
Abstract
Background:
Depression in the U.S. population affects approximately 17.5 million people, with an approximate annual economic cost of US$326 billion. The overall objective of this quality improvement program was implementation of a standardized screening protocol using a validated screening instrument to identify depression in first responders in a primary care setting.
Methods:
This program applied the Knowledge-to-Action framework utilizing the 9-question Patient Health Questionnaire (PHQ-9) screening tool. The outcome measure was screening completion with a process measure of depression questionnaires provided to patients, and balance measures of time of visit and referral rate. In a pre-/postintervention project design, clinic staff were trained on depression screening. PHQ-9 questionnaires were placed in all exam rooms for patients and providers to discuss. Referrals were made to the staff psychologist or to medical providers based on evaluations.
Findings:
From pre- to postintervention, screening increased from less than 1% to a screening rate of 92%. Appointments for depression intervention increased to 50%, 44 patients for counseling and 12 for medical therapy.
Conclusions/Applications to Practice:
A standardized screening protocol using a validated self-assessment tool improved depression surveillance and increased referrals for treatment. A training program with an accompanying policy was designed to sustain this program and may serve as a model for other programs serving first responders.
Keywords
Background
Depression affects approximately 17.3 million Americans annually and is one of the leading causes of disability in the United States (National Institute of Mental Health [NIMH], 2019). Costs for direct care and treatment, suicide-related costs, and workplace costs increased by 38% to an estimated US$326 billion over the past 10 years (Greenberg et al., 2021). Firefighters and other first responders suffer triple the rate of depression-associated symptoms such as substance abuse and suicide (Bartlett et al., 2018). Increased strain on personnel and the organization related to the COVID-19 pandemic highlighted behavioral issues for first responders and the general public. The purpose of this quality improvement project was to implement a depression screening process using a validated instrument consistent with national guidelines to better identify and treat first responders in the primary care clinic of a large urban fire department in a south Texas metro-area.
The Fire Service Joint Labor Wellness-Fitness Initiative (WFI; International Association of Fire Fighters, 2018) recommends prehiring behavioral screening for applicants and annual screening for incumbent firefighters. The U.S. Preventive Services Task Force (USPSTF) and Department of Veterans Affairs/Department of Defense (VA/DoD) guidelines also recommend screening in primary healthcare settings, noting that effective screening combined with psychotherapy, antidepressants, or both can significantly reduce morbidity (Siu, 2016; VA/DoD, 2022).
The city and fire department offers critical incident stress management (CISM), peer support, and short-term counseling through the employee assistance program (EAP), but these are self-referral programs and firefighters often avoid these programs due to cultural factors and perceived stigma (Johnson et al., 2019). Using Donabedian’s (2005) model to describe the problem, the department has a clinic structure to medically screen incumbent firefighters, emergency management services (EMS), dispatch, and other uniformed personnel at annual wellness exams. However, the workflow has not included a standardized process for depression screening treatment or referral (Figure 1). This gap in practice was an opportunity for improvement in early diagnosis and treatment for patients.
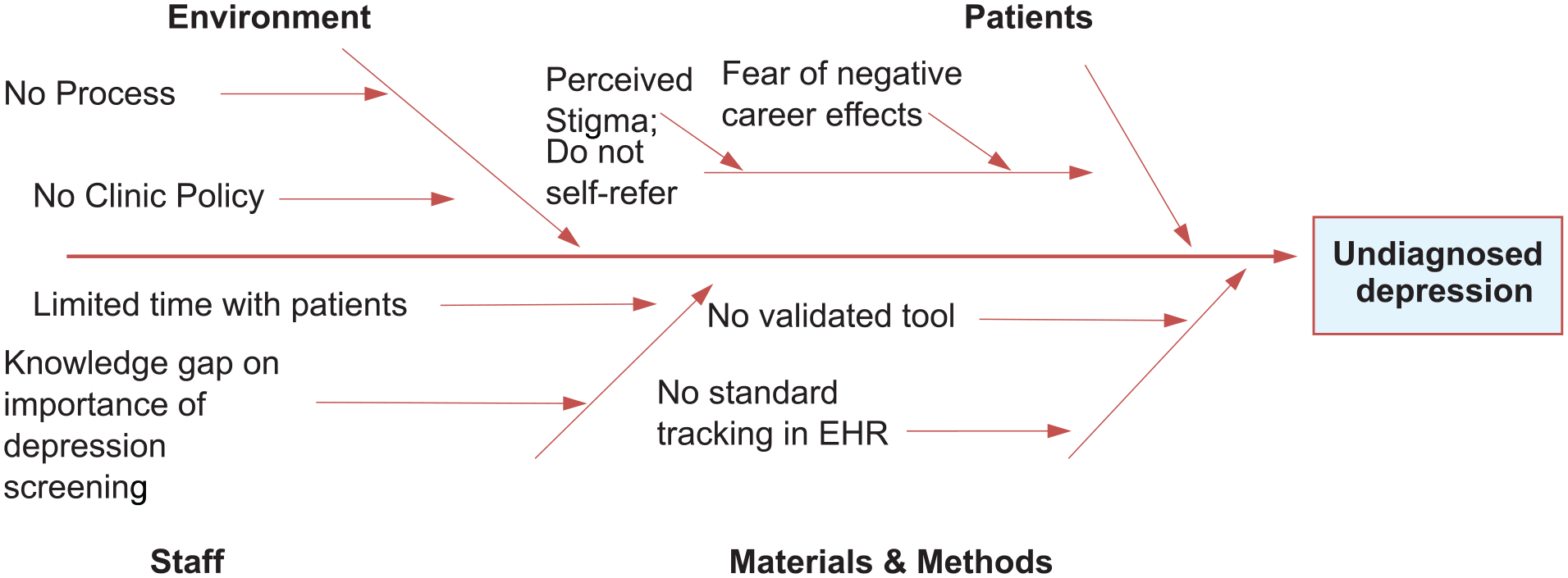
Gap analysis.
Best practice guidelines from the USPSTF and VA recommend screening all adult patients for depression in primary care settings (Siu, 2016; VA/DoD, 2022). The Wellness Clinic described herein had a gap in practice of undiagnosed and untreated depression. Wellness Clinic staff were not using a validated tool, nor utilizing existing electronic charting mechanisms, for depression screening. This presented a gap because first responders often do not recognize the need for behavioral health treatment, and self- and public-stigma-related concerns in the first responder population are significant. The literature shows this barrier to behavioral care is related to first responders’ fear of appearing weak or unable to handle the job and that seeking psychological services could adversely affect their careers. A related stigma described by Karaffa and Koch (2016) is pluralistic ignorance, which is workers’ underestimating their colleagues’ willingness to seek behavioral care. This perceived public and self-stigma was negatively correlated with attitudes toward seeking psychological treatment.
Depression rates in the U.S. population between 2010 and 2018 increased from approximately 15.5 to 17.5 million, an increase of 12.9%, with a 37.9% cost increase of US$236 to US$326 billion (Greenberg et al., 2021). Depression rates related to COVID-19 increased 19.3% in the U.S. population (Ettman et al., 2020) with even higher rates among healthcare workers (Li et al., 2021). Even before the COVID-19 pandemic, depression and conditions related to chronic stress in fire service such as posttraumatic stress disorder (PTSD), substance use, and suicide were prevalent (Martin et al., 2017; Stanley et al., 2018). Intense work conditions, physical demands, and work-related injuries combined with frequent exposure to intense emotional situations, human suffering, trauma, and death increase risk for behavioral health disorders (Paulus et al., 2017). For example, in a recent survey in this specific department, 161 firefighters responded to questions related to suicidal ideation. Of those, 11 individuals (approximately 7%) reported concerning levels of suicidal ideation. The same survey found between 11.7% and 16.2% of personnel expressed symptoms related to PTSD, more than 3 times that of the general population of 3.5% and slightly higher than other similar department rates of 10% (Paulus et al., 2017).
Anecdotally, firefighters have confided in providers that with increased stress and operational changes related to the COVID-19 pandemic, they increasingly use sick leave due to burnout rather than medical illness. Although specific numbers and causes for sick leave are not available due to patient privacy, this fire department human resource (HR) department found sick leave use increased by 16% from January 2019 to January 2020 and an additional 5% from January to October 2021.
Elevated risk of substance use related to depression is well documented. Risks of impaired driving related to substance use are also well documented (National Institute on Drug Abuse, 2019). Operating heavy vehicles and equipment in fire and EMS situations, providing acute medical care, and engaging in fireground operations while impaired increase risk to first responders and the public they serve. State law enacted as early as 1991, exposes the city as a self-insured entity, to potential liability from damages caused by impaired personnel (Texas Constitution and Statutes, 1991).
The purpose of this program was to enhance care through early diagnosis, treatment, and referral for depression. The main outcome of screening implementation was measured through comparison of patients seen for Wellness exams and the number of completed screenings. The goal was to achieve this through implementation of a screening process and collaboration between the staff psychologist, clinic providers, department, and union leadership.
Methods
A standardized screening protocol using a validated self-assessment tool was designed for universal depression screening in the clinic. Staff personnel were trained on use of the tool and steps to take for positive screenings. Measures of questionnaires provided, completed screenings, time of visit, treatment, and referral rates were assessed. A new clinic depression screening policy was developed and approved to sustain the program.
This improvement project incorporated depression screening into annual exams. The intervention began in early September through late October 2021. The improvement was sustained through follow-up training to increase knowledge of the PHQ-9 and steps to take when depression is identified. Following successful implementation, the change team developed a new clinic policy adding the behavioral component to the wellness exam and outlining steps for depression screening and referral.
The Knowledge to Action (KTA) Model of Translational Theory was used as a framework for this improvement project. The KTA was developed in 2006 to clarify various terms used to describe knowledge transfer from research to practice and address the gap between research and implementation in the clinical setting. It consists of two components, Knowledge Creation and Action Cycle (Graham et al., 2006). This translational theory was implemented with the Plan–Do–Study–Act (PDSA) model (Institute for Healthcare Improvement, 2021) to optimize implementation by mitigating barriers, implementing and evaluating the improvement, and revising the process. In the planning phase, focus group meetings were held to educate clinic staff and stakeholders on the screening protocol. Subsequent meetings evaluated measures, discussed problem areas, and made recommendations for adjusting processes to ensure successful and sustainable implementation. The change team moved through the Knowledge Inquiry stage of the KTA asking what behavioral issues affect firefighters and EMS personnel. Knowledge Synthesis revealed these personnel suffering 2 to 3 times the rate of the general populace. The identified problem was no depression screening protocol was in place (Figure 2).
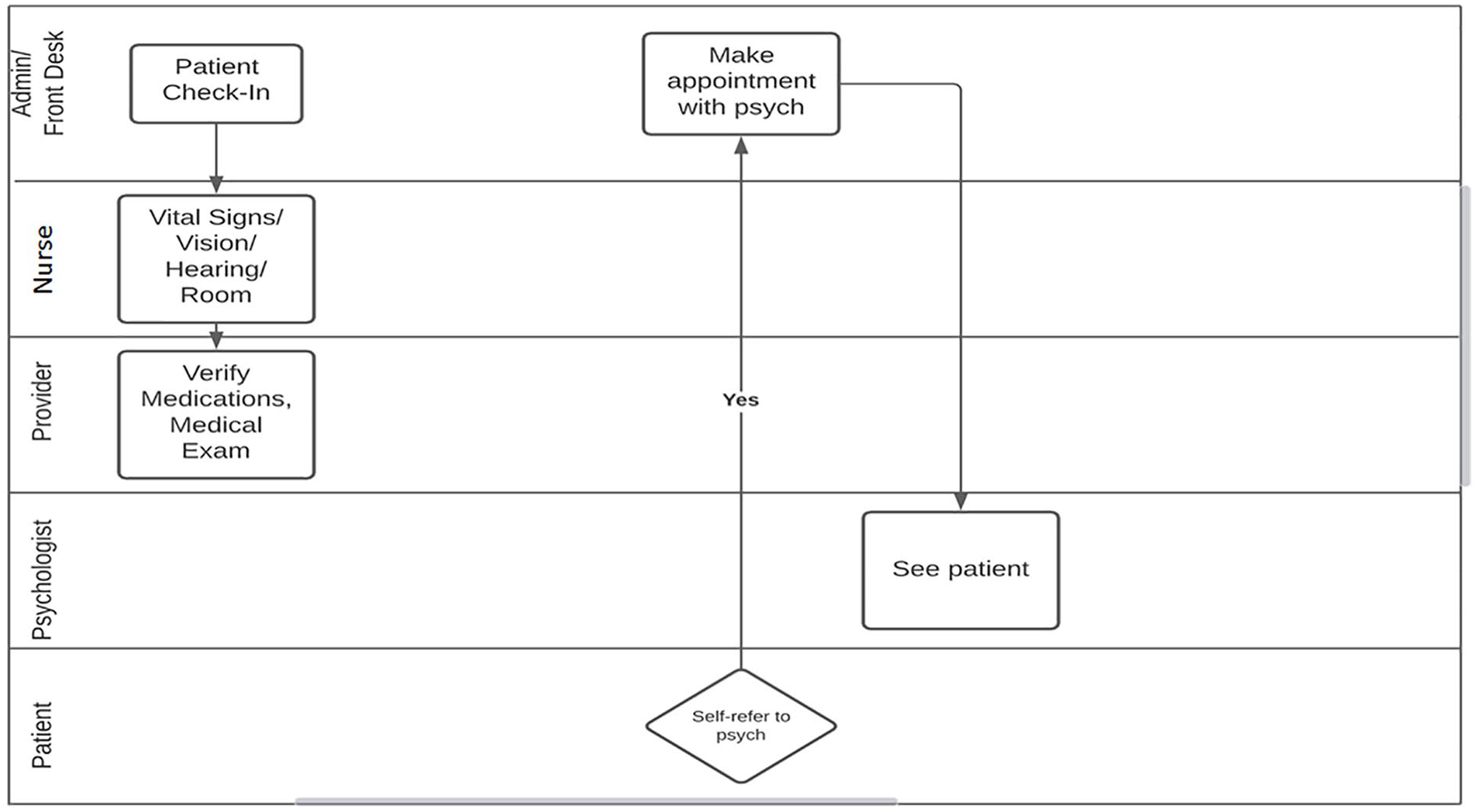
Preintervention workflow.
The 9-question Patient Health Questionnaire (PHQ-9) was selected as the tool to use for this universal screening for several reasons. This public domain tool is standardized (Kroenke et al., 2001; McCord & Provost, 2019) and validated and has a sensitivity of 88% compared with 72% for the 2-question Patient Health Questionnaire (PHQ-2), with increased specificity of 91% to 94% compared with 78% to 92% for the PHQ-2 (Gelenberg, 2017; Levis et al., 2020). The PHQ-9 has been successful in numerous settings (Parker et al., 2020; Sanchez et al., 2019; VA/DoD, 2022). Use of a validated instrument can assist in identifying previously undetected cases and facilitate early diagnosis of depression (Siu, 2016; Haugen et al., 2017) recommend routine, rather than symptom-based, screening to evaluate for depression among all first responders.
This quality improvement program implemented depression screening using the PHQ-9 to complement screening for vision, hearing, hypertension, diabetes, and other conditions. When rooming patients, the nurse handed them the questionnaire prompting them to complete it while waiting for providers. This gave the patient a quiet space, away from other crew members and co-workers, to fill out and score the form. Providers then discussed results and evaluated patient responses during the exam. If the patient had not completed the questionnaire by the time the provider arrived, the provider prompted them to complete. If the patient declined to complete the questionnaire, the provider attempted to conduct a depression assessment verbally following the PHQ-9 format. Following the exam, providers gave the completed questionnaire with the rest of the chart to the administrative assistant where she separated the questionnaire and scanned the rest of the note into the patient’s electronic medical record (EMR). Questionnaire completion and provider evaluation were core aspects of this project. Completed screenings were placed in a folder for weekly count by the clinic manager; numbers were aggregated into a password-protected spreadsheet and the screening questionnaires were destroyed once tallied. All measures were analyzed and presented using run charts.
Patients diagnosed with depression based on a PHQ-9 score of 10 or above; based on a positive answer on Question 9, which screens for suicidal symptoms; or based on discussion with providers could be referred at the end of the visit. Administrative staff made the referral appointment with the staff psychologist or the patient could schedule later. If patients were identified with depression, further testing for PTSD or other comorbid conditions could be administered by the staff psychologist using the PTSD Checklist for Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013; PCL-5). Similar interventions were described by Robertson (2019), but the tool used in this program was modified from the PCL-5 used by Robertson, which specifically screens for PTSD, to the PHQ-9 that has a broader scope. Another adaptation for this context was for patients to be screened during their annual physicals rather during continuing education blocks or specified behavioral health sessions, which was thought to reach as many personnel as possible and decrease stigma. A QR code was created providing contact information for the psychologist so patients could save it in their phones if they wanted to schedule at a later time. Primary development of the intervention was a collaboration between the project lead, staff psychologist, and the executive sponsor with approval from the project mentor. In the KTA monitoring step, the primary outcome measure was screening completion rates. The first process measure was the number of patients seen for Wellness exams provided with a questionnaire and opportunity to complete it. Balance measures were length of visit and number of referral appointments. The KTA evaluation step compared the number of patients seen against the number of completed depression screenings to assess effectiveness of the intervention. In the revised workflow, depression screening was incorporated into the existing screening process, with patients treated or referred as appropriate (Figure 3).
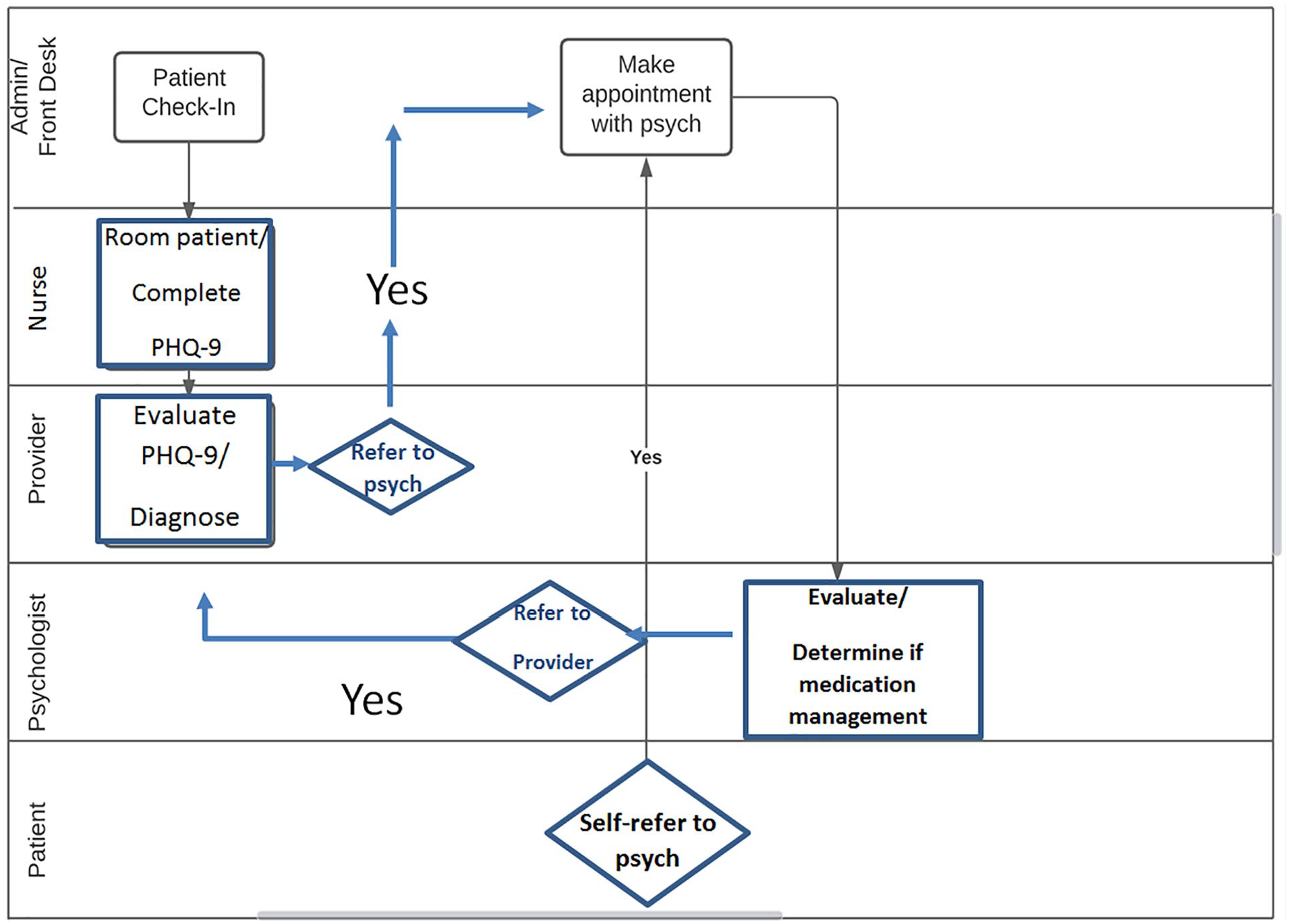
New workflow.
Prior to implementation, the change team planned a training program to assess level of knowledge of depression screening, the PHQ-9, and staff confidence in its use based on Kirkpatrick’s Evaluation Model (Reio et al., 2017). First, staff completed a pretraining quiz to assess knowledge of depression, how to administer the PHQ-9, and actions to take for positive screenings. On the pretraining quiz, staff answered 53% of the questions correctly regarding first-responder rates of depression, depression screening guidelines, and knowledge of the PHQ-9. Following the quiz, the change team conducted a short in-service training on the purpose of screening in this population, characteristics of the questionnaire, and actions to take with positive screenings and crisis situations. Following this, a posttraining quiz was conducted to assess knowledge and correct responses increased to 93%. A posttraining survey was emailed to staff members to determine their perspective on relevance of depression screening and knowledge of how to conduct screening and follow-up. One hundred percent of the staff responded that training on the PHQ-9 was highly relevant to their job and 100% responded that the training would greatly impact their practice or clinic operations. Sixty percent of the staff felt highly confident while 40% felt somewhat confident in using the PHQ-9 as a tool to screen for depression. Similarly, 60% felt highly knowledgeable in what actions to take if the PHQ-9 was positive or the patient showed signs of depression while 40% expressed that they had some knowledge. Based on these results, the change team plans to have a retraining session with a question-and-answer portion as a sustainability effort.
Implementing depression screening using the PHQ-9 progressed as intended. Clinic staff completed training and questionnaires were placed in exam rooms. When rooming patients, the LVN handed patients a clipboard with the PHQ-9 asking them to complete the questionnaire while waiting for the provider. At the end of the first day of implementation as part of the PDSA cycle, the change team discovered that not all questionnaires had been completed. The change team held a short meeting to determine the cause of the discrepancy. A process problem of questionnaires being placed in only three of four exam rooms led to not all patients being offered the opportunity to complete the PHQ-9. Once the change team discovered this, the team acted by adding questionnaires to the other exam room and this issue was easily rectified. As implementation continued, the team continued to study the change and found a high frequency of positive answers on the PHQ-9 regarding sleep disruption and energy levels. When evaluating these answers with patients during the exam, providers found sleep disorder and decreased energy were often correlated with shift-work sleep disorder, possible sleep apnea, or both rather than symptoms of depression. The team made another modification to the process by integrating a follow-on screening for sleep disorder, the Epworth Sleepiness Scale (Johns, 1991) to assess daytime sleepiness and possible referral for sleep study. The change team studied possible barriers to this addition, namely, increasing time to the overall exam and found that it would be minimal. After studying aspects of the possible interaction of sleep and mood disorders, particularly in this population (Johnson et al., 2019; Jones, 2017), the team acted and modified the process. Numerous patients were referred for sleep studies and treated for sleep disorder as a result. As implementation continued, the change team conducted another PDSA cycle finding that some patients were hesitant to being referred to the staff psychologist at the time of the Wellness exam. After studying this potential barrier, the team developed and added a QR code with the staff psychologist’s contact information for easy reference should patients decide to self-refer.
As expected, a small number of patients declined to complete the questionnaire citing privacy concerns and potential adverse effects on their careers. For these patients, providers asked about symptoms of depression related to work or home lives, sometimes verbally following the question format of the PHQ-9; these were not counted as there was no documentation of the screening being completed.
Because the focus of this project was to improve staff processes through implementation of a screening protocol rather than on patient-centered outcomes such as prevalence of depression, effectiveness of treatment, or other individual characteristics, this program was classified as nonregulated research and patients were not required to provide informed consent by the institutional review board.
Findings
Preintervention data were collected over a 3-month period from June 1, 2021, to September 3, 2021, and included 320 patients. The postintervention cohort included 194 patients in the clinic from September 6, 2021, to October 22, 2021. Missing data included those patients who did not complete the form for any reason, approximately 8%.
The primary outcome measure for this QI project was 90% completion rate of depression screening for this first-responder population. The unit of analysis was completed PHQ-9 questionnaires. Overall screening completion rate in the postintervention cohort was 92% (179/194; Figure 4), exceeding the goal of formally and systematically screening patients for depression.
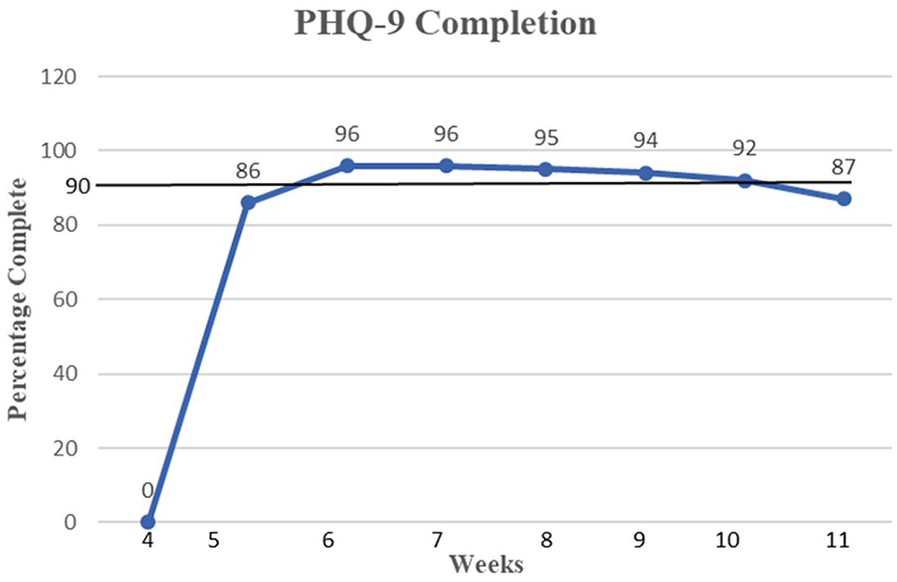
Screening completion rate.
The process measure for this project was for questionnaires to be provided to all patients. For universal screening to be accomplished, all patients had to be given the opportunity to complete the questionnaire. Of the 37 patients who came for exams in the first week, two patients were not provided with the questionnaire due to the exam room not being equipped with a clipboard and copies of questionnaires. This was remedied the following day by adding questionnaires to all rooms and, following this, 100% of patients were given the opportunity to complete the PHQ-9.
The first balance measure tracked average visit time to determine whether additional time should be allotted for future Wellness visits. The change team expected average visit time for all providers during implementation to increase compared with the prior 3 months. In the 3-month preimplementation period, average visit time was 35 minutes and did not change over the course of implementation (Figure 5).
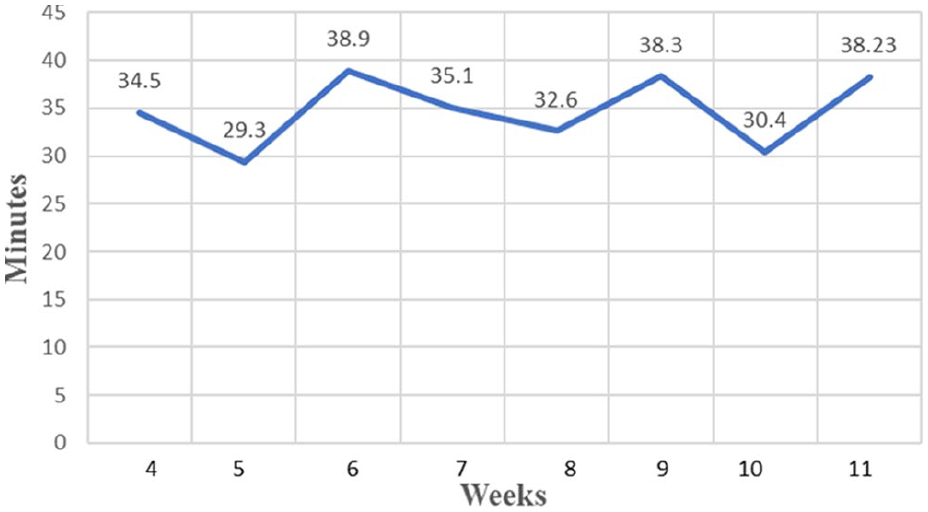
Average visit time.
The change team’s second balance measure unit of analysis was the number of appointments specifically for depression seen by the staff psychologist and clinic providers. An increase was expected as patients were diagnosed and referred for therapy or medical treatment. The balance measure was assessed by comparing the number of appointments the staff psychologist saw for depression before and during the intervention. The number of medical provider office visits for depression either self-referred or referred by the staff psychologist prior to and during implementation was also counted. Referrals were assessed monthly and provided to the project lead. In the preimplementation of June 1, 2021, to September 3, 2021, medical providers saw a total of two patients for depression. In the same period, the staff psychologist averaged 26 appointments for depression per month. During the implementation period of September 6, 2021, to October 22, 2021, the staff psychologist saw 44 patients for depression and medical providers had 12 patients referred for medication therapy. This marked increase may have been related to the line-of-duty death of a firefighter in the department but nevertheless illustrates the need for depression screening and treatment.
Discussion
The purpose of this quality improvement project was to implement a depression screening process using a validated instrument consistent with national guidelines to diagnose and treat first responders in a primary care clinic. Significant barriers to the project were thought to be stigma, followed by potential for increased time per visit, and increased visits for the psychologist and other providers.
Preintervention data were collected over a 3-month period from June 1, 2021, to September 3, 2021 and included 320 personnel. The postintervention cohort included 194 patients presenting to the clinic from September 6 to October 22, 2021. The primary outcome of overall screening completion rate in the postintervention cohort was 92% (179/194), exceeding the goal of 90%. One hundred percent of patients were given the opportunity to complete the questionnaire and to be screened. There was no increase in exam time. There was an increase in the number of patients seen by the staff psychologist and medical providers specifically for depression. Strengths of the project include effective integration of the validated screening tool and high screening completion rate. Success in implementing this screening protocol was largely due to stakeholder buy-in and minimal cost to providers or clinic staff. Fire department leadership and clinic staff were willing to include a mental health component to employment physicals and are studying more programs to improve care for related comorbidities.
The screening protocol incorporated an evidence-based self-assessment tool that was successfully integrated into the clinic workflow in a primary care setting. Using this protocol, the rate of first responders screened as well as those screening positive for depression increased as expected. Although some patients opted not to complete the questionnaire or be screened, this number was small in contrast to significant barriers such as stigma and fear of career repercussions described in the literature (Johnson et al., 2019; Karaffa & Koch, 2016). These findings are consistent with a similar QI project by Robertson (2019).
Based on the increased number of patients seen for depression by the staff psychologist and medical providers, the impact of this project was significant to this fire department and might be expanded to include screening during routine office visits or follow-up appointments at this site. Costs in money and exam time were not burdensome. Opportunity cost of not incorporating PTSD or substance abuse screening was offset by the broader scope of the PHQ-9 and the ability to screen for those comorbidities when patients were seen by the staff psychologist. Screening for specific comorbidities might be included with Wellness exams in the future based on success of this project.
Results of this QI project suggest clinical significance. The efficiency and low cost of the protocol to diagnose and treat patients with this harmful disorder are persuasive. This improvement will be sustained through planned training to increase knowledge and competence with the PHQ-9, actions to take when patients screen positive, and actions to take when patients are in crisis. Higher than expected completion rate opens possibilities for integration in other settings serving first responders and other occupational settings. Positive implications for first responder populations and the public in diagnosing and treating a disorder with such high economic, health, and well-being costs are substantial. Further projects could include measuring positive screening rates over time to see whether integrating screening with collaborative treatment results in decreased positivity rates.
Another potential use for this screening could be to evaluate answers to specific questions in the PHQ-9 to address specific disorders. One pattern that emerged during the project was the high rate of positive answers for Question 3 focusing on sleep. Many patients reported poor sleep even on off-shift days. Focus on sleep as a component of overall mental health might be a focus of future projects.
Next steps to build on this project might be integrating the screening tool into the EMR, potentially using an electronic tablet to complete the questionnaire, automatically calculate, and upload results. This could streamline the screening process, reducing time for assessment and potential for mistakes in counting and tracking. The significantly increased rate of appointments seen by the staff psychologist specifically for this disorder may justify hiring an additional psychologist to address this need. The change team is currently working with leadership to apply for a federal grant to offset the cost of an additional psychologist. We are also investigating funding through county or state agencies, partnership with the significant military presence in this city, or public–private partnerships.
Limitations of the project included a narrow timeframe and relatively small clinic size. With only a 2-month implementation period, long-term benefits are difficult to assess. The limited number of providers also makes generalization difficult. In addition, because patients may self-refer, it is not known whether the increase in appointments for the staff psychologist is a direct result of increased screening. The rate of patients screening positive was not measured as the focus of this QI project was staff processes rather than patient outcomes.
Applications to Professional Practice
Depression and conditions related to chronic stress in fire service such as PTSD, substance use, and suicide are prevalent with firefighters suffering rates of depression of approximately 11% compared with rates in the general population of about 5.4% (Martin et al., 2017; Stanley et al., 2018). This professional practice innovation implemented depression screening in a Wellness Clinic serving firefighters. Employing a standardized process with validated tools for screening mental health disorders should be done during exams in clinics serving first responders. Due to the prevalence and significance of the problem with potential for patient comorbidities, potential liability to the city, and degraded service to the public, this improvement is a worthy investment in people and the organization. Not doing so carries increased risk of reduced productivity, potential for physical and mental injuries, and significant costs to cities and healthcare systems.
Supplemental Material
sj-docx-1-whs-10.1177_21650799221119147 – Supplemental material for Depression Screening Implementation: Quality Improvement Project in a Primary Care Clinic for First Responders
Supplemental material, sj-docx-1-whs-10.1177_21650799221119147 for Depression Screening Implementation: Quality Improvement Project in a Primary Care Clinic for First Responders by Canaan Blake in Workplace Health & Safety
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.