
Abstract
Background: Percutaneous injuries and blood-borne-related infections pose occupational hazards to healthcare professionals. However, the prevalence and associated factors for these hazards among midwives in Hunan Province, China are poorly documented. Methods: A cross-sectional study was conducted among a sample of 1,282 eligible midwives in the cities of Yongzhou, Chenzhou, Hengyang, and Changsha in Hunan Province, China, from January 2017 to July 2017. The association of selected independent variables with percutaneous injuries was investigated using binary logistic regression. Results: 992 participants responded (77.3%), and within the previous 12 months, 15.7% experienced percutaneous injuries. In multivariate analysis, hospital size, age, length of employment as a midwife, weekly working hours, and three aspects of Hospital Safety Climate Scale were associated with percutaneous injuries. The risk of percutaneous injuries among the midwives working in hospitals with ≤399 beds was higher than that among those working in hospitals with ≥400 beds by nearly 3 times. Furthermore, the percutaneous injury prevalence of midwives decreased as age increased. Moreover, the probability of percutaneous injuries among the midwives with weekly working hours of >40 was 4.35 times higher compared with that among midwives with weekly working hours of ≤40. Conclusion/Application to practice: The prevalence of percutaneous injuries among midwives in the study hospitals was substantial. Our results further proved that risk mitigation strategies tailored to midwives are needed to reduce this risk. These strategies include ensuring a positive organizational climate, providing highly safe devices, and reducing the workload.
Introduction
Healthcare workers have a high risk of exposure to blood-borne pathogens, such as hepatitis B virus (HBV), hepatitis C virus (HCV), and human immunodeficiency virus (HIV), which together account for a vast majority of occupational infections (Adams, 2012). The estimated annual proportion of healthcare workers exposed to blood-borne pathogens, namely, HCV, HBV, and HIV was 2.6%, 5.9%, and 0.5%, respectively, with the majority of exposures occurring in developing regions (i.e., percutaneous injuries accounts for 40%–65% of HBV and HCV infections in healthcare workers in developing regions) (Aspinall et al., 2011; J. H. Lee et al., 2017). Furthermore, it was recently estimated that almost half of the healthcare workers in Africa were occupationally exposed to blood-borne pathogens annually and that the exposures were largely due to percutaneous injury (Auta et al., 2017). A study conducted in Taiwan, China, which used a retrospective secondary data analysis approach to analyze 2013 data from the Chinese EPINet reported that percutaneous injury resulted in approximately 99 HIV infections; 1,094 HCV infections; and 970 HBV infections (H. C. Wu et al., 2015).
Thousands of healthcare workers experience at least one episode of percutaneous injury per day worldwide (Auta et al., 2017). Recently, a meta-analysis found that one in three healthcare workers worldwide is at risk of percutaneous injury annually (Auta et al., 2018). In another study, it was found that approximately 3 million occupation-related percutaneous injuries occurred yearly (Kaweti & Abegaz, 2016). In United States, approximately 300,000 healthcare workers reportedly sustain at least one percutaneous injury annually (Grimmond & Good, 2017). Percutaneous injuries may result in serious health risks, including psychological trauma, substantial disability, and even death (Jacob et al., 2010).
Although healthcare workers of all disciplines regularly experience percutaneous injuries, the nursing profession is the most likely to sustain them (Gao et al., 2017; H. C. Wu et al., 2015). This is expected given that nurses frequently perform procedures with hollow-bore, blood-filled needles that carry a greater risk of transmission of occupational infections (Memish et al., 2015). In addition, measures such as training, and use of safety-engineered devices, and surveillance systems to prevent body fluid exposure in healthcare settings and reduce the risk of blood-borne pathogens transmission are not readily available in many countries. Consequently, exposure to body fluid is rarely monitored (Frickmann et al., 2016; Green-McKenzie et al., 2016).
Given the severe consequences of exposure due to percutaneous injuries, the prevalence, and relevant factors of percutaneous injuries among nurses have been extensively studied to minimize such injuries (Garus-Pakowska & Gorajski, 2019). However, such studies only estimated the national incidence of percutaneous injuries with the purpose of identifying the real risk of contaminated percutaneous injuries for full-time healthcare workers in China (H. C. Wu et al., 2015). No similar study has been conducted for nurses, especially for midwives, in this country. Therefore, this study aimed to estimate the prevalence of percutaneous injuries and identify the risk factors for percutaneous injuries among a sample of midwives in Hunan Province, China.
Methods
Participants
We employed a cross-sectional study. Purposive convenience sampling was employed to recruit 70 hospitals in the cities of Yongzhou, Chenzhou, Hengyang and Changsha in Hunan Province, China to host this study. All midwives with >1 year length of employment in the study hospitals were eligible to participate.
First, we contacted the nursing administration and human resources departments of the study hospitals to initiate this possible collaboration, recruiting participants, and obtain approval for the research from the Institutional Review Board (IRB) of hospitals.
We then recruited a nurse representative from nursing administration who served as the main contact and liaison between the hospital and the research team in each hospital. The nurse representative was responsible for communicating with the midwives, recruiting participants, providing a list of all potential participants, and facilitating the IRB approval process. A total of 1,282 midwives were eligible to participate. After ensuring the potential participant met the initial eligibility criteria, research assistant made contact via phone for further screening to confirm inclusion/exclusion criteria. The exclusion criteria in the study were on official leave during the study period, refusing to participate. 131 midwives were on leave at the time of our study, and 35 midwives refused to participate, leaving 1,116 for inclusion. Prior to commencing our study, ethics approval for the study was granted by the Ethics Committee of the XiangNan University. All participants provided written informed consent.
Data Collection
This survey was conducted from January 2017 to July 2017. Self-administered questionnaires were mailed to nursing administration’ addresses of each study hospital. Accompanying the questionnaire was an explanation of the goals of the survey, a recruiting notice, and a preaddressed, prestamped return envelope. Follow-up mailings were sent to nonresponders. Paper surveys were distributed and collected by the nurse representative who were recruited from nursing administration. The nurse representative was trained by the research team through the internet before the onsite survey collection. The study questionnaire was completed anonymously and expected to be returned within 2 weeks. The nurse representative was responsible for retrieving the questionnaires. Participants were given a US$20 incentive for completing the survey as a financial reward.
The survey instrument was a structured, self-administered questionnaire, which mainly required checkbox-style answers, and Likert-type scales. The questionnaire included three sections (i.e., sociodemographic data, percutaneous injuries experience in the previous 12-month period, and the Hospital Safety Climate Scale [HSCS]).
The first section ascertained the information about the participants’ demographic and socioeconomic characteristics, including sex, age, length of employment as a midwife, weekly working hours and education.
The second section was related to percutaneous injuries experience in the previous 12-month period, all of which were based on previous research in this field (Kaweti & Abegaz, 2016). Questions regarding percutaneous injuries experience asked if the injury occurred in the last 12 months, the number of injuries sustained, the factors contributing to the injury (e.g., type of procedure, during disposal, equipment failure, patient caused, and others), the type of instrument that was used at the time of injury, and the interventions after the injuries.
The third section included the HSCS based on the scale developed by Gershon et al. (2000). The 20 questions from the Gershon HSCS were translated into Chinese and then back-translated to validate the translation by a bilingual medical professional. Then, an expert panel of nurses, midwives, social scientists, medical professionals, and organizational managers evaluated the Chinese version for accuracy, clarity, and readability. Questions from the original HSCS that focused on HIV were not considered by the expert panel to be appropriate for use among Chinese midwives due to the fact that China has more HBV and HCV cases than HIV cases. Thus, these sections of the HSCS were amended to a more generic category of “blood-borne diseases.” As such, our final Chinese-version survey consisted of 18 questions, of which two were from the 20-item scale developed by Gershon et al. (2000) that had been changed to a broader term relating to blood-borne diseases, whereas two other questions, which may cause confusion, were deleted. Our final Chinese-version of the survey comprised six parts with 18 items, in which two are related to personal protective equipment and engineering controls, three for support from management, two for decision-making for the absence of job hindrances, five for feedback and training, three for cleanliness and orderliness, and three for minimal conflicts and good communication. The Cronbach’s α score for all safety climate questions was 0.891, indicating a high internal consistency. Minor changes were made for cultural reasons. For example, the 5-point Likert-type scale, which comprises five options (“Strongly Disagree,” “Disagree,” “No Opinion,” “Agree,” or “Strongly Agree”) and was used by the original authors, was changed to a 4-point scale by omitting the middle response. Considering the notion that the responses to Likert-type scale questions are influenced by cultural differences was deemed appropriate because Chinese had a proportionally great likelihood of clustering their answers around the midpoint (Chen et al., 2016; J. W. Lee et al., 2002).
The dependent variable was evaluated on the grounds of participants’ answers to whether the percutaneous injuries occurred in the last 12 months.
Statistical Analysis
We generated descriptive statistics including frequencies of percutaneous injuries from the data set. To determine the association between the independent and the dependent variables, we applied chi-square test and Fisher exact probability method for univariate analysis. A multivariate logistic regression model was then applied to relate statistically significant independent variables with a binary indicator (yes or no) for the 12-month prevalence of percutaneous injuries. Potential risk factors for percutaneous injuries such as hospital size, sex, age, length of employment as a midwife, weekly working hours, education, and items of hospital safety climate were included in the model as independent variables. All statistical analyses were performed using the SPSS 21.0 (SPSS Inc., Chicago, IL). p values <.05 were considered statistically significant throughout the analysis.
Results
A total of 1,116 questionnaires were distributed and 998 (89.4%) were retrieved. Six incompletely answered the questionnaires leaving 992 (88.9%) for analysis. The demographic characteristics of the study participants are presented in Table 1. Nearly all the midwives (99.7%) were female, with a mean age of 30.70 (SD = 7.30) years. Furthermore, 56% of the study participants worked in hospitals with ≥400 beds, and majority of them (87.3%) reported that their weekly working hours were ≥40 hours.
Participant Demographics by Percutaneous Injury (N = 992)
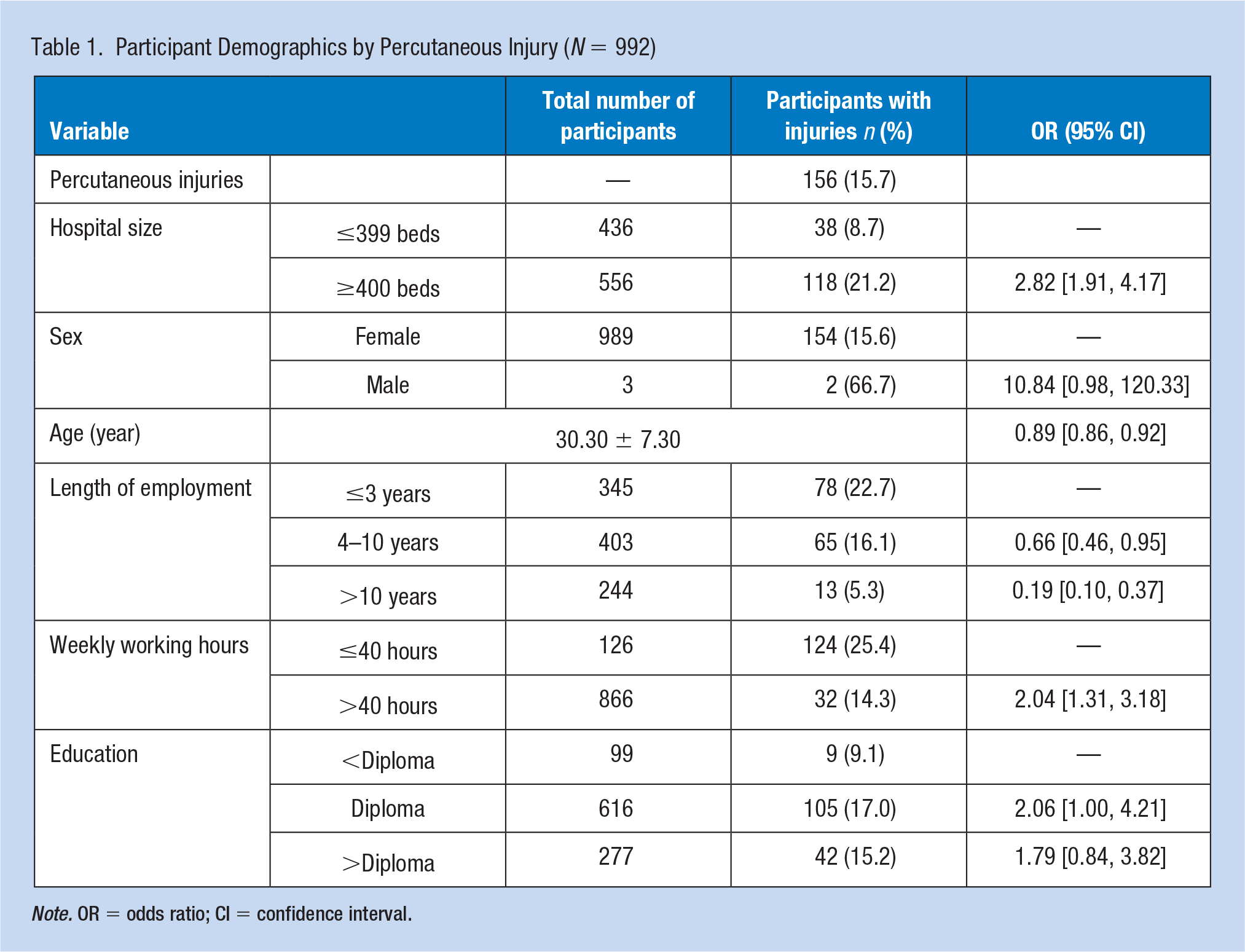
Note. OR = odds ratio; CI = confidence interval.
Among the participants, 156 (15.7%) experienced at least one episode of percutaneous injuries within the past 12 months. Results of the univariate test indicated that hospital size, age, their length of employment as a midwife, and weekly working hours were significantly related to percutaneous injuries.
Affirmative responses to the Chinese HSCS and their relationship with percutaneous injuries are reported in Table 2. A total of 985 (99.3%) participants agreed with the statement “Workers are encouraged to pay attention to health and safety.” A total of 923 (93.0%) participants agreed that sharp containers were readily available at their workplace and 546 (55.0%) reported that a health and safety information manual was available at their workplace. However, only 442 (44.6%) reported that their supervisor discussed safe work practices, and 551 (55.5%) stated that their workplace had a system to prevent exposure to occupational hazards. Finally, 292 (29.4%) participants agreed with the statement that “I think my workplace is always kept tidy”. In univariate analysis, percutaneous injuries was associated with three HSCS questions, namely, “My workplace has a system to prevent exposure to occupational hazards,” “Staff in my unit support one another regarding safety procedures,” and “Open communication between supervisors and staff regarding safety.”
The Relationship Between Items of Hospital Safety Climate Scale and Percutaneous Injuries
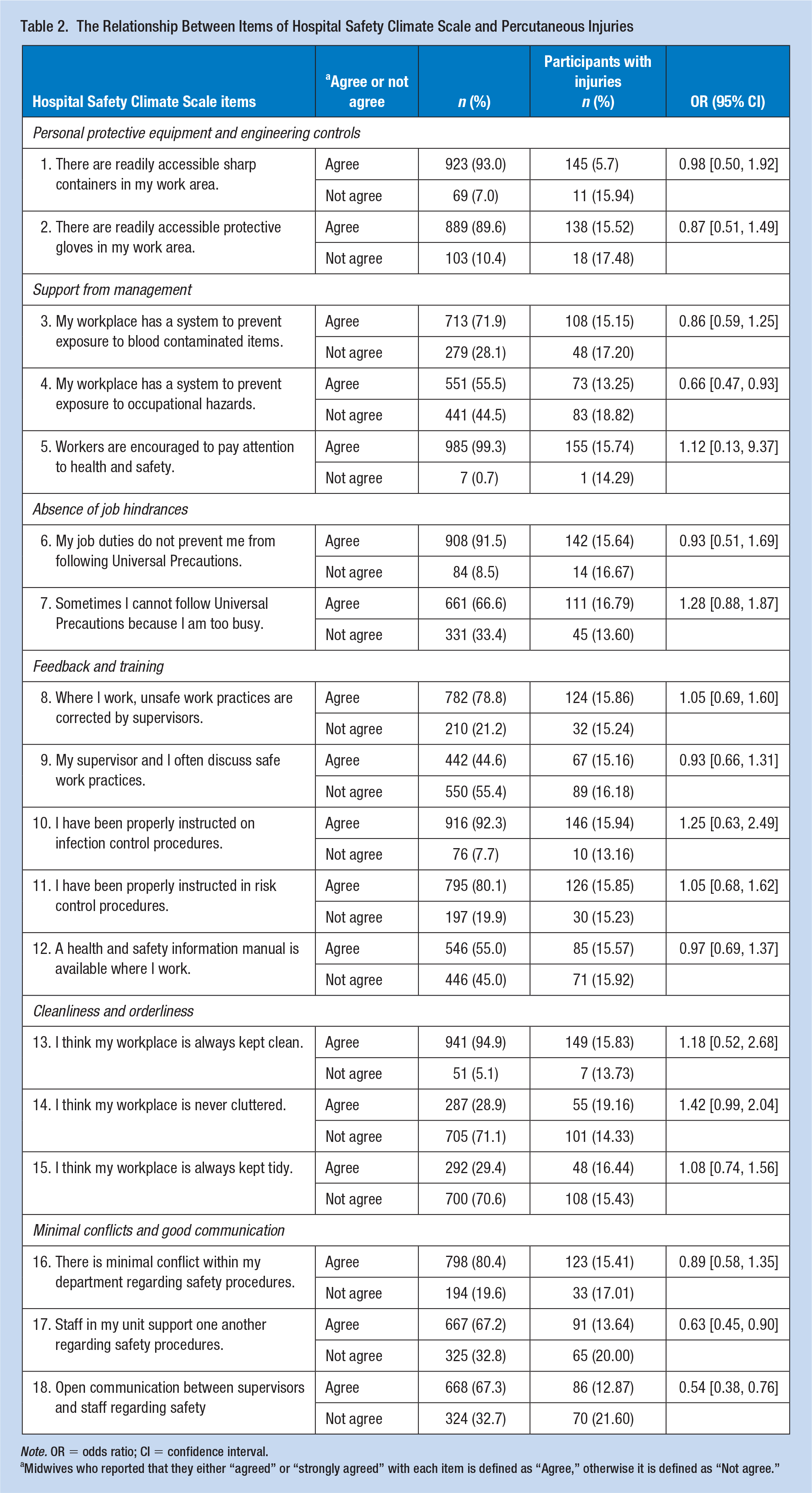
Note. OR = odds ratio; CI = confidence interval.
Midwives who reported that they either “agreed” or “strongly agreed” with each item is defined as “Agree,” otherwise it is defined as “Not agree.”
The variables of the univariate analysis, which had significant differences were imported into the logistic regression. Results from the multivariate analysis suggested that hospital size, age, length of employment as a midwife, weekly working hours, and three HSCS questions were significantly related to percutaneous injuries. The odds of percutaneous injuries among the midwives working in hospitals with ≥400 beds was higher than those working in hospitals with ≤399 beds by twice (odds ratio [OR]: 2.34; 95% confidence interval [CI]: [1.55, 3.54]). We also found that percutaneous injury prevalence in midwives decreased as the age increased (OR: 0.88; 95% CI: [0.84, 0.92]). Midwives with 4 to 10 years of employment as a midwife had 1.48 times the risk of percutaneous injuries compared with those with 3 or fewer years (OR:1.48; 95%CI: [0.92, 2.38]). Meanwhile, midwives with more than 10 years length of employment as a midwife were less likely to exposed to percutaneous injuries compared with those with three or fewer years (OR: 0.65; 95% CI: [0.28, 1.50]).
The probability of percutaneous injuries among the midwives with weekly working hours of >40 was increased compared with that of such injuries among those with weekly working hours of ≤40 by 4.35 times (OR: 4.35; 95% CI: [2.51, 7.52]) (Table 3). Midwives whose workplace has a system to prevent exposure to occupational hazards were 0.62 (95%CI: [0.42, 0.90]) times likely to have suffered percutaneous injuries in the last 12 months. In addition, midwives who thought that staff in their units support one another regarding safety procedures were also less likely to have suffered percutaneous injuries in the last 12 months (OR: 0.68; 95% CI: [0.46, 1.00]), as well as midwives who thought that open communication existed between supervisors and staff regarding safety in their workplace (OR: 0.64; 95% CI: [0.43, 0.94]).
Multivariate Analysis Examining the Relationship Between Related Worker and Work Factors a and Percutaneous Injuries
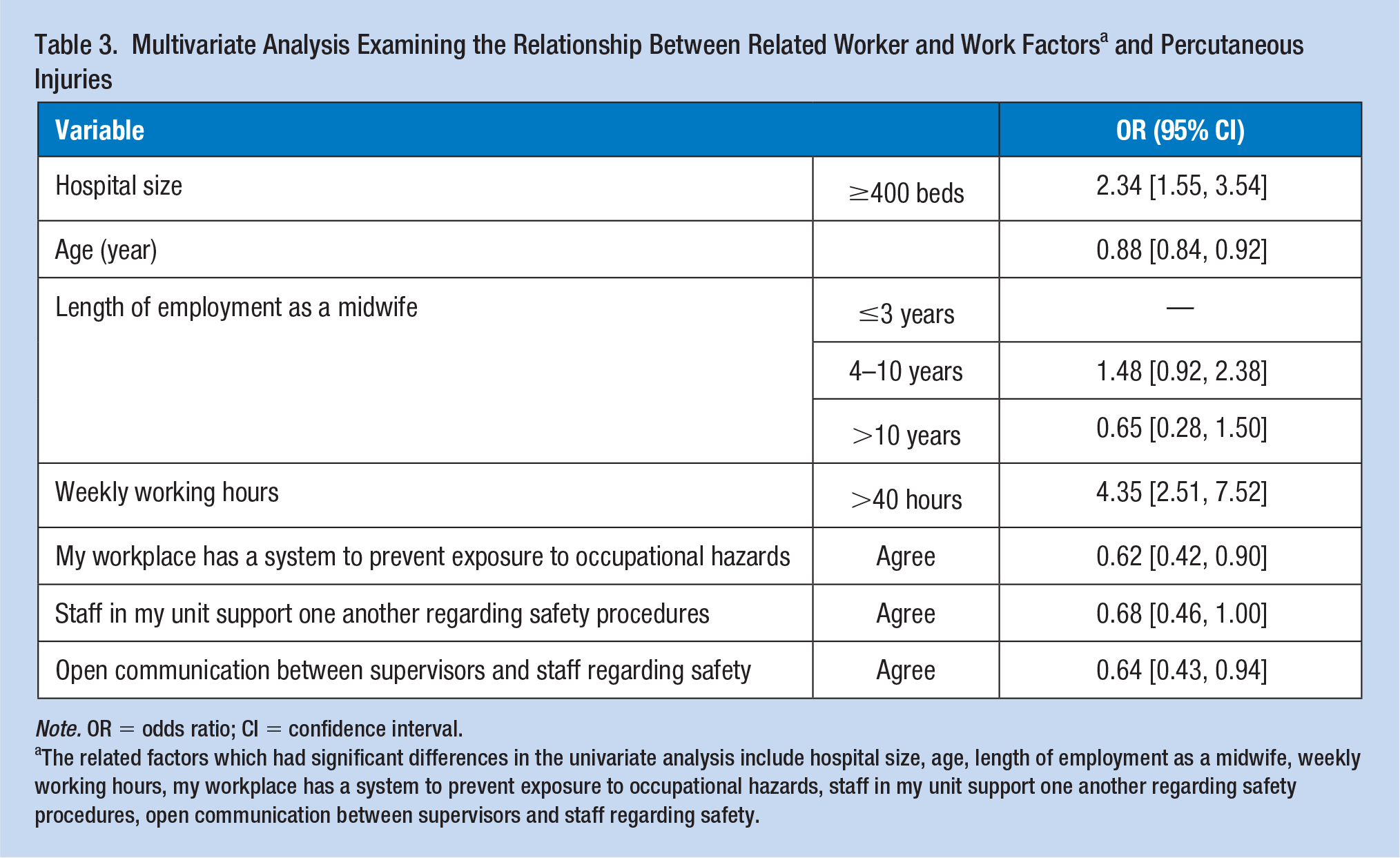
Note. OR = odds ratio; CI = confidence interval.
The related factors which had significant differences in the univariate analysis include hospital size, age, length of employment as a midwife, weekly working hours, my workplace has a system to prevent exposure to occupational hazards, staff in my unit support one another regarding safety procedures, open communication between supervisors and staff regarding safety.
Discussion
This work is the first to investigate the prevalence and predictors of percutaneous injuries among midwives in Hunan Province, China. Based on the results, 15.7% of the midwives sustained percutaneous injuries 1 year prior to the study, which was lower than previously published rates for healthcare workers (Auta et al., 2018; Jacob et al., 2010; Serdar et al., 2013). The lower prevalence of percutaneous injuries in this study may be explained by the underreporting of percutaneous injuries among midwives in China (Cao, 2013). Some studies (Auta et al., 2018; Memish et al., 2015) revealed that the perception of low risk of infection, lack of time, and fear of consequences may be attributed to midwives’ underreporting of percutaneous injuries behavior. Our findings indicate that percutaneous injuries is a serious problem among midwives in Hunan Province. In some studies in which nurses and midwives were combined as a study population (Gershon et al., 2009; Kaweti & Abegaz, 2016; Memish et al., 2015), the prevalence of percutaneous injuries was higher than that in this study. This finding may be explained by the fact that nurses are more vulnerable because they are more frequently in close contact with patients to perform different procedures (intravenous [IV] access procedures, blood sampling, different types of injections, etc.) than the other healthcare workers.
The present study showed that one of the predictors of percutaneous injuries among midwives was working in hospitals with ≥400 beds. This result has not been described previously and is surprising, considering that smaller hospitals are more likely to be in remote and/or poorer areas that lack protective equipment, occupational injuries inspections, and protective measures, especially in economically challenged areas (Bacon & Mark, 2009; Cai et al., 2016). Generally, larger hospitals are often specialized centers and have more experienced personnel, more regular in-service training, and higher levels of senior management support for safety programs, thereby decreasing the incidence of percutaneous injuries (Cai et al., 2016; Yoshikawa et al., 2013). Some studies demonstrate that midwives in smaller hospitals may be at a greater risk of experiencing percutaneous injuries (Cai et al., 2016; Cao, 2013). We did not obtain evidence on this specific finding, but we perceived that hospitals with ≥400 beds have considerably higher risk in maternity than those with lesser bed capacity, and midwives deal more frequently with their tasks, thereby having a higher chance of exposure.
According to this finding, the decrease prevalence of percutaneous injuries as the age increased had a significant trend. This result is consistent with the result of a previous study that reported frequent to occurrence of percutaneous injuries in nurses aged ≤25 years at a university-affiliated hospital compared with that in those >25 years (Cho et al., 2013). Other studies have identified similar findings (Cao, 2013; Zhang et al., 2018). This result could be explained by the fact that younger midwives are particularly susceptible to percutaneous injuries due to insufficient training, underdeveloped skills for midwifery and handling of sharp devices, and limited practical experience. Limited clinical experience and underdeveloped skills were previously identified as reasons for the exposure of nurses and midwives to such injuries (Hambridge, 2011). However, one study showed that age was not a predictor of percutaneous injuries (Kaweti & Abegaz, 2016).
The length of employment as a midwife was significantly associated with percutaneous injuries. Percutaneous injuries exposure was the highest among midwives with 4 to 10 years length of employment as a midwife, followed by midwives with 3 or fewer years length of employment; meanwhile, midwives with more than 10 years length of employment as a midwife were less likely to be exposed to percutaneous injuries. This report is almost similar to one of a previous report in Guangdong Province, China (Cao, 2013). One reason might be that midwives with ≤3 years length of employment as a midwife are clearly a priority when providing educational training concerning percutaneous injuries prevention (Yao et al., 2013). In addition, considering the fact that as the backbone of the maternity ward, most midwives with 4 to 10 years length of employment as a midwife deal more frequently with tasks that are highly at risk for percutaneous injuries (Kaweti & Abegaz, 2016). The risk for percutaneous injuries was associated not only with skill, but also with hazards inherent in the procedures wherein patients’ blood or body fluid are involved (Hambridge, 2011). In contrast, percutaneous injuries occurred less frequently among midwives with more than 10 years length of employment than those with 3 or fewer years. One possible explanation is that midwives with more working years are more focused on administrative tasks (Yoshikawa et al., 2013).
Another predictor of percutaneous injuries among midwives participating in this study was working for more than 40 hours per week; hence, the chance of percutaneous injuries among midwives with weekly working hours greater than 40 hours was at least 4 times as much as those with weekly working hours of ≤40. This result is similar to the study result of E. M. Mbaisi et al., who clearly indicated that working for more than 40 hours per week was associated with percutaneous injuries among nurses and midwives (Matsubara et al., 2017; Mbaisi et al., 2013). Such findings help shed light on workload factors as an important challenge for midwives. Therefore, the acute shortage of midwives in China may have contributed to the present findings. In China, the desperate shortage of midwifery workforce poses a desperate burden on midwifery care (Zhu et al., 2018). The State of the World’s Midwifery 2014 showed that the number of midwives for every 1,000 people in China is only 0.158, far below that of the developed countries, such as Sweden, America, and Britain (Day-Stirk et al., 2014). This has been compounded by China’s limited two-child policy, resulting in an insufficient number of midwives (L. P. Wu, 2016). Inadequate numbers of midwives often results in longer working hours to bridge gaps in personnel, leading to increasing levels of stress and fatigue for midwives. Overworked staff becomes less alert and highly susceptible to percutaneous injuries (Peterson et al., 2016). Meanwhile, midwives’ competencies were clearly deficient, considering that only 0.51% of them in China have a bachelor degree; most of them have technical secondary degree (Li et al., 2014). The undergraduate program in midwifery began in 2017, and midwifery undergraduate schools in China are few (Huang, 2018). In Chinese hospitals, midwives are generally supervised by experienced midwives. Therefore, our findings may highlight the need to address the acute shortage of midwives as well as to develop undergraduate midwifery education programs in China.
Results from our current study offer an interesting insight into the correlation between hospital safety climate and percutaneous injuries among midwives. We revealed that three aspects of safety climate were associated with a reduced percutaneous injuries risk in the current study, namely “My workplace has a system to prevent exposure to occupational hazards,” “Staff in my unit support one another regarding safety procedures,” and “Open communication between supervisors and staff regarding safety.” The concepts of hospital safety climate were introduced in the 1990s by Gershon et al. (2009).
Hospital safety climate is under the umbrella of the organizational climate, which provides a way of identifying characteristics associated with high or low injuries rates among employees (McCaughey et al., 2014; Taylor et al., 2012; Zohar, 1980). Good organizational climate among employers includes having strong support for safety programs and commitment to safety, emphasis on environmental control, frequent safety-related feedback or training, regular and open communication, and a stable workforce (Olds et al., 2017).
In recent years, the impact of organizational climate on healthcare worker’s occupational injuries has been increasingly studied (Braithwaite et al., 2017). To our knowledge, poor safety climate as an important influence on occupational injuries among healthcare workers has been studied (Amponsah-Tawiah & Mensah, 2016; Kiani & Khodabakhsh, 2014). Moreover, improving the safety climate of hospitals offers numerous benefits (Aljabri et al., 2020; Oh et al., 2006; Sekimoto et al., 2008). Our current study supports these findings to some extent. Hence, with an increasingly high requirement of midwifery skills and midwifery workforce shortage, attracting and retaining the services of high-quality midwives in China are desperately needed. This challenge can be achieved by optimizing the organizational climate (Cai et al., 2016). In other words, ensuring a positive safety climate is also essential in reducing percutaneous injuries among midwives.
This study has its own limitations that are worth considering. First, information on percutaneous injuries was collected for the last 12 months prior to the survey through a cross-sectional survey. However, some degree of recall bias could not be ruled out, leading to inaccurate estimations of percutaneous injuries prevalence. Second, purposive convenience sampling was employed in our study, thereby limiting its generalizability, in general.
Implications for Occupational Health Nursing Practice
In the current study, the prevalence of percutaneous injuries among midwives in Hunan Province, China, was substantial. Percutaneous injuries are frequent health hazards among midwives. These findings improve our understanding of the risk of percutaneous injuries among this population. Moreover, the incidence of percutaneous injuries was affected by hospital size as well as by midwives’ age, length of employment as a midwife, weekly working hours, and the three HSCS questions. Accordingly, midwives may derive benefit from training, reduced workload, and good organizational climate in terms of reduced percutaneous injuries (Bagheri et al., 2019; Cheung et al., 2012; Frickmann et al., 2016). In this regard, directors and occupational health midwives should address these issues by providing midwives with training on skills for midwifery, handling of sharp devices, and using of safe instruments; developing increasingly efficient and reasonable work plans; and establishing a stable workforce to decrease their workload. In addition, occupational health midwives can also optimize the organizational climate by fostering the participation of all midwives in decision making on various aspects of the organizational climate (e.g., safety programs and commitment to safety, safety-related feedback and training plans, and environmental control) (Olds et al., 2017).
Conclusion
In conclusion, a high prevalence of percutaneous injuries exists among midwives in Hunan Province, China. Hospital size, age, length of employment as a midwife, weekly working hours, and some aspects of HSCS are associated with percutaneous injuries. Percutaneous injuries should be prevented by measures such as ensuring a positive organizational climate, providing more highly devices, and reducing the workload of midwives. Additional research on developing and evaluating effective interventions to prevent percutaneous injuries among midwives in China, is crucial and needs considerable attention.
Applying Research to Occupational Health Practice
This study provides information about the prevalence of percutaneous injuries and its associated factors among midwives in Hunan Province, China. The results from the current study suggest that the prevalence of percutaneous injuries among midwives was substantial and risk mitigation strategies tailored to midwives are needed to reduce risk of exposure. Midwives may derive benefit from training, reduced workload, and good hospital safety climate in terms of reduced percutaneous injuries. In this regard, directors and occupational health midwives may provide midwives with training on skills for midwifery, handle of sharp devices, and use of safe instruments; develop increasingly efficient and reasonable work plans; and reduce midwives’ workload through increased staffing. In addition, as percutaneous injuries were associated with some aspects of hospital safety climate, ensuring a positive safety climate may also be essential in meeting important challenges for midwives’ occupational health.
Footnotes
Acknowledgements
We would like to express our deepest gratitude to the study participants for their volunteer participation in this research work.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the grants from Scientific Research Fund of Hunan Provincial Education Department (16C1489), Humanities and Social Sciences Planning Project of Ministry of Education (18YJC630065), and Hunan Provincial Social Science Fund Project (17Y3A361).
Author Biographies
Wenjing Cao, MSN,RN, is a lecturer in the School of Nursing, XiangNan University. Her research interests include nursing education, occupational health research in health-care workers and intervention based research.
Nanlin Cao, MSN, is a doctor in the Affiliated Hospital of Xiangnan University, whose researches focus on the effects of work-related factors on occupational attrition and workplace participatory interventions to improve employee health and safety.
Mei Gu, RN, is a senior nurse, currently working at the Department of Thoracic Medicine Department I, Hunan Cancer Hospital. Her research interests are focused on the health effects of modifiable workplace factors and workplace violence prevention.
Pan Li, MSN, RN,is an associate professor of Nursing at Xiangnan University. Her research focuses on the gerontological nursing, nursing education and mental health of health care workers.
Min Li, RN, is a senior nurse, currently working at The Third Xiangya Hospital of Central South University, and has a keen interest in occupational health research in nursing.
Chan Luo, is a student nurse at Xiangnan University. She has worked as a research assistant on this study and is interested in research related to nurses’ occupational health.
Henghui Liu, RN, is a senior nurse, currently working at Central Hospital of Hengyang. Her research interests are focused on the health effects of modifiable workplace factors and the elderly care.
Fuyun Jiang, RN, is a senior nurse, currently working at The First Affiliated Hospital of University of South China. Her research interests are focused on physical and mental health of health care workers.
Chunyan Li, PhD, RN, is a professor at Xiangnan University. Her research focuses on nursing education, the elderly care and occupational health research in nursing.
Shunwang Cao, PhD, is a professor of The Second Affiliated Hospital of Guangzhou University of Chinese Medicine. His research focuses on occupational health and biomarkers for cancers.