
Abstract
Background: Planning and executing healthcare for the patient or resident living with obesity can be a challenging task that has implications to the occupational health professional. Methods: Leading global experts in the areas of occupational health, ergonomics, bariatrics, technology, and patient care were identified and invited to participate in a round table discussion. Questions posed to experts were based on literature that addressed patient handling and mobility, architectural design recommendations, clinical care of the person with obesity, and ergonomic guidelines. Findings: Experts agreed that special considerations must be in place to care for the person who is obese. These special considerations should address not only clinical care of the patient, but ways to protect workers from occupational injury associated with clinical care. Experts suggested that, in some situations, a bariatric training suit may be helpful in better understanding space and design challenges, as well as a better understanding of the physical limitations associated with a larger body habitus (although simulated). Further, experts agreed that insensitivities often stem from failure to have proper space, technology and design accommodations in place. Conclusions/Application to Practice: The occupational health professional is a key resource to teams charged with planning and executing healthcare for the patient or resident living with obesity. Interprofessional understanding and communication can lead to a more comprehensive approach to space, design and technology that not only addresses the patient, but the worker providing direct care.
Keywords
Introduction
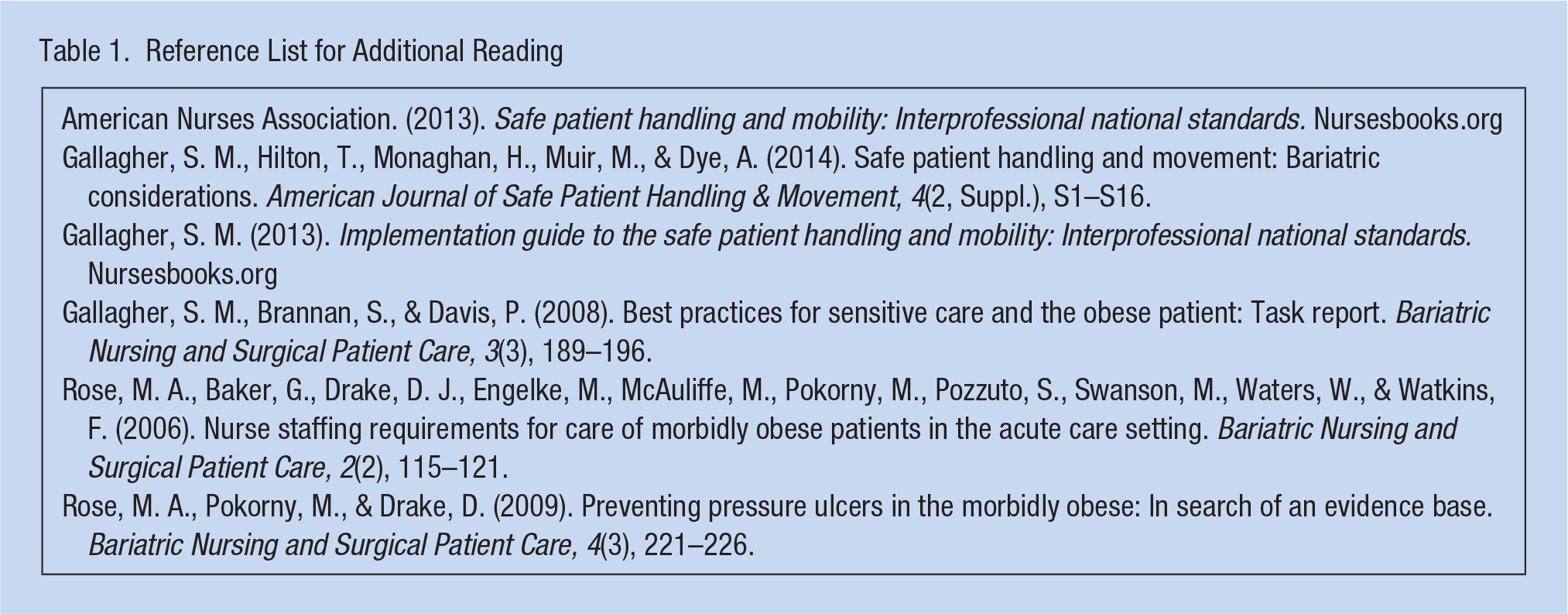
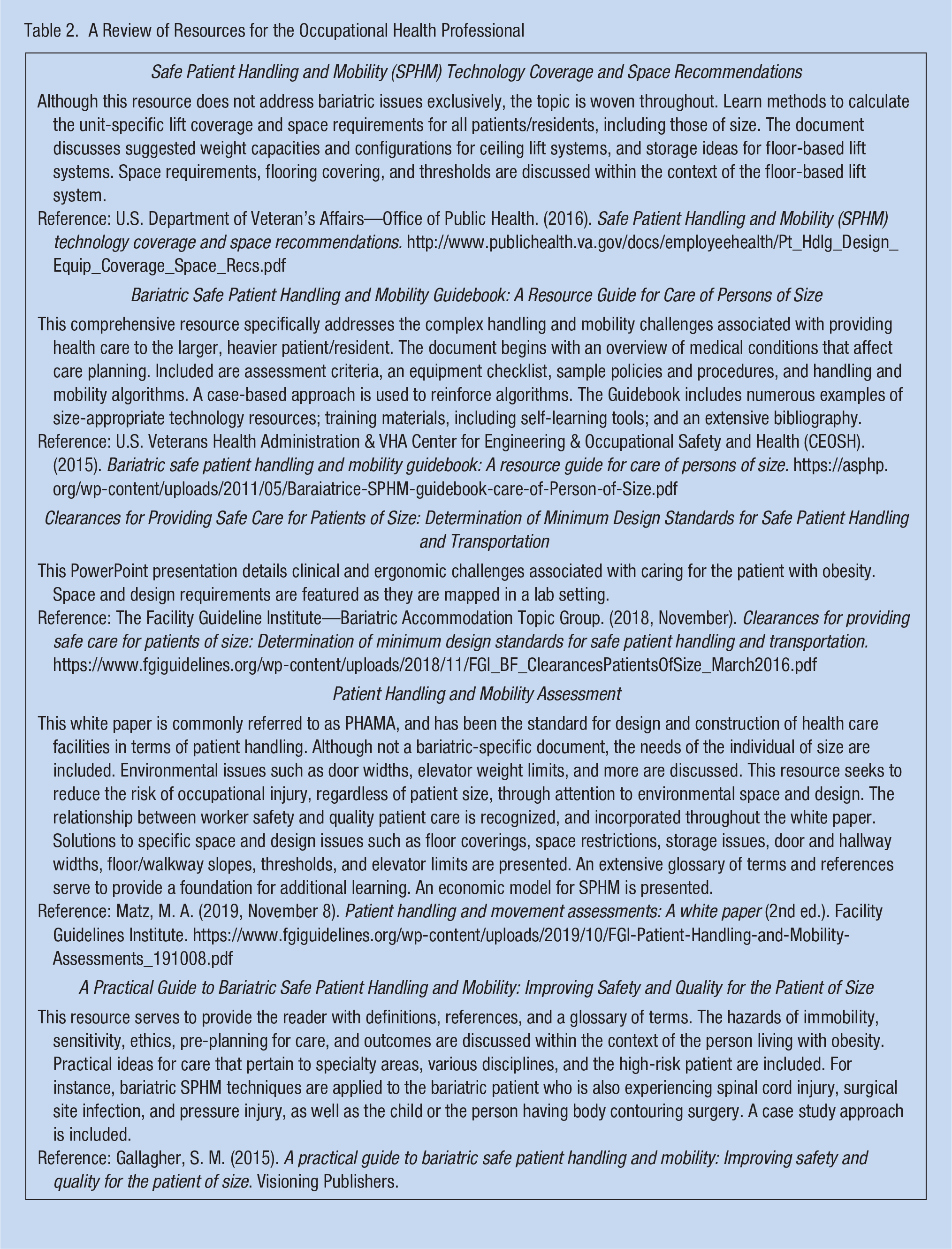
Space, technology, and design considerations associated with increasing numbers of patients with obesity have significant occupational health implications for health care workers and the entire healthcare system. Caring for individuals with obesity can be more complex irrespective of the setting or diagnosis. There are a number of challenges that must be addressed in terms of space, technology, and design as the care environment is often designed in ways that are considered exclusionary to the patient of size. The insensitivity to size requirements creates an environment that threatens occupational safety. For instance, super-sizing a standard piece of equipment or technology does not necessarily address the individual’s weight and/or weight distribution, posing safety issues. Bariatric equipment must combine load limit, appropriate dimensions, and a design aesthetic within a size-appropriate space that blends with the environment in which patient/resident and worker safety, dignity, and comfort are ensured. This Round Table, which includes input from content experts, explores a practical approach to space, technology, and design challenges and solutions that arise when caring for the patient of size. Literature that was either referred to or inferred is included as a reference list in Table 1. Resources that specifically address the topic are listed and summarized in Table 2.
Reference List for Additional Reading
A Review of Resources for the Occupational Health Professional
Experts who have been selected to participate in this Round Table bring a wide variety of education, training, and experience. Nurses, ergonomists, safety professionals, and occupational health professionals were invited to participate. Nursing professionals understand the unique patient and worker safety issues associated with bariatric care. Ergonomists are trained to match the environment to the worker, which is instrumental in understanding space, technology, and design. Risk management specifically addresses ways facilities can identify and manage organizational risk associated with the space, technology, and design issues raised herein. Recognizing the impact this topic poses to the occupational health professional is outlined and interprofessional ideas are presented and debated.
Space, technology, and design all impact delivery of care. In terms of space, if workers don’t have enough room to freely move safe patient handling and mobility (SPHM) equipment or apply slings for transferring to chairs, lifting limbs, or the abdominal panniculus, then it increases the risk of injury to staff members and the patient. This injury occurs because both the worker and patient are in a confined space or because the confined space prevents use of the safety equipment. This barrier limits the ability to mobilize the patient and discourages opportunities to deliver care that would otherwise be received if the patient was not a patient of size. In terms of technology, SPHM equipment is critical to reposition, transfer, lift, and mobilize patients of size safely; many beds do not allow room for adequate bed mobility. In terms of design, ceiling height is an overlooked design feature that significantly impacts care delivery. My opinion is that ceilings need to be a minimum of 9 feet, or shearing injury and staff injury can occur when repositioning, transferring, lifting, and mobilizing patients of size because the patient’s body is dragged across the surface.
Fall-related injury is a significant issue when caring for the person who is 300 to 550 pounds. I think size-appropriate seating is one way to prevent this type of injury. Falls can happen because the patient is not centered properly on the seating surface. A specialized chair with a removable back cushion or extra seat depth is essential for patients who have a large gluteal shelf or excess adiposity over the thoracic area.
In my opinion, sensitivity and preparedness are the most important considerations. As an Occupational Health Nurse Practitioner, I have learned that sensitivity training is key, and that a true culture of sensitivity cannot happen unless workers feel safe and comfortable with use of the appropriate equipment. I’ve observed workers who are afraid when faced with this level of complex care when they feel ill-prepared. A bariatric readiness plan is necessary, including the means to access vetted tools and resources, such as bariatric bedframes, surfaces, transfer devices, and more. An algorithm that specifies equipment that is both immediately available and where, as well as rental options for more obscure equipment is important preparation.
I agree with Cynthia McNaughton. Having basic equipment on standby is a sound aspect of pre-planning. For instance, a range of bariatric beds is important to timely, seamless care. A range is necessary because some bariatric patients are mobile so only require a basic bed that accommodates their weight, width, and weight distribution. Others, on the other hand, are complex and require a frame and support surface that address their specific need such as an egress alarm, turning surface, percussion, scale, or more.
In the above described patient or resident, it is important to match the patient’s weight, body distribution, and body movement with technology. Specialized technology must be available and accessible in a timely manner. I explain to colleagues that physically dependent patients should never be manually transferred. Health care workers often do not realize the risks associated with push and pull load. Further, surroundings and space are often a challenge. This is especially true in the home care setting, where the home is transformed into a place of work. Assessment provides a basis from which to begin the process to ensure safe patient handling in the home setting. Furniture may need to be moved and floor coverings removed before the work environment is acceptable.
I believe preventive skin care is important, especially among this high-risk population. Moisture from perspiration, urine, or other wound drainage can become trapped between skin folds and lead to intertriginous dermatitis or incontinence associated dermatitis. Immobility can lead to pressure injuries. These harmful and preventable skin injuries can be both painful for the patient and costly for the organization by way of penalties, claims, or non-reimbursed care. Performing a comprehensive skin inspection is challenging in the presence of skin folds, but especially under a large abdominal panniculus. Using existing equipment such as a ceiling hoist/lift accompanied by a limb sling or pannus lifter can assist staff members to gain access to areas between heavy skin folds. Further, more easily applied dressing technology such as the silver-impregnated fabrics provide moisture wicking and therefore reduce maceration.
I agree with Tracy; meticulous skin care is essential to bariatric patient care and safety, and can be very challenging. Health care workers have suffered injuries as a result of performing these tasks. We have recently purchased a bariatric simulation suit for staff to experience and practice first-hand when training on equipment for all sorts of tasks, including skin care. A secondary benefit of the simulation suit is a better understanding of facility space and design challenges. It has also been an important and very impactful addition to sensitivity training.
From a risk perspective, the most important consideration when caring for the individual weighing 300 to 550 pounds is a safe working environment. Excellent clinical care can only be delivered in an environment that fits the task. I agree with Cynthia that a simulation suit may be helpful for training use of equipment and sensitivity, but I think that a simulation suit can also be used to help planners better understand the actual space and design needs of the person who is larger. My opinion is that design of the space, arrangement of the furniture, and proper equipment that is readily available and has been tested are key to provide caregivers a safe workplace.
For the LTC (long-term care) resident, we need to focus on promoting and maintaining independence. This includes activities of daily living (ADL) as well as mobilization. Consider the study by Mary Ann Rose at East Carolina University. She suggests that bathing, ambulating, and assisting the bariatric patient to sit on the side of the bed were the most difficult and time-consuming patient care tasks. If we focus on using size-appropriate technology when performing these care tasks, we can expect a better clinical outcome for our resident while keeping the care team safe.
Education and training are key. Risk becomes a problem when staff members do not have sufficient knowledge and/or experience to develop and execute a plan for a bariatric resident in long-term care. Staff members are often not familiar with proper use of the technology and equipment and as Ronda Fritz mentioned earlier, there may not be enough space to use proper techniques or use the features of the technology. Understanding the best way to communicate these challenges within the organization is important. Education and training should include critical thinking and communication for outcomes.
In my mind, the needs of the post-acute patient are the same as those in the acute care setting. Three patient handling tasks that we have found pose the greatest risk to workers are (a) in-bed repositioning because it is performed the most frequently; (b) preventing an unanticipated fall, which we are seeing more often than in the past; and (c) access to the skin, either on the backside, under an abdominal pannus, breasts and between skin folds, and in the perineum. Inserting an indwelling urinary catheter in this population can be a struggle. Each of these tasks pose risks to the worker. I agree with Malene Alexandrowitz, the risk of worker injury is a problem when staff members do not have sufficient knowledge and experience to safely perform patient handling.
Asking for extra space in the ICU is often not negotiable. To that end, successful bariatric progressive or early mobility requires ceiling tracks, preferably a traverse system. The advantage of this system is that less space is required and fewer staff members are needed when providing tasks such as lifts, turns, and transfers. Selecting the right ICU bed is also important. I prefer a bed frame that turns, sits, and stands. Each of these features protects workers, assists in early rehabilitation, and reduces the need for extra bariatric furniture.
I believe all patients, regardless of size, have special needs when providing early/progressive mobility in the ICU. The patient of size requires additional space due to the size of the bed in the room, location of the ventilator, length of tubing, number of IV poles, and the number of people involved in ambulating a vented patient. Support people who may assist in early ambulation could include the respiratory care provider, physical therapist, nursing professionals, and the physician. I agree with Ronda Fritz, a ceiling lift, instead of a mobile floor-based lift, provides the most appropriate means of getting the patient of size up from and out of bed. Using a ceiling lift allows more space in the room and this allows space for members of the care team to be present during the mobility activity.
Early mobilization is a very important aspect of care for patients in the ICU. Even small steps make a big difference on clinical outcomes. We need size-appropriate technology and equipment for a number of tasks. Equipment and technology provide a way for staff members to better perform in bed repositioning, lateral transfers, hygiene, and skin care activities.
In terms of space, too often hospital designers lack healthcare input. Architects are thought to design around esthetics whereas nurses and other providers want the environment to serve their practical and functional needs. In terms of technology, bariatric equipment has often failed the larger patient because it is simply larger, rather than addressing the unique qualities of weight distribution. The challenge we have as health care workers is meeting the needs of a wide range of patient sizes, ages, mobility status, and other complexities.
To better understand environmental needs, it is advisable to mark out the area using tape on the floor. Then place a bariatric bed, seating chair, commode chair, bedside locker, and walker. Once the furniture and equipment are within the outlined space, simulate care using a person wearing a bariatric body suit. This will demonstrate space limitations. Further consider simulating resuscitation efforts within the confines of the space and identify worker safety challenges. These activities help planners understand the space requirements. This type of forward planning assists in securing funding required to make improvements to ensure space is adequate. Further, this prepares worker safety advocates who may be asked to share with architects and designers when renovation or building is planned.
I was fortunate to work with a large health system that supported the effort to include SPHM in the design and plans for any new construction or renovation project. This significant investment in ceiling lifts (100% in ICU rooms) and space requirements for bariatric patients were included in the template for ICU rooms and were based on the PHAMA (Patient Handling and Mobility Assessment) guidelines. We developed detailed guidelines to ensure adequate technology and space was established well before construction projects actually began.
We have learned to order ceiling lifts with “raised carriages” so the lift motor(s) hang within the primary rails on the traversing rail instead of below them. This design allows a 6 to 8-inch increase in lift. The lift may still create some drag when repositioning, lifting, transferring, or mobilizing certain patients of size, but it can reduce the amount of exposure.
Tracy Nowicki makes a great point in suggesting the room design team needs to understand the clinical needs and activities that must occur in that space. Architects and designers follow the old adage, “form follows function” but often times, the design team is not aware of the awkward bending and moving that takes place when the care team is performing clinical care tasks, working around the bed, or when attempting to get the patient out of bed. The Facilities Guidelines Institute (FGI) team, along with several bariatric experts participated in a room builder exercise in 2015. We used a simulation room that included the patient room and bathroom, with moveable walls in order to explore just how much space is actually needed to use lift equipment. The team determined they could actually decrease the room size by 20 square feet if ceiling lifts were installed instead of using the mobile (floor lift) to lift, manage, and move the patient of size. This saving in dollars is attributed to the fact that the care team did not need the turning radius of the mobile lifts if the ceiling lift is in the room. The findings are published in the 2019 FGI PHAMA publication.
I believe we have to be persistent and continually raise the issue to get the necessary space, technology, or design. I agree with Tracy Nowicki in that we must be prepared to interact with our colleagues and become spokespersons for obese individuals and health care workers who provide care. Eventually, we achieve victories and lessen the risk for staff members and patients. Keep in mind that some things just can’t be compromised.
I agree with you, Ronda. We simply can’t knowingly put workers in harm’s way. I think that in occupational health nursing, our role is to remind planning teams of the ethical obligation we have to protect workers as well as patients. This conversation reminds me of a situation where a new hospital was nearing their opening only to discover that the stylish wall-mounted toilets would accommodate no more than 350 pounds. That hospital adapted an unsightly retrofitting to make the wall-mounted toilet safe for individuals of size. If a patient were to fall or be injured in the bathroom because of a broken toilet, workers risk getting injured in the moment of crisis. We can’t let that happen.
I have had the experience of collaborating with design and construction team members to ensure that architects and SPHM teams worked to promote a functional patient care environment. We wrote standards to guide the design team in selecting appropriate configuration, weight capacity, and placement. In addition, for those facilities still developing their infrastructure, we implemented “bariatric equipment bundles” based on the bedside mobility assessment score. Rental equipment was ordered specifically for the patient based on clinical needs (BMI [body mass index], weight distribution, mobility level, fall risk, skin consideration, etc.). Standardizing the process with a checklist to identify the items needed provided a way for bed placement to ensure the right room assignment and equipment would be available.
Recognizing variation in body weight distribution, and integrating this into equipment selection, is a relatively recent and important innovation in both the acute and home care settings.
Preplanning is key. Comprehensive bariatric preparedness that addresses space, technology, and design is the one innovation that, when done right, can protect our employees.
Once staff members understand the emotional and physical challenges associated with larger patients, they can care for the patient of size with dignity and respect. When this understanding occurs, other care falls into place.
Several years ago, we purchased a bariatric training suit (BTS). After multiple attempts to get a bathroom for patients of size in our facility, I used the suit to communicate the need. The previous attempts to get the necessary support from our leadership had raised awareness enough to get our Executive Leadership and Service Chiefs to agree to a facility tour with me to identify challenges for patients of size. An engineer wore the BTS and played the role perfectly. We started in the Executive Offices and had them push the patient in a bariatric wheel chair to the elevator. First obstacle, they couldn’t get the chair through the office door. Next obstacle, they couldn’t see the feet of the patient to judge collision points. The elevator was another enlightening ride for them. The group couldn’t fit in the elevator with the patient and they were very aware of the cramped space. Next, the patient tried to enter every bathroom and stall on our tour. It didn’t take long for senior leaders, engineers, and other non-clinical personnel to see the problem. The patient didn’t fit through the doorway, couldn’t fit on the toilet, no ability to use a lift or rescue the patient if needed or even wash their hands. I’m happy to report we now have a bariatric bathroom in our facility!
Like the others, we found awareness to be the first step. We sponsored a regional SPHM conference with hands-on sessions in a simulation lab. One lab breakout focused on the bariatric patient. With a bariatric model and expert instructors, we took participants through troubleshooting, the use of technology, and skills needed to overcome challenges and issues with providing SPHM to the person who has obesity. We found it opened eyes to see the actual space needed in an actual patient room.
Summary
Protecting workers while providing safe, dignified care for larger, heavier patients/residents is becoming more important today than ever before. In the past three decades, obesity has quadrupled in some segments of the international population. Experts herein have offered practical ideas for addressing space, technology, and design challenges associated with caring for the patient of size. Research and resources have been summarized and offer an evidence-based approach to the topic. Healthcare providers and stakeholders are in key positions to move the approach from simply ordering a “Big Boy” bed for the bariatric patient and hoping for the best. The time is right to consider a well-orchestrated strategy to address worker and patient safety, dignity, and satisfaction issues associated with care delivery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Susan Gallagher, PhD RN CSPHP, president of the association of Safe Patient Handling Professionals (2019-2020), holds a PhD in public policy ethics, and has written and trained extensively on the intersections of patient safety, worker health, bariatrics, and outcome opportunities across care settings. Author of the Implementation Guide to the American Nurses Association SPHM Interprofessioanl National Standards. Professional Practice Associate Editor for Workplace Health & Safety.
Malene Alexandrowiz, MA, OT, head of Cobi Academy based in Denmark. Currently serves as vice president at The Danish Obesity Board. Malene has worldwide experience and knowledge in developing equipment that accommodates individual needs based on body habitus. She provides resources and education in bariatric mobilization, rehabilitation and seating.
Ronda Fritz, MA BSN RN, formerly safe patient handling facility champion at the VA Nebraska-Western Iowa Health Care System in Omaha, where Ronda and her team reported on the economic, clinical and humanistic outcomes associated with a comprehensive SPHM program. She serves as contributor to the American Nurses Association SPHM Interprofessioanl National Standards.
Dee Kumpar MBA, BSN, RN, CSPHP, member of National Pressure Injury Advisory Panel Corporate Advisory Council, contributor to American Nurses Association SPHM Interprofessioanl National Standards, past Board Member of the Association of Safe Patient Handling Professionals. Contributed to the Facility Guideline Institute Bariatric Patient Handling and Mobility Assessment document. She is a published author and speaker on bariatrics, SPHM, fall prevention, and pressure injury prevention.
Merl Miller, CPE, worksite injury prevention consultant and co-author of the Banner Mobility Assessment Tool (BMAT), serves as OSHA education center instructor for SPHM and ergonomics. Founder of Performance Ergonomics, which helps organizations concerned with improving their safety performance and outcomes.
Cynthia McNaughton RN-C OHNP, occupational health nurse practitioner from the Employee Wellness and Health Services at El Camino Health in Mountain View, California. Involved in worker and patient safety as it pertains to the patient or worker living with obesity.
Tracy Nowicki, RN, clinical nurse consultant and equipment manager at The Prince Charles Hospital located in Brisbane, Queensland, Australia. Nursing director at QuEST in Queensland, Australia. As a patient advocate, she lectures and consults worldwide.