
Abstract
Background: The application of external abdominal pressure by endoscopy nurses has long been recognized to facilitate passage of the endoscope during colonoscopy. Applying sustained abdominal pressure during a colonoscopy for an obese patient is especially challenging and may result in musculoskeletal injury for the endoscopy nurse. Methods: Four experienced endoscopy nurses cared for 100 obese adult patients scheduled for colonoscopy who had a body mass index (BMI) greater than 25 kg/m2. Duration of applied pressure, as well as nurse pain and fatigue were examined after they cared for 50 patients with and 50 patients without a positioning wedge. Findings: No difference in the mean fatigue score between nurses providing standard care versus those using the positing wedge was observed (mean score: 2.6 vs. 2.0, respectively); however, self-reported pain was higher for those providing standard care relative to those using the positioning wedge (mean score: 2.9 vs. 1.3, p = .0143). In 18 patients who required both the wedge and pressure, these nurses still reported lower pain scores relative to nurses who provided care without a wedge (M = 1.3 vs. 2.9, respectively). Conclusion/Application to practice: A positioning wedge for obese patients undergoing a colonoscopy can reduce the need for external abdominal pressure applied by endoscopy nurses. Occupational health nurses should endorse the use of a gel wedge to promote safe patient handling and reduce the potential for musculoskeletal injury among endoscopy nurses.
Keywords
Background
A recent study of California nurses described a 67% prevalence of work-related musculoskeletal pain in the past 12 months (Kim & Lee, 2019). Safe patient handling and no-lifting campaigns have targeted the risk of lower back injuries using assistive devices (Vendittelli et al., 2016). Nurses practicing in endoscopy suites are at particularly high risk for shoulder, neck, and upper extremity injury due to the need to assist with patient positioning during colonoscopy (Biggers, 2018).
Nursing activities during colonoscopy include assisting the endoscopist during passage of the colonoscope. During a colonoscopy, the standard position for entering the: places the patient in a left-lateral position. Unsuccessful colon intubation is related to the tendency for loops to form in the flexible scope. As loops form and increase in size, the risk of bowel perforation and patient discomfort increases (Prechel et al., 2015). The application of external abdominal pressure has been advocated to facilitate passage by splinting the endoscope to prevent loop formation, pushing the colon over the scope (Prechel et al., 2006; Prechel & Huckle, 2009).
Historically, two different types of external abdominal pressure approaches have been prescribed during colonoscopy, nonspecific and specific, both requiring the application of strong external force by the nurse (Waye et al., 1991). Nonspecific pressure is proactive and compresses the abdomen to maintain the colonoscope in a straight configuration to avoid looping. Specific pressure is reactive and applied at a desired site to actively assist in advancing the colonoscope. The usefulness of external pressure to yield successful colonoscopies was first reported by Waye and others in 1991. In 201 patients, proactive nonspecific pressure was used nearly twice as frequently as reactive specific pressure. Nurses or endoscopy technicians are responsible for providing external abdominal pressure during a colonoscopy. Proactive and reactive external pressure require the endoscopy nurse to reach over the lateral lying patient from behind and lift or compress the abdomen.
A known risk factor for colorectal cancer is obesity (Ma et al., 2013). When placed in the left-lateral position, the extra abdominal adipose tissue of an obese patient, the panniculus, must be lifted from its position of gravity before external pressure can be applied. In some instances, lifting pressure may be needed throughout the procedure leading to sustained lifting postures and positions by endoscopy nurses.
Dedicated endoscopy nurses have reported a comparable or higher prevalence of upper extremity disorders than other subspecialties (Biggers, 2018). A study of Canadian endoscopy nurses found that one-third reported missing work because of upper extremity pain (Drysdale, 2011), while one in every five endoscopy nurses in the United States reported upper extremity symptoms accompanied by pain and fatigue (Drysdale, 2013). A study of Scottish endoscopy nurses reported the top four ranked musculoskeletal disorders were neck, back, shoulder/arm, and wrist/hand, respectively, with the duration of exposure of particular concern (Murty, 2010). Darby et al. (2013) found that nearly half of the endoscopy nurses surveyed (n = 192, 46%) reported neck problems and shoulder problems in the previous 12 months.
Strategies to reduce musculoskeletal injury in endoscopy nurses have included ergonomic education and the application of positioning devices. Techniques of applying nonspecific and specific abdominal pressure have been described in the literature (Prechel et al., 2015; Prechel & Huckle, 2009) and demonstrated during continuing education programs. The Society for Gastrointestinal Nurses and Associates annual conference offers courses on applying abdominal pressure. Educators suggest that nurses be mindful of “good body mechanics and positioning” when applying external abdominal pressure during a colonoscopy (Prechel & Huckle, 2009, p. 30).
More recently, positioning devices have been developed to apply nonspecific pressure to facilitate colonoscopies. Schulman et al. (2017) tested a hands-free, reusable, abdominal compression device for colonoscopy patients when using a prone position. Prone positioning, advocated for obese patients during colonoscopy, can result in shorter cecal intubation times with a decreased need for pressure application (DeSilva et al., 2011; Uddin et al., 2013). The wide U-shaped compression device, the N-Doe Pillow® (NM Beale Co., Inc., Harvard, MA, USA), is placed against the patient’s left lower quadrant, with the patient rolled prone-ward. Evaluation of the N-Doe on 50 consecutive patients found a significantly reduced mean cecal intubation time compared with matched controls that received externally applied pressure (Schulman et al., 2017). However, the effectiveness of the N-Doe Pillow® to reduce duration of applied pressure, pain, fatigue, or musculoskeletal injury of endoscopy nurses was not evaluated. In an earlier study, Hartman and Cronin (2016) found no significant difference in staff musculoskeletal symptomology using the N-Doe Pillow® at 6 to 8 months after use. However, the “one-size fits all” device may have different effects in patients with greater waist circumference and has only been tested with colonoscopy patients in the prone position.
The ColoWrap (ColoWrap, LLC, Durham, NC, USA), an external abdominal compression device, resembles an abdominal binder and provides sustained pressure across the sigmoid and transverse colon (Biggers, 2018). Placed preprocedure, additional pressure can be applied during the procedure. In a pilot study, 45 colonoscopy patients with the ColoWrap were compared with 131 control patients and the need for manual external pressure was significantly reduced (Crockett et al., 2013). However, in a follow-up randomized controlled study of 350 patients there was no difference in manual pressure between the ColoWrap and sham group (Crockett et al., 2016). The single-use ColoWrap must be purchased and stocked in a variety of patient sizes.
Positioning wedges have been used in the operating room during general surgery to maintain patient positioning and offer support to internal structures. Made of foam or gel, they can be cleaned, reused, and one size can be used for a variety of body habitus. However, their application in endoscopy has not been investigated. By placing a positioning wedge under the abdomen of an obese patient prior to a colonoscopy, the panniculus could be lifted thus avoiding the need for proactive nonspecific pressure applied by the endoscopy nurse. The need for specific procedural pressure may also be reduced with a positioning wedge. Decreasing pressure application duration may reduce nurse fatigue and pain while mitigating musculoskeletal injury. Therefore, the purpose of this study was to determine if the use of a positioning wedge during a left-lying colonoscopy in obese patients decreases duration of nurse applied pressure, nurse fatigue, and nurse pain.
Methods
A descriptive correlational study compared the standard positioning of obese patients during a colonoscopy to the use of a gel positioning wedge on the need for the nurse to apply pressure. We also measured nurse report of fatigue and pain related to the application of pressure when using and not using the gel positioning wedge.
Four experienced endoscopy nurses, comprising the staff of a small community hospital endoscopy suite, were approached in person and asked to participate in the study. We obtained measures from the four nurse participants when they cared for 100 patients, aged 18 years and older with a BMI greater than 25 kg/m2, and who were scheduled to undergo an elective colonoscopy. BMI was ranked as overweight (25–<30 kg/m2), moderately obese (30 to <35 kg/m2), severely obese (35 to <40 kg/m2), or extremely obese (>40 kg/m2). The study was approved as exempt by the Institutional Review Board and informed consent waived (Southern New Hampshire Medical Center).
Patients were screened for body weight and the type of elective procedure 1 day prior to the procedure. The first 50 patients meeting the inclusion criteria received standard care by one of the four nurses, including application of nonspecific or specific external abdominal pressure as requested by the endoscopist. The second 50 patients meeting the criteria, were also cared for by one of the four study nurses, in which the positioning wedge was used: the Adult Gel Chest Roll (16ʺ L × 4ʺ W × 4ʺ H polymer gel based; Action Products, Inc., Hagerstown, MA, USA). The wedge was placed by the nurse prior to the colonoscopy (Figure 1). If the positioned wedge was insufficient during endoscopy intubation, the nurse applied external abdominal pressure as requested.

Wedge positioned with patient in a left lying position.
At the end of each colonoscopy procedure, the endoscopy nurse recorded abdominal pressure application time in minutes. They also self-reported their degree of fatigue and pain on 0 to 10 scales, with 0 being none and 10 being as much as possible. Schwartz and colleagues (2002) observed that the single-item fatigue scale (0–10) was sensitive to moderate changes in fatigue and useful in the clinical setting. The numerical rating scale for pain (NRS-11) is one of the most widely used scales to assess self-reported pain intensity. Childs et al. (2005) studied patients with low back pain and concluded that a change of 2 on the NRS-11 was clinically meaningful.
Data Analysis
Data were entered into SPSS v 21 (SPSS Inc., Chicago, IL, USA) and descriptive statistics were calculated. Independent t-tests were conducted to determine the difference in the frequency and duration of applied pressure, fatigue, and pain. Pearson’s correlation determined the relationships among the variables.
Results
The four nurses in this study cared for a similar number of patients with and without the positioning wedge (Table 1). The patients’ BMI ranged from 25.8 to 67.0 kg/m2 with a mean of 32.9 kg/m2 (SD = 6.4). One-third of patients (32%) were severely or extremely obese.
Demographic characteristics of patients and nurses with and without a positioning wedge during a colonoscopy.
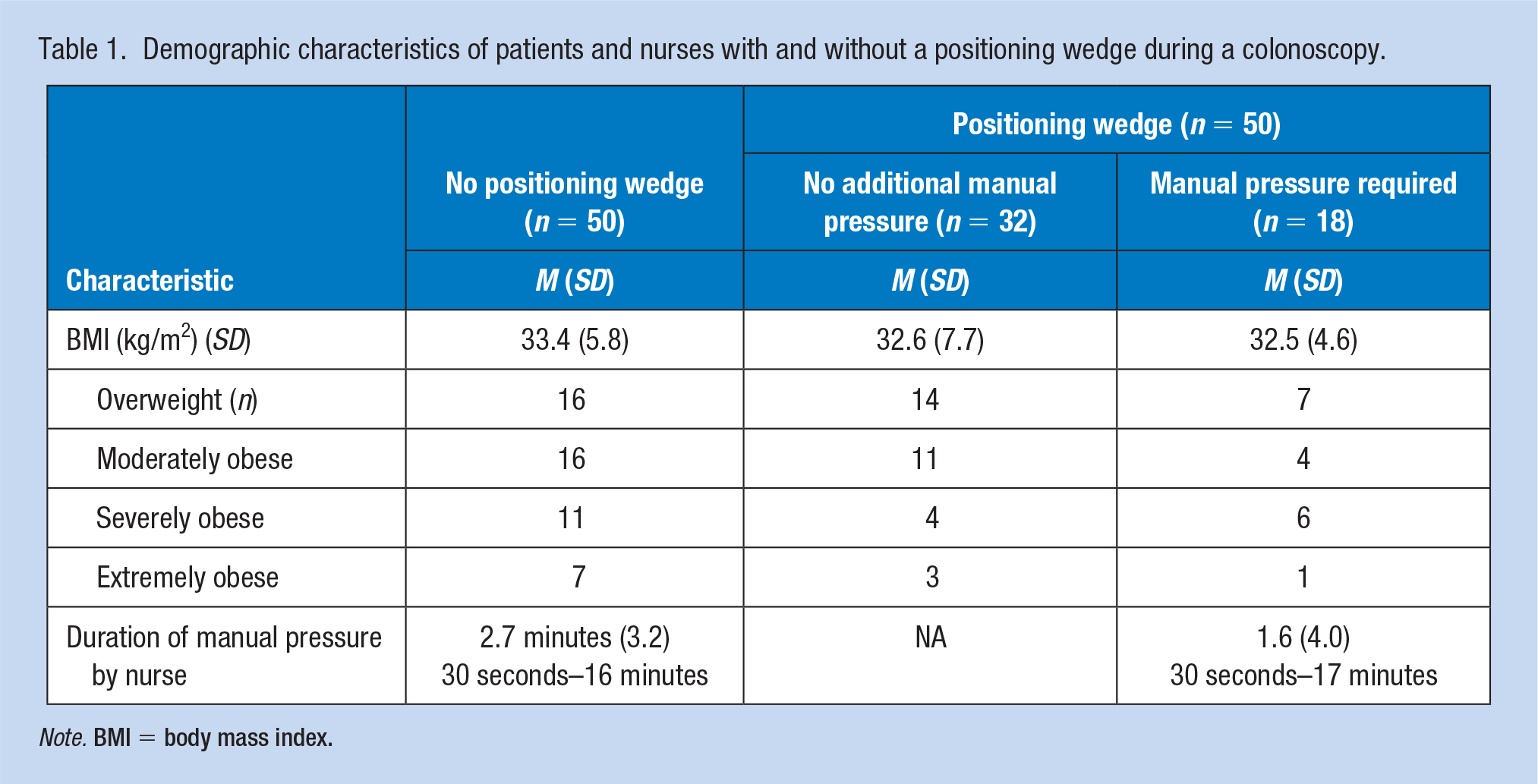
Note. BMI = body mass index.
A nurse was required to apply external abdominal pressure during the colonoscopy for all of the 50 patients in the standard care group for a mean duration of 2.7 minutes (SD = 3.2; range 30 seconds–16 minutes). Only 18 of the 50 (36%) patients in the positioning wedge group required additional applied external pressure by the nurse, with a mean duration of 1.6 minutes (SD = 4.0; range 30 seconds–17 minutes). There was no significant difference between groups on duration of nurse-applied external pressure.
Fatigue reported by nurses caring for the standard care group ranged from 0 to 8 on the 11-point scale (M = 2.6, SD = 2.1), compared with the positioning wedge group range of 0 to 9 (M = 2.0, SD = 2.2), with no significant difference between groups (Table 2). Self-reported pain when nurses provided standard care ranged from 1 to 9 (M = 2.9, SD = 2.2), compared with the positioning wedge group of 0 to 6 (M = 1.3, SD = 1.7). The difference was significant (t = 2.52, p = .0143).
Measure of nurse fatigue and pain among four nurses that did and did not apply a positioning wedge during 100 colonoscopy procedures.
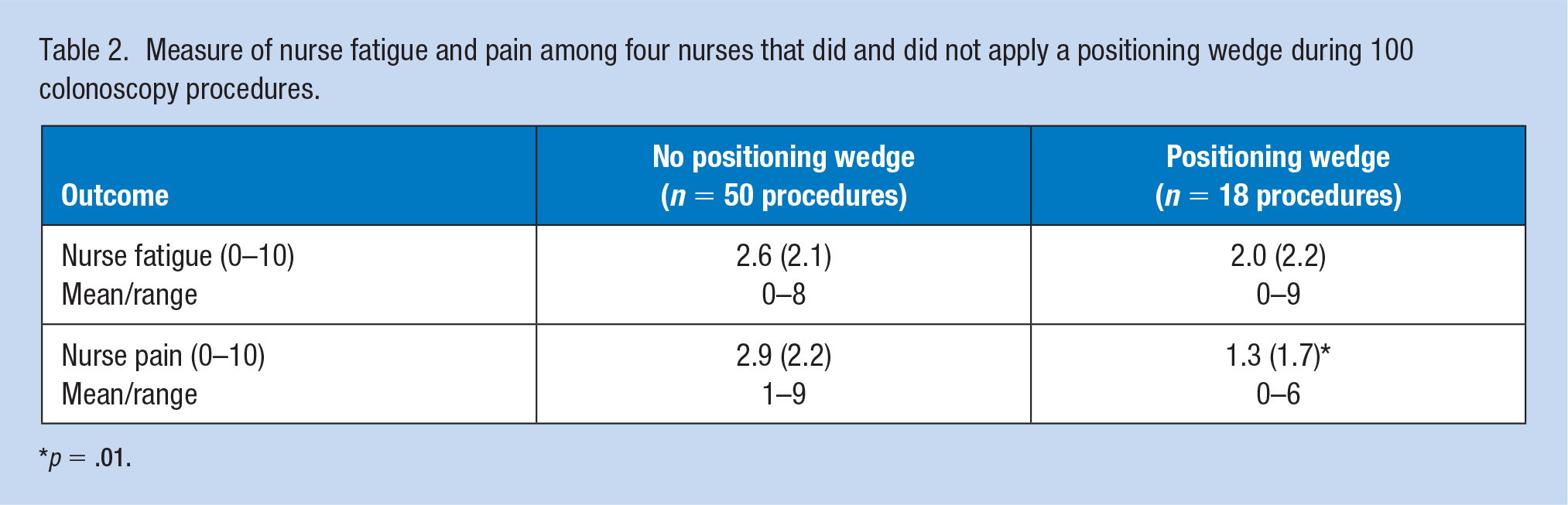
p = .01.
A positioning wedge for obese patients prior to colonoscopy reduced the need for nurses to apply any external abdominal pressure in 32 of 50 (64%) of the patients. In the 18 patients who required pressure, the nurse-reported pain scores with a wedge (M = 1.3, SD=1.7) were significantly different from nurse-reported pain scores, when care was provided for 50 patients, without a wedge (M = 2.9, SD = 2.2).
As expected, there was a strong significant positive correlation between nurse fatigue and pain with or without the use of a positioning wedge (rstandard care = .801, p = .0001; rpositioning wedge = .785, p = .0001; data not shown). There was no relationship between fatigue and duration of pressure in either group. Although there was no relationship between the duration of external pressure and pain in the standard care group, there was a significant relationship (r= 7.37, p = .001) between the duration of external pressure and pain in the positioning wedge group (data not shown).
Discussion
The patients in this study were similar to the general population of obese patients (Fryar et al., 2016). The presence of a positioning wedge eliminated nurse-applied nonspecific external pressure in two-thirds of the obese colonoscopy patients in this study while also significantly reducing the duration of specifically applied external pressure. Abdominal adiposity creates pressure over the entire abdomen (Prechel et al., 2006). It is likely that the positioning wedge was able to reduce the need for additional abdominal pressure to facilitate cecal intubation. The mean duration of pressure required in both groups (1.8 ± 3.2 minutes) was less than that reported by Drysdale (2013) (6.3 ± 4.3 minutes). The difference may be due to immediate recording in the current study versus delayed recording reported by Drysdale (2013).
The current study is the first known report of positioning fatigue among endoscopy nurses. The lack of a relationship between fatigue and the duration of applied external pressure may be due to the relatively short pressure duration and low level of fatigue experienced by nurses in this study.
In addition to reducing the need for nonspecific external abdominal pressure, the use of a positioning wedge significantly decreased nurse-reported pain when specific external pressure was required. When fatigue sets in, alternative upper extremity muscles act to realign and reposition the torso. The realignment may not be ergonomically appropriate and result in pain. Although there was a strong significant positive correlation between fatigue and pain, cause and effect was not determined in this study.
The difference between the standard care and the positioning wedge group related to pressure duration and nurse self-reported pain is noteworthy. In the standard care group, the nurse applied both nonspecific and specific external abdominal pressures. It is possible that the nonspecific pressure was a routine position based on nurse experience and did not require positional realignment, therefore not pain producing. Placement of the positioning wedge substituted for nonspecific external pressure. The request for additional pressure for one-third of the patients in the positioning wedge group reflected a need for specific pressure. Specific pressure can be applied in any location on a large obese abdomen but also creates fatigue leading to pain.
The study findings are limited to the subjective reports of four nurses in one endoscopy suite and cannot be generalized to all endoscopy nurses. A multisite study is required to increase the number of endoscopy nurses studied as most endoscopy suites have limited nurse staffing. Obese patients in the current study were purposefully selected and the requirement for nurse-applied pressure may be different for normal or underweight patients.
Implications for Occupational Health Nurse Practice
The use of a positioning wedge for left-lateral positioning of an obese patient prior to colonoscopy reduces the requirement for the application of nonspecific external abdominal pressure and nurses’ self-report of pain during additional pressure requirements. Occupational health nurses evaluating the endoscopy environment to prevent workplace injury should suggest the application of positioning wedge device when colonoscopies are performed on patients using a left-lateral position and strongly recommend positioning devices when caring for obese patients. Although positioning devices can decrease the requirements for nurse-applied external pressure during a colonoscopy, further study is needed to design systems to eliminate the need for nurse-applied pressure and promote safe-handling for the patient and the nurse.
Application to Professional Practice
Applying external abdominal pressure during a colonoscopy of an obese patient is challenging. Endoscopy nurses are at high risk for upper back, neck, and upper extremity musculoskeletal disorders. Two groups of 50 patients were managed by four experienced endoscopy nurses. Compared with no device, the use of a positioning wedge placed under the abdomen eliminated the requirement for endoscopy nurses to apply external pressure for two-thirds of the obese colonoscopy patients. In addition, when specific external pressure was required, the positioning wedge significantly decreased nurse-reported pain. To prevent or minimize workplace musculoskeletal disorders of endoscopy nurses, occupational health nurses should recommend the use of a positioning wedge.
Footnotes
Acknowledgements
The author acknowledges Bethany St. Onge BSN, RN; Kristina Crecco BSN, RN; and Dennie Wing AD, RN, in the conception and implementation of the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biography
Susan J. Fetzer is the nurse researcher at Southern New Hampshire Medical Center in Nashua, New Hampshire which has been Magnet designated for the past 13 years. She has extensive research interests in surgical nursing.