
Abstract
Background: Injury and illness incidence rates continue to be higher in healthcare facilities than in the manufacturing environment despite improvement efforts implemented by various organizations. The prevention of workplace injury and illness is a challenge for facilities due to reasons including exposure to body fluids, infectious diseases, and patient handling activities. The purpose of this project was to reduce workplace safety-related incidents and prevent employee injuries through leadership involvement in employment of preventive, directive, and corrective controls. Methods: A tertiary medical center in California experienced 114 accepted injury claims in 1 year. As a response to the problem, the medical center developed a safety management system consisting of a process for engagement between leadership and staff members/employees to increase accountability and reduce injury risks. Findings: The medical center achieved a 59% reduction from 114 to 67 injury claims over a period of 2 years and a two-point increase in engagement scores from both leaders and staff members. Conclusion/Application to Practice: The development of a safety culture starts with leadership behavior, establishment of clear safety processes, and hazard mitigation activities. Workplace safety is a shared responsibility between frontline staff managers and leadership within an organization. Senior leaders must serve as role models to promote a speak-up culture to support safe work practices.
Keywords
Background
According to the Bureau of Labor and Statistics, U.S. Department of Labor (2018), there were 2.8 million nonfatal workplace injuries and illnesses reported by private industry in 2017, and 51,380 of which were cases reported by hospitals resulting in days away from work (Bureau of Labor and Statistics, U.S. Department of Labor, 2018). Nursing assistants and nurses had the highest injury rates, related to patient handling and workplace violence, of all occupations as reported by 112 facilities participating in the Centers for Disease Control and Prevention’s (CDC) Occupational Health Safety Network (OHSN) from January 1, 2012 to September 30, 2014 (Gomaa et al., 2015). Hospitals reported an injury and illness incidence rate of 129.8 cases per 10,000 full-time equivalent (FTE) workers in 2017 compared with 93 cases per 10,000 FTE workers in the manufacturing industry (Bureau of Labor and Statistics, U.S. Department of Labor, 2018). In addition, there were 4,674 injuries related to patient handling and movement reported to the OHSN from 2012 to 2014, equivalent to a rate of 11.3 incidents per 10,000 worker months, and lifting equipment was not used in 51% of the reported patient handling incidents (Gomaa et al., 2015). Studies have shown that increased access to ceiling lifts and other patient handling equipment improves efficiency and is directly related to a decrease in incidence of musculoskeletal disorders (Enos, 2018). California’s safe patient handling regulation requires every hospital to have adequate equipment available for safe patient handling, have a robust training program, and review the plan annually (California Department of Industrial Relations, 2016). Every employer is held responsible to comply with the Occupational Safety and Health Act of 1970 and may be held legally liable for employee sufferings due to violation of the Occupational Safety and Health Administration (OSHA) standard (Pozgar, 2016). As of January 2018, the penalty fine is US$12,934 per violation and US$129,336 per willful violations (OSHA, 2018). Organizations are also at risk of criminal litigations if a willful violation due to lack of prevention, despite knowledge of risks, result in an employee’s death. The criminal penalty for a willful violation of OSHA was amended to be punishable by fines up to US$500,000 for organizations (Conn & McMahon, 2016).
Nursing and residential care facilities continue to have the highest incidence rate of workplace injuries and illnesses despite safety initiatives that are currently in place (Bureau of Labor and Statistics, U.S. Department of Labor, 2019). According to a Northern California (NCAL, 2016) hospital system’s workplace safety report, one of its facilities experienced as high as 114 injury claims in a period of 1 year from October 2015 to September 2016, at a rate of 10 injuries per 1,000 employee productive hours (NCAL, 2016). Although the injury claims decreased to 93 occurrences the following year, the continued high injury rate is costing the organization between US$3.6 million and US$4.4 million for both direct and indirect costs using an estimated cost of a medically consulted injury claim at US$39,000 per claim (National Safety Council, 2019).
Workplace injuries continue to pose challenges to healthcare organizations. Although hospitals have reduced the rate of worker injuries over time, construction and manufacturing industries have surpassed the improvements made by hospitals (OSHA, 2013). There are unique hazards inherent among healthcare workers and those who work in a hospital setting. These hazards contribute to an increased risk for injury and illness. Some of the hazards include exposure to infectious medical conditions and contaminated sharp instruments and devices, lifting and repositioning patients, and caring for violent and combative patients (Bureau of Labor and Statistics, U.S. Department of Labor, 2019). These unique circumstances led multiple national groups and associations to learn more about contributing factors and promote safe practices for healthcare workers.
McCaughey et al. (2016) used the modified National Institute for Occupational Safety and Health (NIOSH) framework to analyze findings, specifically the organization of work that includes both management or supervisory work practices and work design. The authors endorsed the use of the NIOSH framework in the identification of antecedents to injuries so organizations can link their safety programs to injury prevention approaches and leaders can support the development of safety structures and facilitate performance improvement initiatives surrounding workplace safety.
It has been shown that organizational and supervisory support play an important part in the prevention of workplace injuries and promotion of worker safety. Tveito et al. (2014) emphasized the importance of having a nurturing and supportive working environment and better organizational practices and policies to reduce injuries and disability costs for nurses. An analysis of the nursing assistant survey showed that employee training on safety practices is not enough to prevent injuries, and that supervisor support and employee engagement have an indirect relationship with injury incidence in the nursing assistant group (McCaughey et al., 2014). Peer feedback, combined with supportive empowerment and adequate training on equipment use, has been proven to reduce injury rates (Cortez et al., 2017). In fact, the direct relationship between ethical leadership and occupational safety outcomes is apparent in high-reliable organizations (Freiwald et al., 2015). For example, the relationship between an organization’s ethical climate and its employees’ safety motivation or engagement is one that can be changed and influenced positively by the organizational leaders.
Leadership behavior is important in transforming the culture through role-modeling of safe behaviors and deliberate actions. A cross-sectional survey conducted in Belgium revealed that transformational leadership had a positive impact on nurses’ safety practices and compliance with safety (Lievens & Vlerick, 2014).
In 2011, the NIOSH launched the Total Worker Health (TWH) Program. This program combines policies, programs, and safe practices to integrate job hazard mitigation, and illness and injury prevention (CDC, 2018). It emphasizes the importance of a consistent process for job hazard identification and oversight to promote and support personal and departmental safety.
The Harvard Chan School Center for Work, Health, and Well-being developed the Workplace Integrated Safety and Health (WISH) assessment, which is an instrument to measure an organization’s workplace policies and programs that includes six constructs, namely, leadership commitment, participation, policies and programs that foster supportive working conditions, comprehensive and collaborative strategies, adherence, and data-driven change (Sorensen et al., 2018). The purpose of this project was to reduce workplace safety–related incidents and prevent employee injuries through leadership involvement in employment of preventive, directive, and corrective controls.
Methods
The continued high rate of workplace injury at a northern California medical center posed a risk to the organization and a challenge for the leadership team. This project aimed to utilize evidence-based risk mitigation strategies to decrease its worker injury rate of 10 injuries per 1,000 productive hours in 2016 by at least 20% to eight injuries per 1,000 productive hours by the end of performance year 2018, from October 2017 to September 2018. The high-risk departments in the medical center, including environmental services, inpatient nursing departments, and perioperative departments, were asked to participate in current assessment and action planning to improve workplace safety and reduce the incidence of the top 3 injuries: overexertion, contact with objects, and patient handling.
To achieve The Joint Commission’s (2012) goal to promote patient and worker safety, the medical center embarked on a safety journey to assess its risks and other antecedents to workplace injury. Table 1 describes short-, medium-, and long-term workplace safety risks across risk categories such as financial, infrastructure, reputational, and risks within the market place. One of the initiatives implemented by the facility was the consistent and thoughtful completion of job safety analysis (JSA) tools for every employee in each job category within the workplace.
Workplace Safety Risks
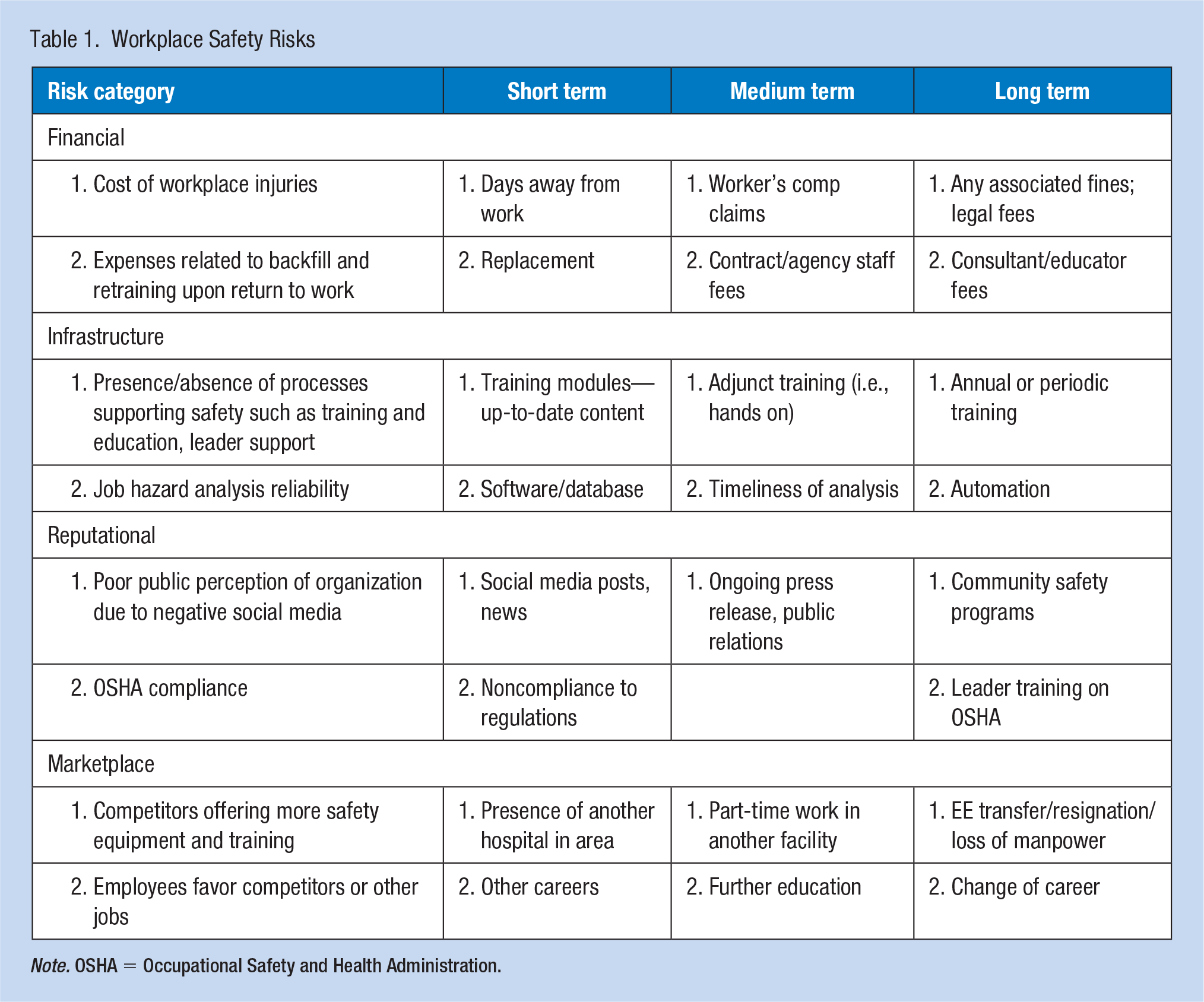
Note. OSHA = Occupational Safety and Health Administration.
The previous process of JSA completion was inconsistent and not purposeful. There was no engagement from the employees and the hazards identified were generalized to a larger population rather than specific to the department’s risks and environmental factors. The JSA tools were made available in the medical center’s intranet site and were preloaded with set templates based on common tasks performed and associated hazards. There was also an option to customize the tool and add department-specific mitigation activities. Managers identified potential job hazards and discussed mitigation and prevention activities with each employee. In turn, the employees’ acknowledgment of known risks heightened their awareness to safe practices.
The newly implemented process engaged employees by having them help identify their own job hazards and develop action plans to decrease or eliminate them. Employee engagement was reflected in the employee satisfaction survey administered in the medical center 3 months after implementation of new standards and structures for workplace safety.
In addition, the employee health and safety department, in partnership with an ergonomist, assessed the work environment for each job category to help identify ergonomic-related injury risks and eliminate them. Prevention of accidents and injuries was important in promoting the morale of staff and improving productivity.
The previous training schedule was scheduled once a year, typically in October, to capture all employees. This annual training schedule created gaps. For purposes of this project, the medical center put directive controls in place specific to safe patient handling trainings. There was a regular cadence of training sessions offered weekly and all direct care staff members were required to attend each year near or prior to their annual performance appraisal dates. Leaders and educators leveraged the safety trainings to highlight policies and procedures on ergonomic principles, proper use of personal protective equipment and safe patient handling equipment, stretch exercises, and risk identification and injury prevention. The clinical education department and workplace safety champions partnered together and provided training sessions to all direct care staff.
The medical center instituted corrective controls that were exercised either after an incident had occurred and root causes had been identified or as a proactive intervention when risks were recognized. For example, environmental service workers used visual signs and pop-up cones to caution staff of wet floors or presence of biohazard or noxious substance. All frontline staff members were required to use personal protective equipment and safe patient handling equipment with every patient mobility task, and the manager ensured the rotation of staff assignment for fair distribution of work and to prevent continuous exposure to physical activity and repetitive motion. The inpatient units assessed safe patient handling equipment inventory to inform purchase of additional equipment as needed, resulting in the testing and purchase of additional bed repositioning sheets. In 2017, ceiling lifts had been installed with the goal of increasing convenience and easy access to the lifts; leaders reinforced use of the lifts through additional trainings offered in 2018.
The medical center conducted several safety stand down events where senior leaders came to various units during department huddles and had engaging conversations with staff members on topics such as high hazard activities, safe practice of pausing, planning, and preparing, and speaking up for safety. All leaders, including the executive chiefs, incorporated daily and weekly department safety rounds as part of their standard work and documented them in the medical center’s rounding intranet site. In addition to department rounds, leaders came together every morning for a safety briefing where safety issues were raised for the past 24 hours with the goal of raising staff awareness.
Both outcome and process measures were monitored to determine progress and opportunities for improvement. The reported injuries, both first aid only and injury claim, were monitored as outcome measures. The rate of injury was defined as the number of accepted injury claims per 1,000 productive labor hours occurring in the performance year for 2 years from October 2016 of the previous calendar year to September 2018.
Findings
The baseline performance used for the improvement project was the number of employee injuries from 2016 to 2017, with a total of 114 injury claims at a rate of 10 injuries per 1,000 productive hours. The injuries ranged from being struck by an object, needlestick or sharps injuries, eye splash, muscle strain due to material or patient handling, and slips/trips/falls.
The medical center also monitored process measures such as employee peer-to-peer safety conversations, occurrences of leader safety rounds, JSA completion rate, and documented use of safe patient handling equipment. The employee safety conversations and leader rounds are reported through the medical center’s database and have exceeded the target of 85% for safety conversations and 90% for leader rounds every month for the past year. The medical center’s current JSA completion rate was at 93% as of May 2019, compared with a 45% completion rate in May 2018. Improvement in employee engagement as evidenced in the employee satisfaction survey was represented by a two-point increase in the employee engagement scores in comparison with baseline. Finally, the electronic medical records showed a 175% improvement of documentation of equipment use to 74% in April 2019, compared with 27% in March 2018.
At the end of performance year 2018, the medical center was able to reduce its incidences of injury claims to 67 and decreased the rate to 8.9 injuries per 1,000 productive hours. The first quarter results for 2019 showed a total of 14 injury claims at a lower rate of 6.6 per 1,000 productive hours.
Discussion
The promotion of workplace safety in this medical center started with leadership commitment and support for a speak-up and safe culture. The reduction in workplace injuries was realized once leadership efforts were put in place to implement combined preventive and corrective actions addressing identified risks over a period of time. The leaders modeled safe behaviors through safety messages and reminders and purposeful safe actions. The result trend only included 2 years of data and will need to be monitored to ensure sustainability. In the meantime, the heightened awareness of all employees and leaders to existing job hazards was a change in mind-set reflective of the developing safety culture and values.
Some of the key challenges in the culture change journey included leadership turnover in multiple departments, which led to inconsistent processes for hazard identification and mitigation, and employee training on safe practices. Leader standard work is a phrase that describes a set of established and routine tasks where managers and supervisors engage in proactive work to improve processes in the department, mitigate risks, and support the frontline staff members rather than troubleshoot issues. The lack of leader standard work played a role in the reactive practices rather than proactive and preventive actions. The leaders were engaged in non-value-added tasks and had daily variation in schedules. The development of leader standard work allowed for coaching time by leaders and rounding on the departments to meet and coach frontline staff.
Conclusion
An engaging transformational leader who shares a vision of safety will attract followers who ultimately develop a sustainable commitment to injury and accident prevention.
Employee engagement, together with leadership behavior, was necessary in upholding a culture of safety. Peer-to-peer conversations and feedback also a role in fostering safe behaviors and promoted a speak-up culture where everyone is encouraged to stop the line and speak up if they feel that safety of the patient or a coworker may be compromised.
Development of a safety culture leading to decreased patient harm and decreased worker injuries was the result of a united vision and the collaborative work between leaders, managers, and frontline staff members. The role of the executive leader was vital in shaping the future of safety in every organization through role-modeling and positive reinforcement.
One characteristic of a highly reliable organization was its preoccupation with failure, where every employee thinks of ways their work processes may break down so this breakdown can be prevented. This trait compels leaders, managers, and frontline staff to constantly look for risks and mitigate them before an accident occurs. Safety must be ingrained in the organization’s culture where it serves as the driver of every deliberate activity. Leadership was key to this goal.
Applications to Professional Practice
Promoting a culture of safety is the responsibility of every member of an organization. Leadership behavior and employee engagement are key in supporting safety processes and sustaining results. Identification of risks and prevention of injury are important in the field of occupational health and environmental nursing. It is crucial for organizations to focus efforts on the reduction of injuries experienced by healthcare workers. This improvement project addressed how one medical center dedicated resources to make employee safety a priority and understand that results are obtained over a period of time. It is important for the leadership team to set a realistic target and support managers and frontline staff members in achieving this targeted goal.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.