
Abstract
Background: Although nurses are well described as being at risk of work-related asthma, certified nurse aides (CNAs) are understudied. Using a statewide registry in Texas, we measured prevalence and risk factors for work-related asthma and bronchial hyperresponsiveness (BHR) symptoms among CNAs. Methods: For this cross-sectional study, a questionnaire was mailed to a random sample of CNAs (n = 2,114) identified through the Texas Department of Aging and Disability Services registry, working in health care during 2016–2017, to collect data on job history, asthma symptoms, and sociodemographics. Two outcomes were defined: (a) new-onset asthma (NOA) after entry into the health care field and (b) BHR-related symptoms. Job exposures to cleaning compounds and tasks were assigned using an externally coded CNA-specific job-exposure matrix. Logistic regression modeling was used to measure associations between cleaning exposures and the two asthma outcomes. Findings: The final sample consisted of 413 CNAs (response rate 21.6%). The prevalence of NOA and BHR symptoms were 3.6% and 26.9%, respectively. In adjusted models, elevated odds for BHR symptoms were observed for patient care cleaning (odds ratio [OR] = 1.71, 95% confidence interval [CI] = [0.45, 6.51]), instrument cleaning (OR = 1.33, 95% CI = [0.66, 2.68]), building-surface cleaning (OR = 1.39, 95% CI = [0.35, 5.60]), exposure to glutaraldehyde/orthophthalaldehyde (OR = 1.33, 95% CI = [0.66, 2.68]), and latex glove use during 1992–2000 (OR = 1.62, 95% CI = [0.84, 3.12]). There were too few NOA cases to warrant meaningful regression analysis. Conclusion/Application to Practice: Although not statistically significant, we observed elevated odds of BHR symptoms among nurse aides, associated with cleaning exposures, suggesting this is an at-risk group of health care professionals for work-related respiratory disease, meriting further study.
Keywords
Introduction
Asthma is both a health and economic concern in the United States, with a lifetime prevalence of 8% among adults (Centers for Disease Control and Prevention [CDC], 2019a). Work-related factors are implicated in one out of every six cases of asthma in working-aged adults (Arif et al., 2002; Balmes et al., 2003; Kogevinas et al., 2007; Mazurek & Syamlal, 2018). Work-related asthma (WRA) encompasses both pre-existing asthma worsened by workplace factors (i.e., work-exacerbated asthma) and new-onset adult asthma caused by a workplace sensitizer or irritant (i.e., occupational asthma, OA). Overall, OA accounts for approximately 10% to 25% of adult-onset asthma cases (Cartier & Bernstein, 2016; Dykewicz, 2009; Maestrelli et al., 2009). Workers at risk of OA include bakers, isocyanate workers, Western red cedar workers, spray painters and, more recently, health care workers (HCWs) (Ameille et al., 2003; Delclos et al., 2007; Jeebhay et al., 2019; Jeebhay & Quirce, 2007; Latza & Baur, 2005; Vandenplas et al., 2005). According to recent statistics from Bureau of Labor Statistics, the resulting 2016 cost for WRA was estimated to be US$2,281 per case (Caridi et al., 2019; Dodd & Mazurek, 2016). With over 2 million U.S. workers having WRA in 2016, the projected annual cost of WRA was around US$6 billion (Dodd & Mazurek, 2016).
Previous studies have described an increased occurrence of WRA among specific HCW groups, notably nursing, in association with exposures involving cleaning, disinfecting, use of powdered latex gloves, and administration of certain aerosolized medications (Delclos et al., 2007; Meredith et al., 1991; Vandenplas et al., 1995; Vizcaya et al., 2015). Among nursing professionals, registered nurses had the highest prevalence of new-onset adult asthma (10.2%), followed by vocational nurses (8.0%), nurse practitioners, and nurse aides (6.9% each) (Arif et al., 2009). Nurses reported a significantly higher risk of new-onset physician-diagnosed asthma and nasal symptoms at work than administrative staff working in health care. This risk was particularly marked during cleaning and disinfection tasks, including with exposure to quaternary ammonium compounds, a commonly used disinfectant and known sensitizer (Folletti et al., 2017; Gonzalez et al., 2014). The use of latex gloves between 1992 and 2000 was found to be a risk factor for both new-onset asthma and symptoms, but this risk decreased after 2000 due to widespread implementation of policies to reduce the use of latex in health care setting in the year 2000 (Delclos et al., 2007), suggesting that the policies had a beneficial effect. Importantly, nurses are at greatest risk, with at least twice the odds of reporting asthma compared to physicians (Arif et al., 2009; Delclos et al., 2007). However, there are many subgroups of nursing-related occupations, and risk is likely to vary according to subgroup (Arif et al., 2009). In addition, there has been a significant growth in nursing professions and also more diverse classification of nursing occupations, including nursing assistants and home health aides (Arif et al., 2009).
In 2014, there were 1.5 million jobs related to nursing assistants and orderlies in the United States, which is projected to increase by 17% by 2024 (Bureau of Labor Statistics, 2016). Nurse aides assist other higher nursing professions and physicians by providing hands-on care to patients in various settings, cleaning and disinfecting tasks, feeding patients, performing light housekeeping duties in patient rooms, providing skin care, and/or changing bed linen (America’s Job Exchange, 2016). Consequently, they may represent a greater at-risk group among health care professionals, by engaging in cleaning and disinfection to a greater extent. Studies have also shown a clear social gradient across workforce categories, which is widening over time. Within workforce categories, there are significant racial disparities in health status and prevalence of obesity among different types of nursing professions (Chou & Johnson, 2008). Nurse aides are often less educated and poorly paid despite being accountable for major caregiving responsibilities (Mercer et al., 1994). In some cases, they may also lack equivalent benefits, such as health insurance, as compared to other health care professionals (Squillace et al., 2009). This all underscores the importance of an increased focus on nurse aides with respect to their occupational risks and health.
This study focuses on certified nurse aides (CNAs) registered by the Texas Department of Aging and Disability Services. We examined the prevalence of asthma risk factors and WRA among CNAs, and associations of asthma and asthma symptoms with exposures to selected cleaning products, tasks, and practices.
Methods
This was a cross-sectional survey of CNAs working in Texas, conducted in 2016–2017. The primary outcomes of the study were new-onset asthma after entry into the health care field, and bronchial hyperresponsiveness (BHR)-related symptoms, and exposures were coded externally using a job-exposure matrix (JEM) specific to CNAs.
Study Population and Recruitment
The target population and sampling frame consisted of 108,718 CNAs registered in 2016 through the Texas Department of Aging and Disability Services. Based on sample size calculations to achieve adequate power, the survey was mailed to 2,114 randomly selected CNAs during 2016–2017, using six contact waves, comprised of introduction letters, questionnaire with U$1 incentives, resends and final postcard reminder. This method was modified from those proposed by Dillman et al. (2009). Informed consent in the form of an introduction letter was provided to all the participants who either responded by mail or online.
Data Collection
Questionnaire
The survey instrument was adapted from a validated questionnaire previously developed to study asthma in HCWs (Delclos et al., 2006, 2007). The questionnaire included occupational exposures and non-OA-related risk factors (e.g., pre-existing allergies) as well as items on asthma from which we defined two health outcomes: (a) physician-diagnosed asthma with onset after entry into the health care profession (“new-onset asthma”), based on the questions “Have you ever had asthma?” and “If YES, has your asthma been confirmed by a doctor?.” To determine “new onset for persons with a history of physician-diagnosed asthma,” we compared the age at which this diagnosis was made to the number of years employed as a health care professional. Asthma that began after entry into the health care field was considered “new onset” and (b) presence of BHR-related symptoms, determined based on a previously validated eight-item, symptom-based predictor of PC20 (provocative concentration of methacholine causing a 20% fall in FEV1) of 4 mg/mL for methacholine (Arif et al., 2009; Delclos et al., 2007). The eight items from the questionnaire were based on asthma and allergy symptoms. The asthma symptoms included were (a) trouble breathing, (b) wheezing in the previous 12 months, (c) attacks of shortness of breath in the previous 12 months, (d) nocturnal cough in previous 12 months, and (e) chest tightness in the previous 12 months. Allergic symptoms included (a) itchy or watery eyes in the presence of animals, feathers, or dust; (b) chest tightness in the presence of animals, feathers, or dust; and (c) itchy or watery eyes in the presence of pollen or near trees, grass, or flowers (Delclos et al., 2006). Along with questions on asthma and allergy, other questions were related to occupational history and demographics including age, sex, race/ethnicity, years as health professional, smoking, and obesity.
Job Exposure Matrix
Job exposures were assessed using an externally developed and coded JEM, specifically designed for CNAs (Delclos et al., 2007). The JEM structure was based on walkthroughs and focus groups led by a multidisciplinary team of occupational health professionals, conducted in three hospitals, three nursing homes, and two outpatient clinics in Houston in 2015 (Delclos et al., 2007). On the exposure axis of the JEM, cleaning-related exposures were classified into two broad categories: (a) tasks and (b) compounds. Tasks consisted of patient care cleaning and disinfection, instrument cleaning (including endoscopy), and building surface cleaning (including use of sprays). Compounds were classified into cleaning agents that included glutaraldehyde, orthophthalaldehyde, enzymatic cleaners, bleach, quaternary ammonium compounds, sprays, and powdered latex glove use from 1992 to 2000. On the job axis, CNAs were classified by their place of practice, which included hospitals and hospital units such as intensive care units, nursing homes, home health settings, outpatient clinics, and other respective units.
The JEM was developed and coded before administering the survey. Six experts (one occupational physician, one environmental safety specialist, two industrial hygienists, and two research health scientists) assigned codes to each cell of the JEM, based on the probability that the majority of workers in that cell were occupationally exposed at least once per week to this class of agents. A code of “0” was assigned if there was a high probability of no exposure; a “1” or a “2” was assigned when the probability of exposure at least once a week was low or high, respectively. Disagreements were resolved by consensus among the expert panel. The coded matrix was then applied to each respondent’s current and longest held jobs as a CNA, based on the job title and practice setting reported for that job.
After examining the coded JEM, it became apparent that the number of occupation–practice setting combinations assigned a code “1” (low probability) for exposure was very small for almost all considered exposures. As a result, this intermediate exposure group was too small for meaningful analyses. Therefore, occupational exposure variables were dichotomized by collapsing codes 1 and 2 from the JEM into a single “exposed” category, with code “0” reflecting the non-exposed groups. Job-exposure matrix codes for longest held HCW/CNA job were used because the majority (59%) of respondents indicated their current job was also their longest held job. For those whose longest held job was outside the health care sector, JEM codes from their current CNA job were used.
Covariates from the questionnaire included age, sex, race/ethnicity, years as a health professional (i.e., years at job), smoking, obesity (i.e., body mass index [BMI] ≥30 kg/m2), and atopy (yes/no). Atopy was defined based on a previously validated combination of history of allergies to dust and animals (Delclos et al., 2006).
Data analysis: Post-stratification weighting was performed to obtain estimates of both counts and prevalences that were representative of the actual population size (i.e., the state list of 108,718 CNAs), based on four age groups: ≤25, 26–40, 41–60, and ≥61 years. Descriptive statistics were assessed to compare characteristics of the analytical sample (n = 239) and the excluded sample (n = 174, consisting of those with any missing values for either exposures or outcomes) out of a total 413 CNA respondents.
All regression analyses were performed using only the analytical sample. After checking for collinearity using the variance inflation factor (VIF), multivariable logistic regression models were conducted for tasks and compounds and their associations with BHR symptoms and new-onset asthma, adjusted for race, atopy, obesity, smoking, and years at job. Only models with adequate counts and meaningful analyses were reported. Moderate to strong collinearity (>70%) was found mainly among building surface cleaners (bleach and quaternary ammonium compounds), patient care cleaners, and latex use (before 1992). Thus, separate multivariable regression models were built for different subclasses of exposures in the JEM. Associations were expressed as the adjusted odds ratios (ORs) and corresponding 95% confidence interval (95% CI). Goodness of fit was assessed as recommended for survey sample data (Archer & Lemeshow, 2006). Stata/SE v. 14.0 was used for the statistical analyses (StataCorp, 2019).
The study was approved by the University of Texas Health Science Center at Houston Committee for the Protection of Human Subjects.
Results
After removing 10 incorrect addresses, surveys were mailed to 2104 CNAs in Texas. Of these, 311 were returned as “undeliverable address” and were replaced with individuals from a new randomized list from the registry to obtain an additional 90 responses. Of the total 455 respondents (21%), 25 refused to participate, 17 no longer worked as CNAs and their longest held job was not as a CNA. Thus, the final sample for analysis consisted of 413 participants with a final overall response rate of 21.6%.
Table 1 summarizes the descriptive statistics for the final analytic sample (n = 239) and the excluded sample with missing data (n = 174). Compared to the analytic sample, the excluded sample had significantly higher atopy (p < .001) and weighted prevalence of BHR symptoms (p = .03). There were no significant differences between samples with respect to age, gender, race, obesity, smoking status, or years at job. In the analytical sample, the overall weighted prevalence estimates for new-onset asthma and BHR-related symptoms were 3.6% and 26.9%, respectively. Ninety percent of respondents (n = 216) were female. The weighted prevalence of obesity, BMI ≥30 kg/m2, was 41.2% (n = 101); 36.7% (n = 85) of respondents were Hispanic, and 75.3% (n = 178) were non-smokers.
Descriptive Statistics for Analytical Sample (n = 239, All Missing Values Excluded) Versus Excluded Sample (n = 174, Only Those With Any Missing Value) Out of a Total 413 CNA Respondents, 2016–2017
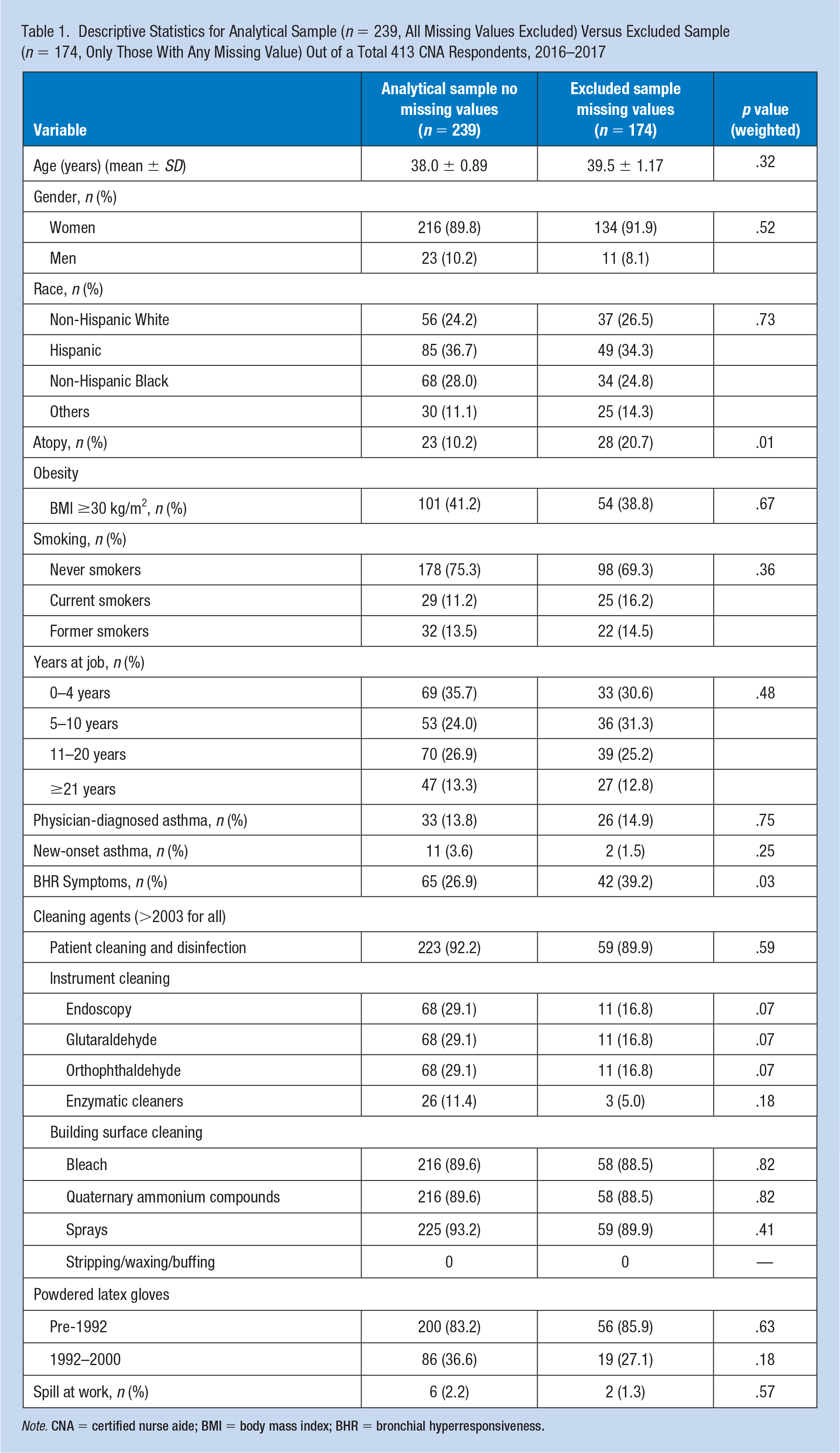
Note. CNA = certified nurse aide; BMI = body mass index; BHR = bronchial hyperresponsiveness.
Since there were very few cases of new-onset asthma (n = 11), only BHR symptoms were considered as the main outcome in the multivariable analysis. Of these 11 new-onset asthma cases, five were current or former smokers, and three had atopy. Two reported a simultaneous diagnosis of chronic obstructive pulmonary disease (COPD)/emphysema; both had a history of smoking. Over 50% of new-onset asthma cases reported exposures to bleach, abrasive cleaners, detergents, disinfectants, and nebulized drugs.
Table 2 presents the univariate analysis for BHR symptoms. Positive associations were found for obesity, years at job, and latex glove use in the 1992–2000 time period. For race, an inverse association was observed for BHR-related symptoms among non-Hispanic Blacks (OR = 0.39, 95% CI [0.16, 0.94]) as compared to non-Hispanic Whites.
Univariate Analysis for Analytical Sample (n = 231—Excludes Missing Values) Between Independent Variables Assessed by Job-Exposure Matrix Among Texas CNAs and the Two Asthma Outcomes, Weighted by Age Groups
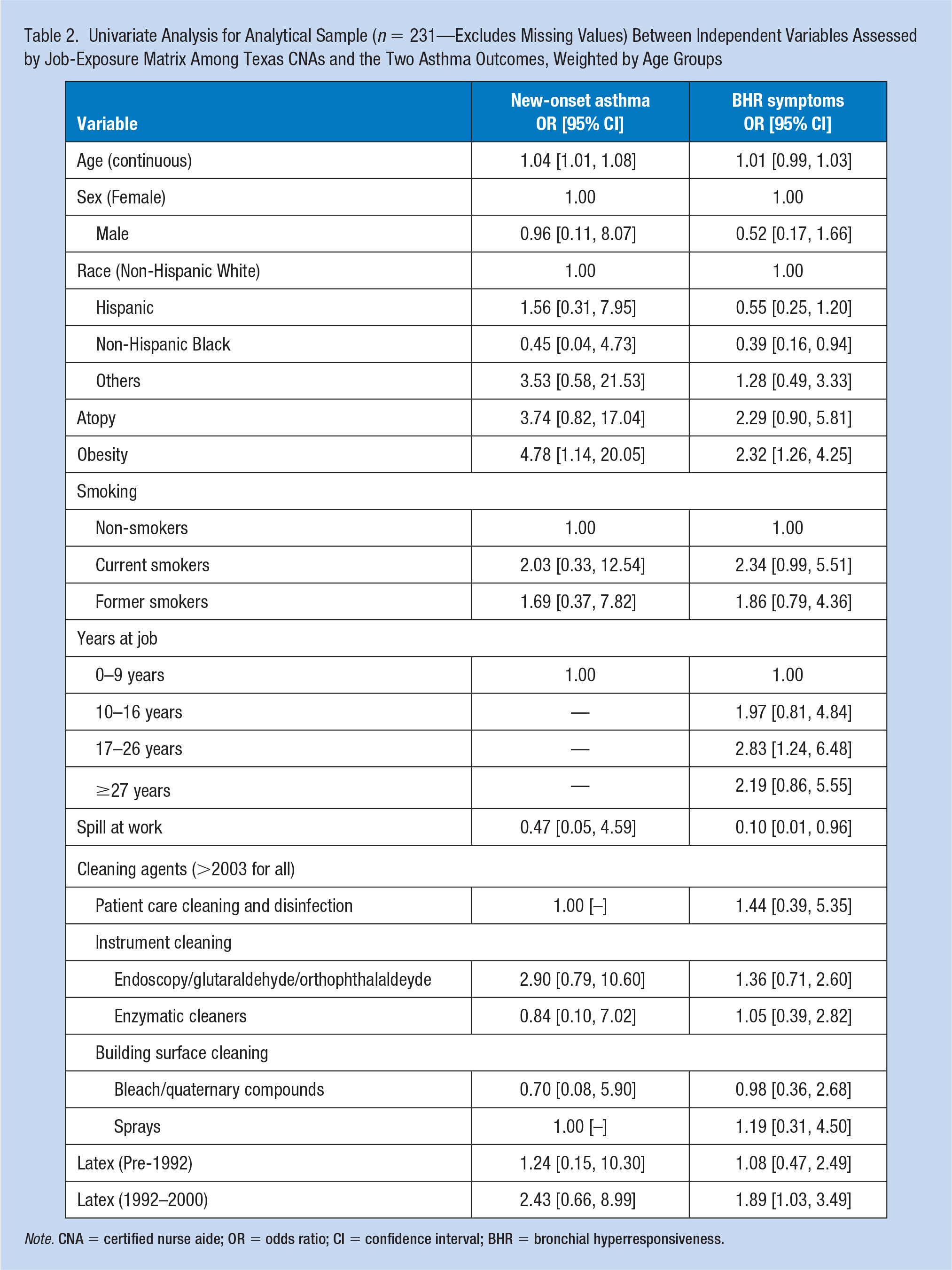
Note. CNA = certified nurse aide; OR = odds ratio; CI = confidence interval; BHR = bronchial hyperresponsiveness.
The final multivariable models with BHR symptoms as the outcome were adjusted for race, atopy, obesity, smoking status, and years at job (Table 3). There were no statistically significant associations, but some showed elevated point estimates. For tasks, elevated odds for BHR-related symptoms were observed for patient care cleaning and disinfection (OR = 1.71, 95% CI = [0.45, 6.51]), instrument cleaning that included endoscopy (OR = 1.33, 95% CI = [0.66, 2.68]), and building surface cleaning that included sprays (OR = 1.39, 95% CI = [0.35, 5.60]). For compounds, elevated odds were observed for instrument cleaning compounds including glutaraldehyde (OR = 1.33, 95% CI = [0.66, 2.68]), orthophthalaldehyde (OR = 1.33, 95% CI = [0.66, 2.68]), enzymatic cleaners (OR = 1.23, 95% CI = [0.39, 3.86]), and use of latex gloves from years 1992–2000 (OR = 1.62, 95% CI = [0.84, 3.12]).
Multivariable Logistic Regression Analysis for Tasks and Compounds and Their Association With Bronchial-Hyperresponsiveness (BHR) Symptoms
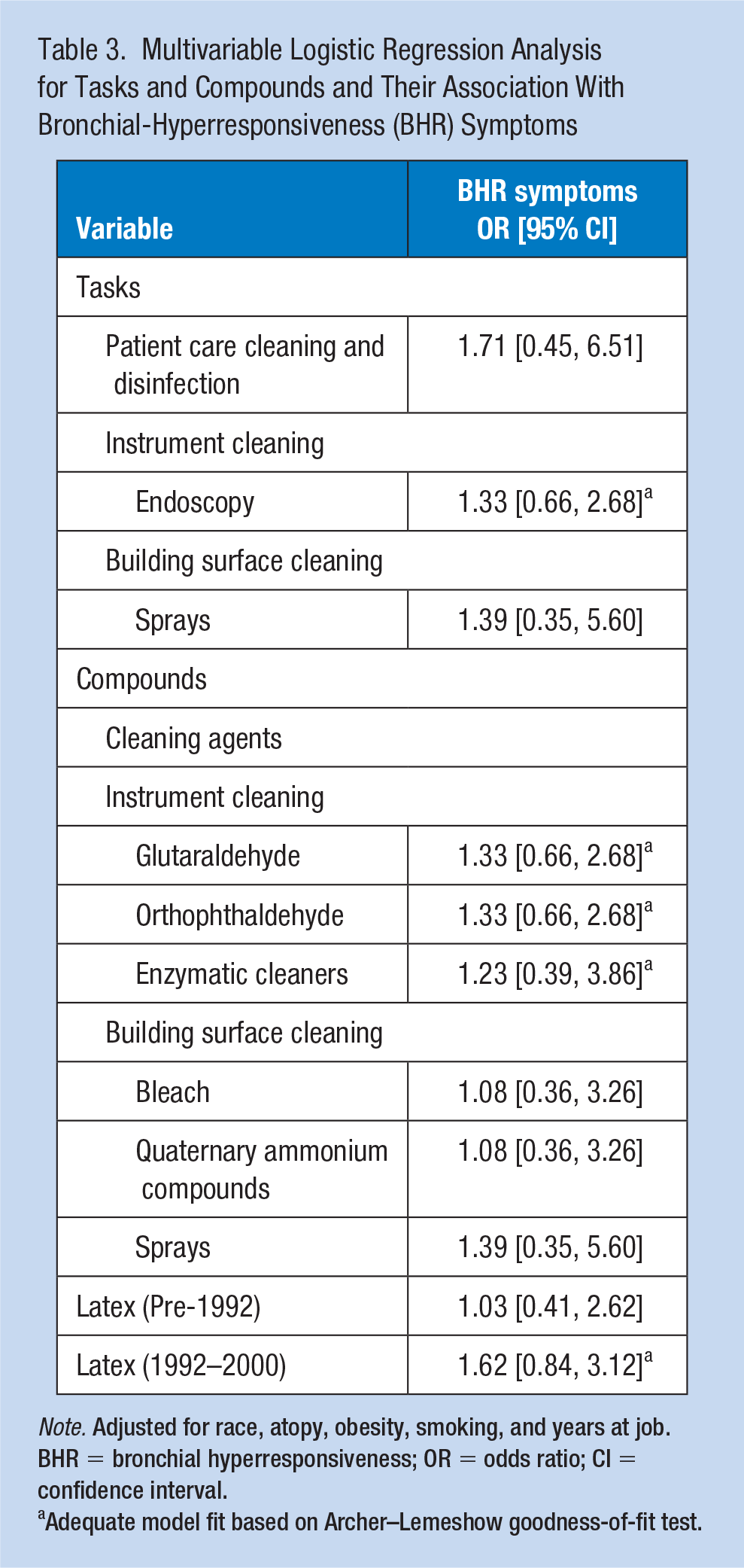
Note. Adjusted for race, atopy, obesity, smoking, and years at job. BHR = bronchial hyperresponsiveness; OR = odds ratio; CI = confidence interval.
Adequate model fit based on Archer–Lemeshow goodness-of-fit test.
Model fit was good for models with BHR-related symptoms for instrument cleaning classes and latex glove use from 1992 to 2000 (Archer–Lemeshow goodness of fit, p > .05), but not for the other exposure models, that is, patient care cleaners, building surface cleaners, and sprays.
Discussion
We report several elevated odds of BHR-related symptoms for tasks performed by CNAs: patient care cleaning and disinfection, instrument cleaning (endoscopy), building surface cleaning, use of sprays, exposure to glutaraldehyde, orthophthalaldehyde, and enzymatic cleaners, as well as use of latex gloves in the period 1992–2000. Although not statistically significant, these results are consistent with previous studies that focused primarily on nurses and other major health care occupations (Arif et al., 2009). To our knowledge, this is the first study to specifically examine nurse aides, an understudied group.
These results suggest that, similar to other HCWs, nurse aides may also be at risk for WRA. The associations with cleaning tasks and products were similar or slightly less than those reported for other nursing professions. Specifically, a cross-sectional study conducted by Arif et al. among licensed Texas nurses and three other health care professional groups found a 2.7 higher odds for new-onset asthma as compared to the 1.7 times higher odds in this study. Also, for instrument cleaning, Arif et al. found a 1.7 times higher odds compared to 1.3 times in this study (Arif et al., 2009; Delclos et al., 2007; Kurai et al., 2015; Vizcaya et al., 2015). We found a lower, but still positive association for building surface cleaners, such as bleach and quaternary compounds, compared to Arif et al. (OR = 1.7). While the study design for both studies was similar, the lower and non-significant findings in our study can partly be explained by lower response rate (70% in Arif et al. study). However, the lower point estimate may be due to either bias (i.e., related to the lower response rate so the CNAs are biased regarding either the exposure or the outcome, or both) or it is the reflection of a true association (i.e., CNAs might in fact have lower odds for WRA or BHR symptoms). In addition, the lower risk could be also due, in part, to differences in workplaces among nurse aides and nurses. Nurse aides are more often employed in nursing homes, hospice, and home facilities compared to registered nurses (Bishop et al., 2008; Gruss et al., 2004). These workplaces tend to use less bleach and quaternary ammonium compounds than in hospitals (Dumas et al., 2017). Another explanation could be that cleaning practices and instruments have changed over the past decade, resulting in a lower opportunity for exposure to the same compounds. Although the need to control Clostridium difficile has led to a resurgence of bleach in recent years, we did not find bleach to be associated with an increased risk of BHR symptoms.
Our findings for use of latex gloves was similar to previous studies, reflecting a trend of marked increase in use of latex-containing protective equipment in years 1992–2000, in comparison to prior years, followed by an important decrease in its use after the turn of the century (Delclos et al., 2007).
Some demographic differences between nurses and nurse aides in Texas may also have influenced some of our results. Among these, a higher proportion of Hispanics among nurse aides (37%) could explain the low prevalence of new-onset asthma in this collective. In general, Hispanics, notably Mexican Americans, have a lower prevalence of asthma as compared to Whites and African Americans (CDC, 2019b). In the CDC report of “Most Recent Asthma Data” as of 2016 (updated May 2018), the prevalence of 5.7% of current asthma in Mexican Americans was lower than in Whites (8.3%) and African Americans (11.6%) (CDC, 2019b).
Another difference is in the age distribution, with 23.3% of our participants being under age 30 years, whereas in the study by Arif et al. (2009), only 4.1% of all nurses were in this younger age group. It is possible that this shift toward a younger workforce represents a shorter “at risk” time for developing asthma than in other nursing professionals. In addition, there is a tendency of nurse aides to change jobs sooner than other nursing professions, which would also lessen potential exposure time to workplace asthmagens. The prevalence of BHR symptoms among nurse aides (27%) was similar to that observed in other nursing professionals (31%) by Arif et al. (2009).
The study had several strengths. To our knowledge, it is the first to address the burden of WRA in the population of nurse aides. Despite the low response rate (see below), the results should be generalizable to nurse aides in Texas and possibly the United States, given its population-based design. The use of a statewide registry to identify the target population and representative sampling approach affords it external validity. Using previously validated methods for ascertainment of exposures (i.e., an updated JEM, specific to nurse aide job and practice categories) and respiratory outcomes also add solidity to the findings. Similar methods are being used in a larger, ongoing study of Texas HCWs where the data collection period overlapped with the present study. When complete, this will allow us to compare our findings in nurse aides to those of other health care professionals, and to earlier findings in the 2007 study by Delclos et al. (2007).
The study also had some limitations. The analytical sample (n = 239) was 38% smaller than the minimum estimated sample size (n = 383). Consequently, our study had less power than originally estimated to detect differences and, thus, our results were less precise (i.e., CIs were often wide) than intended. We considered multiple imputation techniques but given the main source of missingness in our sample was related to the main outcome, BHR symptoms, imputing was decided against. It is known that the outcome carries information about the missing values of the potential predictors, thus, with a large proportion of the outcome missing, the imputation procedures may have not performed adequately (Sterne et al., 2009). In addition, it was not possible to impute exposure data that was externally coded through JEM. Nonetheless, our results were coherent with prior literature, both regarding the direction and magnitude of the association estimates (i.e., ORs).
Another potential limitation was the overall response rate (21.6%) as compared to a previous study on OA in health care professionals in Texas by Delclos et al. (2007), which approximated 66%. Even though both these studies focused on OA in health care professionals, the respondent groups are not comparable as this study focuses only on CNAs that were not a part of the previous study. Since the study by Delclos et al. (2007) focused on physicians, nurses, and respiratory and occupational therapists, there is a possibility of differences in the characteristics of these groups that might be leading to a lower response rate such as frequent change in jobs and younger population in CNAs. Declining response rates to surveys in recent years have been widely described in literature, with current average response rates for health care professionals being around 30% (Bladon, 2009; Czajka & Beyler, 2016; Wiebe et al., 2012). Considering these trends, our response rate is consistent with the current norm for surveys pertaining to health care professionals. Many reasons are suggested, including internal company policies limiting participation in research, and more rigorous filtering of mail to avoid spam and phishing. Some of these reasons may underlie the low response rate in our study, along with factors more specific to nurse aides, such as their tendency to switch jobs frequently. Oftentimes the change is due to “moving up” the professional ladder, to nursing or other health care professions. At other times, nurse aides move entirely out of health care. It is possible that adding the traditional technique of telephone interviews could have improved the response rate a bit, although this may have added bias due to using a different survey approach. Also, during the analysis, it was observed that we had a greater proportion of Latino population among the respondent. If we had known this prior to initiating the study, we would have designed a Spanish version of the questionnaire that would have yielded for a better response rate. Finally, although the prevalence of BHR-related symptoms was high, the small number of new-onset asthma cases, likely influenced by reasons previously stated, precluded more detailed statistical analysis.
In summary, in this study, we observed elevated odds of asthma symptoms among nurse aides, associated with specific tasks, products, and practices, suggesting this is an at-risk group for work-related respiratory disease, as occurs with other health care occupations. Despite being limited by statistical significance, the results should serve as a starting point for further research in this worker collective. Among these, more detailed comparison of nurse aides to other at-risk health care professionals, and more detailed analysis of exposures to current cleaning products and practices, will guide in setting the stage for preventive interventions.
Implications for Occupational Health Practice
The results suggest that nurse aides may be an at-risk worker population for work-related respiratory disease. This is especially relevant considering the majority of nurse aides have several cleaning-related responsibilities in health care. Occupational health professionals can use these findings when performing clinical evaluations of nursing aides or when developing screening questionnaires for surveillance. They can also use these findings to identify risky exposures to cleaning products, practices, and procedures in this worker population; and, finally, they can counsel nurses’ aides on proper preventive measures when handling cleaning products, including safe practices and proper use of personal protective equipment.
Applying Research to Occupational Health Practice
Nurse aides are likely to use cleaning chemicals in their jobs and be at risk for asthma and BHR-related symptoms. Occupational health professionals should review cleaning chemicals and Safety Data Sheets when conducting clinical exams of nurses aides. They can also use these findings to develop respiratory medical surveillance programs as well as provide counseling and training regarding the use of engineering, administrative, and personal protective equipment to minimize exposure.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Institute for Occupational Safety and Health Grant No. 5T42OH008421—SWCOEH NIOSH Pilot Projects and R01 CDC/NIOSH Grant No. 5R01OH010648-02/010648OH14. G.L.D. and D.G.R.d.P. were partially funded by the Southwest Center for Occupational and Environmental Health, a Centers for Disease Control and Prevention National Institute for Occupational Safety and Health Education and Research Center [Grant 5T42OH008421] at the University of Texas Health Science Center at Houston School of Public Health.
Author Biographies
Jenil Patel is a postdoctoral research Fellow in the Department of Epidemiology at University of Arkansas for Medical Sciences. After receiving medical training from Gujarat, India, he received his PhD in Epidemiology from the UTHealth School of Public Health (UTSPH) in Houston with a breadth in research methods and practices in occupational health. His current research focuses on occupational and perinatal epidemiology, with an emphasis on exploration of occupational and environmental risk factors for birth defects.
David Gimeno Ruiz de Porras is professor and director of the Southwest Center for Occupational and Environmental Health, the NIOSH-funded Education and Research Center at The University of Texas Health Science Center at Houston (UTHealth) School of Public Health in San Antonio. His current research focused on cross-national epidemiological studies on working conditions and health, work-related lost productivity, and vulnerable workers.
Laura Mitchell is professor in the Department of Epidemiology, Human Genetics and Environmental Sciences at The University of Texas Health Science Center at Houston (UTHealth) School of Public Health. Her research focuses on the epidemiology and genetics of adverse pregnancy outcomes with an emphasis on maternal factors that are associated with the risk of congenital malformations in offspring.
Riddhi. R. Patel is a second year PhD Epidemiology student at the University of Texas Health Science Center School of Public Health at Houston. She works as a graduate research assistant at the Sarcoma medical Oncology department at the University of Texas MD Anderson Cancer Center that will be shaping her carrier in the field of synovial sarcoma research. She is actively involved with multiple epidemiological studies as part of her PhD program.
Joy De Los Reyes, MPH, is a senior grants and contracts specialist with the University of Texas Health Science Center at Houston School of Public Health. Her background is in public health and disease control.
George L. Delclos, MD, MPH, PhD, is tenured professor in the Department of Epidemiology, Human Genetics and Environmental Sciences (EHGES) at the UTHealth School of Public Health (UTSPH) in Houston, Professor and Marcus M. Key, M.D. - Shell Occupational and Environmental Health Endowed Chair, and Distinguished Teaching Professor of The University of Texas System. He obtained his medical degree from the University of Barcelona in 1981 and completed residency training in internal medicine and pulmonary diseases at the Baylor College of Medicine. He has an MPH degree from the University of Texas School of Public Health, a PhD in Health and Life Sciences from Pompeu Fabra University in Barcelona, and is board-certified in internal medicine, pulmonary diseases and occupational medicine.