking at different boxes until they disappear. This practice gave the participants the understanding of using their gaze to complete a task within the VE and move from one scenario to another. In addition, one practice trial of 20 seconds consisting of standing stationary on a building rooftop at 40 ft. height was provided. This marked the completion of the VR familiarization, following which the participant removed the HMD, sat down for a 10-minute rest/washout period, and completed the second round of the SSQ.
After the washout period, all participants were directed to stand on the force platform in bilateral stance with feet at shoulder width apart and provided instruction to stand erect and as quiet as possible with the hands by the side of the body. During the experimental VR trials, the urban city construction environment was used for assessing participants’ postural stability. The participants were standing on wooden scaffoldings attached to a building at different heights. Postural stability assessments included three trials of 20 seconds each in four testing conditions: (standing on force platform at ground level with no VR [No VR]; standing on force platform at ground level in VR [VR0]; standing on force platform at fourth floor level [40 ft. [12.2 m] in height] in VR [VR40]; and standing on force platform at 12th floor level [120 ft. [36.6 m] in height] in VR [VR120; Figure 2]). This also illustrates an example of the different experimental testing environments. Participants were instructed to stay as still and erect as possible and in Trial 3 of each VR condition they were allowed to look around the environment. No VR condition was always performed first and treated as the baseline measure, whereas VR0, VR40, and VR120 trials were randomized using a computer algorithm. Completion of three 20-second trials in all four testing conditions marked the end of postural stability assessment. Participants were then asked to remove the headset and sit down to rest for 5 minutes, following which they completed a third round of SSQ and a PQ (Witmer & Singer, 1998), which marked the end of the experiment.
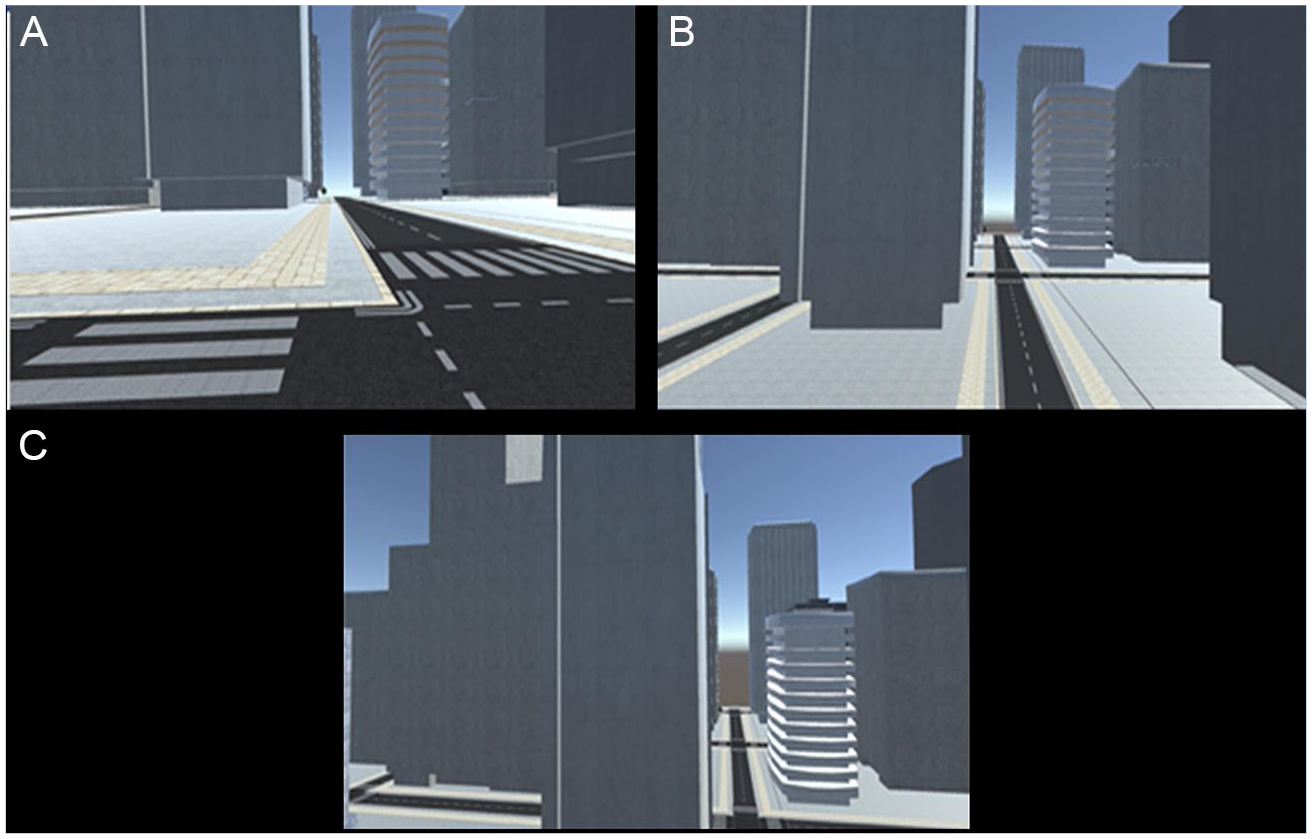
Experimental testing VR exposure environments: (A) VR0, (B) VR40, and (C) VR120.
Center of pressure (COP) excursions during the balance assessments, derived from the force platform, were analyzed to quantify postural sway as a measure of postural stability. COP excursions were used to calculate postural sway variables, average displacements in the medial-lateral (M/L) and anterior–posterior (A/P) directions (M/L-DISP and A/P-DISP), the 95% ellipsoid area (EA) and average sway velocity (SV). An increase in the displacements, EA, and SV, represent faster and greater COP excursions, indicating decreased postural stability. All postural sway–dependent variables were analyzed for all four testing conditions (No VR, VR0, VR40, and VR120). Participants’ self-reported ratings on the 19-item PQ were collected on a 7-point scale and the total score was calculated by adding scores for each team (reversing scores for items 14, 17, and 18). The PQ posits four subscales: involvement, immersion, visual fidelity, and interface quality. Among the subscale scores, the immersion score indicates that the VE responded realistically to participants’ actions; the visual fidelity score confirms the reliability of the VE regarding its visual clarity and depth perception; and the interface quality score shows the ease of using this VR setting to perform assigned tasks. Descriptive statistics (mean and standard deviation) for each factor were evaluated along with the total PQ score.
All dependent postural sway variables were analyzed using a one-way within subjects repeated measures analysis of variance (RM-ANOVA) between the four testing conditions (No VR vs. VR0 vs. VR40 vs. VR120). Main effect significance was followed up with post hoc pairwise comparisons with a Fisher’s Least Significant Difference correction. Descriptive statistics for each of the survey items were used to analyze survey response. All statistical analyses were performed with an alpha level of p < .05 using IBM SPSS statistical software v.25.
Results
All 20 participants completed the study; however, based on the SSQ, one participant was excluded from the data analysis which resulted in a total sample size of 19 participants. Their mean age was 25 ± 5.6 years, mean height was 166.13 ± 11.1 cm, and weight was 67.86 ± 12.4 kg. The participants were novice in terms of their exposure to work conditions at height. The age of the participants and their lack of exposure to work conditions at height was in line with the aim of using VE for novice construction workers training before exposing them to the real-world high-altitude worksite.
The RM-ANOVA revealed significant main effect differences for the exposure environment for three out of the four postural sway–dependent variables average M/L and A/P displacement and 95% ellipsoid sway area. Table 1 provides p value, F statistic, and partial eta-squared effect sizes
Results From Repeated Measures ANOVA Including Descriptive Statistics for Postural Sway Variables
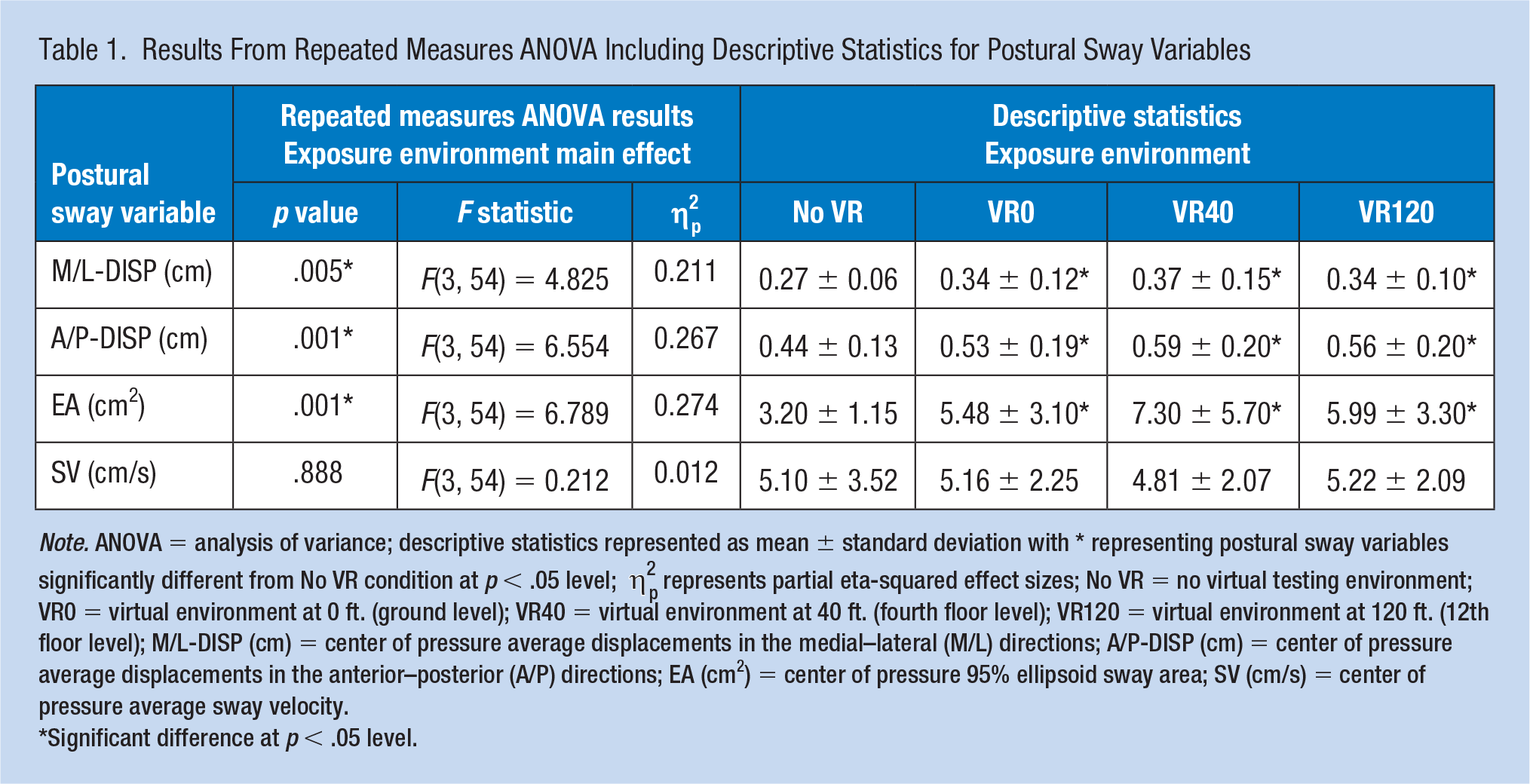
Note. ANOVA = analysis of variance; descriptive statistics represented as mean ± standard deviation with * representing postural sway variables significantly different from No VR condition at p < .05 level; η2p represents partial eta-squared effect sizes; No VR = no virtual testing environment; VR0 = virtual environment at 0 ft. (ground level); VR40 = virtual environment at 40 ft. (fourth floor level); VR120 = virtual environment at 120 ft. (12th floor level); M/L-DISP (cm) = center of pressure average displacements in the medial–lateral (M/L) directions; A/P-DISP (cm) = center of pressure average displacements in the anterior–posterior (A/P) directions; EA (cm2) = center of pressure 95% ellipsoid sway area; SV (cm/s) = center of pressure average sway velocity.
Significant difference at p < .05 level.
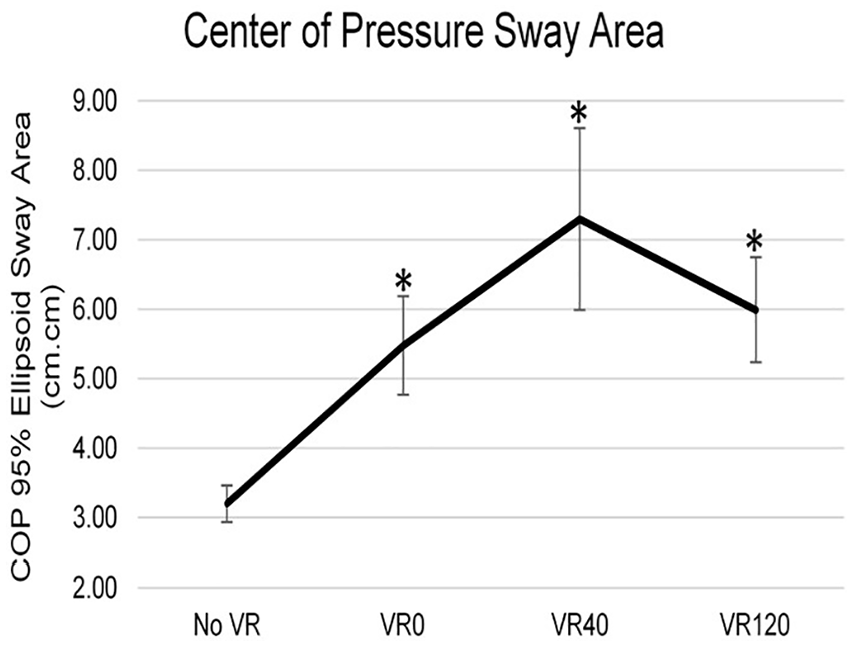
Center of pressure (COP) 95% ellipsoid sway area during postural stability testing with no virtual reality (No VR), virtual reality environment at ground level (VR0), virtual reality environment at 40 ft. (VR40) and virtual reality environment at 120 ft. (VR120).
Descriptive Statistics for the Subscales of Presence Questionnaire (PQ)
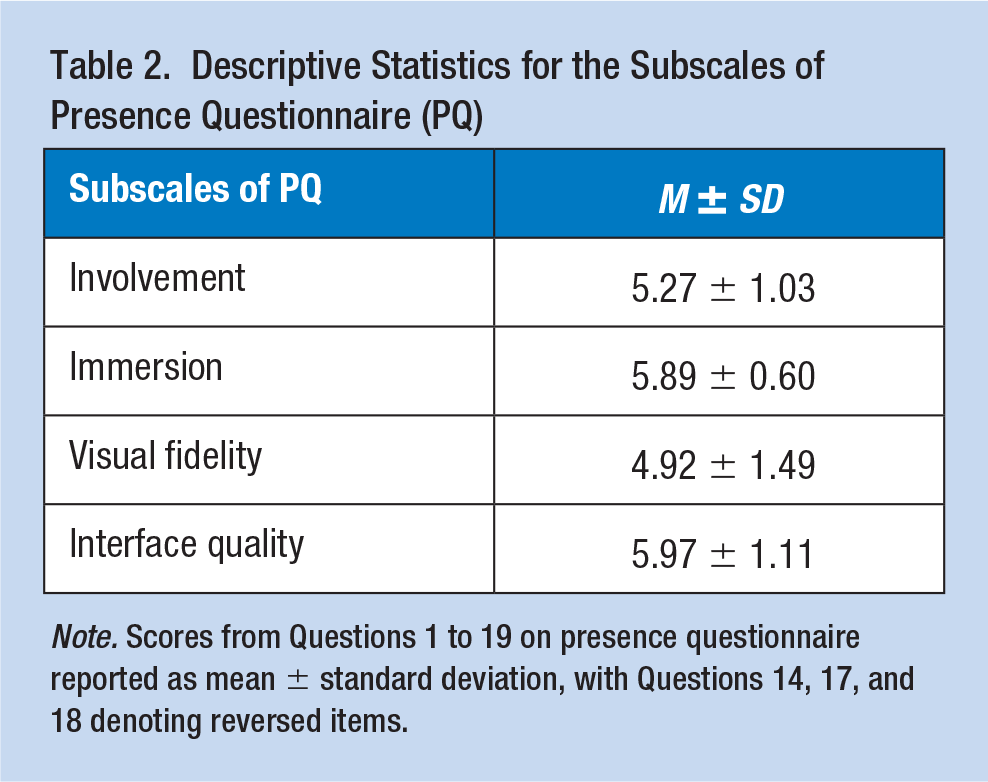
Note. Scores from Questions 1 to 19 on presence questionnaire reported as mean ± standard deviation, with Questions 14, 17, and 18 denoting reversed items.
Discussion
The purpose of the study was to investigate the impact of VR-induced high-altitude environments on postural stability. Postural stability of an individual, analyzed through postural sway, is an indicator for overall safety status of the postural control system and subsequently, an indicator of fall risk. Higher values for postural sway variables of A/P-DISP, M/L-DISP, and EA suggest that VR environments, regardless of the virtual heights, induced significantly increased postural instability compared with the No VR condition, which can be attributed to VE’s visual sensory conflicts of the postural control system. While significant differences were not found between different heights in the VR-generated environments, descriptive statistics of postural sway variables during VR0, VR40, V120, indicated that the VR40 condition induced the greatest postural sway variables, subsequently greatest postural instability, and fall risk. These results can be attributed to the saturation of visual cues for maintaining postural stability.
The survey responses confirmed that participants experienced realistic immersion in VR environments with high level of involvement, immersion, and interface quality. Even though the visual fidelity score was higher than the neutral score (4), it was lower than the other three scores. A past study validated four VEs in terms of realistic immersion using the PQ scores and reported a standard mean score of 98.11, with a standard deviation of 15.78 (Witmer & Singer, 1998). In the current study, a high average score for PQ (M = 104.21, SD = 14.03, Min = 72, Max = 129) confirmed the realism of the developed VE and participants’ perception of successful immersion. The average scores for all four subscales of the PQ were found to be greater than the neutral score four and can be considered as positive perception for realistic and high-quality virtual immersion.
The participants of this study were not construction workers and had no experience of exposing them in such a high-risk environment. Therefore, their perception of visual fidelity items must have been influenced by the representation of high-altitude fall-prone VR environments. During the study, each participant was tested for simulation sickness three times (beginning, after first VR exposure, and at the end). Although successfully participated, one (out of 20) participants provided a simulation sickness score greater than five at the end of the study. To avoid any bias from the simulation sickness, that participant data were removed from the analysis. Based on the results, VR can be a potentially safer, easier, and convenient method to expose individuals to outdoor and high-altitude construction environments for training to improve their postural stability performance and subsequently prevent falls. Significant differences between No VR and VR conditions and differences between VR conditions from the current study are discussed below.
Comparison Between No VR and VR Conditions
Greater postural instability in the VR conditions was identified regardless of the virtual heights as compared with the No VR condition. Results could be attributed to changes in the visual field of the VR environments, as visual system provides an important afferent feedback in the maintenance of postural stability (Horak, 2006). The use of VR during standing tasks has been reported to cause postural instability similar to standing with eyes closed (Horlings et al., 2009). In addition, the use of head-mounted displays for VR exposure produces sensory conflicts between the visual, vestibular, and somatosensory systems, resulting in poor postural stability (Robert et al., 2016). The results from the current study support previous literature assessing the impact of VR on posture that have identified increased postural instability in the VE (Cleworth et al., 2012, 2016; Robert et al., 2016). This increased postural instability has been attributed to altered visual sensory information and the presence of sensory conflict between the afferent postural control sensory systems (Akizuki et al., 2005; Horlings et al., 2009; Robert et al., 2016). However, according to the Cleworth et al. (2012) study, when a VE is created as a duplicate of the real environment, the effects of VR-induced postural instability can be minimized. In the current study, the VE used was not a duplicate of the real environment used for the baseline No VR condition (laboratory space). The virtual transitioning lobby environment, though not a duplicate of the real laboratory environment, still mimicked the laboratory room’s dimensions. However, the lobby environment was used for familiarizing participants with VR, transitioning them from one environment to the other, and providing them with instructions within VE. This environment was not a part of the postural stability analysis. Such sensory conflict between the real environment and non-duplicate VE could potentially be attributed to the significantly increased postural instability observed in the VR conditions regardless of height (VR0 vs. VR40 vs. VR120) as compared with No VR condition and could show nonsignificant differences between the VR conditions.
Comparison Between VR Height Conditions
Current findings also support previous literature that have identified that VEs were successful in reproducing the effects of standing at a physical height on postural control (Cleworth et al., 2012, 2016; Simeonov et al., 2005). In the current study, the increase in the postural instability with varying heights could be attributed to the visual height intolerance which leads to an apprehension of postural instability and falling from a height (Huppert et al., 2013). The greatest postural instability was observed in the VR40 condition followed by the VR120 condition, which also supports previous literature that postural instability was shown to increase between 5 and 20 m heights (T (Brandt et al., 1979, 1980), and plateau after 20 m (Bles et al., 1980; Brandt et al., 1979, 1980; Salassa & Zapala, 2009). In the current study, VR40 condition was at 40 ft. elevation, corresponding to 12.19 m and VR120 condition was at 120 ft. elevation, corresponding to 36.57 m. Thus, the visual height intolerance present at VR40 (Brandt et al., 1979, 1980) and the potential saturation of visual cues at VR120 (Salassa & Zapala, 2009), could be attributed as the potential rationale of the observed results in the current study. However, as a statistically significant difference was not identified between different VR-induced heights, postural instability results comparing different VR heights should be considered with caution.
Limitations of the current study include the use of a VE which is not a duplicate of the real environment. However, the No VR condition was merely an interpretation of baseline postural stability among all participants. In addition, testing participants at 40 ft. and 120 ft. of real environment was both a safety issue and feasibility issue. Hence, the comparison of the VR-generated outdoor and high-altitude construction site was used to analyze the impact of virtual height on postural stability. However, exposing participants in virtual heights could create severe simulation sickness in them. Therefore, only three different heights were tested to see the change in postural stability within 20 m height and beyond 20 m to a higher altitude. Future studies should include additional heights for each range. The current study did not incorporate any moving entities in the VR construction environment, which can negatively impact postural stability. Future studies on VR exposure and postural stability specific to construction environments should incorporate moving entities such as concrete mixer trucks, cranes, other construction workers with additional environmental changes such as inclined standing surface and different daylight conditions.
In addition, young healthy adults with no prior exposure to high-altitude construction environments were utilized as participants, which may not be a true representation of the current construction workforce. However, the current sample of participants can be seen as a representation of amateur and novice workers, who do not have experience in outdoor and high-altitude construction environments and are more prone to falls and fall-related injuries due to postural instability. Finally, even though the current study provided familiarization of the VR environments before testing, exposure during both familiarization and experimental testing accounted for only a few minutes of acute exposure to VR. Postural stability might be impacted differently with long duration and repeated exposure to VR. Future studies should analyze the impact of repeated exposures to outdoor and high-altitude construction environments to investigate potential training effects of VR.
Although the fear of height (acrophobia) of the participants could be an issue, all the possible measures were taken to avoid recruiting individuals with acrophobia. The experimental protocol with the virtual heights were explained to the participants before they were recruited. During the explanation, they were informed regarding the 40 and 120 ft. virtual heights and it was included in the consent form as well. None of the participants disclosed any acrophobia before recruitment and only with the participants’ consent, they were provided familiarization trails, during which each participant underwent a familiarization session which included standing on 40 ft. height. None of the participants experienced acrophobia during the familiarization or the testing. Furthermore, assessing for acrophobia due to heights, and claustrophobia due to enclosed VR HMDs should be possible precautionary measures for future studies, especially if such VR environments are used for longer durations and repetitively. While the current study only assessed flat surface standing conditions, future studies should also incorporate slopped roofs in VR environment while standing on inclined surfaces to address construction workers and roofers who work at an altitude on an inclined surface. Finally, donning the HMD, even though it adds extra mass to the head, on the distal segment of the kinetic chain of the body from the ankle joint, the mass is only a minimal 470 g. In addition, the HMD mass is evenly distributed to achieve a balanced COM, as reported by HTC Vive (HTC America). However, the impact of the added 470 g of HMD on postural stability was not assessed in this current study, as the current study aimed to understand the differences between VR and No VR and understand differences between VR altitude comparisons. Future studies assessing postural stability with the use of different types of HMD, should consider the impact of their mass on postural stability.
The current project’s research goals address multiple key needs identified in the National Occupational Research Agenda (NORA) for Construction, with specific emphasis on “Objective 1: Falls from heights—Eliminate falls in construction; Objective 2: Falls from the same level—Significantly reduce or eliminate slips, trips, and falls; and Objective 16: Training—Research to increase the reach, scope, and effectiveness of training in construction” (TWU Council, 2018). While falls from a height may not be completely eradicated from occupational environments, such as construction and roofing environments, early exposure to different heights and experience with working on heights can positively impact postural stability and aid in fall prevention in ergonomics. In addition, there are many costs associated with experimental setup, replication of trials, change in scenarios, time and labor cost, and control of surveillance factors. The use of VE can eliminate most of these costs by providing a flexible mean for modification in scenarios and trials.
Implications for Occupational Health Practice
The findings from the study suggest that VR-induced high-altitude work environment had positive perception for realistic and high-quality virtual immersion and also demonstrated significant differences between No VR and VR environments in postural stability, in that VR-generated environments induced a significantly greater postural instability. Findings suggest that VR environments regardless of virtual height, induced increased postural instability, which can be attributed to visual sensory conflicts to the postural control system created by VR exposure. Participants’ subjective responses on SSQ and PQ confirmed the feasibility of using VR to represent realistic immersions in virtual heights. In the current study, all the participants had no previous exposure to VR altitudes and the PQ was administered to assess the “presence” in an acute session of VR exposure to high altitudes. In addition, the different altitude environments (VR0, VR 40, and VR120) were all randomized and hence the participants did not have a gradual increase in height exposure which might have influenced the PQ negatively. However, objectively, VR could potentially lead to postural instability, stressing caution. Even though the VR-induced heights did not produce a significant difference in the postural stability, a virtual height of 40 ft. induced greater postural instability compared with 0 ft. and 120 ft., while the use of VR by itself induced greater postural instability compared with no VR. However, with more VR familiarization, repeated exposure and training with randomized virtual heights, VR could potentially be used as a training tool for fall prevention training by exposing novice workers to high-altitude hazardous work environments in a safe and convenient way.
Applying Research to Occupational Health Practice
Virtual reality (VR) can be used to expose novice individuals to high-altitude work environments with realistic perception. The use of VR and the VR-induced Virtual Environment (VE) at different altitudes can impact postural stability and ultimately fall risk. Results from the study further contribute to understanding the impact of virtual height on postural stability, specific to construction environments in outdoor and in high-altitude VEs. Findings can help in implementing VR as a potential tool for providing virtual high-altitude construction environment exposure for training and thereby preventing falls and promoting safety, however, more research is needed on postural adaptation with acute and chronic exposure to VR.
Supplemental Material
WHandS_-_Supplemental_Figure_1 – Supplemental material for Impact of Virtual Reality–Generated Construction Environments at Different Heights on Postural Stability and Fall Risk
Supplemental material, WHandS_-_Supplemental_Figure_1 for Impact of Virtual Reality–Generated Construction Environments at Different Heights on Postural Stability and Fall Risk by Harish Chander, Alireza Shojaei, Shuchisnigdha Deb, Sachini N. K. Kodithuwakku Arachchige, Christopher Hudson, Adam C. Knight and Daniel W. Carruth in Workplace Health & Safety
Supplemental Material
WHandS_-_Supplemental_Figure_2 – Supplemental material for Impact of Virtual Reality–Generated Construction Environments at Different Heights on Postural Stability and Fall Risk
Supplemental material, WHandS_-_Supplemental_Figure_2 for Impact of Virtual Reality–Generated Construction Environments at Different Heights on Postural Stability and Fall Risk by Harish Chander, Alireza Shojaei, Shuchisnigdha Deb, Sachini N. K. Kodithuwakku Arachchige, Christopher Hudson, Adam C. Knight and Daniel W. Carruth in Workplace Health & Safety
Supplemental Material
WHandS_-_Supplemental_Figure_3 – Supplemental material for Impact of Virtual Reality–Generated Construction Environments at Different Heights on Postural Stability and Fall Risk
Supplemental material, WHandS_-_Supplemental_Figure_3 for Impact of Virtual Reality–Generated Construction Environments at Different Heights on Postural Stability and Fall Risk by Harish Chander, Alireza Shojaei, Shuchisnigdha Deb, Sachini N. K. Kodithuwakku Arachchige, Christopher Hudson, Adam C. Knight and Daniel W. Carruth in Workplace Health & Safety
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental Material is available online for this article.
Author Biographies
Harish Chander, PhD, is an assistant professor of Biomechanics and the Co-Director of the Neuromechanics Laboratory in the Department of Kinesiology at Mississippi State University. Chander’s area of research includes biomechanics, human factors and ergonomics, slips, trips and falls, fall prevention, injury prevention and safety promotion.
Alireza Shojaei, PhD, is an assistant professor in the Department of Building Construction Science at Mississippi State University. Shojaei’s area of research includes computer-based modeling and simulation, smart and connected buildings and cities, intelligent infrastructure and smart design and construction, construction informatics, sustainability, project management and economics in construction, automation and safety.
Shuchisnigdha Deb, PhD, is an assistant professor in the Department of Industrial, Manufacturing, and Systems Engineering at University of Texas-Arlington. Deb’s area of research includes human factors and ergonomics, virtual reality, transportation and safety promotion.
Sachini N.K. Kodithuwakku Arachchige, MD, MS, is a PhD student in the Neuromechanics Laboratory in the Department of Kinesiology at Mississippi State University. Arachchige’s area of research includes biomechanics, human factors and ergonomics, fall prevention, injury prevention and safety promotion.
Christopher Hudson, MS, is a research associate and a PhD student in the Center for Advanced Vehicular Systems (CAVS) at Mississippi State University. Hudson’s area of research includes human computer interaction, autonomous vehicle modelling, virtual reality.
Adam C. Knight, PhD, is an associate professor, Co-Director of the Neuromechanics Laboratory and the Graduate Program Coordinator in the Department of Kinesiology at Mississippi State University. Knight’s area of research includes biomechanics, athletic training, and injury prevention and performance enhancement.
Daniel W. Carruth, PhD, is the associate director for Human Factors Division in the Center for Advanced Vehicular Systems (CAVS) at Mississippi State University. Carruth’s area of research includes human factors, autonomous vehicle modelling, virtual reality and human robot interaction.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.