
Abstract
Background: Mild traumatic brain injury (mTBI) is a nationwide problem; yet, no firefighter mTBI data are available. Methods: In this cross-sectional study, we assessed retrospective head injuries using WHO guidelines. We captured mTBI frequency and examined firefighters’ symptoms (e.g., using Ohio State University Traumatic Brain Injury Identification method, Brief Traumatic Brain Injury Screen, Warrior Administered Retrospective Causality Assessment Tool). Findings: Of 1,112 firefighters contacted, 60 responses were included. Most participants were White (80%), male (90%), former athletes (75%). 62% met mTBI symptom criteria. 75% reported at least one lifetime head injury. Number of head injuries and depression symptoms were associated (r = .36, p < .05). Conclusion/application to practice: Overall, it appears most firefighters have sustained at least one lifetime mTBI. Those with multiple head injuries may be at increased risk of depression. Occupational health professionals should be aware of firefighters’ mTBI risk. Further research is warranted given findings.
Background
Over 1 million Americans serve as career firefighters. In 2017, upward of 58,000 firefighters were injured in the line of duty, and 60 firefighters died on duty (Evarts & Molis, 2018). In 2014, there were approximately 288,000 Americans diagnosed with traumatic brain injury (TBI) at hospitals, and 56,800 Americans died of TBI-related injuries (Peterson et al., 2019). The true annual incidence of TBIs is thought to be much higher because many people may not seek medical services for mild traumatic brain injuries (mTBIs; Greenwald et al., 2012). Yet, there is currently no prevalence and incidence data on TBIs in firefighters.
The World Health Organization (WHO) Collaborating Centre Task Force on Mild Traumatic Brain Injury defines mTBI as “. . . an acute brain injury resulting from mechanical energy to the head from external physical forces” (Carroll et al., 2004, p. 115). Mild traumatic brain injuries can result in deleterious consequences including attention, memory, learning, processing speed, and/or inhibition difficulties within the first 3 months (Terry et al., 2019). Prolonged motor deficits (Collins et al., 1999) and memory problems for years post-injury (Bedard et al., 2017) have also been noted.
The National Fire Protection Agency estimates that there were 58,835 U.S. firefighter line-of-duty injuries in 2017. Injuries to extremities are most common (42% of fire-related injuries), followed by head and shoulder injuries (26%) (U.S. Fire Administration, 2016). Falls, motor vehicle accidents, loss of oxygen, and exposure to blast may involve head trauma (Brain Injury Alliance of Utah, n.d.); however, the frequency of TBI has not been reported suggesting that it has not been systematically studied among firefighters.
Symptoms commonly associated with mTBI and post-concussive syndrome (PCS) among military veterans (Tanielian & Jaycox, 2008) appear to be experienced among firefighters as well (Barr et al., 2016; Billings & Focht, 2016; Carpenter et al., 2015). These symptoms include headaches, memory loss, musculoskeletal pain, neurological deficits, and depression (Tanielian & Jaycox, 2008). Given these injury data, the inherent dangers involved in fighting fires, and insufficient TBI documentation among firefighters, we aimed to examine the prevalence of mTBI among firefighters and to capture initial estimates of PCS and mTBI symptoms among firefighters.
Methods
Our team received permission from a southwestern USA fire department chief to contact 1,032 firefighters via email containing a Qualtrics survey link. In addition, to increase the generalizability of study results, 80 firefighters from across the United States who had participated in previous Warriors Research Institute (WRI) studies and given their permission to be contacted for future research opportunities were also invited to participate. English-speaking, active-duty firefighters with computer access were eligible for the study. Respondents were entered in a drawing for one of three US$100 gift cards. Study procedures were approved by Baylor Scott & White’s Institutional Review Board (IRB), and all participants provided informed consent.
Our survey was designed to gather mTBI symptoms, focusing on injuries acquired through athletics, military, and fire service. The results do not constitute an official diagnosis of mTBI. Symptom criteria for lifetime mTBI was defined as exhibiting one or more of the following: confusion, disorientation, loss of consciousness (LOC; ≤30 minutes), or posttraumatic amnesia (≤24 hours after injury). Symptoms could not be attributed to substance use and were not exacerbated by preexisting medical conditions. Symptom criteria for lifetime mTBI was based on WHO guidelines (Ruff et al., 2009).
Data Collection
The Ohio State University Traumatic Brain Injury Identification (OSU TBI-ID) method is a self-report questionnaire regarding lifetime history of head and neck injuries (Corrigan & Bogner, 2007). Studies of concordance between medical documentation and adult recall revealed a 68% recall rate (McKinlay et al., 2017) with high test–retest (r > .60; Bogner & Corrigan, 2009) and interrater reliability (r > .80; Corrigan & Bogner, 2007).
The Brief Traumatic Brain Injury Screen (BTBIS)–Modified for Athletes is a three-item measure of seven post-concussive symptoms (Schwab et al., 2007), which was used to assess mTBI-related factors that occurred during athletics. In prior studies, convergent validity was fair (neurobehavioral symptom inventory: r = .48, p < .001) and concurrent validity was good (72%–88%; Schwab et al., 2007).
The Warrior Administered Retrospective Causality Assessment Tool for Firefighters (WARCAT-FF) was adapted from the original WARCAT for veterans to assess first responder-related injuries in this study. The language was modified to encompass firefighter-related activities. The WARCAT-FF is a 20-item self-report measure of blast exposure, probability of associated TBI, and presence of altered mental state, somatic and neuropsychiatric symptoms post-injury and/or post-deployment (Terrio et al., 2009). The WARCAT’s psychometric properties indicate 60% sensitivity and 96% specificity (Terrio et al., 2011).
Pittsburgh Sleep Quality Index (PSQI) was used to assess sleep quality (Buysse et al., 1989). Responses on a Likert-type scale (0 = not during the past month to 3 = 3 or more times a week) yielded a global score (range = 0–21) and scores exceeding “5” indicated “poor” sleep quality. Previously, the global PSQI score indicated a high degree of internal consistency (α = .85, p < .001), and the seven PSQI component scores had strong internal homogeneity (α = .83) (Buysse et al., 1989).
Beck Depression Inventory–Primary Care (BDI-PC) is a seven-item measure used to assess depressive symptoms occurring over the past 2 weeks using a Likert-type scale from 0 to 3 (Beck et al., 1997). Possible total scores range from 0 to 21, and total scores exceeding “4” indicated a positive screen for depression. The BDI-PC has high reliability, internal consistency, specificity, and sensitivity (Green et al., 2001).
The PTSD Checklist–Civilian (PCL-C) is a 17-item self-report measure used to assess posttraumatic stress disorder (PTSD) symptoms over the past month using Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association [APA], 1994) criteria (Weathers et al., 1993). Responses were provided on a Likert-type scale (1 = not at all to 5 = extremely) with a clinical cutoff score of “50” indicating a positive screen for PTSD (Weathers et al., 1993). The PCL-C has high rates of internal consistency (α = .93; Meyer et al., 2012), test–retest reliability (rs ranging from .68 to .92; p < .001), convergent validity (r > .75), and discriminant validity (r = .82; Ruggiero et al., 2003).
Depression Anxiety Stress Scale (DASS-21) is a 21-item questionnaire used to assess symptoms of depression, anxiety, and stress over the previous week using a 4-point Likert-type scale (0 = did not apply to me at all to 3 = applied to me very much or most of the time; Lovibond, 1983). Responses were calculated, and total subscale scores were considered symptomatic if they fell in the following ranges: depression 10 to 42, anxiety 8 to 42, and stress 15 to 42. The DASS-21 total scale Cronbach’s alpha was .93, and subscale alphas ranged from .82 to .94 (Antony et al., 1998; Henry & Crawford, 2005).
The Rivermead Post-Concussion Symptoms Questionnaire (RPQ) is a 16-item measure of post-concussive symptoms on a 5-point Likert-type scale (0 = not experienced at all to 4 = severe problem; King et al., 1995). Symptom scores of 2 or higher were summed to produce total scores. Higher scores indicated more severe symptoms. The RPQ has good test–retest reliability (r = .72–.89, p < .01; Eyres et al., 2005).
Data Analysis
Analyses were calculated using IBM SPSS for Windows (Version 25). First, characteristics of the firefighter population including demographic features were summarized using descriptive statistics. Second, lifetime mTBI was defined as at least one head injury with at least one WHO mTBI symptom from athletic, military, or fire service involvement using data from OSU TBI-ID, BTBIS, and/or WARCAT-FF. Next, demographic features, mechanisms of injury, and mental health symptoms were summed and cross-tabulated with mTBI symptoms. Finally, a bivariate correlation was run to examine the association between head injuries and depression symptoms.
Findings
In total, 64 firefighters completed the survey; however, four firefighters who reported ongoing injury-related litigation were excluded. Twelve injuries reported on the OSU were unreadable or non-applicable as injury occurred outside of the study criteria (i.e., not from athletic, fire, or military experience; sprained wrist). The majority of participants were White (80%), males (90%) aged 27 - 67 (M = 41.64, SD = 9.36; Table 1). Ninety-five percent of respondents participated in sports prior to entering the fire service. Fifteen percent were in the military, and 65% classified themselves as firefighter, 8% as driver engineers; 8% as captains.
Characteristics of Firefighter Study Population
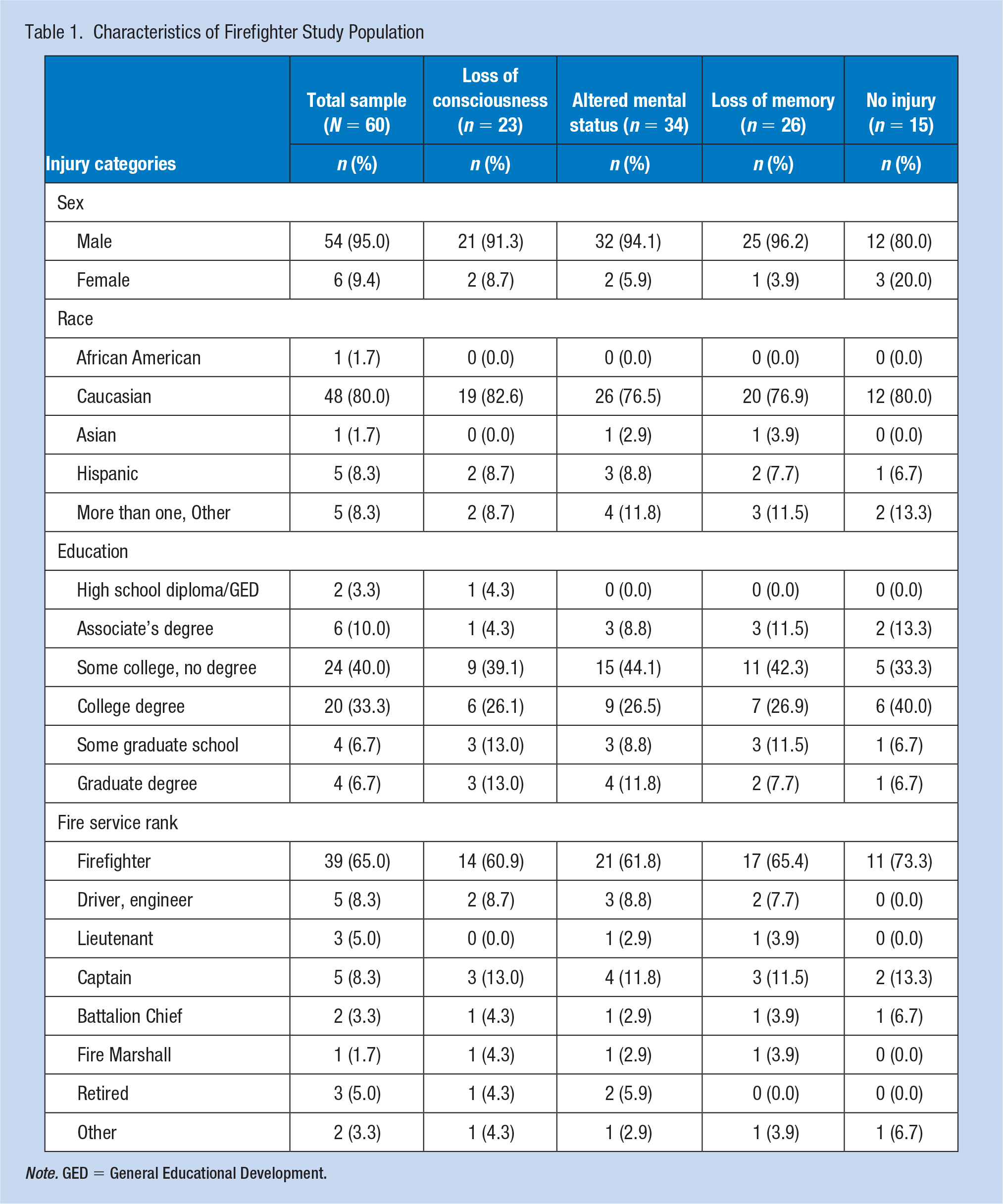
Note. GED = General Educational Development.
Out of 60 responses, 45 (75%) firefighters reported sustaining at least one head injury in their lifetime (Table 2); 38% of all participants reported an injury with LOC, 43% reported loss of memory after injury, and 57% indicated feeling dazed and confused after sustaining the injury. Thirty-nine (65%) respondents reported experiencing at least one of these symptoms after their injury. Sixteen (27%) firefighters endorsed experiencing two mTBI symptoms in the same injury, and 17 (28%) indicated experiencing all three symptoms in the same injury. Participants met symptom criteria for lifetime mTBIs if they reported sustaining a head injury that resulted in at least one WHO mTBI symptom such as confusion or disorientation, LOC for 30 minutes or less, or posttraumatic amnesia for less than 24 hours after sustaining a head injury.
Reported Lifetime Mental Health Symptoms Among a Sample of Firefighters (N = 60)
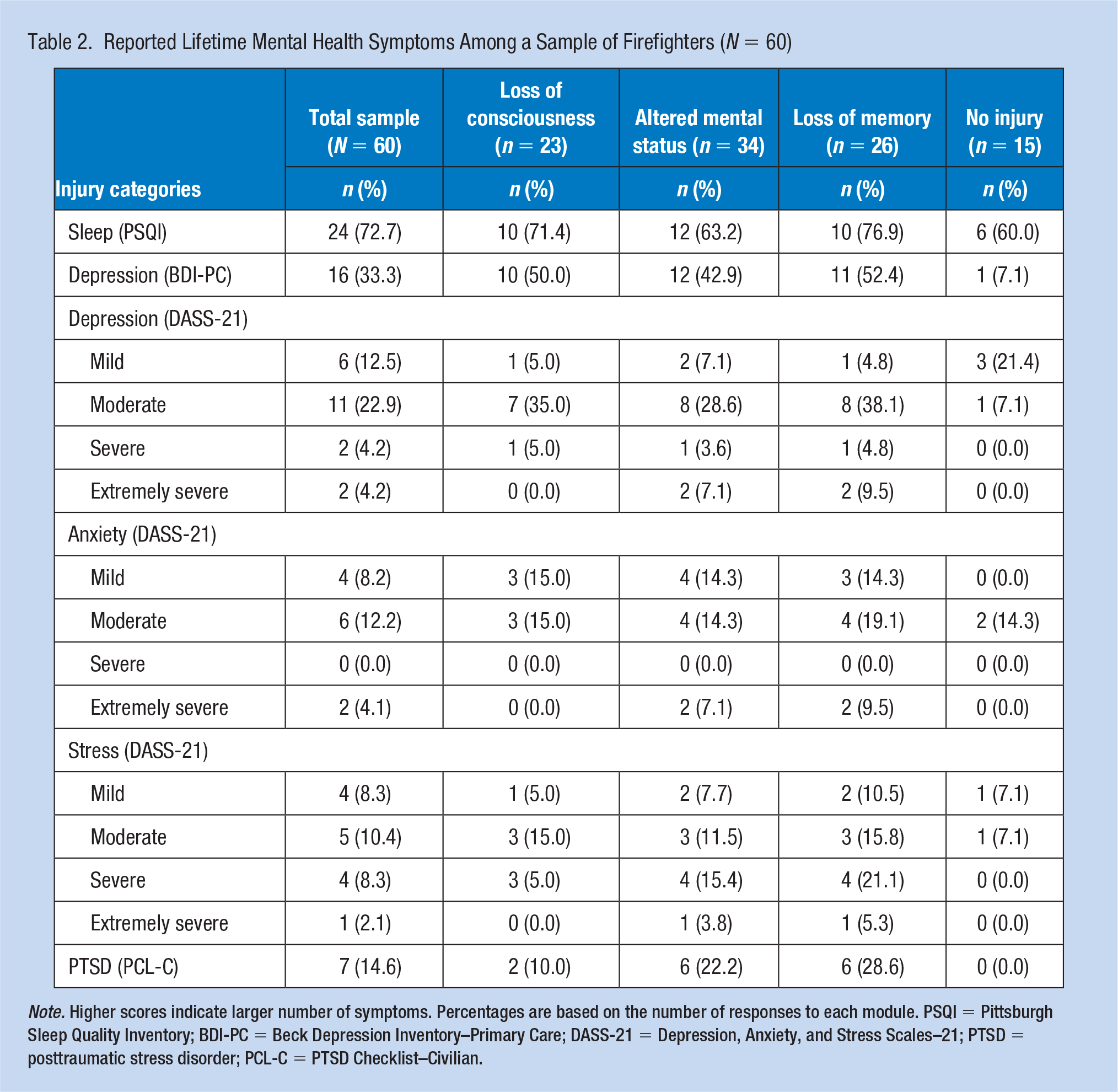
Note. Higher scores indicate larger number of symptoms. Percentages are based on the number of responses to each module. PSQI = Pittsburgh Sleep Quality Inventory; BDI-PC = Beck Depression Inventory–Primary Care; DASS-21 = Depression, Anxiety, and Stress Scales–21; PTSD = posttraumatic stress disorder; PCL-C = PTSD Checklist–Civilian.
Of the 45 firefighters who reported lifetime head injuries, 37 (82%) met symptom criteria for lifetime mTBI (Table 3). Twenty-four (53%) of the participants with head injuries reported sustaining their injury while playing a sport, and 23 (51%) of those injuries met the symptom criteria for mTBI. Nine (20%) of the firefighters with head injuries reported at least one head injury from fire service. Of those nine, eight met the symptom criteria for mTBI. Five (11%) firefighters with head injuries reported that the injury was due to an improvised explosive device (IED). Following these IED-sustained head injuries, four (9%) met symptom criteria for mTBI. Concerning military service, no firefighters reported experiencing an injury that resulted in mTBI-related symptoms.
Mechanisms of Injury and Associated Mild TBI Symptoms Among a Sample of Firefighters (N = 60)
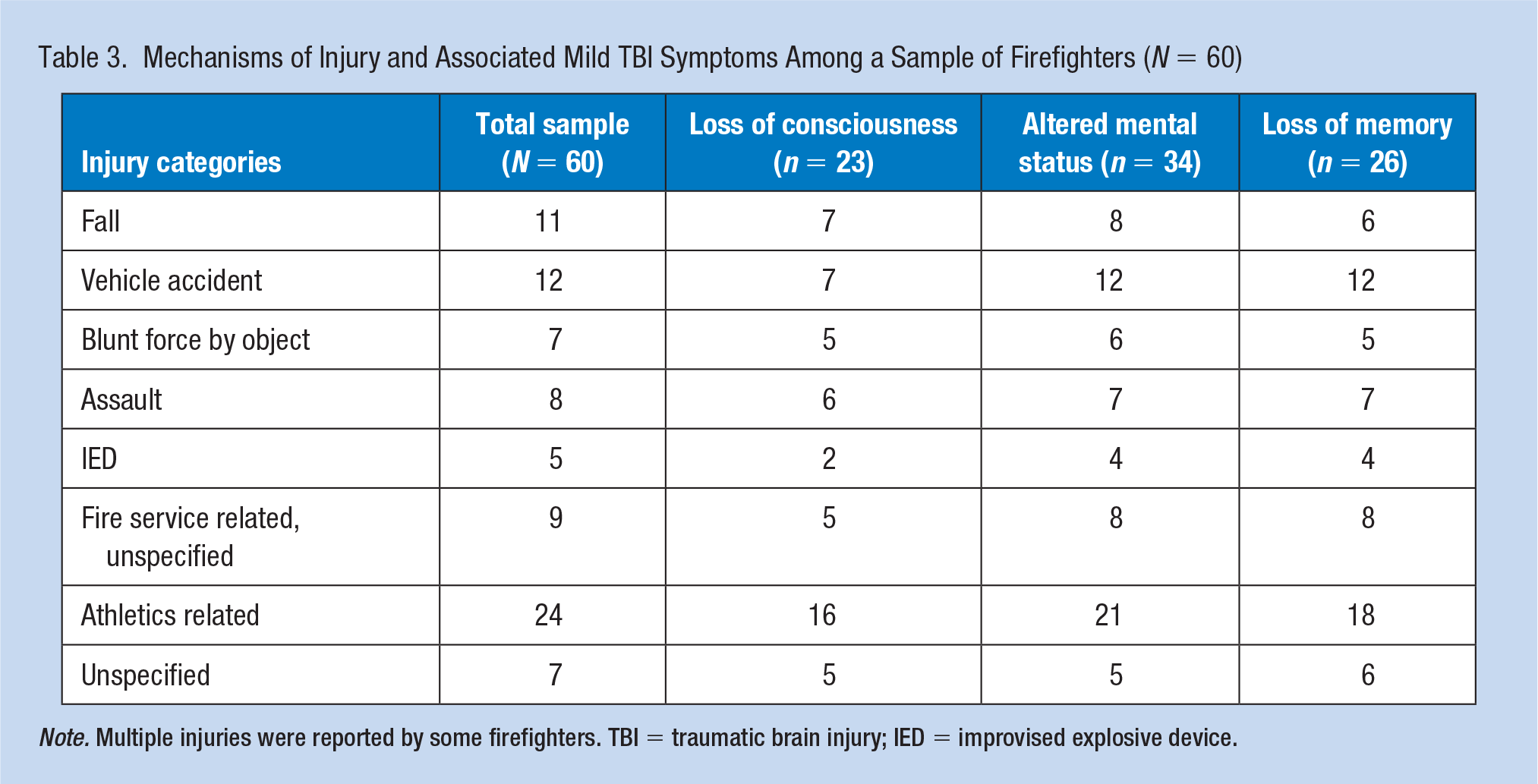
Note. Multiple injuries were reported by some firefighters. TBI = traumatic brain injury; IED = improvised explosive device.
Information concerning physical and mental health symptoms commonly associated with TBI was also gathered. These symptoms included headaches, dizziness, memory problems, concentration issues, recall difficulty, nausea, noise and light sensitivity, sleep disturbances, fatigue, blurred or double vision, and restlessness. Mood-related symptoms included irritability, depressive symptoms, frustration, stress, anxiety, and anger.
Of 45 firefighters who completed the RPQ, 20 (44%) reported at least one physical mTBI-related symptom after their head injury (data not shown). The highest reported symptoms were “feeling frustrated or impatient” (40%), “being irritable/easily angered” (35%), and “having poor concentration” (33%). In addition, there was a positive correlation between number of reported head injuries (M = 2.4, SD = 2.4) and depression symptoms (M = 3.1; SD = 3.0), as indicated by the BDI-PC (r = .36, p < .05).
Discussion
In this study of U.S. firefighters, the majority of participants reported at least one lifetime head injury and over half of their injuries met WHO mTBI criteria through endorsement of at least one associated mTBI symptom (e.g., confusion or disorientation, LOC for 30 minutes or less, or posttraumatic amnesia for less than 24 hours after injury). These findings are consistent with literature indicating that the second most common location of line-of-duty injuries is the head or shoulders (U.S. Fire Administration, 2016). Our survey allowed for a more accurate account of firefighter injuries by investigating details adjacent to injuries. Specifically, investigation of physical and mental health symptoms commonly associated with mTBI revealed that close to half of participants who endorsed a lifetime head injury also reported an mTBI-related physical symptom. Consistent with Bryan and Clemans’s (2013) investigation of cumulative head injuries and depression symptoms among military personnel, firefighters who endorsed more head injuries than their counterparts also endorsed more symptoms of depression.
This study was limited by several factors. As noted, some instruments (i.e., OSU TBI-ID, WARCAT-FF, BTBIS) were adapted for specific study purposes. Changes, such as in language or interview to self-report format, may have influenced information ultimately captured. In addition, some measures, such as the PCL-C which assessed DSM-IV rather than Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; APA, 2013) criteria, are now dated. Likewise, minimal data are available on firefighter health resulting in citations older than a decade being included. Hopefully, this article will serve as a resource for future research on firefighter health. Furthermore, firefighters with a positive mTBI history may have self-selected into the study ultimately skewing the data. The small sample size suggests our findings should be interpreted with caution. Some possible reasons for the low response rate to our survey include the length of the survey, the lack of a guaranteed stipend, and sending the recruiting email out to firefighters only once. Evidence suggests that sleep disturbances, which are common in the fire service, may exacerbate negative symptoms of injury (Bryant et al., 2010). Likewise, heat exhaustion symptoms overlap with mTBI symptoms (Scandella, 2012). These factors may represent confounding variables. Still, head injuries could occur simultaneously with heat exhaustion symptoms if the firefighter passed out due to these symptoms, hitting their head.
Sixty-two percent of the firefighter respondents reported meeting the symptom criteria for mTBI and 75% reported sustaining a head injury. Further research is warranted to capture the prevalence rate of mTBIs among firefighters and the relationship between mTBI and psychological symptoms among firefighters and other emergency-response personnel. Future research with larger sample sizes and in-person clinical diagnostic interviews may serve to clarify some of these questions.
Implications for Occupational Health Practice
Findings have clinical application for the diagnosis and treatment of firefighters. Symptoms such as feeling frustrated or experiencing sleep disturbances might be falsely attributed to a firefighter’s job; however, these problems might be better explained by a diagnosed mTBI condition. Similarly, depression symptoms may be due to multiple head injuries. If clinicians are aware that head injuries and mTBIs are common among firefighters, they will make more informed decisions when diagnosing firefighters.
The awareness of mTBI as a risk factor for firefighters allows occupational health professionals to adjust their injury and illness prevention program. The first step in reducing workplace mTBIs is to collect and evaluate existing information about workplace hazards (Occupational Safety and Health Administration, n.d.). Occupational health professionals should encourage firefighters to report workplace hazards that could result in mTBIs. The findings of this article are a preliminary step in evaluating the number of mTBIs firefighters report. This may aid in conducting cost–benefit analyses when implementing policies. Due to the implications of the study findings, it is important that occupational health professionals continue to monitor the research concerning firefighters with head injuries.
Applying Research to Occupational Health Nursing Practice
In total, 62% of firefighter respondents reported meeting the symptom criteria for mild traumatic brain injury (mTBI) and 75% reported sustaining a head injury. Clinicians should be aware of the prevalence of mTBI and head injuries among firefighters because it will allow them to make more informed decisions when diagnosing symptoms such as feeling frustrated or experiencing sleep disturbances. These symptoms might be falsely attributed to a firefighter’s job or other life circumstances; however, they may be better explained by diagnosed mTBI. Similarly, the awareness of mTBI as a risk factor for firefighters allows occupational health nurses to adjust their employer’s injury and illness prevention program. Occupational health nurses should encourage firefighters to report possible workplace hazards that could result in mTBIs.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a Research Mentorship Award (RMA) grant from Baylor Scott & White (150278) and approved by the Institutional Review Boards for the Protection of Human Research Subjects at Baylor Scott & White.
Author Biographies
Victoria A. Torres is a fourth-year clinical psychology doctoral candidate at the University of Mississippi. She has been involved in all aspects of the research project, beginning with procuring the research grant, developing the study, and writing the manuscript.
Jordan E. Strack is a research assistant at the Warriors Research Institute (WRI). She assisted with analysis and interpretation of data, manuscript writing, and managed the submission process.
Sara Dolan currently serves as an associate professor and Graduate Clinical Program Director in the Psychology and Neuroscience Department at Baylor University. Prior to her time at Baylor, she worked as a National Institute of Alcohol Abuse and Alcoholism–funded postdoctoral fellow and subsequently as a National Cancer Institute–funded faculty member at the Brown University Center for Alcohol and Addiction Studies. She served as a collaborator on the design of the assessment battery and consulted on multiple study aspects.
Marc I. Kruse is the staff psychologist for the Austin Fire Department and Austin–Travis County Emergency Medical Services. He is a licensed clinical psychologist who earned his PhD from the University of Texas at Austin and completed his clinical internship at the Center for Alcohol and Addiction Studies at Brown Medical School and the Providence, Rhode Island Veterans Medical Center. He contributed to initial study design, conception, and data collection.
Michelle L. Pennington is currently a program manager at WRI of Baylor Scott & White who has been instrumental in a variety of research projects examining topics, including suicide postvention in fire service and neuropsychological deficits in schizotypy. For the current project, she contributed to authorship of the Research Mentorship Award (RMA) grant, study design, and implementation.
Samantha J. Synett is a research therapist for the University of Texas Health Science Center at San Antonio, where she collaborates with both the Center of Excellence (CoE) in Waco, Texas, and STRONG STAR Research Consortium at Ft. Hood in Killeen, Texas. She was involved in initial study aspects, including study design and data management.
Nathan Kimbrel is a clinical research psychologist at the Durham Veteran’s Affairs Medical Center (VAMC) and an assistant professor in the Department of Psychiatry and Behavioral Science at Duke University Medical Center. He served as a collaborator during the initial phases of project development.
Suzy B. Gulliver is the director and chief of WRI and professor at the Texas A&M Health Science Center. She provided direct supervision to her mentee, Victoria A. Torres, throughout the research process.