
Abstract
Background:
The International Safety Center disseminates the Exposure Prevention Information Network (EPINet) surveillance system to standardize a system for healthcare facilities to track mucocutaneous blood and body fluid exposures.
Methods:
Occupational exposure incidents to blood and body fluids were recorded within the participant health systems and hospitals (N = 41), using the EPINet Blood and Body Fluid Exposure Report Form. Forms include detailed questions about the circumstances surrounding the exposure, including the type of exposure, body part(s) involved, and if the employee reporting the incident was wearing personal protective equipment (PPE).
Results:
There were statistically significant differences between participants who wore PPE at time of exposure versus those who did not. Differences were noted by job category (χ2 =32.91, p-value = <.001); where the exposure occurred (χ2 = 32.31, p-value = <.001); what the exposure was a result of (χ2 = 50.19, p-value = <.001); and day versus night shift (χ2 = 11.47, p-value = .001).
Conclusion/Applications to Practice:
The study found that occupational exposure to blood and body fluids in 2021 remain high risk given the frequency with which they happen, the exposure site (face) and lack of PPE use. The pandemic seemed to matter little in changing frequencies despite high awareness and growing PPE availability and supply. The findings provide robust information about how exposures occur, why they remain high risk, and how important it is to improve reporting and surveillance to prevent occupational exposures and disease in healthcare in future.
Keywords
Background
Healthcare workers (HCWs) are at risk of blood and body fluid (BBF) exposure during their job duties that result in occupational exposures to blood-borne and infectious diseases (Centers for Disease Control and Prevention [CDC], 2017). The Occupational Health and Safety Administration (OSHA, 1991) Bloodborne Pathogens Standard requires a robust exposure control plan (ECP) that is updated annually. It also requires the use of engineering controls including sharps injury prevention devices, safe disposal of regulated waste, use of personal protective equipment (PPE), and hepatitis B vaccines.
From June 1995 to December 2007, a national summary of BBF exposure data collected among participating healthcare facilities across the United States found 30,945 reported exposures (CDC, 2011). The surveillance study included participants across 28 states and the District of Columbia and had 81 facilities participate for at least 1 year. Most reported exposures occurred within impatient units and in operating rooms, with 72% of reported exposures involving nurses and physicians.
In the context of the COVID-19 pandemic, HCWs are at almost 12 times greater risk for COVID-19 infection when compared with the general population (Nguyen et al., 2020). Furthermore, they are often confronted with difficult working conditions and environments, such as longer working hours and staff shortages (Brophy et al., 2021). There has been reported associations between protocols healthcare facilities follow due to the COVID-19 pandemic and violence against HCWs. In a systematic review, emergency medical personnel commonly report spitting and biting from their patients (Murray et al., 2020). Arguably, the conditions brought on by the COVID-19 pandemic including workplace violence (Byon et al., 2021) and risk of infection further demonstrate the need to protect HCWs from BBF exposure.
The International Safety Center (ISC) developed the Exposure Prevention Information Network (EPINet) Microsoft Access based surveillance system to standardize a system for healthcare facilities to record and track BBF exposures (ISC, 2022). The EPINet can be used as a tool to support facilities in identifying where occupational exposures are occurring, so they can be prevented in the future. Since 1992, participating hospitals have submitted data on occupational BBF exposures to ISC. Over many years, EPINet data illustrate that among reported exposures, the majority of BBF occurred to the eyes and 80% of exposures are to the head. Unfortunately, only about 12% of HCWs indicate that are were wearing any eye protection during their exposure. The majority of occurrences, about 75%, happened in the patient room, surgery, or emergency department.
This study aims to analyze the data collected by the ISC for 2021 and compare if there were differences in exposure types and PPE use during the COVID-19 pandemic given the added focus on exposure prevention. The authors hypothesize that the 2021 findings will demonstrate continued occurrence of high-risk mucocutaneous exposure incidents and under-utilization of PPE despite the COVID-19 pandemic.
Methods
Study Population
Through agreements in the United States, ISC collects EPINet Blood and Body Fluid Exposure reports as entered into EPINet Microsoft Access database among participant network healthcare systems (Supplemental Appendix A). Network facilities include mostly acute care hospitals (N = 41). The largest proportion of network systems has been providing their EPINet data to the Center since the 2000s, making data easily comparable over time.
There is no active recruitment being done and contributing facilities are not reimbursed for their data. The data that are provided annually are provided by facility-based occupational health professionals that have been using EPINet for many years, some since the 1990s. As such, the researchers realize this could contribute to a volunteer bias. The 2021 data are aggregated from 41 facilities, some of which include outpatient settings and home care. Data are sent without employee identifiers. Participating hospitals vary in size, location, and teaching status.
Data Collection
When an occupational exposure to BBF occurs within the participant hospital, the exposed worker reports the incident to their occupational health professional, who then enters that information into the EPINet Blood and Body Fluid Exposure (BBE) Report module (ISC, 2021). The report form is available in Supplemental Appendix A. The report form includes information about date and time of exposure, job category of exposed worker, department or facility location, body location of the exposure, if the source patient is known, type of body fluid and if it was visibly contaminated with blood, if and what type of PPE is worn, and more. The worker is also asked to fill in a free text description of how the incident occurred.
The instrument was developed from the feedback and participation of subject matter experts through an iterative process. Participant use of the instrument and user feedback has helped observe if the instrument measures as intended. The 30-year participatory development and revision of the instrument has supported evidence for content and face validity. The exposure patterns are similar across organizations and throughout the annual basis, supporting reliability of the instrument. Data collected and analyzed is from January 1 to December 31, 2021.
Data Analysis
Quantitative data collected for frequency and percentage of responses from the closed-ended items were tabulated. Day shift was categorized as 7 AM to 7 PM and night shift as 7 PM to 7 AM. Any overlapping time period was considered night shift. The PPE use was considered if a respondent reported wearing a barrier garment and or PPE at the time of exposure. Selection of “other” was not considered PPE use as it cannot be clearly defined and some respondents who selected “other” described it as “none.” Chi-square tests were used to compare participants who wore PPE at time of exposure versus those who did not with job category; where the exposure occurred; what the exposure was a result of; contact time; and day versus night shift. Qualitative data collected describing incident circumstance was explored for common themes that emerged related to PPE and exposure types. No personal identifying information was included in the quantitative analysis. Any qualitative information that could be linked to a participant was removed or paraphrased. All quantitative analyses were performed using IBM SPSS Statistics version 26. All qualitative analyses were performed using NVivo Version 12.
Results
There were 41 facilities reporting their EPINet data to ISC in 2021. There were a total of 571 occupational incidents reported from all facilities. Information about facility type including size, profit status, or geography is not included in the analysis. The EPINet does capture information about whether the facilities are “teaching” or “non-teaching” and does report out those ratios and rates separately.
Since EPINet is an occupational incident surveillance system that is administered by each facility separately and not a survey, it is not possible to capture how adequately all incidents are reported and captured. This means that a response rate cannot be calculated.
Exposure Incidents, Quantitative Data
Of the 571 incidents recorded, only 279 of records (54.6%) indicated wearing any kind of PPE or barrier garment at the time of exposure. No respondent selected more than three PPE items. The source patient (or specimen) was identifiable in 524 of the participants (91.8%). This adds greatly in the performance of appropriate post-exposure prophylaxis and follow-up.
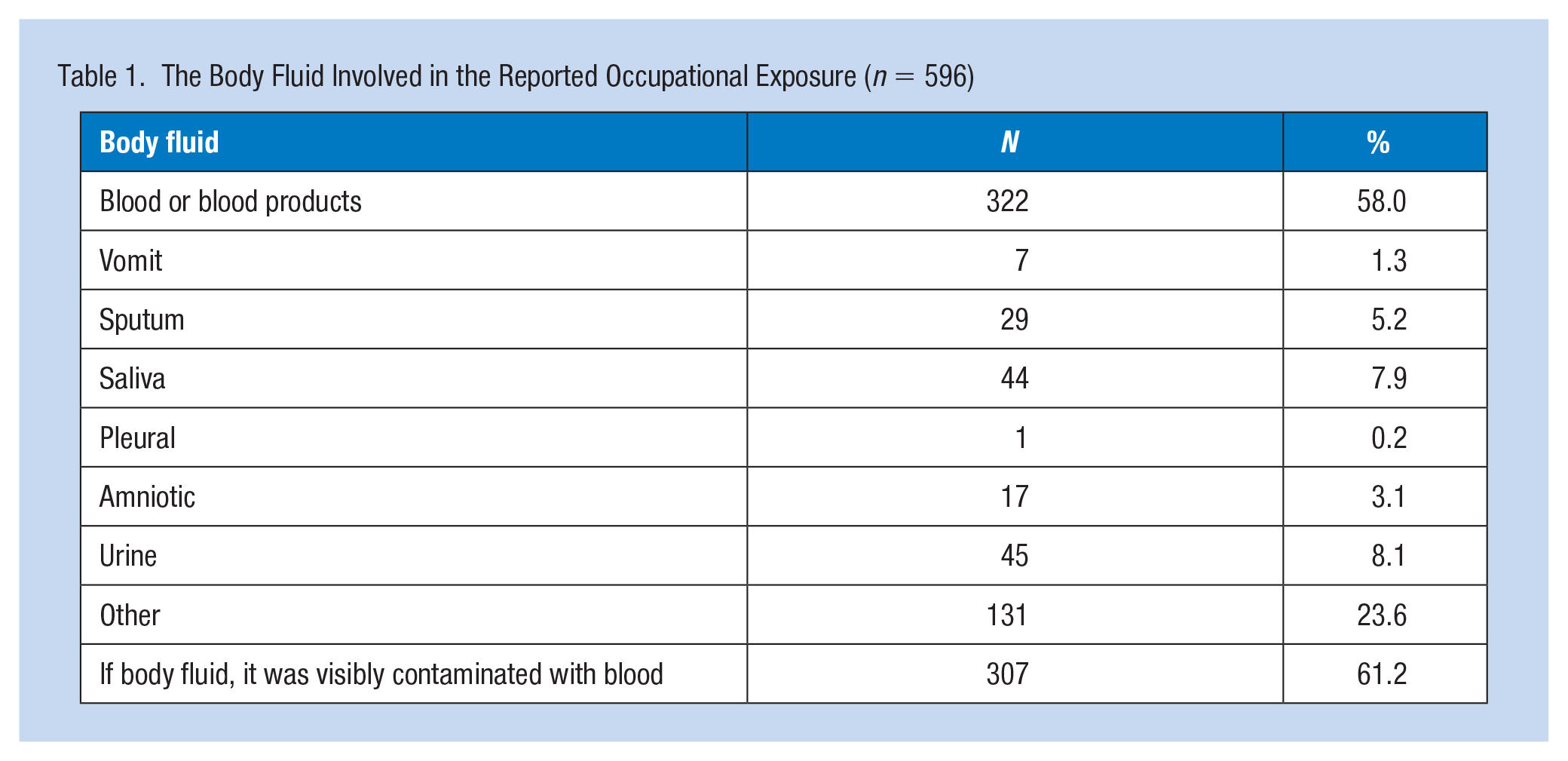
The most common body fluid involved in the BBF exposures was blood or blood products (n = 322, 58.0%), followed by urine (n = 45, 8.1%), and saliva (n = 44, 7.9%). The body fluid was visibly contaminated with blood among 307 (61.2%) reported exposures. This is important as urine and saliva are not included as other potentially infectious materials in the OSHA Bloodborne Pathogens Standard, however, when they are visibly contaminated with blood, they are included. The body fluids involved in reported occupational exposure are summarized in Table 1.
The Body Fluid Involved in the Reported Occupational Exposure (n = 596)
Reported exposures to BBFs are summarized in Table 2. The most common job category of exposure was among Nurses (57.0%), which included the “nurse” and “nursing student” responses. Physicians were defined by “doctor” and “medical student.” Patient Care Providers, Specialty and Support category included the “home health aide,” “respiratory therapist,” “physician assistant,” “phlebotomist,” “intravenous team,” and “other attendant” response options. Ambulatory, Laboratory, and Administrative Personnel included “clinical laboratory worker,” “technologist,” “dentist,” “security,” and “paramedic” as response options.
Occupational Exposures (N = 571) to Blood or Body Fluid and Personal Protective Equipment (PPE) in 2021
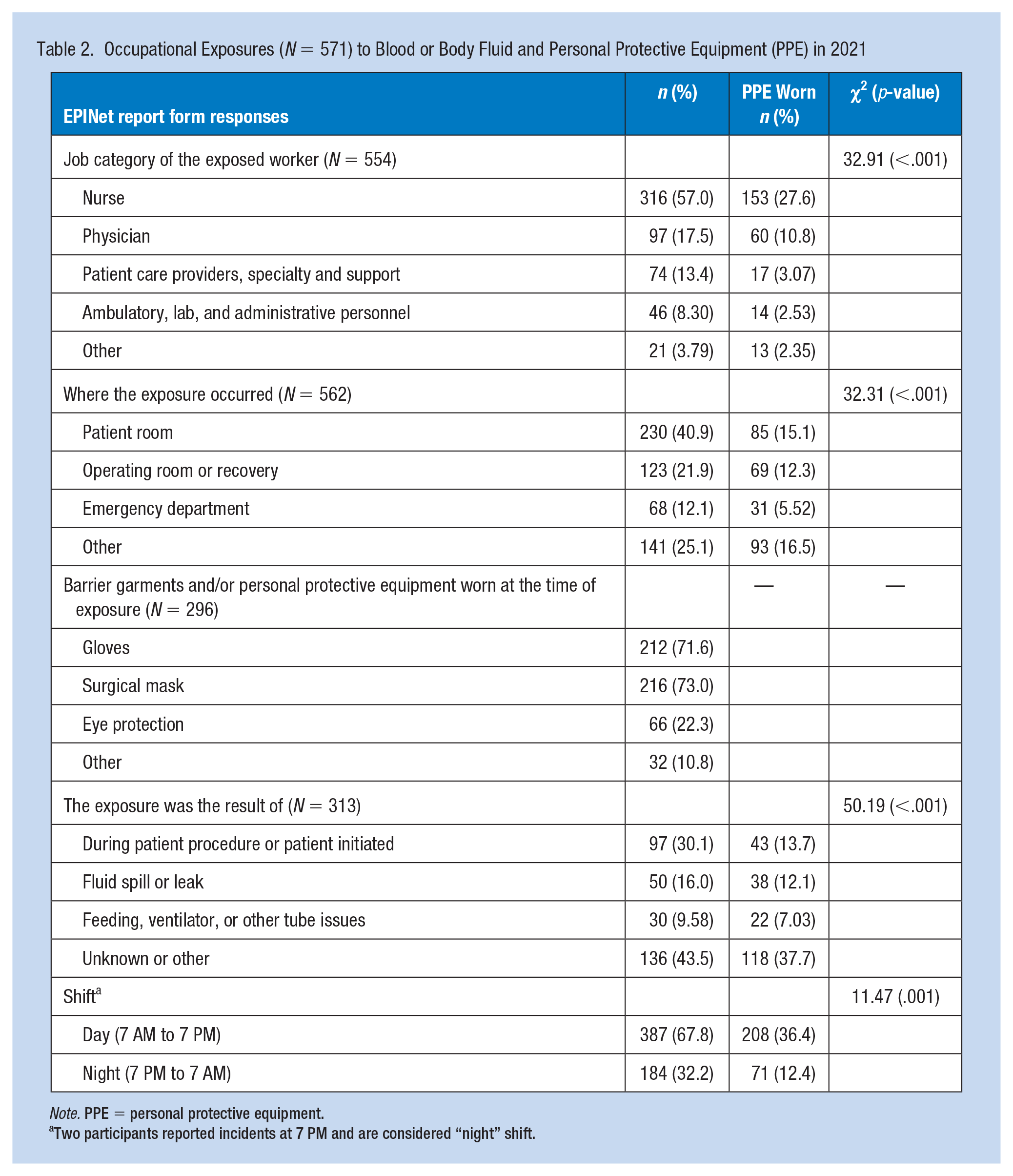
Note. PPE = personal protective equipment.
Two participants reported incidents at 7 PM and are considered “night” shift.
There were statistically significant differences between participants who wore PPE at time of exposure versus those who did not with job category (χ2 =32.91, p-value = < .001); where the exposure occurred (χ2 = 32.31, p-value =< .001); what the exposure was a result of (χ2 = 50.19, p-value = < .001); and day versus night shift (χ2 = 11.47, p-value = < .001).
Respondents did not report wearing respirators (0%), despite the focus on respiratory protection during the COVID-19 pandemic. Though surgical masks are not considered PPE for worker protection, 73% did report wearing a “surgical mask” during the exposure. It may be that if employees are exposed while wearing PPE that they do not report it and therefore, those wearing respirators and faceshields, for example do not report the incident and therefore are not captured.
Of those workers reporting an exposure, 116 (97.48%) indicated the blood was a “small amount (up to 5 cc)” that came in contact with skin or mucous membranes. There were not enough responses to >5 minutes of contact time to generate an analysis, with 80 (74.8%) reported <5 minutes of contact time.
Among those who reported BBF exposure touched or soaked the skin or protective garment of the HCW (n = 112), 83 (74.1%) reported BBF touched unprotected skin, 25 (22.3%) touched skin between gap in protective garments, 3 (2.7%) soaked through barrier garment or protective garment, and 2 (1.8%) soaked through clothing uniform.
There were no records where the worker reported having to remove a garment and obtain a replacement. There were no incidents reported that were exposures to hazardous drugs, such as chemotherapy or antineoplastics.
The frequency of where the exposure occurred on the body (N = 376) is summarized in Table 3. Despite the added focus to eye protection during the COVID-19 pandemic, most BBF exposures occurred to the eyes (n = 275, 73.1%), and only 11.2% indicated wearing some kind of protection that included the eyes (eyeglasses with side shields, goggles, faceshield).
The Location on Body of Occupational Blood or Body Fluid Exposure in 2021 (N = 376)
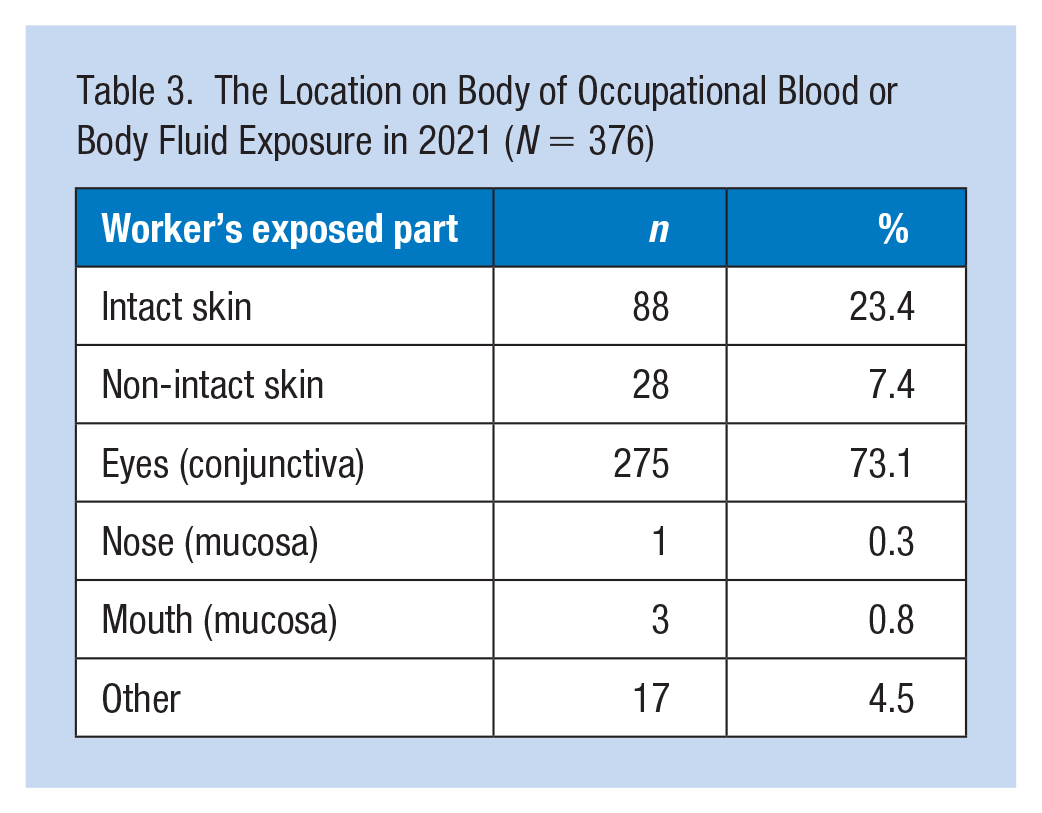
Skin exposure was reported among 116 responses (30.8%) with non-intact skin making up 7.4% of those exposures. No workers reported wearing a surgical gown or any type of protective clothing. Only one person indicated they were wearing an apron at the time of exposure.
Exposures were noted most frequently (30.1%) while performing a patient procedure, such as specimen collection, patient coughing or sneezing, placing urinary or vascular catheter and patient biting or spitting. Specimens or containers leaking occurred with next frequency (16.0%) and blood or body fluids coming from feeding, ventilator, or other medical tubes (9.58%). There were free text incidents filled out describing the incidents further and some notable ones are captured in the next qualitative section.
Exposure Incidents, Qualitative Data
Participants described the activities they were performing when the BBF exposure occurred. Incident exposures occurred often in surgery and emergency room situations and splashed from the wound to the face, eyes, arms, hair, and clothing of HCWs. There were also incidents where emergency medical services were involved and exposed: During the intubation blood sprayed out of the AMBU bag and patient’s mouth. Face shields were placed after the blood started to spray. However, blood spray had come into contact with my upper facial area and a wound on my arm prior to placing the shield. After the code was over, it was made known to me that the patient has a history of hepatitis C During our operation we got into arterial bleeding and the blood splashed my face including my mask, glasses, forehead and skin and right eye despite wearing safety glasses Upon arrival of the patient, medical staff were attempting to move him over to our stretcher. Once onto our stretcher, the patient became violent trying to sit up and get out of the bed. I was to the patients right at the head of bed when he looked to my direction and spit in my face. This patient had a previous mouth injury with bleeding involved and was not wearing a mask. Blood was noticed on my right eyelid, my mask and my neck. I immediately washed my eyes and contacted supervisory
Respondents often described eye exposure to BBF and the relationship of wearing protective equipment, citing at times patients spitting blood in the face or HCWs. Unprotected skin contact was mentioned among various BBF incident reports: I walked into the room and the patient had pulled her trach collar off, all monitor wires, IV solution, and had pulled an AC IV out of her left arm and blood was everywhere. I was in the doorway and blood hit me in the face. It got on my mask and on top of my reading glasses and in my left eye Unit of blood sent through tube system was leaking, got blood on both hands, was not wearing gloves, washed hands immediately RN and I were giving the patient a bath. After she and I were done, I took my gloves off and there was blood on my left hand. The blood was transferred from my shirt to my ungloved hand where I have a small cut on my thumb. This patient is HIV positive and I am unsure if the blood touched my cut
Patients were found to sometimes bite, hit, kick, scratch, spit and commit other violent and aggressive actions against HCWs resulting in BBF exposure: While performing a nasopharyngeal swab on a pediatric patient the patient bit my finger. The bite punctured through my PPE and broke the skin on my finger. Causing bleeding and bruising Patient was being combative. . .upon attempting to give Ativan via right arm peripheral IV, patient turned head and spit a large amount of sputum in my left eye and the left side of my face Dispatched to unknown call for the ambulance. Upon arrival police department was on scene and patient was very combative and not willing to cooperate with EMS. My partner then called the doctors to get orders. After orders were received, patient then was asked nicely to cooperate with EMS, patient didn’t cooperate and that’s when she started spitting and it may have gotten into my eyes and patient then was stating that she has AIDs
Discussion
Despite being amid a global pandemic, high-risk mucocutaneous exposures are occurring and PPE is still extremely under-utilized putting HCWs at ongoing and unacceptable risk of occupational exposure to blood-borne and infectious disease. The EPINet findings are consistent with eye exposure being the most frequent body location of BBF exposure and that the majority of occurrences happen in the patient and operating rooms/departments. Compared with 2020, there was a slight decrease (0.5%) in 2021 in eye protection usage. There was a jump in usage of “surgical masks” from 2020 (57.8%) to 2021 (73%). Although these do not protect the eyes and while they are intended for source control, rather than used as PPE, it does indicate an improved trend. Unfortunately, in both 2020 and 2021, no (0%) workers indicate wearing a respirator at the time of the exposure. Whether this is because they are not wearing one or because they are inappropriately classifying a respirator like an N95 warrants future research and attention.
PPE Usage and Exposure
There were numerous incidents describing how BBF exposures occurred when the HCW was not protecting their skin and face, especially their eyes. Blood and body fluid touching unprotected skin and the lack of eye protection were supported by the results.
To consider, it may be that if employees are exposed while wearing PPE that they do not report it, meaning that the PPE was accomplishing its purpose and the splash or splatter was on the PPE itself. It may not be that no one was wearing a respirator, it may rather be that those wearing respirators and faceshields, for example do not report the incident and therefore these incidents are not captured. This is a limitation of the data, as it is not a survey and does not capture all PPE being worn during incidents. It just shows the exposure incidents that resulted in mucocutaneous exposures despite other PPE being worn.
Improving PPE use can be accomplished by having it immediately accessible where and when needed, as well as worker training about proper donning, doffing, and disposal. For example, face protection like faceshields and goggles are not traditionally on infection prevention carts or wall mounts meaning that if a worker feels that they are at risk of a face exposure during work, they have to proactively go find it and put it on.
The accessibility to PPE may prevent BBF exposure among HCWs by having it available in practical ways when exposure is possible. Given the large proportion of health workers that wear glasses for correcting vision, it is also important to have face protection that can be used in combination with eyeglasses or eye protection that includes corrective lenses.
Since the facility’s ECP is required to include the exposure determination and the controls and PPE put in place to prevent exposures, using exposure incident and OSHA 300 log data can be a useful tool for identifying where to focus and what improvements to make. This applies to not just type of PPE used, but location, training elements, and feedback from frontline employees about what engineering controls and work practices should be used to protect them.
There is a need to further educate and train employers on how to make PPE more readily accessible and what ensembles are available for purchase and use. There is also a need to improve training and awareness for HCWs to recognize biological and bloodborne hazards in and outside of patient care areas. Healthcare workers need to have readily available access to PPE and are required to have annual training to recognize when and how to wear such equipment.
Some incidents occurred when the BBF was not anticipated, underscoring the need to implement greater controls and practices in the hierarchy of controls that can prevent BBF exposure. However, the majority of incidents did occur during frequently performed procedures like leaking specimen containers, placing or maintaining vascular lines or catheters, or from feeding tubes. Reviewing a facility’s data and descriptions about how the exposures occurred is a useful way to address the most frequently occurring first and to put controls and PPE in place to prevent them in the future.
Violence in the Workplace
Some cases were the result of combative and aggressive patients who bit, spit, and committed other acts of violence against the HCW. There is a need to better protect HCWs not just from the exposure to BBFs but have access to PPE, and also have systems in place to prevent and respond to violent patient behaviors. A violence plan may support healthcare facilities in having a mechanism on how to prevent and respond to such incidents and may reduce BBF exposure to HCWs. Although OSHA does not have a workplace violence standard, if there is potential exposure to blood or body fluids during incidents, they also need to be addressed in the facility’s ECP.
Limitations and Strengths
The study relies on the reporting of HCWs at the facility level and by occupational health professionals reporting it annually to the Center, this can contribute to volunteer bias. Although post-exposure prophylaxis for HIV and HCV need to occur as quickly as possible, often within 1 to 2 hours, some workers may not report their exposure until days or weeks later. This can contribute to recall bias. In addition, HCWs may not report incidents out of fear of stigma or lack of awareness health and safety risk.
Workers that hold important support services like environmental services, laundry, or operations may not have the same access and awareness that a clinical professional has about risk and timely reporting in the participating facility. Oftentimes, these professional groups are contract services and as such their incident data may not appear on the EPINet forms being reported by the healthcare facility itself. This means that fewer than actual facility-based exposure incidents are reflected in this dataset.
Since EPINet only captures information about the worker and their experience, it is not designed to capture information about whether the source patient had any existing blood-borne or infectious disease. There is an EPINet Post Exposure Follow-up Form that facilities can use, but it is not reported to the Center and would be valuable to study and analyze at a later date.
There also exists no data collection regarding worker compensation. Several reporting network facilities are self-insured. And while there is a field in the report form to capture “cost” of exposure, very few OH&S EPINet users know this information or fill out that piece. Both blood-borne disease source patient prevalence and worker baseline as well as worker compensation data collection should be explored in future studies.
Implications for Occupational Health Practice
There continues to be risk to BBF exposure among HCWs that put personnel at unacceptable levels of vulnerability to blood-borne and infectious disease. This study may help occupational infection prevention and control practitioners, risk managers, healthcare leadership identify ways to monitor and to develop surveillance systems to track BBF exposures and PPE availability and usage among those working in patient and resident care in any setting.
It can also add in more effective documentation of risks and controls in an employer’s ECP as part of OSHA Bloodborne Pathogens compliance. Since high-risk exposures and lack of PPE use are still happening despite increased attention to PPE use during a global pandemic, it becomes clear that OSHA is also not adequately enforcing the Bloodborne Pathogens Standard, quality, and accrediting organizations such as Centers for Medicare & Medicaid Services and Joint Commission, and Food and Drug Administration are not taking effective action, and employers do not feel enough pressure to improve working environments.
There is a need for more hospitals to participate by joining something like EPINet or developing other surveillance systems to monitor BBF exposures to illustrate to policymakers and regulatory bodies, that mucocutaneous exposures are continuing to happen and PPE use is not adequate. To better quantify how and where exposures are happening, more robust occupational incident surveillance and data sharing and publishing must be done. Since the Bloodborne Pathogens Standard requires maintaining a Sharps Injury Log, it may be useful for OSHA to explore expanding this beyond sharps and needles and into mucocutaneous exposures as well.
Applying Research to Occupational Health Practice
High-risk exposures to the eyes continue to be the most frequently occurring incident type and most workers are not wearing eye (goggles) or face protection (face shields) during the exposure. Face and eye protection did not improve significantly prior to and during the pandemic, illustrating the need to continue to stay focused on preventing occupational blood and body fluid mucocutaneous exposures. Improved blood and body exposure incident surveillance is an important tool in preventing future exposures and increasing personal protective equipment (PPE) availability and use at a facility- and national level.
Encouraging employees to report mucocutaneous splashes and splatters is not only important for Occupational Safety and Health Administration (OSHA) recordkeeping and blood-borne pathogens compliance but also to improve post-exposure medical evaluation, follow-up, and prophylaxis if needed.
Supplemental Material
sj-docx-1-whs-10.1177_21650799231163132 – Supplemental material for Blood and Body Fluid Exposure Among Healthcare Workers and Personal Protective Equipment Usage in the United States
Supplemental material, sj-docx-1-whs-10.1177_21650799231163132 for Blood and Body Fluid Exposure Among Healthcare Workers and Personal Protective Equipment Usage in the United States by Eric Persaud, Ginger B. Parker and Amber Hogan Mitchell in Workplace Health & Safety
Footnotes
Acknowledgements
Thank you to our EPINet network facilities for continuing to help us drive national and international awareness about the importance of incident and exposure surveillance for sharps injuries, needlesticks, and mucocutaneous (blood and body fluid) exposures. During this critical time, based on experiences and data from our EPINet network facilities, we can help to shape and improve the public health landscape.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The International Safety Center is a 501c3 IRS-designated non-profit. EPINet surveillance and study are self-funded by the Center.
Human Subjects
This analysis of hospital-reported data is not subject to human subjects oversight.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.