
Abstract
Background
The experiences of graduate nurses and midwives transitioning into the clinical environment as beginning practitioners has been reported as a time period of great challenge. For the graduate double degree nurse midwife, often transitioning into two disciplines of practice concurrently, their experiences have the potential to be heightened. The aim of this research was to explore the transition to practice experiences of double degree graduate nurse midwives practicing in either or both nursing and midwifery in the Australian health care system.
Methods
This research used a Husserlian descriptive phenomenological approach to understand the experiences of 23 double degree graduate nurse midwives working in 20 different health care facilities across Australia.
Results
The findings showed that most participants experienced exhaustion from an emotional, physical, and mental perspective during their first year of practice. These experiences were linked with cognitive saturation, professional loneliness, sleep deprivation, and an inability to achieve a work–life balance. The data also highlighted the graduate nurse midwife’s concerns for safe practice when feeling mentally, physically, and emotionally depleted.
Conclusion/Application to Practice
Safe practice is paramount for both patient and health care worker. The levels of exhaustion described by the participants in this study influenced their perceived ability to practice safely. As a result, it should be recognized that the graduate nurse midwife’s health and well-being is central to their perceptions of safe practice and is fundamental to a positive transition to practice experience.
Keywords
Background
Nursing and midwifery are health care professions that require an energy that is both physical and cerebral. Graduate nurses and midwives have consistently reported a mix of challenges in their first year of practice. This stems from working in health care environments and with people with whom they are unfamiliar (Barry et al., 2013). The difficulties are noted to be multifactorial, with concerns often linked with a lack of support due to short staffing and skill mix imbalance, intra- and interprofessional communication conflict, difficulties in adjusting to shift work and work–life intrusions (Boamah et al., 2017).
Graduate double degree nurse midwives are health care professionals who study and graduate with two degrees simultaneously. This concept is a global initiative with programs offered not only in Australia but in European (Kompanets & Väätänen, 2019), Canadian, and American universities such as Queens University in Ontario and the University of Houston.The 4-year Australian double degree Bachelor of Nursing/Bachelor of Midwifery program was initially introduced to address a shortage of nurses and midwives working in the rural sector (Francis et al., 2010). While the concept was positively identified as a means to secure both a nurse and a midwife in one employee (Yates et al., 2011), for the beginning double degree nurse midwife, transitioning into two unique disciplines of practice simultaneously had the potential for the transition to practice challenges already reported by single degree baccalaureate nurses and midwives to be heightened.
Exhaustion is described as the result of long-term mind and/or body activities leading to a chronic lack of energy that cannot be resolved with normal rest periods (Schaffner, 2017). Exhaustion, in a nursing context, has been attributed to a mismatch between job expectations and available resources (Zito et al., 2016), and is associated with terms such as extreme fatigue and physical and mental tiredness (Dahlgren et al., 2016). Nursing research has shown that while fatigue and tiredness increases the need for staff sick leave (Roelen et al., 2013), it is the mental stress and emotional exhaustion that influence even experienced nurses and midwives to leave their professions (Havaei et al., 2016; Welford, 2018;). The reason for early attrition in graduate nurses and midwives (within the first 12 months of practice) has been reported to be multifactorial, with concerns emphasized such as a lack of support due to short staffing and skill mix imbalance, intra- and interprofessional communication issues, difficulties in adjusting to shift work and work–life intrusions (Boamah et al., 2017). While these workforce and workplace factors have been regularly reported in the literature, it is the more personal concerns of fatigue and exhaustion as highlighted in this study that has received limited attention or explanation.
Emotional exhaustion for nurses and midwives is well represented in the literature and described under descriptive terms such as emotional labor (Edward et al., 2017) and compassion fatigue (Drury et al., 2014; Edwards & Anderson, 2016). These terms highlight the emotional effort and fatigue that the nurse or midwife experiences, when providing ongoing and at times demanding empathic and compassionate care (Hong & Lee, 2016; Hunter, 2010). For the graduate nurse, emotional exhaustion is often aligned with workplace and workforce issues such as incivility from colleagues, job dissatisfaction (Laschinger & Grau, 2012), and feeling poorly supported and undervalued (Nitzsche et al., 2013). The literature refers to the intensity that emotional care provided by midwives can impact their emotional well-being (Bacchus & Firth, 2017) with graduate midwife’s reporting challenges when working autonomously without adequate support (Cummins et al., 2017) and being unable to effectively support the woman in their care (Barry et al., 2013, p. 1354).
Rudman and Gustavsson (2011) showed that these types of experiences lead not only to high levels of emotional stress, but also to poor-quality sleep, bad eating habits, and stress-related musculoskeletal pain. The physical and psychosocial stressors of clinical work have also been identified as causal factors for musculoskeletal injuries and chronic pain which hinder the ability to work effectively and safely (Rahman et al., 2017). Emergency and critical care nurses have identified neck, shoulder, wrist and foot pain associated with both the emotional tension and their physical workload. Others have noted that, poor nutrition (Siqueria et al., 2015), sleep deprivation (Dorrian et al., 2011), and reduced social contact (Gifkins et al., 2017; Pugh et al., 2013) add to nurses and midwives’ physical and emotional stressors, causing short and long-term health issues including insomnia, depression, obesity, and cardiovascular disease (Matheson et al., 2014).
Reduced cognitive function in emotionally and physically tired as well as sleep-deprived midwives and nurses has been linked to care safety concerns, where clinical decision-making errors (Johnson et al., 2014; Marion, 2015) and missed care needs may occur (Geiger-Brown et al., 2012). Sleep deprivation has also been shown to impair communication skills, to reduce coping in emotionally charged environments and to impede memory, including the ability to learn new facts (Goel et al., 2009). While studies have shown the positive relationship between quality sleep and cognitive function (Caruso, 2014), the literature rarely considers the impact of sleep-related tiredness or fatigue on the graduate nurse or midwife’s transition to practice experiences. Studies have instead focused on support structures provided to meet organizational needs that ensure graduates achieve competencies, patient safety expectations, and are retained in the profession (Sullivan et al., 2011; Tyndall et al., 2018). Apart from one study, that advocates for graduate nurses to be placed in less clinically complex and stressful environments (Phillips et al., 2014), and one reporting the importance of emotional well-being for graduate midwives (Bacchus & Firth, 2017), no literature was identified that considered physical and mental exhaustion as a primary concern for the graduate nurse or midwife’s well-being or their ability to practice safely.
The aim of this research was to explore the occupational transition to practice experiences of 23 double degree Bachelor of Nursing/ Bachelor of Midwifery graduates, who were employed in 20 different health care facilities across Australia. The purpose of the research was to explore and identify the experiences of these graduates from a dual degree, dual role perspective.
Methods
A descriptive phenomenological approach in the Husserlian tradition was utilized for this study (Husserl, 2012). This methodology has been noted to be valuable when previous studies of the subject matter are unavailable (Dowling, 2007), The unstructured interview process enables the participant to express their experiences from their own priorities of importance and relevance (Husserl, 2012). Therefore, the interview was commenced with a general question “Could you please tell me about your experiences in the past year while working as a graduate nurse/midwife here at . . . .” The only other input would be to ask for further description to their responses or to direct the focus back to the original question if needed. Inclusion criteria stipulated participants who were registered with the Australian Nursing and Midwifery Board of Australia (NMBA, n.d) and had been employed to work either as a nurse or a midwife or as a dual nurse midwife within the past 9 to 12 months. Participants had to be working in Australia for the timeframe and were interviewed individually in their place of choice.
Ethics approval was gained through the Central Queensland University’s Human Research Ethics Committee (H13/10-183). Consent was gained via email prior to the commencement of the interview. All participants were provided with information that outlined the purpose of the study; that is, to understand their experiences as graduate nurse midwives and also a verbal and written reassurance of privacy which included deidentified transcripts and secured files. As part of the university’s support agreements, participants were offered the availability of free university funded counseling sessions should professional support be needed.
Data Collection and Analysis
Using a descriptive phenomenological approach, data were gathered through face to face unstructured interviews. In line with the flexible nature of the methodology, and the philosophy to not lead or influence the participant response (Husserl, 2012) the opening question for each participant was “Please describe your experience as a graduate nurse and/or a graduate midwife in the clinical setting in the previous 9 – 12 months.” To gain the underlying meaning behind the participant experiences, detailed explanation or descriptions of experiences were encouraged, and participants were redirected back to the focus of the study if needed. The venue for the interviews was the choice of the participants and ranged from public areas such as parks through to the participant’s workplace and the university library. The majority of participants preferred to be interviewed in their own home. All interviews were audio recorded with most lasting 60 minutes, and the interview closing at the participant’s discretion. The transcripts were analyzed using Colaizzi’s (1978) procedural framework of seven steps of data analysis. Colaizzi’s framework was chosen as the seven auditable and transparent steps enable meanings, categories and themes to be realized from significant participant statements that relate to the research phenomenon. A final step, where a summary of the findings are made available to and validated by the participants enhanced the rigor of the analysis. Colaizzi’s procedural framework is often applied in health care research, and this type of process is reported to facilitate a detailed, credible and trustworthy approach to data collection and analysis (Lincoln & Guba, 1985).
Findings
A purposive sample of 29 double degree Bachelor of Nursing/Bachelor of Midwifery graduates from one Australian university were invited by email to participate in the study. All of the double degree graduates were identified via the university’s alumni database and contacted directly by alumni staff. All participants had completed a 4-year Bachelor of Nursing/Bachelor of Midwifery double degree, were registered with the Nursing and Midwifery Board of Australia (NMBA, n.d) and had been working as either a nurse and/or a midwife in an Australian health care facility for the past for 9 to 12 months. Participants worked in a variety of acute care settings with 13 working in metropolitan hospitals and 10 working in regional centers. Apart from three of the participants working only as a nurse and two working only as a midwife, all the remaining participants worked as both nurses and midwives either concurrently or consecutively at some time during their graduate year.
This sample group was considered to be unique in that not only were they double degree graduate registered nurses and midwives for whom no previous research was identified, their undergraduate education occurred at the same university and they had traveled widely within Australia to find employment. Therefore, the findings were expected to reflect the graduate’s transition to practice experiences within the clinical facilities, rather than be overtly influenced by differing undergraduate educational experiences.
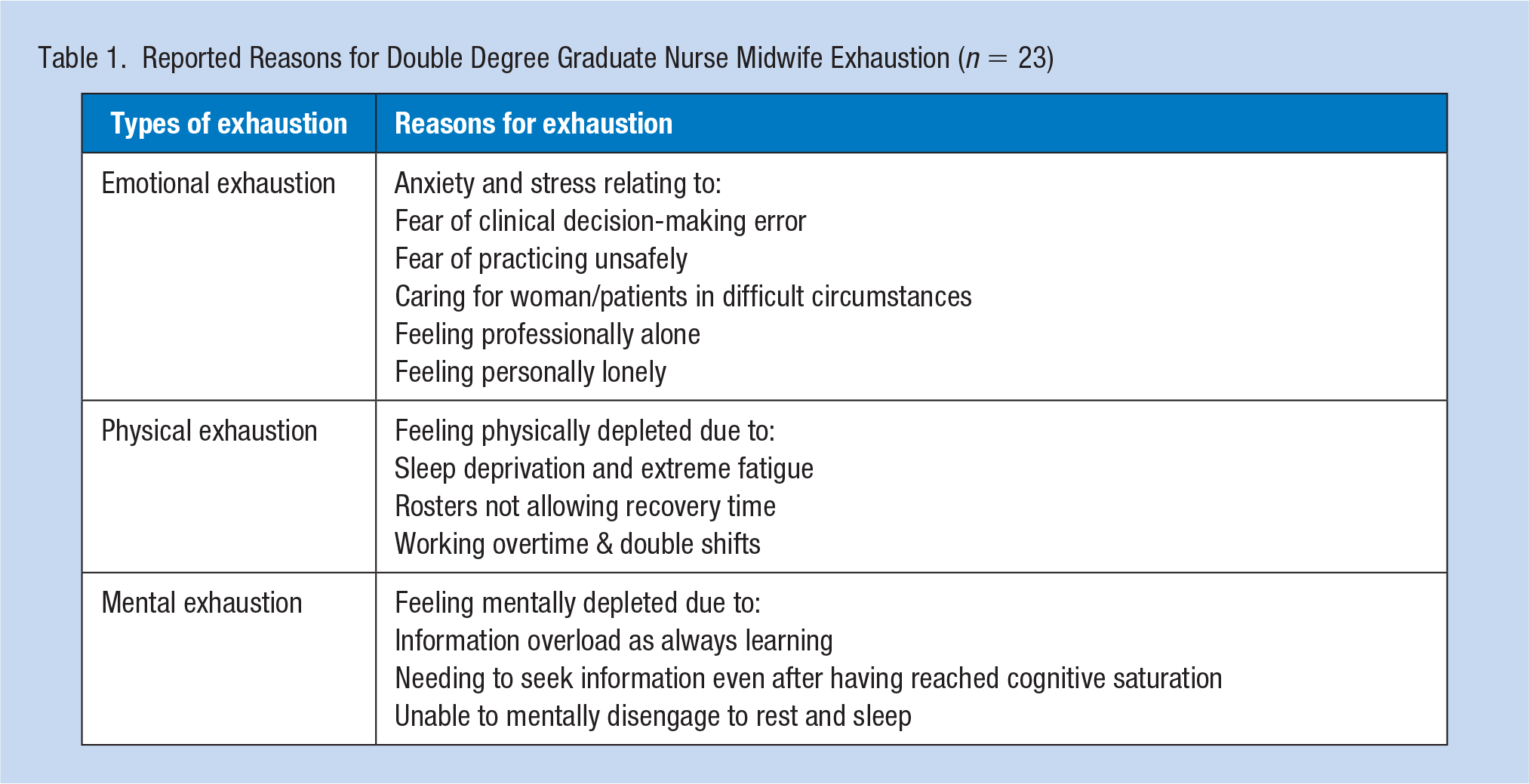
Themes that emerged from the data analysis were related to exhaustion, safe practice, difficulties in achieving a work–life balance, and the importance of time to rest and reflect. Participants provided significant detail when describing the differences between physical, emotional, and mental exhaustion, explaining how each manifested and impacted on their experience (Table 1). Specifically, the levels of exhaustion related to the limited ability to gain sufficient sleep, the physicality of the work in relation to the length of shifts, the stress associated with increased responsibility, relentless learning demands, emotional demands from working with distressed people in their care, and the ongoing cycle of mental/physical fatigue. The findings are reflective of the graduates’ 9 to 12 months’ experience as a whole, and apart from one participant (working in the dual role concurrently as a nurse midwife), who commented on the increased demands of nursing work over midwifery work, none of the other participants differentiated between each discipline’s expectations. The findings are presented with identifiers that include the letter N to denote that this participant worked in a nursing only environment or NM which indicates that the participate worked either concurrently, consecutively, or sporadically as a nurse and/or midwife during their first year of practice. A discussion of each theme will follow.
Reported Reasons for Double Degree Graduate Nurse Midwife Exhaustion (n = 23)
Physical Exhaustion
Physical exhaustion was described by the participants as something that related to tiredness, fatigue, and the inability to gain enough time for rest and relaxation. “It’s just exhausting, just physically. Some days you just need to sleep” (P2NM). Physical exhaustion was also attributed to shift work, with long shifts, overtime, and rostering that did not allow suitable rest between workdays as key problems. “Physically very draining. Especially if it’s understaffed and you end up doing a double shift because someone needs to do it” (P10NM). Recovery time frames were noted to invade days off so that the participants returned to work feeling as though they had not had a suitable break. “If you do three twelve-hour shifts in a row, and you have three days (off), one or two days of that is recovery. It’s not as if you’ve got those days off, you’re recoverin.” (P6N). The lack of routine was a common concern for a many of the graduates, who found it difficult to get back to their normal sleep routine. “There’s no regularity to it, almost every day it’s a different time you’re waking up and going to bed” (P22NM).
Emotional Exhaustion
Emotional exhaustion was perceived by participants to emanate from a number of different sources. Many of the participants expressed emotional challenges in emergency situations, particularly when they had little support. “You’ve been with this lady for 8 hours and then her baby is rushed to the (special care) nursery. You’re emotionally involved in that situation” (P17NM). For those graduates who worked concurrently as a nurse and a midwife, the movement from one discipline to another provided a new challenge. This was particularly so for one graduate working in a rural center. “I was absolutely terrified just because I hadn’t done it (nursing) for so long . . . and I would be like, I don’t know if I can do this. I don’t know what I’m doing” (P7NM).
For those graduates living away from family and friends, the emotional loneliness and the need to debrief with family was clear in their descriptions.
Just the loneliness was probably the most emotionally draining thing. (P15NM) It’s really important that you are able to debrief with friends and family because you will say things to friends and family that you wouldn’t say to work colleagues. (P16N) So I did spend a lot of my time on the phone with friends and family. They were really supportive. (P7NM)
Mental Exhaustion
The persistent need and expectation to learn placed a burden on the participants. “You’re learning so much . . . there’s not a shift where you don’t learn something . . . your brain doesn’t stop the whole time” (P22NM). The demands of new experiences every day were particularly challenging for the participants. “. . . those first few months every day you were having first experiences which is quite nerve-wracking” (P9M). Other participants explained how they struggled to mentally disengage after a busy shift. “I find that even on my days off I’m going to bed at eleven at night because my brain isn’t actually disengaging” (P9M).
Exhaustion and Safe Practice
Many graduates commented on their concerns regarding safe practice. Their descriptions of extreme tiredness were significant.
The first couple of times I did a 12 hour shift I thought I was going to fall asleep on my feet. (P19N) I would sleep [as soon as I got home] and I would wake up for the next shift the following morning. So, I needed 12 or 13 hours of sleep everyday just to survive. (P12NM)
The concerns for potential unsafe practice were often linked to shift work. “I don’t think I will ever get used to shift work! It’s almost debilitating . . . you just start to doubt yourself and I think ‘Am I safe practicing when I’m this tired or this exhausted?’” (P1NM). Participants reported the need to take sick leave for fear of not being able to practice safely due to tiredness. “You end up calling in sick because you realize that you’re not safe to practice when you’re that tired” (P21NM).
Exhaustion and Work–Life Balance
The inability to find a balance between their workload and clinical responsibility was clear, and for some of the graduates, it was impossible to achieve a work–life balance. “Around here I spend a lot more of my time at work. I don’t know how to balance it” (P13NM) and “there is no work–life balance. It is all work and no life” (P17NM). Multiple graduates noted the importance of time with family and friends to improve their work–life balance. “I hadn’t seen mum and dad in ages, so I felt like I was missing out on the good parts of my life through working” (P2NM). Participants discovered that to achieve any sort of work life balance or keep in contact with family and friends, they needed to plan well ahead. “Our rosters are out 2 and 3 months in advance, so I have learnt to plan things ahead of time if I wanted to have any sort of a social life” (P8NM).
Exhaustion and Time
Feelings of exhaustion were experienced at some time by 20 of the 23 participants. The three remaining participants were unique in that one did not work shift work, (10-hour day shifts) another had extended supernumerary support when they had no direct patient responsibilities for 3 months and the other had a workload that was not consistently high (small rural hospital). All participants however, identified time as the commodity essential for a quality lifestyle. For one participant, time enabled learning and reflection. “If I had more time, to read up on these areas . . . It gives you time to look things up you don’t know . . . to reflect and recover” (P22NM). For three of the graduates, the relentless tiredness overwhelmed them and at about 6 months into their graduate year they needed to take leave away from the work environment. “I was crying all the time and had to take a week off” (P9M). Time constraints were relieved by participants working less that a full-time load with 0.7 to 0.8 FTE (full-time equivalent) and choosing not to work regular overtime or double shifts. “I found if I work 0.8, it works quite well. I get a good balance and your sanity is it much better” (P10M) and “I don’t feel physically exhausted at all working 0.7” (P18NM).
Discussion
The concept of exhaustion described by the participants in this study related to persistent learning and information overload, personal and professional loneliness, sleep deficits related to working long shifts/overtime and not being able to achieve a healthy lifestyle and a work–life balance. All of these factors contributed to most of the participants experiencing emotional, physical and mental exhaustion at some time in the first 9 to 12 months of their graduate year. Data analysis did not extend to the comparison of the participants experiences in relation to nursing or midwifery practice as the sporadic nature of their allocations to nursing or midwifery areas of practice was unreliable, and the aim to understand their experiences were not specifically discipline based.
Emotional exhaustion has been noted to be the primary cause of job dissatisfaction and the core component of burnout among nurses and midwives (Welford, 2018; Hong & Lee, 2016). The emotional demands described by the participants in this study related to caring for patients and women in difficult situations, fear of making a mistake, homesickness, and loneliness. While emotional labor and exhaustion for the experienced nurse and midwife are primarily drawn from the need to engage with the people in their care and respond effectively to meet their needs (Badolamenti et al., 2017; Hunter, 2010), for the participants in this study their emotional exhaustion related mostly to caring for patients and women in difficult situations, and anxiety and concerns that they may make a clinical decision error, leading to unsafe practice. Their levels of emotional exhaustion escalated in situations where they felt professionally alone, and/or personally lonely, with many seeking guidance by debriefing and sharing clinical experiences with family and friends. While the participants reported feeling that this support was valuable, these interactions had the potential to breach professional boundaries and to reduce family interactions to counseling sessions.
The negative impact of shift work in nursing and midwifery is wide and varied, with the literature reporting physical as well as psychological implications (Lowden et al., 2010). Ineffective rostering that did not allow the participants in this study time to rest and recover were noted to cause extreme fatigue and physical exhaustion as well as an inability to think clearly. This was reported from both a nursing and a midwifery context, with difficulties to get enough sleep often central to their responses. Neurological studies have shown sleep deprivation to cause cognitive decline impacting on a person’s ability to communicate and cope with emotional demands (Belcher et al., 2015). In nursing, attention lapses (or microsleeps) have been associated with clinical errors of judgment and missed care episodes (Geiger-Brown et al., 2012). This involuntary response to sleep deprivation is described as being awake (with eyes open) but not aware of surroundings or what is going on around them. From this research, most participants reported physical and mental exhaustion due to a prolonged sleep deficit, and raised concerns about their ability to practice safely when tired. All participants either worked an 8 or 12 hour shift, with 12-hour shifts being nursing-specific. None of the participants working in the midwifery environment needed to be “on call,” and none worked from a continuity of care perspective. Those participants working 0.7 or 0.8 FTE as opposed to those working 1.0 FTE did not report physical exhaustion or concerns about the potential for unsafe practice due to physical tiredness.
The need to be consistently learning for the whole of every shift was an expectation that the transitioning nurse midwives in this study found to be mentally challenging and exhausting. Their descriptions of having reached learning capacity yet needing to continue to seek and absorb more information was distressing for them. This was a common concern for most of the participants, and was not nursing or midwifery specific, nor was it more common in those participants working across both disciplines simultaneously. One participant described the need to “rest their brain” as they found the incessant learning and trying to remember information from one day to the next overwhelming, as their “brain was full.” Cognitive saturation due to persistent learning has been shown to affect a person’s attention span and their ability to retain information in their short-term memory (Kingberg, 2008). An effective working short-term memory is essential for the graduate nurse midwife, as they often find themselves in unfamiliar clinical scenarios and need to gain, retain and recall information quickly to fulfill their role during the shift. Equally as important is for the graduate to build a repository of information in their long-term memory. Long-term memory storage however is known to be most effective during sleep (Goel et al., 2009), hence for those participants who reported an inability to cognitively disengage or to gain enough sleep, their inability to store experiences in long-term memory may also have negative repercussions on their practice
While the participants valued the need to learn as a graduate, finding the time to rest and recover in preparation for the next shift was reported as the primary goal. Currently graduate nurses and midwives are expected to learn and develop their competencies as quickly as possible (Tyndall et al., 2018). This approach has been challenged by two European workforce studies (Paulsson et al., 2005; Proost et al., 2012), that proposed the importance of the employee to learn and reflect in a well-paced and stress-free environment. Recommendations included that the learner must have a sense of control of their learning experiences, and that learning should not place an extra burden on the learner but be factored into the workday. Even though neither of these studies had a nursing or midwifery context, the core finding that time must be set aside for learning and reflection to occur remains valid for this transition cohort.
This research focused on the experiences of graduate double degree nurse midwives, working in their first year of clinical practice. While transition to practice challenges reported by single discipline graduate nurses and midwives are similar by nature, it is the degree of exhaustion and the safety implications described by the participants in this research that is unique to the literature. Further research is needed to identify if the experiences of exhaustion described by this cohort of nurse midwives were unique to double degree graduates or is common to all graduate nurses and midwives. Also, the participants’ descriptions of exhaustion, being physical, mental, and emotional needs to be explored further to understand if it is the exhaustion itself, or the components that lead to the exhaustion that impacts on their perceptions of unsafe practice.
While the study is limited by a single cohort of graduates from one university, it is also a strength of this study. With the variables of educational preparation reduced, the ability to explore the graduate’s clinical experiences during their transition was less hindered. A further strength is the inclusion of multiple health care settings from metropolitan to regional areas of both nursing and midwifery practice. A limitation however was the sporadic nature of the participants working as either or both nurses or midwives, which posed a difficulty to determine if working as both nurse and midwife concurrently increased the levels of exhaustion more than those participants working in a single discipline.
Implications for Occupational Health Nursing Practice
Nursing and midwifery are careers where optimal physical, cognitive, and mental well-being are essential for best practice outcomes. The levels of occupational exhaustion described by the majority of participants in this study, related to the dual degree graduate nurse midwife’s beginner status, where adapting to shift work, intense learning requirements and trying to find a work–life balance provided challenges that had many of the participants questioning their ability to be able to practice safely. While the findings from the study can be reflective of single degree nurses and midwives, the intensity of the described challenges impacted negatively on the participant’s ability to sleep, learn effectively, and their perceived inability to practice safely. The participants craved time to reflect, rest and recover, and time to achieve a work–life balance. As safe patient care and positive patient outcomes are central to the role of the nurse and midwife, for the participants in this study their perceived inability to meet these expectations impacted negatively on their perception of self-worth in their profession of choice. Unit managers and educators are encouraged to ensure that rostering and transition to practice programs enable the graduate nurse midwife to transition into a learning environment where they feel well supported, well rested, and safe in their provision of patient care.
Applying Research to Occupational Health Practice
The findings from this research link safe practice concerns among double degree graduate nurse midwives who reported feeling physically, emotionally, and mentally exhausted. While the participants worked in a variety of heath care facilities, mental and emotional exhaustion commonly related to cognitive saturation, professional loneliness in an emotionally charged health care environment, and a fear of making clinical errors. Physical exhaustion was influenced by the rostering system, the demands of shift work and associated sleep deprivation. Workplaces should be cognizant of the potential for exhaustion in their graduate nurse midwife workforce and be mindful of the potential negative patient care outcomes if their levels of tiredness and fatigue impacts their ability to work safely.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Central Queensland University Scholarship fund for PhD students.
Author Biographies
Helen Donovan is a lecturer and researcher at the Queensland University of Technology, with workforce and workplace interests primarily related to the graduate nurse and midwife.
Anthony Welch is an associate professor at Central Queensland University and was a supervisor and mentor for this project. His mental health background laid a strong foundation to explore the issues of practice noted in the findings.
Moira Williamson is a professor of nursing and midwifery, and Head of School at Central Queensland University. Her supervision was underpinned by her extensive clinical, teaching and academic background so as to view the findings from a diverse perspective.