
Abstract
This article discusses the development of professional advocacy in the U.K. nursing and midwifery professions. Initially established in midwifery, the discourse of professional advocacy has gradually shifted from a patient focus to advocating for the professionals in their professional roles. This move is driven by the need to influence the health, well-being, and efficacy of the health professions, thereby positively impacting patient care. The concept of advocacy is thus expanding from advocacy focussing on patients/social groups, to incorporating advocating for health professionals by health professionals. However, it is unclear if literature and evidence is keeping pace with this potential conceptual shift taking place in the practice setting, and it is unclear if past patient-centered conceptualizations of advocacy are relevant to the context of professional-oriented advocacy. This article aims to initiate this discussion specific to the nursing profession.
Introduction
To set the context of this article, it is important to consider three parameters within which the concept of advocacy operates. Firstly, this article is set within the U.K. National Health Service (NHS), but from the outset, we recognize that the concept of Professional Advocacy in relation to nursing and midwifery is globally applicable. Set in the practice context of an increasing workload, shortfalls in staffing and the growing complexities of care, The Courage of Compassion document (West et al., 2020) indicates that nurses and midwives’ well-being is inherently linked to their professionalism, the quality of care they provide and the health outcomes for individuals and communities. This is important because globally, nurses are the largest professional group in health care (Boniol et al., 2022) providing direct or indirect care to patients (Westbrook et al., 2011) with responsibility for quality improvement in patient care and safety of services (Makary & Daniel, 2016) alongside consistent limitations of resources (Vaughn et al., 2019). As such, the problems faced in the United Kingdom are reflective internationally.
Secondly, this article is set within a post-COVID-19 pandemic era. It is important to recognize that prior to the pandemic, there was wide recognition that the United Kingdom’s NHS workforce was chronically stressed, overstretched, and underresourced (Sykes et al., 2019). In the United Kingdom, this has been described as the pre-COVID-19 legacy, and when the pandemic hit, an already stressed (and in many cases, chronically distressed) workforce were further stretched. Alongside, health policy is seeking to catch up with, and adapt to the “new normal” of the health context, which Kluge (2022) defines as a “permacrisis,” where the frequency of crises is increasing and becoming a “new normal.”
Thirdly, as professions, the disciplines of nursing and midwifery have a long history of engaging in advocacy to strengthen and advance their professions, patient care and outcomes, health systems, and public policy. Historically, advocacy in these disciplines refers to acting on behalf of another and viewed as the cornerstone of care (DoH, 2020; Grace, 2001; Toll et al., 2023). Therefore, it is within this aspect of care that the discussions presented in this paper are located, with the aim of seeking further understanding and clarity about what the concept of professional advocacy means to contemporary nursing and midwifery practice.
In opening this discussion, we need to understand that advocacy may be considered as a taken-for-granted concept and so, an overview of what advocacy means, is needed. Conceptually, advocacy is the act of defending or arguing in favor of something, such as a cause, idea, or policy (Hearrell, 2011), and as a means for citizens and professionals to be agents of change. For advocacy to occur, there needs to be both a purpose and an action. Accordingly, advocacy can differ depending on the types of action it is associated with, for example: (a) actions based on a cause to protect/promote the health of a particular population or social group; (b) actions to strengthen people's capacity to act autonomously in order to improve their own health; (c) actions aimed at reducing structural barriers to health; and (d) actions that use the media to influence public policy initiatives (Cohen & Marshel, 2017). Nursing and midwifery are therefore ideally positioned professions to fulfill the purpose and the practice of advocacy because of their unique relationships with patients, underpinning philosophies of care and positioning of equity across practice (Cohen & Marshall, 2017; Farrer et al., 2015).
However, recognizing advocacy as a situated (practice-orientated) concept is difficult as previous and accepted notions of advocacy may be lagging the changing health care context. One example of a conceptual lag is the roll out of Professional Advocacy in the U.K. nursing and midwifery professions. Introduced firstly in midwifery following statutory changes in supervisory practice (Dunkley-Bent, 2017) then to nursing (May, 2021), the Professional Nurse Advocate (PNA) role (as a designated position within the workforce) was introduced by NHS England as a response to the system-wide recovery needed from the COVID-19 pandemic, relating to patients, services, and the workforce. Doing so, as part of a system wide response, repositioned the nursing and midwifery workforce with the remit to advocate for their fellow nurses/midwives, to respond to colleagues’ concerns, alongside the enhancement of leadership skills, engagement with quality improvement and Restorative Clinical Supervision (RCS; Capito et al., 2022). As such, professionally advocating for their colleagues, centralizes nurses, and midwives in the transformation of service delivery, with aspirations that professionally orientated advocacy will increase patient outcomes, whilst simultaneously tackling staff wellbeing and burnout to improve retention.
Because of this shift toward advocacy for and with professionals, prior notions about advocacy feel out of touch with the contemporary demands of advocacy in the health care context. This article examines how the concept of advocacy is refocusing nurses and midwives to overtly influence the wellbeing of their profession, in tandem with enhancing care outcomes and improving services (Smythe et al., 2023). To achieve this, we start by considering how the concept of advocacy has transformed over time to its current application in relation to professional advocacy in the nursing and midwifery professions.
Origins of Advocacy
Advocacy can be represented in several ways, most frequently based on a social justice model, where advocacy is “the office, position, or function of an advocate” and the role of the advocate is “support, recommend, or speak in favor of (a person or thing).” In other words, advocacy is based on the intention of doing something on behalf of someone else/group. However, in the professional domain, a more complex picture emerges, where advocacy is also aligned with distinct roles, such as professional advocates supporting families and children, patient advocates, professional advocates to individuals who have a learning disability. Alongside, U.K. legal frameworks such as the Mental Health Act 2007 includes nonstatutory advocacy (for people who do not meet the eligibility criteria for statutory provision) and statutory advocacy, linked to the legal entitlement of Independent Mental Health Advocates, Independent Mental Capacity Advocates, and Social Care Advocates. Therefore, the multilayered nature of advocacy means that the scope, reach, and influence of advocacy is diverse and distinctly aligned to the underpinning disciplinary purpose of each professional group and context. In this way, advocacy means different things to different disciplines in different settings, so a one size fits all definition is not useful and new, more contextually nuanced definitions are required.
Patient-Orientated Advocacy
The demand for nurses and midwives to advocate for others was framed in nursing literature after 1973 (Annas & Healey, 1974), when the International Council of Nurses introduced the concept into its Professional Codes (Vaartio & Leino-Kilpi, 2005) as a means of “speaking out and speaking for patients” (Hanks, 2008, p. 468). Curtain's (1979, p. 2) seminal work on advocacy deliberately separated the concept from legal frameworks or patient rights groups to emphasize the shared humanity of nurse and patient. Seedhouse (2000) also acknowledged the conceptual haziness of advocacy by observing variations between his descriptor of “the normal sense of advocacy” and “the nurse theorist sense of advocacy.” In particular, the day-to-day understanding is recognized as supporting another person to be heard to have their needs met (Water et al., 2016). In contrast, a more complex view is held by “the nurse theorist perspective” as professional knowledge influences how patient need is understood, therefore influencing the nature of support given. Whereas Bandman and Bandman (2002, p. 23) asserted a more general view by connecting nurse advocacy with holistic care saying, “the nurse who understands the advocacy role promotes, protects and thereby advocates patient interests and rights in an effort to make them whole and well again.” However, these positions do not consider the concept from those on the receiving end of advocacy (Scott, 2017).
Over time, definitions of patient advocacy moved on to incorporate an ethical obligation to ensure that the needs of the patient and family, and medical decisions are made in line with their wishes (Dadzie et al., 2017), because patients may be deemed as vulnerable in the healthcare setting (Cole et al., 2014) and may need an advocate for information and to help make decisions about their health (Abbasinia et al., 2020; Choi, 2015; Davoodvand et al., 2016). Indeed, the United Kingdom’s nursing and midwifery regulatory and governing body, the NMC, promotes advocacy as an essential requirement in professional practice, with section 2 stating nurses and midwives must “act as an advocate for the vulnerable, challenging poor practice and discriminatory attitudes and behavior relating to their care” (section 3) and to “respect, support and document a person's right to accept or refuse care and treatment” (section 2). Nurses and midwives acting as advocates for patients also makes sense because, out of all the health care professions, they have a higher degree of contact with patients. However, Tomaschewski-Barlem et al., (2017) argue that healthcare providers such as nurses and midwives experience deep seated disciplinary hurdles in their enactment of advocacy surrounding power differentials instilled by hierarchical and overly bureaucratic structures, a limited sense of agency and time pressured interactions (Nsiah et al., 2020, 2023).
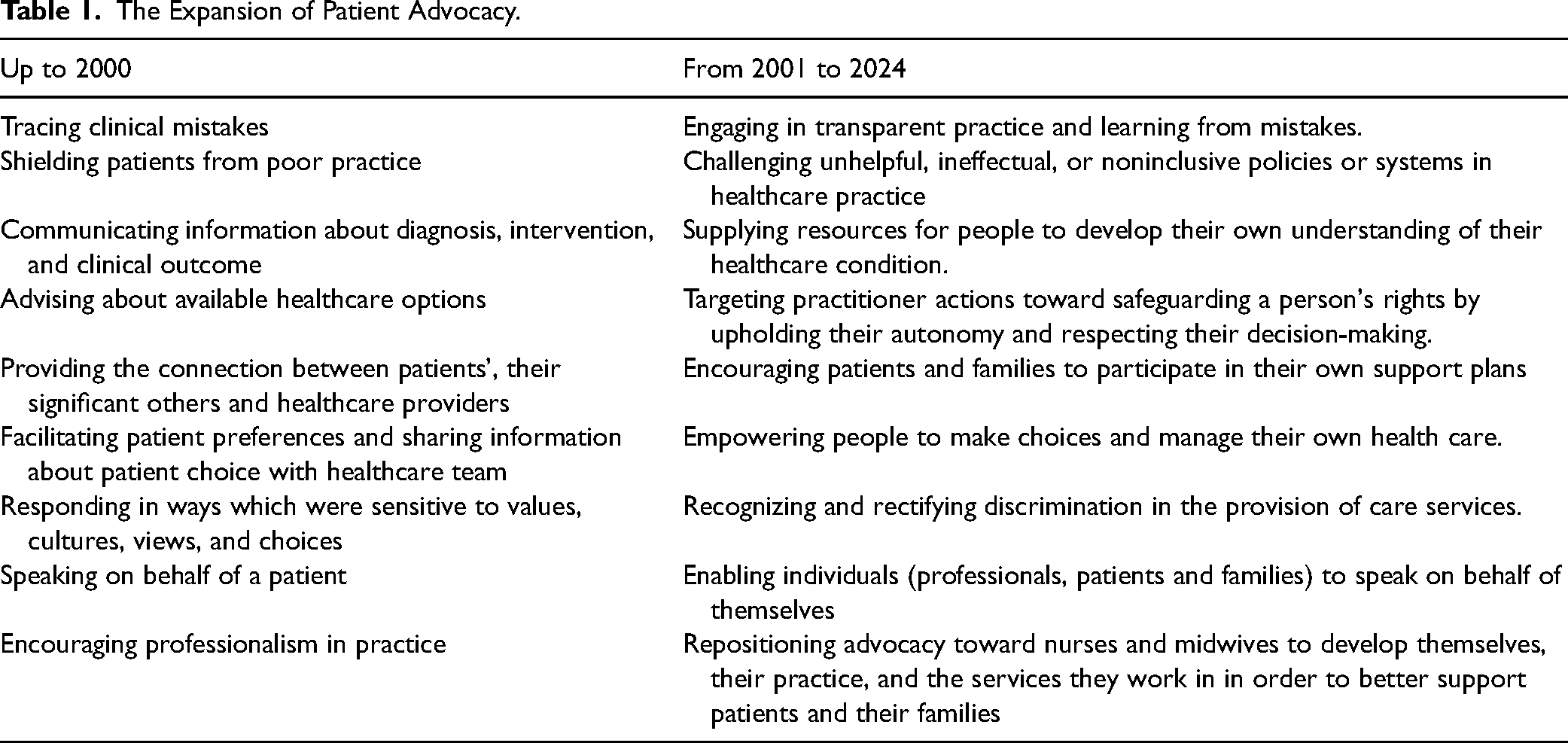
So, while advocacy is regarded as part of the everyday practice-based vocabulary of nurses and midwives, it is not a straightforward or static concept to describe. Consequently, subtle shifts have emerged in what constitutes advocacy, how it is understood and used, and to what extent nurses and midwives can and should advocate on behalf of patients. Abbasinia et al.'s (2020) concept analysis (Table 1) helpfully details that until the year 2000, patient advocacy was primarily directed at more individualized patient level and concerned with guarding patients against poor health care practice, offering patient-centered information about healthcare conditions, involvement in hospital discharge preparation, facilitating patient-led decision-making, sustaining person-orientated care, upholding the patients’ preferences and priorities by giving voice to the patient, and acting as intermediary for patients and their significant others. In contrast, the following years saw a change in focus toward the broader care setting through preserving patient privacy, challenging ineffective or restrictive policies/systems, and challenging disparities in the delivery of care. Whereas the expansion of priorities for advocacy from 2001 to 2024 demonstrates a distinct move from the initial person/patient focus of advocacy, toward advocacy for others within wider health and social care systems, and further reflects the transitory nature of the concept of advocacy
The Expansion of Patient Advocacy.
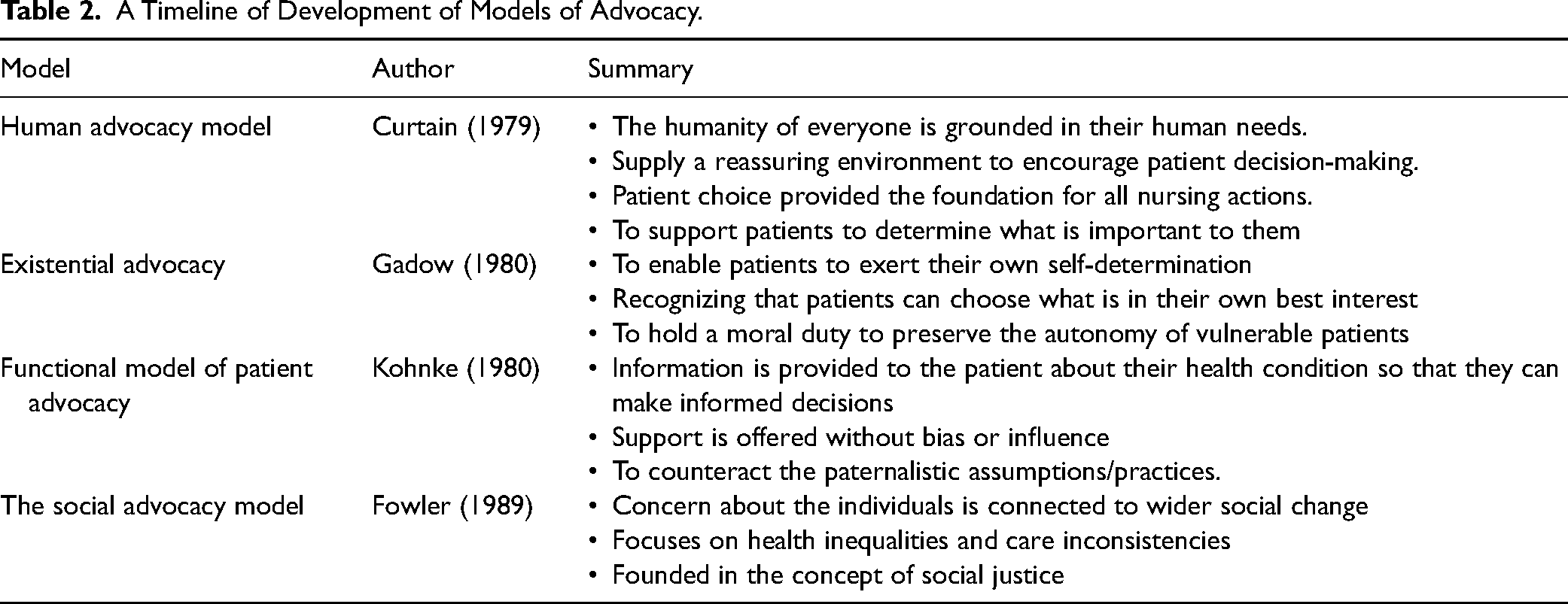
Therefore, conceptual understandings have gradually progressed in line with developing social trends filtering into practice-based assumptions. The intention and practice of advocacy redirects from “being the voice for patients” (doing advocacy for patients) to enabling patients to find and use their own voice (patients as their own advocates). The switch in focus connects with initial efforts to recognize and develop patient advocacy models, stemming from philosophical ideas to accentuate the core features of the practitioner–patient relationship, rather than the associated clinical tasks and behaviors (Reed et al., 2018). In the literature, examples of the foundational philosophical models of advocacy frequently referred to include the human advocacy model (Curtain, 1979), existential advocacy (Gadow, 1980), the functional model of patient advocacy (Kohnke, 1980), and the social advocacy model (Fowler, 1989). The key assertions for these models are summarized in Table 2.
A Timeline of Development of Models of Advocacy.
Since the inception of patient advocacy models, Kalaitzidis and Jewell (2015) observe the literature, evidence, and policy presents differing views and application. No single definition or model is agreed and as such, it is difficult to ascertain the significance and focus of health care advocacy, and therefore its limits. Indeed, Cole et al. (2014) stresses that to define the underlying concept of patient advocacy is tricky because it associated with assumptions stretching from the individualized patient–practitioner relationship through to the wider sociopolitical context of health and social care. Considering this, ideas about patient advocacy are transforming again and moving toward notions of empowerment (Cole et al., 2022). As a concept, empowerment is attuned to centralizing the patient in managing their own health and determining own health care. Therefore, empowerment provides another viewpoint to the previously accepted notions of advocacy. There are now calls in the literature to recast advocacy away from advocating on behalf of another as this perspective alignment is out of kilter with contemporary health care practice, drawing a line between what professionals might like to do, but what they can do, while reorientating the position of the patient as an active contributor in their own health.
The most recent progression is most evident in the current drive in the United Kingdom for PNAs and Professional Midwifery Advocates. Theses Professional Advocate roles has significantly nudged the discourse from a patient orientation to a position of advocating for peer professional staff to influence the health, well-being and retention of staff, which, in turn, is assumed will positively impact patient care (May, 2021). To date, there is limited discussion as to how this has occurred from a conceptual perspective, nor how this vision is to be implemented, and it is also clear what can be learnt or transferred from patient-centered conceptualizations. It is from this stance that we consider what professional advocacy might, or might not be, and what we need to understand to support its implementation in a fair and equitable way, which enables staff empowerment, and not creating additional burden on already professionally saturated expectations.
Professionally Orientated Advocacy
In the United Kingdom, there are approximately 50,000 nursing and midwifery vacancies (Palmer & Rolewicz, 2022). The NHS Staff Survey (NHS Staff Survey, 2020) proposes an upward trend is anticipated with responses reporting 49% as having experienced work-related stress that had impacted their health, and 40% experienced stress and burnout (Kinman et al., 2020; NHS Staff Survey, 2020). As such, there is a need to understand and support professional well-being in the work environment (Department of Health and Social Care [DHSC] (2022), alongside the need to retain nurses and midwives (Holmes, 2022) and develop services (NHS England & NHS Innovation, 2021). One means of doing so is via the introduction of Professional Midwifery and Nursing Advocacy (Dunkley-Bent, 2017; May, 2021). The concept was introduced as a means of skilling the nursing workforce to be equipped to deal with the increasing challenges within health care settings, to respond to their colleagues’ emotional concerns, enhance leadership skills and engage with quality improvement. The ambition for this employer-led strategy (Stephens, 2019; Sterry, 2019) was to create tangible support to improve the wellbeing of midwives and nurses through the growth of compassionate work cultures, focusing on delivering high-quality care, meaningful educational opportunities in an atmosphere promoting emotional security (Royal College of Nursing, 2020).
At its core, the PNA/PMA role was as a means of addressing the general low morale in the United Kingdom’s nursing and midwifery workforce and improving staff retention, both of which constitute significant challenges. With a 35% of approximately 46,000 vacancies (Shembavnekar et al., 2022), and increasing leaver rates for nurses increasing from 9% to 11.5%, it is unlikely the NHS Long Term Plan's stated (prepandemic) ambition to bring the nursing vacancy rate down to 5% by 2028 will occur, and if the NHS does not change its culture to significantly improve staff retention, NHS workforce shortfalls will continue to persist. It is also known that various factors influence why people leave the NHS workforce, including pay and reward, work–life balance, progression and continuing professional development, and health and well-being, evidenced via almost 27,000 professionals leaving the NMCs register, with more than half leaving earlier than planned, citing burnout, workload and concerns over care quality (Royal College of Nursing, 2023). The 2023 NHS Staff Survey additionally details problems with workplace culture, with nearly one in five staff reporting bullying or harassment from colleagues. The origins and ambitions of the Professional Advocate role is therefore informed by and embedded within complex and politically charged contexts.
One means of doing so was via the roll out of the PNA, as a new initiative, in 2021, developed from its predecessor, the Professional Midwifery Advocate, introduced in 2017. Since, PNAs and PMAs are trained to use the Advocating and Education for Quality Improvement (A-EQUIP) model (Ariss et al., 2017), within which, RCS is one of the four elements of the model (Capito et al., 2022; Wallbank, 2016). The use of RCS and the A-EQUIP model together significantly differs from previous versions of clinical supervision (Smythe et al., 2023) in that its aim is to build personal and professional resilience, enhance the quality of care and support preparedness for appraisal and professional revalidation.
An integral part of the Professional Advocate role, therefore, is the concept of clinical supervision. Clinical supervision in the field of nursing began over 40 years and is identified as improving care (Driscoll et al., 2019), leads to better health outcomes (Snowdon et al., 2017) and can help manage work-related stress (O'Connor et al., 2018). However, no agreed or consistent approaches were adopted (Driscoll et al., 2019; Rouse, 2019; Pollock et al., 2017; Sawbridge & Hewison, 2013), and despite many prominent reviews and reports detailing the need to ensure professionals are supported and enabled to voice their concerns (Frances, 2013; Gosport Independent Panel, 2018; Keogh, 2013, Ockenden, 2023), how to do so via clinical supervision has never been clarified. Snowdon et al. (2017) forward that a major deficit for previous versions was a focus on structural objectives rather than attending to the individualized nurse/midwives needs. The A-EQUIP model aims to reestablish the practitioner as central to the delivery of effective, efficient, and safe care, making their views, concerns, and well-being integral to the provision of high-quality care (Mahachi, 2020; Scanlan & Hart, 2024), with Pearce (2023) identifying six key areas for the role of a professional advocate as a position in the workforce
Advocating for patients. Creating collaborative care plans. Supporting change in clinical areas. Demonstrating inspirational leadership. Discussing professional issues, ranging from stress to career progression. Enabling reflection after a traumatic or stressful event.
However, the advocacy aspect of the professional advocate role requires careful definition. At present, the literature, evidence, policy, and guidelines focus on what PNAs/PMAs do rather than the attributes connected to what professional advocacy means. Observing the challenges with definition, Jennison and Walker (2022) observe that more explanation is needed to secure the role, and not lead into what they describe as “servant leadership,” rather than to transform the leadership to embody compassion, contextualized understanding and a genuine desire to help others (Pattison & Corser, 2022). This presents us with a cautionary note: to learn how professional advocacy could be effective, it will be useful to learn what works, and does not work, in other forms of advocacy.
Tensions in Nursing Advocacy
Firstly, the nurse as an advocate for patients is prone to distortion by the institutional and hierarchical constraints in which nurses operates (Bernal, 1992), which, in turn, threatens both the autonomy and rights of the patient. Secondly, traditional notions of biomedicalization place health professionals, including nurses, as the holders of expertise. This places the patient as in need of this expertise and that nurses are best placed for this work and assumes inherent vulnerabilities of the patient. This assumes that nurses, always “know best” with patients expected to remain compliant in the face of their expertise. Indeed, to act otherwise than is advised, can raise questions regarding patient capacity and for such patients to be considered “difficult” (Cole, 2022). Advocacy, in other words, can also be paternalistic and can compromise patient autonomy, capacity and competency. Thirdly, because of the institutionalized nature of health care, advocacy can be viewed as simply as assisting a patient through a clinical event (Schwartz, 2002; Sellin, 1995) with the role of the nurse as an advocate limited in effect to the act of providing information to the patient. Fourthly, there are claims that nurses stress their potential advocacy work purely as a professionalization strategy for occupational advancement (Mahlin, 2010). Fifthly, advocacy itself is, at best, a reactive, stop gap mechanism to solve singular problems, rather than preventing problems from happening. As a result of these complications, Cole et al. (2022) argues that the theory and practice of advocacy in nursing is mismatched and lacks cohesion. Yet, this does not mean we cannot learn from these problems and further understanding is needed as to the implications of what these problems might mean for the current PNA/PMA role. By recognizing what works may usefully inform, guide and secure the underpinning assumptions of professional advocacy in the contemporary practice context.
Patient and Professional Advocacy Alignment
To develop deeper understandings of the conceptual underpinnings of professional advocacy, lessons may be learnt from how patient advocacy has been previously described and transformed. Inherent to the terminologies associated with definitions of patient advocacy and professional advocacy are that of empowerment and of action. In this way, advocacy points toward being empowered to engage in actions that achieve a defined purpose, whether for the individual or another person (or persons). However, the very nature of professional advocacy involving work-based issues is inherently entangled with the wider system of care, professional advocacy impacts on individual healthcare worker well-being, service developments, and improved patient outcomes. So, unlike previous notions reflecting the dyad of nurse and patient, professional advocacy has a wider reach and while initially directed to the individual, extends to enhancing services and organizations through the shared aim of advancing patient care. Although the exact interpretation of what healthcare professionals perceive as advocacy remains unclear, key assets for individual and service level transformation can be applied. The process of supporting the individual practitioner while supporting continuous quality improvement in practice creates a symbiotic relationship between the professional and the healthcare system, they are part of. The blend of well-being and educational strategies are used as a conduit to advance care delivery by the individual practitioner to influence their impact for the services they are connected to. When combined, the ripple effect of professional advocacy has the potential to transcend individual issues to improve the workplace environment and patient-oriented outcomes. Thus, the overall result is seen in the improved working lives for healthcare professionals which enhances patient health outcomes and provides a better overall experience for everyone involved.
However, for professional advocacy to be effective, it is dependent on numerous integrated and complex factors including perspectives of leadership, social relationships, professional responsibilities, understandings moral distress and its side effects, workforce issues and conceptualizations of supervision, professional well-being, the role of education, governance, and the potential for service/role blurring. This list is not exhaustive as given the brief history of professional advocacy; other aspects may not yet be detected. As the evidence base develops, further definition and explanation of professional advocacy may come into view. At present, the limited interpretations of what professional advocacy means rather than what professional advocates do allows for new conversations. To assist in this developing dialog, Table 3 identifies the similarities and differences between advocacy focusing on patients and advocacy focusing on professionals.
Similarities and Differences Between Patient Advocacy and Professional Advocacy.
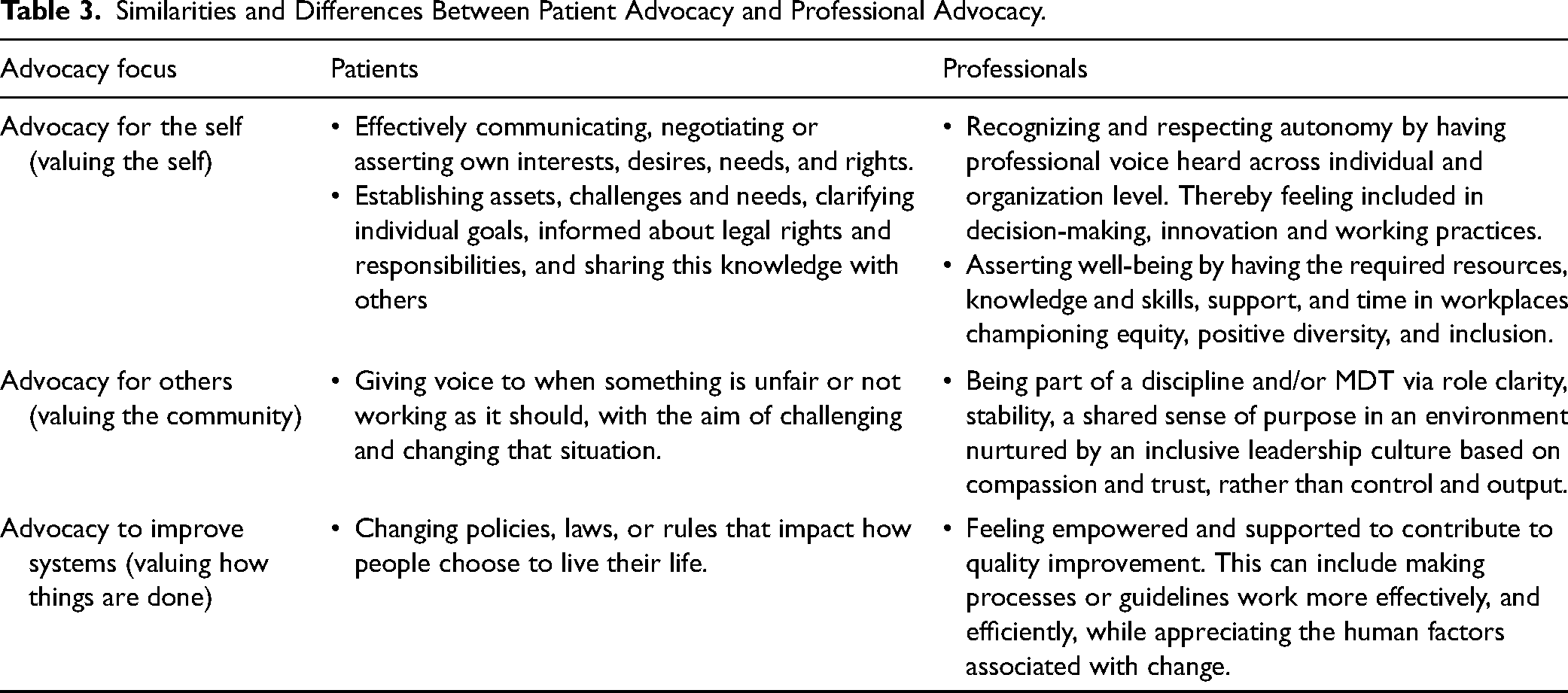
Table 3 describes how advocacy is linked to values-oriented thinking and practice for the self, others, and the wider system. So, while the professional advocate profile requires a more detailed description, the core underpinning features need to move beyond a task-centered definition to a shared acceptance of what advocacy means in the context of this role in the practice environment. In this way, professional advocacy combines individual advocacy with the fundamental principles of the discipline the individual is aligned with. Therefore, if professional advocacy is to be recognized and considered as an essential activity, further work is needed to also clarify the opportunities and the limits of advocacy.
As models of patient advocacy have evolved, professional advocacy is expected to follow a similar trajectory. However, professional advocacy remains a relatively new concept, still finding its footing in practice. Unlike patient advocacy, which was founded on philosophical principles, professional advocacy has emerged from a tangible and urgent need to protect staff well-being and develop services. While implementation structures have been established to bring professional advocacy into practice, the specific conceptual models are still a work in progress. The rollout of professional advocacy is currently focused on operational frameworks for applying the role, with professional disciplines yet to agree on the most suitable theories and concepts to support professional advocate activities.
As the conceptual models for professional advocacy continue to evolve, ongoing policy support will be crucial in realizing the full potential of these roles. Ensuring that professional advocacy becomes a central aspect of the policy agenda will not only enhance healthcare delivery and outcomes but also foster a culture of continuous improvement and innovation within the NHS. Currently, professional advocacy aligns with key NHS policies such as the NHS People Plan (2020/21) and the NHS Long-Term Plan (2019). The focus on staff well-being, the promotion of professional development through mentorship and knowledge sharing, and the fostering of interdisciplinary collaboration to improve patient outcomes are also in step with The Health and Care Act 2022 and AHPs Deliver Strategy (2022–2027) (NHS England, 2022). As such, the professional advocate role provides a tangible mechanism to translate policy into action. However, work is now needed to move professional advocacy from alignment to a more central aspect of the policy agenda. Without centralizing within the policy domain, there is a danger that professional advocacy does not receive the type and level of recognition needed to fully establish into routine practice, and opportunities missed to contribute to a more resilient and effective healthcare system. Ultimately, a well-supported and motivated healthcare workforce is essential for driving better service delivery, operational efficiency, and patient care outcomes across the United Kingdom.
Conclusion
The traditional conception of advocacy in clinical settings focuses on the care recipient; however, professional advocacy shifts the focus to the caregiver. There is, however, scant literature on this subject, demonstrating that the provision for healthcare professionals advocating for their peers is a recent and underresearched area of practice. An example can be found in the fields of nursing and midwifery. In a dynamic and increasingly demanding healthcare environment, a broader understanding of advocacy is necessary. Definitions need to extend beyond the patient–professional divide to consider how to enact systemic changes that support both care recipients and caregivers, enabling their voices to be heard.
For the purposes of this article, we propose a working definition for professional advocacy in the context of PNA/PMA as: “empowering value-oriented practice, encouraging positive well-being, and promoting engagement with service transformation.”
The role of PNA/PMA exposes the negative demands of practice and offers a structured, peer-to-peer solution to foster a constructive workplace ethos. Braithwaite et al. (2017) identified that improving the healthcare environment directly correlates with better patient outcomes and satisfaction. Such transformation is necessary, as the detrimental physical and psychological effects on nurses and midwives are well documented (Kinman et al., 2020; Maben et al., 2022; NHS Confederation, 2023). Distressing emotions, including anxiety, anger, irritation, hopelessness, and disconnection from peers, are linked not only with healthcare failings but also occur even when practitioners perceive they have performed their roles well (Hanks, 2008; Tomaschewski-Barlem et al., 2015). Consequently, it is now essential to develop a situated understanding of how practitioners experience their practice, despite the complexity involved.
Maintaining practitioner well-being requires a cultural shift, as failing to do so compromises the quality of care provided and increases the risk of moral injury. To counteract the harmful aspects of working in health care, West et al. (2020) found that three key elements must be integrated into routine practice. Firstly, autonomy, which refers to the extent to which a practitioner can act in alignment with their professional values and maintain a sense of control. Secondly, belonging, which relates to the experience of being appreciated and supported. Finally, contribution recognition, whereby practitioners and others can observe the impact of their work.
Professional advocacy provides practical steps toward a more effective, healthy, and sustainable workforce. Addressing the need for restorative supervisory support, professional advocacy prioritizes learning and professional development, rather than fault-finding and directive control. As such, professional advocacy must be recognized to empower and enable the workforce. However, professional advocacy alone cannot address the profound challenges faced by health care staff. In this deeply challenging context of contemporary healthcare practice, Cleary et al. (2019) suggest that ownership is required for effective change management to occur. Thus, professional advocacy must take place in an environment where those accessing advocacy are given opportunities to discover and implement their own self-directed strategies to enhance both their personal development and the services they contribute to.
Footnotes
Author Contributions
S.G., H.E., and M.A. conceived the project. S.G. and H.E. developed the theoretical arguments. N.V. and A.T. aided in the further theory development. S.G. and H.E. supervised the project. N.V., A.T., N.A., and M.A. contributed to the project. All authors contributed to the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Considerations
Ethical approval was not required for the work contained in this article because no human participants or data on human participants were used.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the East Suffolk and North Essex NHS Foundation Trust.