
Abstract
Background: Patient safety has been a concern over the past two decades. The value of nurses and their work environment in relation to patient safety has been acknowledged by studies and international organizations. This study aimed to examine the relationship between patient safety practices and the nursing work environment. Methods: In total, 570 registered nurses were invited from the inpatient units in public and private hospitals. Perceived patient safety was evaluated using the Overall Perceptions of Patient Safety subscale from the Hospital Survey of Patient Safety Culture (HSPSC). The nursing work environment was assessed using the Practice Environment Scale of the Nursing Work Index (PES-NWI). Findings: Of the 350 of 570 (64.6%) nurses surveyed, 35.2% (125) reported positive levels of perceived patient safety. Staffing and resource adequacy, professional communication style, and nurses’ participation in hospital quality improvement activities were associated with higher levels of perceived patient safety. Conclusion/Application to Practice: This study provided empirical results about perceived patient safety culture in relation to nursing work environment. It is paramount to focus on specific dimensions of the nursing work environment, such as staffing and resource adequacy, nurses’ participation and advancement, and communication style to improve the quality of care provided to patients. Hospitals are considered one of the most hazardous places compared with industries. Policy makers would help reduce injuries, save resources, and build a culture of safety when taking into consideration the importance of the nursing work environment in relation to patient safety.
Background
Over the last two decades, patient safety has been the center of attention in health care organizations globally. Patient safety is an essential element in delivering individualized quality care. Internationally, well-recognized reports such as from the United States “To Err Is Human” (Institute of Medicine [IOM], 2000), from the United Kingdom “An Organization With a Memory” (Donaldson et al., 2000), and the Garling Report in Australia (Garling, 2008) focused on the importance of improving patient safety within health care settings. Because the work environment is an important facet with respect to patient safety, the IOM issued a report in 2004 “Keeping Patients Safe: Transforming the Work Environment of Nurses” reporting an inverse relationship between patient safety and a negative nursing work environment (Page, 2004). This report identified common shortcomings regarding patient safety in areas such as administration practices and elements of organizational structure. It also emphasized that the degree to which nurses are involved with inpatient health decisions also influences patient outcomes. When nurses are given an opportunity to participate in managing a health setting, they are empowered to view patient safety as a priority. In addition, it addressed the importance of active nursing leadership, which engenders a constructive work environment and enhances a culture of safety. This report also ascertained that many hospitals have insufficient number of staff which in turn would reduce quality of health care and threaten patient safety (Page, 2004).
Inadequate nursing staff ratios have shown to result in decreased quality of nursing care and increased patient mortality rates (Mudallal et al., 2017). A systematic review revealed that self-governance, positive relationships between doctors and nurses, and nursing care and leadership focused on professional development and growth have been associated with better patient outcomes (Aiken et al., 2008). It is plausible that suboptimal nursing practice environments correlate with poor patient health outcomes, including hospital-associated infections and medication errors (Olds et al., 2017). A 2015 study of Jordanian nurses assessed the perceptions of patient safety and revealed that nurses believed certain aspects of the nursing environment need serious improvement, especially communication and staffing (Khater et al., 2015). To date, no studies have evaluated a possible relationship between perceived patient safety and the nursing practice environment among Jordanian nurses. The purpose of this study was to examine the relationship between perceived patient safety culture and nursing work environments in Jordan.
Methods
This study was conducted using a cross-sectional design. Participants were registered nurses and midwives employed in the inpatient hospital setting. A convenience sample of 570 registered nurses were invited to participate between January 2016 and June 2016 from inpatient units of different public and private hospitals in Jordan. To be included, the participant had to be a registered nurse or midwife, who delivered bedside care for a minimum of 3 months before the data collection started. We included only registered nurses because the study addressed a high level of nurses’ work domains in which only registered nurses are typically engaged. Nurses with less than 3 months’ clinical experience were considered too inexperienced to provide relevant information about the study-related variables. Nurses who occupied administrative roles were also excluded because it was previously reported that they spent only 25% of their time in direct patient care (Armstrong et al., 2015).
Potential participants were approached by the main researcher or by the research facilitators in their institutions and the purpose of the study explained. Those who met the inclusion criteria and agreed to participate were asked to sign a consent form. Thereafter, nurses were provided with a paper survey. To ensure anonymity, participants were provided with a self-sealed envelope to place the completed tool, which was collected by the study researcher within 1 week after distribution. Approval for this study was issued by the Institutional Review Board (IRB) at the Applied Science Private University, Amman, Jordan, and each of the IRBs of participating hospitals.
Questionnaires ascertained information about (a) worker demographics (sex, marital status, and age), (b) Hospital Survey of Patient Safety Culture (HSPSC), and (c) Practice Environment Scale of the Nursing Work Index (PES-NWI).
Patient safety was measured using the HSPSC. The instrument is composed of 12 subscales and 42 items. The HSPSC was initially devised by the Agency for Healthcare Research and Quality (AHRQ) in 2012 to assess organizational perception of safety culture with the intent to identify areas of improvement, discover progress in patient safety culture, evaluate cultural effect on patient safety, and compare results internally with external benchmarks (Sorra & Nieva, 2004). The 12 sections of the instrument are (a) teamwork within hospital units, (b) supervisor/manager expectations and promotion of safety, (c) organizational action for learning and continuous improvement, (d) feedback and communication in relation to error, (e) communication openness, (f) staffing, (g) nonpunitive response toward error, (h) management support about patient safety, (i) teamwork across units, (j) hands-off and transitions, (k) overall perceptions of safety, and (l) frequency of reporting events. This scale is reliable and valid with Cronbach’s alpha of .63 to .84 (AbuAlRub & Abu Alhijaa, 2014). The subscale that was used in this study was the Overall Perceptions of Patient Safety, which is comprised of four items: Patient safety is never sacrificed to get more work done, our procedures and systems are good at preventing errors from happening, it is just by chance that more serious mistakes do not happen around here, and we have patient safety problems in this unit. Each item is rated by a 5-point Likert-type scale, with scores ranging from (1 = strongly disagree to 5 = strongly agree; Sorra & Nieva, 2004). The Likert-type scale was collapsed to form three categories: (a) the two lowest scores (negative response), (b) the two highest scores (positive response), and (c) responses at the midpoint of the Likert-type scale (Famolaro et al., 2016). For this scale, we calculated the average number of positive responses over the total number of items as recommended by the developer (Famolaro et al., 2016). Items that scored 50% or less are considered as areas requiring improvement as reported by AHRQ (Famolaro et al., 2016). The score for each dimension of the instrument was calculated as the average number of positive responses over the total number of items. The higher the score, the better is the perception on patient safety culture (AbuAlRub & Abu Alhijaa, 2014).
We employed the PES-NWI to measure the nursing work environment. It is a reliable and valid Likert-type scale with Cronbach’s alpha ranging between .88 and .98, and has been widely used in the literature (Lake & Friese, 2006; Warshawsky & Havens, 2011). It is composed of 31 items using the following response format of 1 = strongly agree to 4 = strongly disagree. It measures five areas: (a) staffing and resource adequacy, (b) nurse manager’s ability, (c) nurse participation and advancement, (d) nursing model for professional growth and quality assurance, and (e) collegial nurse–physician relationship (Lake, 2002). In this current study, Cronbach’s alpha for this scale was .971.
Data Analysis
The Statistical Package for the Social Sciences, Version 22 (SPSS 22) was used to analyze data. Descriptive analysis was utilized to describe the demographic data of the respondents. Composite scores of the PES-NWI and the overall perceptions of patient safety were obtained after we reverse-coded the negatively worded items as recommended by Lake (2002). The dependent variable was perceived patient safety culture, while the independent variables included worker demographics and the PES-NWI. Covariate correlation was conducted to assess the magnitude of the relationship between perceived patient safety and the dimensions of nursing work environment. Pearson’s R was computed to determine the magnitude of the relationship between the Nursing Work Environment and the Overall Perceived Patient Safety subscales. Logistic regression was employed to examine the predictors of patient safety. Adjusted models were calculated which controlled for demographics and PES-NWI variables. Adjusted odds ratios (AORs) and 95% confidence intervals (95% CIs) were calculated.
Results
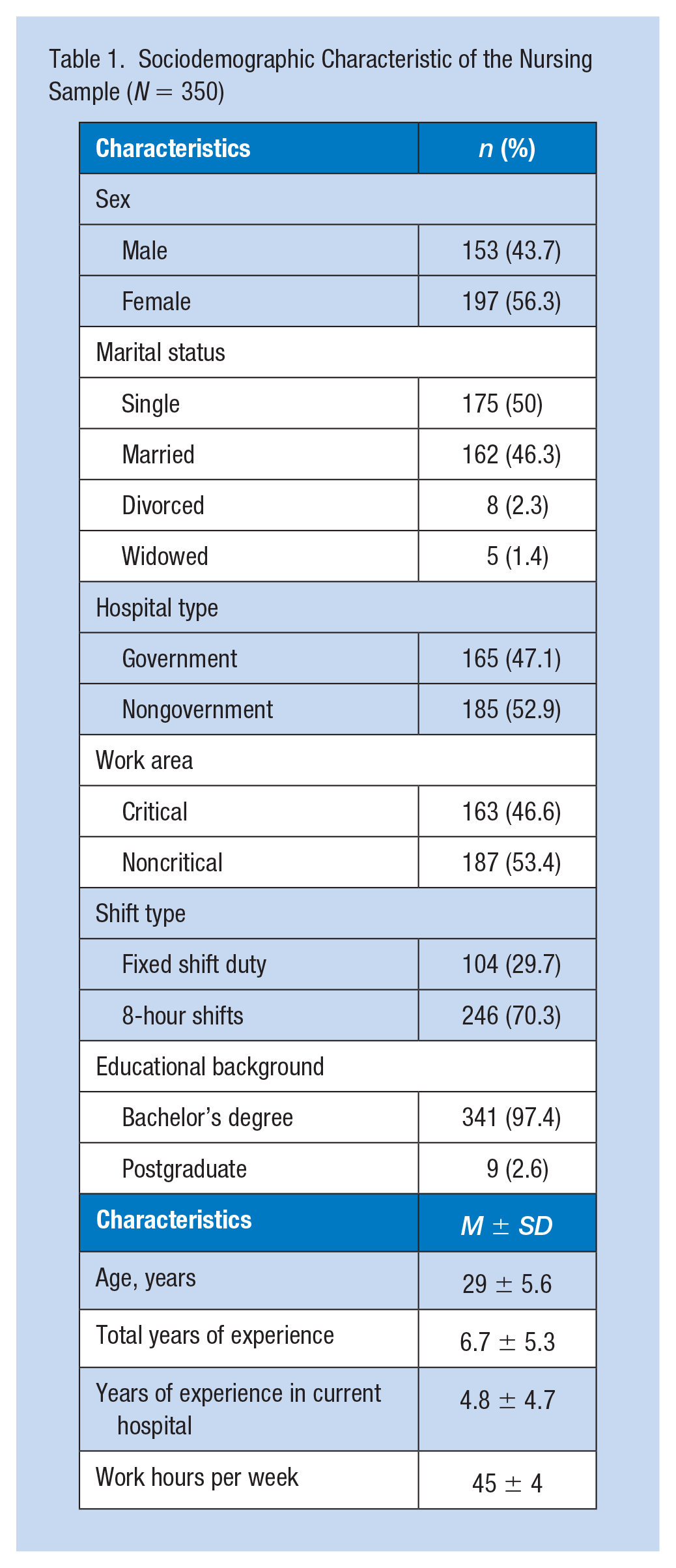
A total of 368 nurses responded (response rate of 64.6%), and 18 questionnaires were excluded due to missing data. This sample included 350 participants; 56.3% were women, 50% were single in comparison with 46.3% married, 3.7% were either divorced or widowed, and 52% worked at nongovernmental (private and nonprofit) hospitals (Table 1). The mean age of the study participants was 29 (SD = ±6) years. In relation to the educational levels, 97.4% had a bachelor’s degree and 2.6% had a postgraduate degree. The average years of experience was 6.7 (SD = ±5.3). A vast majority (70.3%) of the participants of the study worked 8-hour shifts compared with 29.7% who worked 12-hour shifts.
Sociodemographic Characteristic of the Nursing Sample (N = 350)
The nurses’ positive response in relation to perceived patient safety reached 35.2% for the “Overall Patient Safety” subscale, taking into consideration that each item that scored 50% or less is considered as area requiring improvement (Famolaro et al., 2016). Analysis of individual item responses of this subscale revealed that 52.9% of the nurses perceived that the “procedures and systems at their units were good at preventing the occurrence of errors.” Moreover, 36.3% believed that “patient safety is never sacrificed to get more work done,” 27.4% perceived “no safety problems in their clinical unit,” and 24.2% believed that “chance has nothing to do with preventing serious mistakes.” Figure 1 illustrates the percentages of positive responses per item in the overall perceived patient safety.
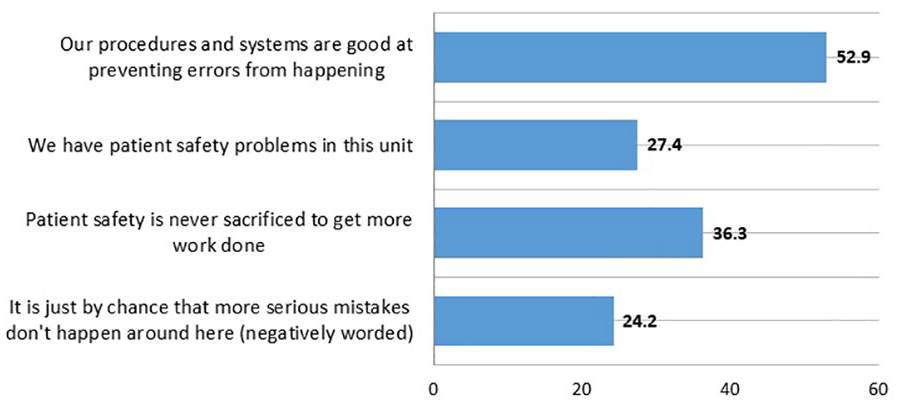
Percentage and distribution of positive responses per item in the Overall Perceived Patient Safety scale (N = 350).
Table 2 illustrates M (±SD) for all dimensions of PES-NWI. The highest nursing work environment dimension was for Collegial Nurse–Physician Relationship, the average score was M = 2.84, SD = ±0.83, followed by Nursing Model for Professional Growth and Quality Assurance, M = 2.73, SD = ±0.60. Conversely, the lowest nursing work dimension score was for Staffing and Resource Adequacy (M = 2.40, SD = ±0.83). The overall Nursing Work Environment (M = 2.65, SD = ±0.71) and Nurse Participation in Hospital Affairs (M = 2.65, SD = ±0.72) had similar weight in terms of patient safety, respectively.
The PES-NWI (N = 350)
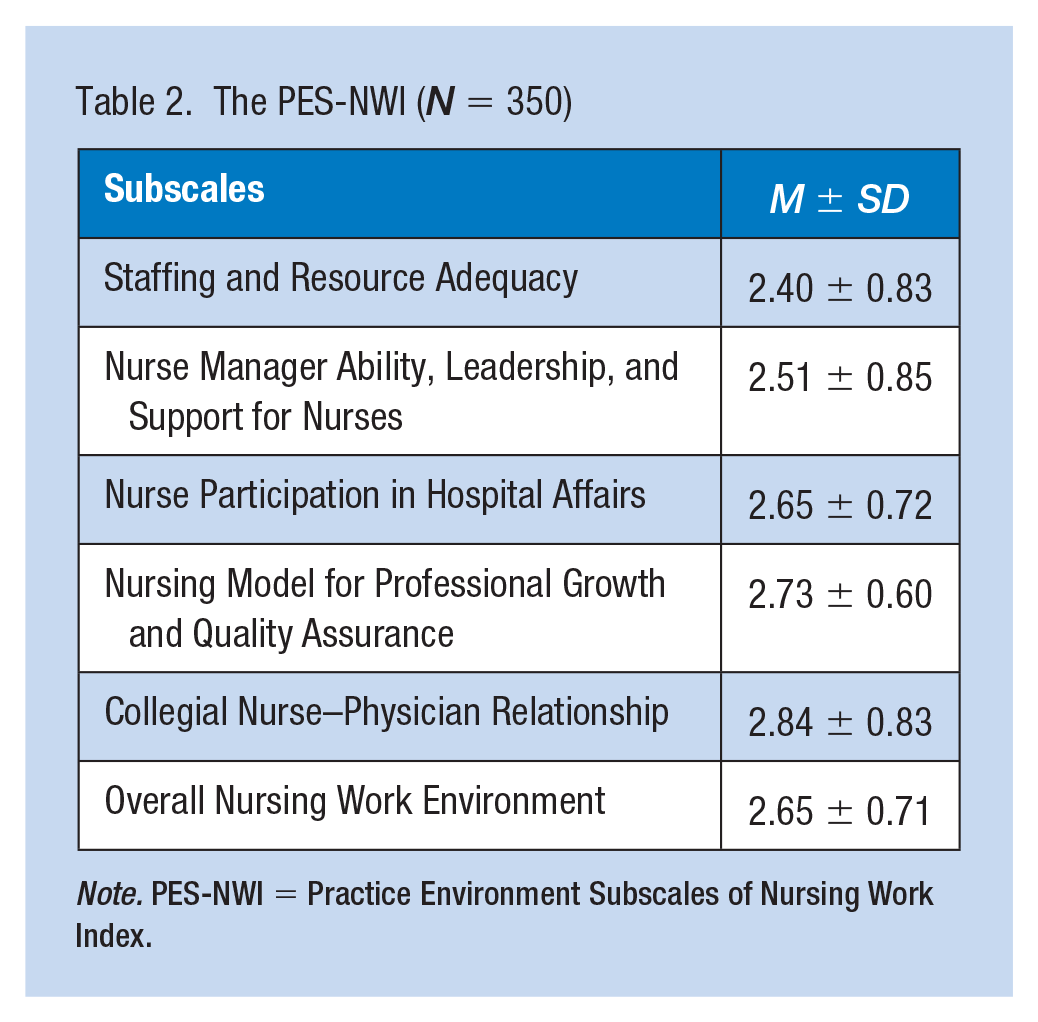
Note. PES-NWI = Practice Environment Subscales of Nursing Work Index.
Table 3 shows that the selected subscales of nursing work environment correlated positively with the Perceived Patient Safety Culture scale. Nurse manager’s ability yielded the highest correlation with perceived patient safety culture (r = .579, p < .001), followed by staffing and resource adequacy (r = .565, p < .001).
Correlation Measures of Perceived Patient Safety and Selected PES-NWI (N = 350)
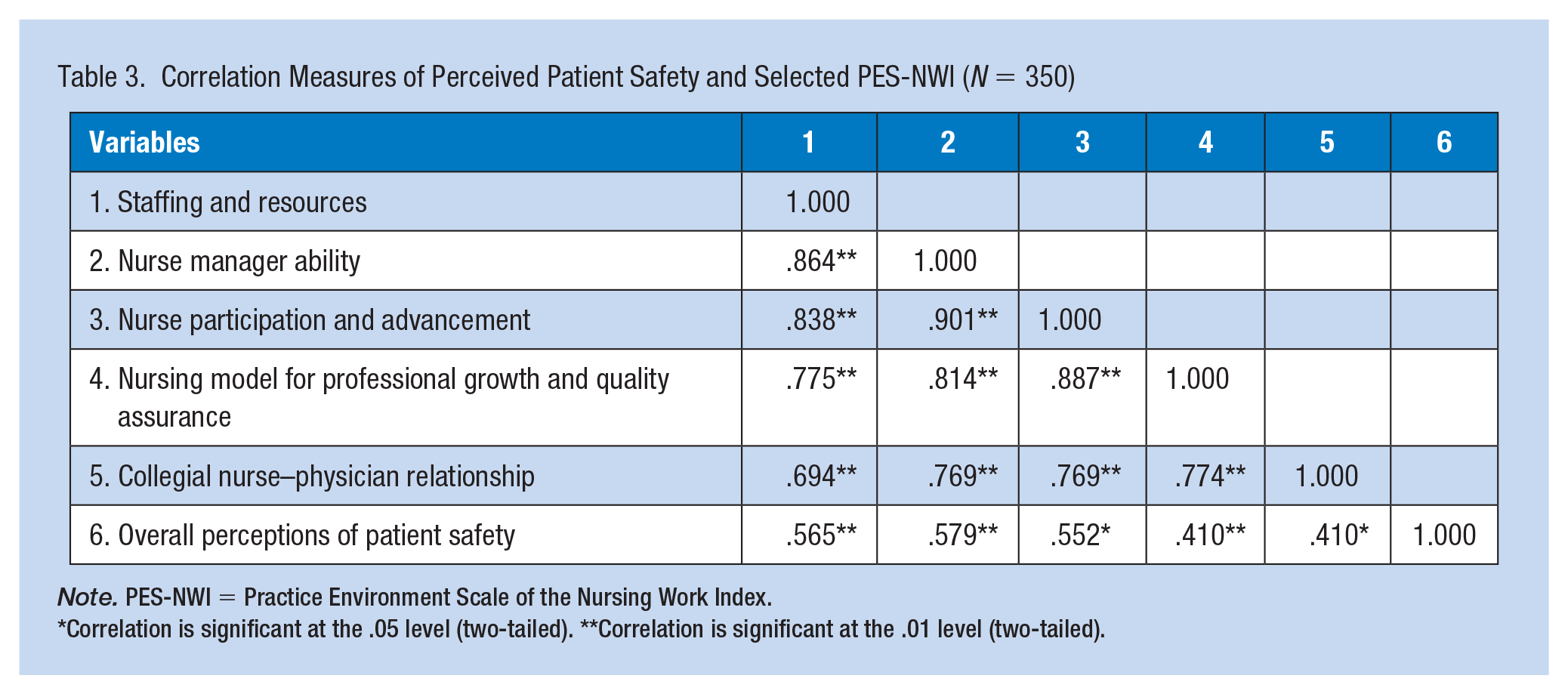
Note. PES-NWI = Practice Environment Scale of the Nursing Work Index.
Correlation is significant at the .05 level (two-tailed). **Correlation is significant at the .01 level (two-tailed).
For the multivariate analysis, Table 4 illustrates that only sex in the sociodemographic factors was a significant predictor of the perceived patient safety culture (AOR = 0.419, 95% CI = [0.224, 0.783]). Marital status and age did not have a significant relationship to perceived patient safety culture. Female nurses’ perception of patient safety culture was lower than that among male nurses. The regression analysis indicated that three out of five subscales of nursing work environment were significantly associated with perceived patient safety. Those who perceived that the staffing resources were low were more likely to report lower perception of patient safety culture (AOR = 0.441, 95% CI = [0.201, 0.968]), and those who recognized that nurses do not participate actively in the hospital affairs are 4 times more likely to report low score on perceived patient safety (AOR = 0.40, 95% CI = [0.16, 1.02]). Nurses who perceived low levels of collegial nurse–physician relationship were approximately 3 times more likely to report negative patients’ outcomes (AOR = 0.27, 95% CI = [0.134, 0.567]).
Multivariate Model of Sociodemographic and Nursing Work Environment (PES-NWI) Subscales on Patient Safety (N = 350)
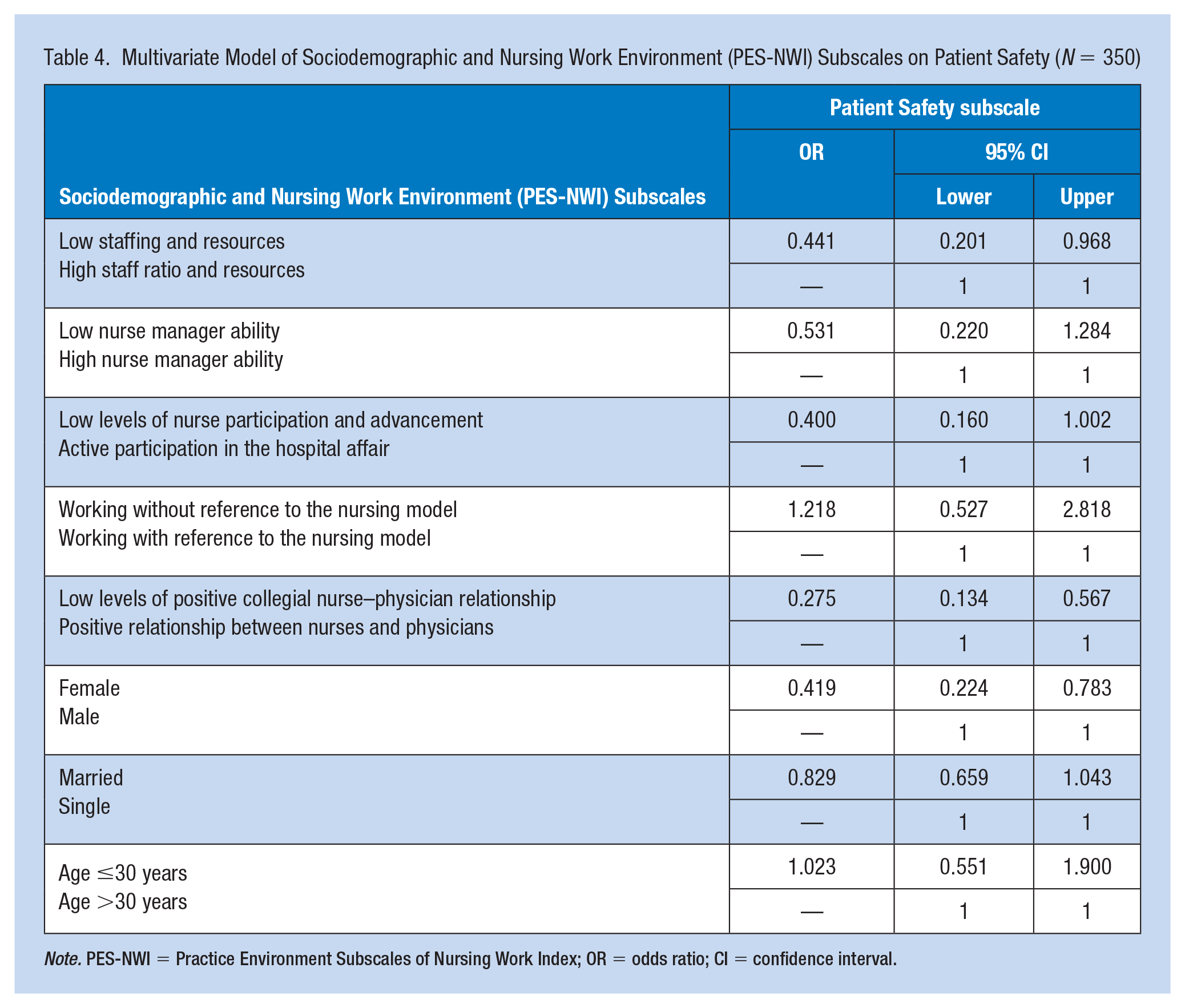
Note. PES-NWI = Practice Environment Subscales of Nursing Work Index; OR = odds ratio; CI = confidence interval.
Discussion
To our knowledge, this study is the first to evaluate a possible relationship between perceived patient safety and the nursing practice environment among Jordanian nurses. The findings of this study revealed that nurses perceived there was a significant relationship between the nursing work environment and perceived patient safety. The nurses perceived a low level of patient safety in our sample of hospitals in Jordan. Around half of the participants of this study reported that the procedures and the health system are not good at preventing mistakes, and around two thirds of them believed that patient safety was jeopardized to get more of the work done. Moreover, around three quarters of the study participants provided negative responses in relation to the occurrence of mistakes and reported that critical mistakes were prevented by chance. These results could be related to the shortage of nurses and the high workload in hospitals in Jordan (Khater et al., 2015; Mrayyan, 2006). Furthermore, the health system in Jordan is lacking the use of innovative technology such as barcode scanning and Computer Physician Order Entry (CPOE), which would reduce medical errors and enhance positive patients’ outcomes (Salami et al., 2018).
The most significant predictors of perceived patient safety were adequacy of staffing and resources. This could be explained by the high workload that is encountered daily by nurses. Jordanian hospitals experience high pressure due to the fact that nurse–patient ratio on average is one nurse for nine to 14 patients, in comparison with other regions such as the United States in which nurse–patient ratio is one nurse for five patients (Salami et al., 2018). Such nurse–patient ratios are highly likely to reduce the quality of care and result in poor patients’ outcomes. These findings lend support to previous literature, which reported that high workload would reduce the quality of patients’ care and lead to negative patients’ outcomes (DeCola & Riggins, 2010; Habibi et al., 2017). Moreover, the current study showed that nurses’ participation in hospital affairs and advancement predicated higher levels of perceived patient safety. The possible reason is that effective engagement by nurses in hospital management would empower them to make decisions in relation to patient safety, which in turn lead to positive patient outcomes and vice versa. Similarly, previous studies reported that nurses’ participation and advancement are key issues in respect to patient safety (Habibi et al., 2017; Mudallal et al., 2017; Sears & Stockley, 2017).
The study findings revealed collegial nurse–physician relationships are an important aspect of perceived patient safety. These results lend support to former research that found a significant relationship between professional nurse–physician interconnection and patient safety (Cho & Han, 2018). Miscommunication between nurses and physicians was reported to be the leading cause of inadvertent patient harm (Sears & Stockley, 2017), and professional communication is important for patient safety. These findings are consistent with other literature that reported professional communication would increase the levels of patient safety and enhance the quality of patient care. In addition, alarming results were reported by the Joint Commission for Hospital Accreditation in which around 2,455 events in U.S. hospitals that jeopardized patient safety were analyzed and found that communication failure was a main cause for such incidents (Sears & Stockley, 2017). Effective communication and teamwork in promoting positive patients’ outcomes is crucial (Cho & Han, 2018).
This study is similar to other cross-sectional designed studies in which some limitations need to be considered. The nature of the mentioned design does not allow the study to draw causal associations. Furthermore, the study recruited a convenience sample of nurses, and this type of sampling has its own limitations as only motivated individuals to participate. This also limits the generalizability of the study findings. Moreover, this study was conducted in hospital settings; hence, the study did not echo the voice of nurses working in primary health care settings. Although the study has limitations, we believe that it has yielded important empirical data that would be the baseline data for upcoming research, not only in Jordan but also in the Arab region where such data are scarce.
Conclusion
This study provided empirical results about perceived patient safety culture in relation to nursing work environment among nurses. It is paramount to focus on specific dimensions of the nursing work environment, such as staffing and resources adequacy, nurses’ participation and advancement, and communication style to improve the quality of care provided to the patients. Taking into account that nursing is a science and art that deals with patients on a continuous basis, the provision of care should be combined with a positive work environment that empowers nurses to improve patients’ outcomes.
Implications for Occupational Health Nursing Practice
The nurse work environment has gained great attention because it is a detrimental factor that influences health care practices. Working in conditions with high working load, lack of staff and resources, unprofessional communication, and lack of engagement in decision-making policy in hospitals would negatively affect the nurses’ physical, psychological, and social health, which in turn will result in negative patient outcomes. If these conditions lasted for a long time, they might result in an irreversible harm in terms of patients’ care and nurses’ health, leaving minimal options for impactful recovery. Poor work environment dimensions including the constraints in reaching management positions (lack the access to work of greater complexity); might result in disruption in nursing self-worth, increasing the role ambiguity, which in turn might lead to low-quality of life among nurses. In addition, health difficulties would stem from physical overload that is related to shortage of staff and work resources. Hence, the finding from this study embodied the importance of considering teaching occupational health to nursing students to help nurses be more aware and well suited for supporting, advocating, and planning initiatives that serve health care providers as well as patients.
The data provided by our work could be used by policy makers to coordinate and deliver service programs that emphasize the importance of an interdisciplinary approach to health care. In addition, the data can be used to advocate for nurses’ rights in terms of receiving professional communication. Supporting nurses’ rights to be at higher positions in health care settings will encourage nurses to take responsibility for their health. For example, nurses at administrative positions can create exercises/fitness, nutrition activities, and stress management programs. Also, nurses at such positions can encourage research that study workplace health in health care settings.
Applying Research to Practice
This research study suggests that there are significant nurse work environment dimensions that may not be directly observable. These dimensions include safe nursing staffing levels and availability of resources, nurses’ participation levels in decision making at the organization, and communication and collegial relationship. Occupational health nurses should focus on these dimensions, as they can be determinant factors affecting the health of both nurses and their patients. Occupational health nurses may use a variety of approaches to address the impact of these dimensions on health. This includes enhancing hospitals’ preparedness to implement safe nursing staffing levels, ensuring availability of safe levels of practice resources, supporting nurses’ participation in leadership activities, and enhancing collegial relationship and communication between health care providers. In addition, occupational health future research can build on the results of this study by investigating the impact of each nurse work environment dimension separately on nurses’ safety and patient safety.
Footnotes
Acknowledgements
The authors are thankful for all the nursing managers, research facilitators, and nurses who generously shared their time for the purpose of this study. They also acknowledge the effort of Professor Samiha Jarrah for her support, and Dr. Ahmad Saifan, Dr. Waddah Aldomeh, and Dr. Malakeh Malak for their invaluable feedback.
Author’s Note
Rima Darwish is now affiliated with the Jordanian Medical Services as an Endodontic Resident.
Author Contributions
M.M. conceived the study, participated in its design, collected the data, and drafted the manuscript. R.A.-A. and R.D. conducted the statistical analysis, wrote the “Results” section, and provided substantial contribution in editing drafts of the study. S.R. and T.A. wrote the “Discussion” section and edited the final draft. All authors read and approved the final manuscript.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Permissions
The permission to utilize the study instruments was gained from their respective authors via email. The Hospital Survey of Patient Safety Culture (HSPSC) was gained by contacting the Agency for Healthcare Research and Quality (AHRQ) who devised the scale (despite being available for use without permission). Practice Environment Scale of the Nursing Work Index (PES-NWI) secured by contacting the author Ms. Lake also via email.
Author Biographies
Maha Mihdawi, RN, MSN, is lecturer at Isra University of Jordan (IUJ), School of Nursing and Midwifery. She received her MSN degree in clinical nursing from the Applied Science University in Amman, in 2016. She worked as nursing quality improvement coordinator; she designed and implemented many performance improvement and patient safety projects.
Rasmieh Al-Amer, RN, BSc, MSc, PhD, is assistant professor in mental health nursing at IUJ, School of Nursing and Midwifery. She is an adjunct fellow with Western Sydney University at School of Nursing and Midwifery. Her research interests include mental health issues, patient safety, and nursing workforce mental health.
Rima Darwish, DDS, is doctor in Ministry of Health. She had her bachelor’s degree of dentistry from Jordan University in Amman.
Sue Randall, RGN, PhD, is senior lecturer in Primary Health Care Nursing at the University of Sydney, Susan Wakil School of Nursing and Midwifery, Sydney, Australia. Her teaching and research seek to address workforce issues and improve equity and access, thus improving quality of care and outcomes for patients.
Tareq Afaneh, RN, MSN, CPHQ, is head of Planning, Studies, and Policies Department, Jordanian Nursing Council. He is a PhD candidate at University of Jordan, School of Nursing. He has been directly involved in performance improvement at organizational level of different health care organizations.