
Abstract
Background: Nurses working in hospitals face unique influences on their workplace dietary behaviors, but little is known about what nurses experience as dietary influencers in the hospital setting. Understanding these influences is paramount in developing effective programs that target healthy workplace eating. This study aimed to explore hospital shift nurses’ experiences and perceptions of influences on making healthy nutritional choices while at work. Methods: This qualitative, descriptive study was guided by the Theoretical Domains Framework and analyzed using thematic analysis. Twenty-one Registered Nurses working 10- to 12-hour shifts in hospitals in South Carolina, USA, in 2018 were interviewed individually or in focus groups about their workplace dietary behaviors and influences. Findings: Framework constructs most relevant to hospital shift nurses included (a) environmental context and resources; (b) social/professional role and identity; (c) memory, attention, and decision processes; (d) social influences; (e) emotion; and (f) behavioral regulation. In addition, four major themes emerged: (a) Nursing roles and responsibilities restrict freedom of movement and minimize individual control over dietary practices; (b) The hospital food environment is oppressively unhealthy; (c) Free food is currency and influences consumption; and (d) Shift work is a major barrier to healthy eating. Conclusions/Applications to Practice: To achieve healthy eating practices in the workplace, hospital shift nurses need supportive systems, policies, and interventions that target and reduce the barriers inherent in hospital-based nursing shift work. To improve hospital shift nurses’ workplace dietary behaviors, these findings should inform hospital food policies, workplace wellness programs, administrative practices, and staff education.
Background
Nurses comprise the largest health care profession (approximately three million) in the United States, making a healthy nursing workforce imperative to meeting national health care needs (U.S. Department of Health and Human Services, Health Resources and Services Administration, 2010). Initiatives such as the Healthy Nurse and Healthy Nation™ Grand Challenge aim to improve nurses’ health, and in turn, the health of their patients (American Nurses Association, 2018). Yet, nurses continue to suffer from a multitude of health concerns due, in part, to the unique nature of their role and where they work (American Nurses Association, 2017; Occupational Safety and Health Administration, 2013).
Nurses are most likely to work in hospitals, where staffing is required 24 hours a day and 10- to 12-hour shifts typically are used for coverage (U.S. Department of Health and Human Services, Health Resources and Services Administration, 2010). Shift work, across various industries, is associated with unhealthy eating and obesity (Amani & Gill, 2013; Han et al., 2011). Similar to the general population, most nurses continue to follow the standard American diet which is low in fruits, vegetables, and unprocessed foods (American Nurses Association, 2017); the number one risk factor for death and disability in the United States (Murray et al., 2013). As a result, most U.S. nurses are overweight or obese, increasing the risk of many chronic illnesses (American Nurses Association, 2017; Krussig et al., 2012).
Interventions that encourage proper nutrition for health promotion and disease prevention have the potential to improve nurses’ health (Slawson et al., 2013). Even with the advent of many workplace wellness programs in hospitals over the last decades, few have specifically targeted nurses for dietary behavior change (Torquati et al., 2017). An integrative review by Nicholls et al. (2017) assessed nurses’ workplace influences on healthy eating and found few facilitators; rather, they identified many barriers. Most of the reviewed studies were from outside of the United States and included nurses from various practice settings, not just hospitals. However, hospitals are unique environments with internal cultures, structures, and politics, and the influences inherent in hospital shift work may be very different from that in other practice settings. In addition, as cultural and health care systems differ between countries, there is limited applicability to U.S. hospital shift nurses’ experiences. Within the United States, variations in cultural norms and dietary practices can impose additional influences on workplace dietary behaviors. To date, no exploratory studies have examined workplace influences on hospital nurses’ dietary behaviors in the Southeast region of the United States, where many preventable chronic illnesses are the most prevalent (Centers for Disease Control and Prevention, 2014). This study aimed to explore (a) hospital shift nurses’ experiences with healthy eating while at work and (b) nurses’ perceived dietary influencers in the hospital setting.
Methods
Design
The Theoretical Domains Framework (TDF) guided this qualitative, descriptive study, including the design, interview/focus group guides, data collection, and data analysis (Atkins et al., 2017; Power et al., 2017). The TDF includes 14 theoretical domains derived from a synthesis of 128 theoretical constructs from 33 relevant theories; see Table 1 for domains and definitions (Atkins et al., 2017). The TDF represents the multifaceted nature of human behavior, and the inclusivity of the framework offers a versatile tool for categorizing the most salient influences on a particular behavior. The COnsolidated criteria for REporting Qualitative research (COREQ checklist), which is a comprehensive guideline in qualitative research, was followed in reporting this study methods and results (Tong et al., 2007).
Theoretical Domains Framework with Definitions and Associated Findings
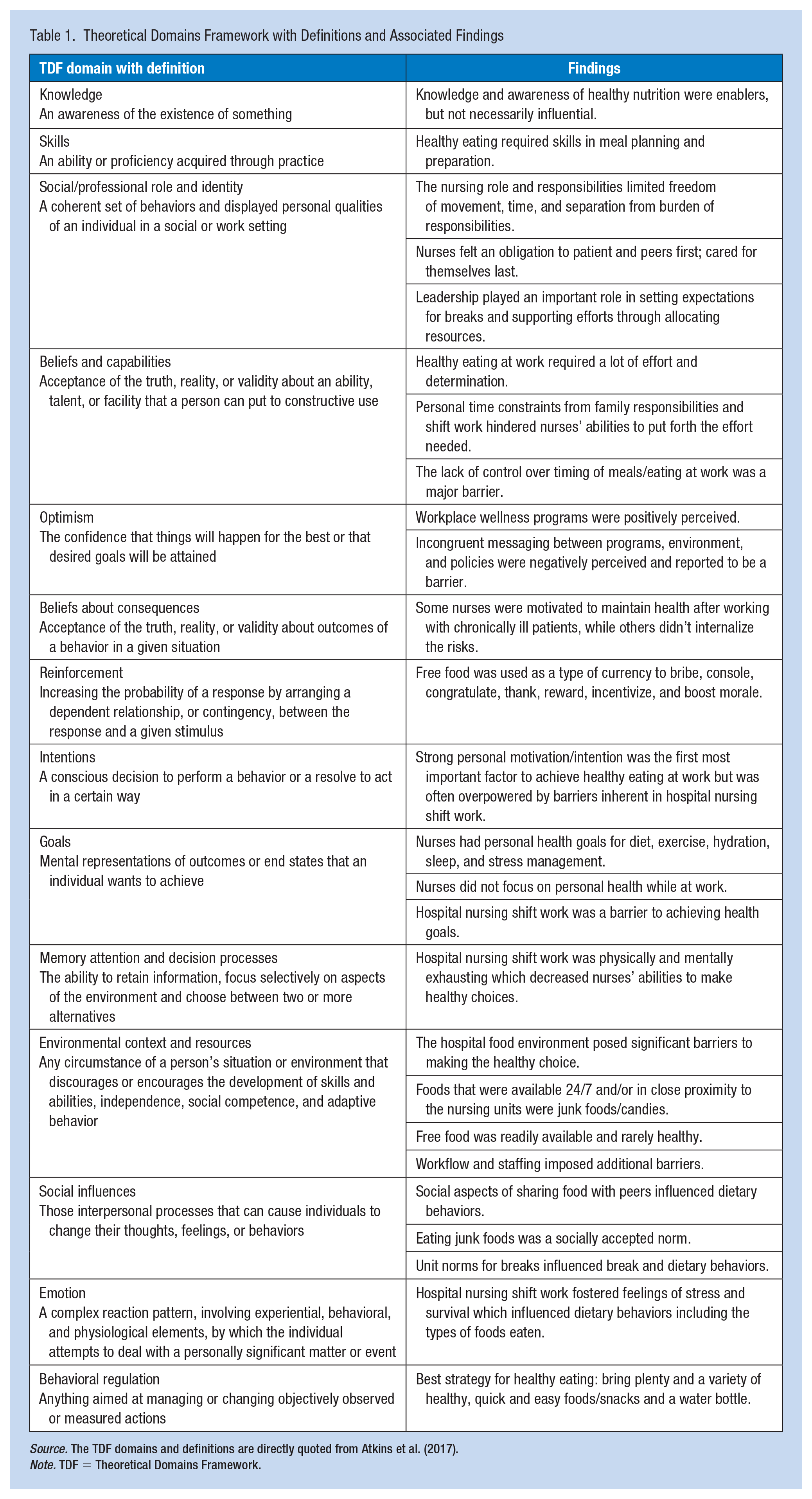
Source. The TDF domains and definitions are directly quoted from Atkins et al. (2017).
Note. TDF = Theoretical Domains Framework.
Prior to the study activities, human subjects’ approval was obtained through the Greenville Health System Internal Review Board (IRB File # Pro00073307). Informed, written consent was obtained from participants prior to data collection. Nurses from seven hospitals in the upstate region of South Carolina were recruited through paper flyers, electronic mailings, and word of mouth. Personal acquaintances of the primary investigator (PI) meeting inclusion criteria were also asked to participate. Participants were informed of the PI’s nursing experience and interest in the research topic. The sample included registered nurses (RNs) currently employed full-time, part-time, or as-needed (PRN) by a hospital, working 10- to 12-hour shifts and able to meet in-person. Based on the scheduling convenience, either an interview or focus group could be chosen by the participant.
Data Collection
In-person interviews and focus groups were conducted using a semi-structured interview or focus group guide with open-ended questions based on the TDF domains. Interviews ranged from 26 minutes to 1 hour; focus groups lasted 40 to 61 minutes. All sessions were held in a quiet room or public space, free from distractions, and were audiotaped and transcribed verbatim. Only participants and the interviewer were present during interviews/focus groups. No incentives were offered for participation and encounters were conducted on the participants’ personal time.
Interviews/focus groups were facilitated by the PI, a female BSN-prepared RN with qualitative research training and 12 years of nursing experience in the acute-care hospital setting. Study design and data analysis were conducted by the PI and a female PhD-prepared Advanced Practice Nurse with expertise in qualitative research methods. During and after interviews/focus groups, the PI conducted reflective journaling and field notes (Williams, 2015). All study materials were kept confidential. Self-reported demographic information was collected without any identifiers attached.
Data Analysis
The data were analyzed according to the TDF, using the thematic analysis approach and began immediately upon data collection (Braun & Clarke, 2006). Transcripts were generated and then compared with the original recordings to assure that the text represented the participant statements as accurately as possible. The iterative processes of transcribing, coding, and returning to further data collection provided a more complex understanding of the themes as they emerged from the data. Both researchers coded the data while considering the TDF so that the primary domains of influence were identified. Although data saturation was achieved at eight participants, data collection continued until a number of RNs representing various work areas and different hospitals were interviewed. To ensure confidentiality, participant quotes were identified by the participant’s nursing specialty.
Results
Sixteen one-on-one interviews and two focus groups (n = 5 participants) were conducted for a total of 21 participants (Table 2). Reported dietary influences were categorized according to the TDF domains. The findings revealed dietary influences from all 14 TDF domains; however, the most relevant to hospital shift nurses included (a) environmental context and resources; (b) social/professional role and identity; (c) memory, attention, and decision processes; (d) social influences; (e) emotion; and (f) behavioral regulation. Findings for each TDF domain are summarized in Table 1 and supporting participant quotes in Supplemental Table 1.
Sample Demographics and Nursing Experience
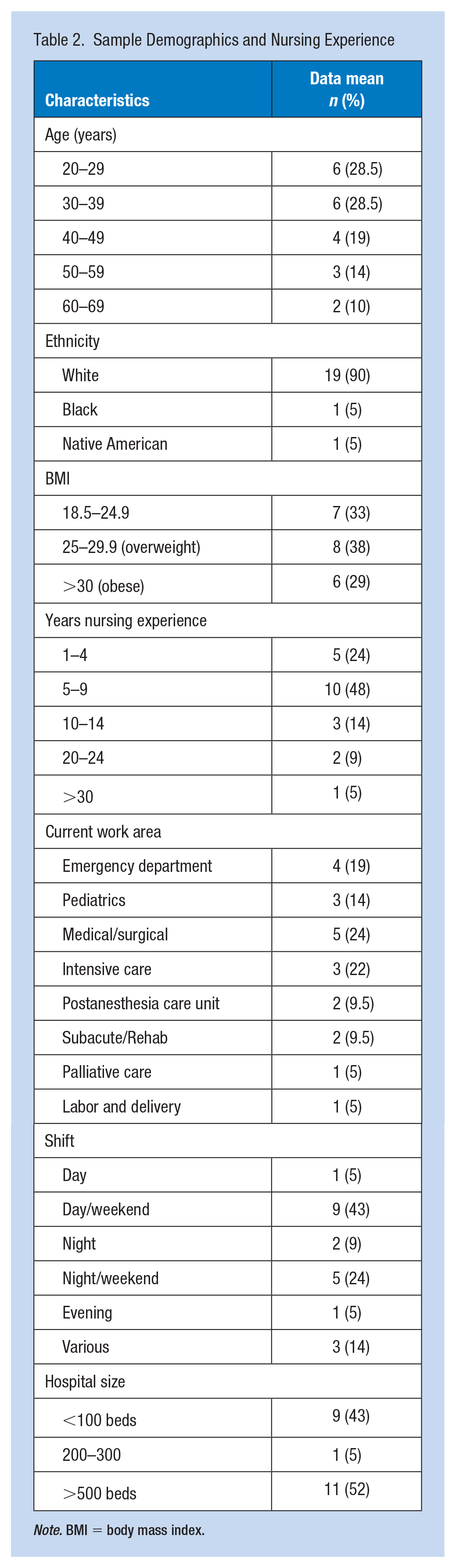
Note. BMI = body mass index.
Major Dietary Influences
The analysis revealed four predominant themes of influence that had the greatest impact on hospital shift nurses’ eating behaviors while at work: Nursing role and responsibilities restrict freedom of movement and minimize individual control over dietary practices; the hospital food environment is oppressively unhealthy; free food is currency and influences consumption; and shift work is a major barrier to healthy eating.
Nursing role and responsibilities restrict freedom of movement and minimize individual control over dietary practices
Nurses with patient assignments retained responsibility for their patients’ health and safety during the entire shift, typically including during breaks. Therefore, nurses could not leave their assigned patients without getting another nurse to cover their responsibilities during that time. Finding coverage could be challenging depending on staffing level and patient acuity. In most acute care areas, nurses that covered for peers on break had their own assigned patient load and were covering an additional set of patients. Depending on the assigned patients’ acuity and pace of workflow, nurses may not have been able to take on the additional responsibility. Furthermore, there was a perceived expectation from other disciplines, peers, and patients that the nurse should be available at all times. This expectation influenced how far away from the unit the nurse could go, the break duration, interruptions, and rest during the break: It is very sick people, and just don’t have the time to get away. And again, they call. If you do sit down to eat lunch, and you have your phone, and you’ve got to have your phone with you, they call you right back. Very rarely, I would say, in the last three weeks I have had two lunches where I actually sat down for 30 minutes, and this just happened to be slower days. (Emergency Department)
Nurses often felt a sense of obligation to their team during busy workflows and preferred to stay and continue to work rather than to take care of personal needs and take a break. One nurse described the hesitancy and obligation she felt about leaving the unit: “I feel like when you are that far away, which isn’t even that far, but when you remove yourself, what if there’s something that comes, like a trauma, or something where your team needs you?” (Emergency Department).
The constant pressure of maintaining responsibility at every moment of a long shift exacerbated busy workflows and caused extra stress which heavily influenced the nurses’ dietary behaviors. Nurses often used “comfort” foods to cope with job-related stress and exhaustion: “If I’ve had a bad day at work, or it’s been a long day at work, I will be like ‘give me the worst thing that I can have’, and I want to go to bed!” (Subacute/Rehab) and You feel like if you are working these long hours, you’re away from your family already, you feel like “I deserve this bag of potato chips, and I’m going to walk it off anyways because I’m going to go to room 10, 15 times in the next 20 minutes!” so you kind of start validating those choices. (Subacute/Rehab)
Regulatory requirements prohibit eating/drinking in patient care areas due to infection control concerns (Occupational Safety and Health Administration, 2018). Yet, nursing responsibilities keep nurses at or near the bedside, creating a burden to go somewhere to get food/drink, no matter how close that is. As a result, nurses reported not eating for long periods and dehydration. Although participants were not asked specifically about drinking practices, most (n = 18) reported dehydration at work. Even if the nurse was able to hydrate adequately, the time-burden of having to go to the bathroom more frequently post-hydrating was perceived as an unwelcome consequence: If I happen to have a lull in between patients, I will grab a quick drink of water, but then if you do drink too much, you have to go to the bathroom and there’s definitely no time for that! (Post-Anesthesia Care Unit)
When nurses became very hungry but didn’t have the time or ability to step away, foods were stored in pockets, bags, or drawers at the nurses’ station. These were typically dry, quick, and easy-to-eat foods while on the go: Whatever I can put in my mouth when I am walking or running or moving, it has to be convenient, so most things that are convenient aren’t really healthy. I can’t really walk down the hall eating an apple or a banana, but I can stick a bag of chips in my pocket, or a pack of cookies in my pocket that I can snack on when I’m running around (Subacute/Rehab)
Hurried eating was another alteration from normal eating patterns. Due to the nurses’ responsibilities and busy and uncertain workflows, sitting down and eating at a normal pace was often not possible, affecting the types and amount of foods consumed: If you’re a nurse, you don’t stop until your patients are done and they don’t need you. And that’s when you take care of yourself. You’re holding your bladder and you’re eating junk food instead of the salad you made for yourself, because it’s quicker and you can get back to your patients. (Emergency Department)
Even when nurses were prepared and motivated to eat healthfully at work, the lack of control over workflow and timing of patient-care needs dictated when and how they could eat. This was especially true for areas with a high degree of uncertainty in the workflow, such as the Emergency Department: “You can’t say like every day at 6:30, maybe before shift change, ‘I’m going to sit down and take 31 minutes to eat’, because that’s just not always an option” (Emergency Department), or in small units with limited staffing: “We get a lunch break, but we don’t really get a break, because if there’s only two of us, it’s not like someone can just go away. If someone needs something, we are still there” (Pediatrics), or on night shift: It’s a small unit; we can’t clock out and go anywhere . . . you should be able to take your 30 minutes and do what you want with it, and you can’t here. So, that makes it a little bit difficult because it would be nice to go off and do something; go for a walk, but you can’t. I can’t leave. (Intensive Care Unit)
Hospital food environment is oppressively unhealthy
The food landscape inside the hospital was a major influencer on nurses’ dietary behaviors due to the disproportionate availability of unhealthy food options as opposed to healthy ones. There were three main channels of food access in the hospital: (a) food for purchase, which included cafeteria and vending; (b) brought-in food (e.g., packed lunches); and (c) free food, which was any kind of food/candy/beverage available at no financial cost. Free food was frequently available in the hospital environment and was usually found in close proximity to nurses (e.g., the nurses’ station), influencing consumption. Free food emerged as a separate predominant theme and is discussed later in detail.
Healthy choices available for purchase were generally limited to a baked option and/or salad bar only in the cafeteria. The cafeteria, however, was not open 24/7, and in smaller facilities, might be closed at night and/or on the weekend: The cafeteria here does have these healthy choice options that they put out every week, but its only targeted for one small specific group of people, and you think about the bigger population that’s here working in the hospital, that’s the minority who work 7 to 3. (Emergency Department)
Furthermore, tempting “comfort” foods were made available in the cafeteria and distracted nurses from the healthy options: “It’s the same old salad every day, and I don’t want a salad, and then it’s like, ‘oh well, they have chicken alfredo or ravioli!’ and I’m going to get pasta!” (Medical/Surgical). Nurses also reported that cost influenced choice. Healthy options tended to be more expensive, with salads costing upward of US$12 as compared to a US$2 hamburger: “The healthy options that they have here are expensive. You are not really going to, in a real world, pay $5 and some change for a cup of strawberries” (Subacute/Rehab).
In addition to the limited hours and options, some nurses had the challenge of accessing a cafeteria located remotely from the nursing units. The time needed to get to the cafeteria—and potentially stand in line—was a barrier to nurses who were restricted to 30-minute breaks: Everyone says “Oh my god! You eat so fast!” I said “because I am a nurse!” I have about 16 minutes to eat by the time you walk all the way there and then you have to walk all the way back. (Post-Anesthesia Care Unit)
Outside of the cafeteria, foods for purchase were obtained from vending machines, gift shops, fast food restaurants (located both inside and outside the hospital), and restaurant delivery. Vending machines were the main food source available on site 24/7, typically on or near the nursing units, and stocked with processed, calorie-dense, low-nutrient snacks and candies. When nurses were pressed for time, tired, and hungry, vending machine foods became the easiest option: It’s really easy to just walk over to a vending machine and grab something. When you haven’t taken a bathroom break in six hours, it’s hard to take the time to go back and pour dressing over your salad and then actually eat it as opposed to just grabbing a Snicker’s bar. (Emergency Department)
The hospital food landscape and stressful environment posed barriers for healthy eating. The stress and exhaustion that nurses felt while at work inhibited their ability to make the healthy food choice given the abundance of unhealthy foods: It’s kind of odd how many unhealthy options there are, even in the hospital cafeteria, just like those giant pastries and stuff like that . . . even if you’re a family member there, or working there, or, no matter why you are in the hospital, you are probably under some kind of stress, and you don’t always make the best decisions when you are like that. (Intensive Care Unit)
Free food is currency and influences consumption
Free food was a common element in the hospital environment and became a kind of currency exchanged for many reasons. In cases where offering money would be inappropriate, nurses were given free food.
Leadership offered free food to nurses as a reward, incentive, consolation, and for celebrations. Free food was also used as a bribe for attendance at meetings, to lure staff into management’s office, and to boost morale on the unit. Patients and families offered free food to nurses to show their appreciation. Peers brought and shared food for comradery. Typically, free foods included indulgent, low-nutrient, “comfort” foods such as candy, cookies, pizza, chips, cake, and donuts. The availability of free junk foods in the environment influenced nurses’ consumption: I try not to eat those things. I will say, I have had a cookie or two, so there are things that I’ve eaten that I wouldn’t normally choose. (Emergency Department)
An Emergency Department nurse added, Usually when people are bringing in extra snacks for everybody, you are snacking, you are eating some of that. Even if you don’t want it, you are eating it, because it’s there. You are walking by, you see it, it’s there, I’m going to have some of that.
The very fact that food was provided at no cost, influenced consumption: It doesn’t matter [what it is], if it’s free food, I’m going to take it! (Medical/Surgical)
Another nurse explained the power of free food: Honestly, we are the easiest people to bribe. Give us food . . . we will eat it! We don’t really turn down free food. That’s the hardest part if you are trying to be good and trying to not have that temptation, you go into work and you are just like, “but there’s donuts and all this stuff on the table, and I just want one!” . . . And then one turns into four, and then, you are like “well, I guess I was already bad today, so I guess the week is kind of already shot, so I’ll start again Monday” and then it’s just a vicious cycle. (Pediatrics)
All participants reported access to free food on a regular basis. Due to social aspects, ease of access, and the indulgent types of foods provided, nurses were inclined to consume free foods adding unplanned calories to work days.
Shift work is a major barrier to healthy eating
The eating patterns of nurses while at work were significantly different from home, largely because of the lengthy shift. Working 10- to 12-hour shifts caused nurses to eat earlier, later, or in the middle of the night. Often, they did not eat at all. Most nurses ate when they returned home, and due to time constraints imposed by long shifts, would then go to bed with a full stomach. Subsequently, nurses suffered from sleep-quality compromise, gastric reflux, and weight gain.
Overeating was reported as a common occurrence due to exhaustion and extreme hunger after lengthy shifts and long periods without food: If you wait too long to eat, you will overeat, you’ll stress-eat. There tends to be way too many sweets, like candies or stuff that families will bring in to you, and you will gorge yourself on that if you are waiting too long to eat, so you shove like 5 fun-size Snicker’s in your mouth. (Intensive Care Unit)
If nurses anticipated that breaks would be unlikely, then eating when and what was available, even if not hungry, was common. One nurse described this as a survival instinct: I get home, I’m like “wow! I ate three doughnuts while I was at work today!” But it’s almost like a panic, is what I feel when I think back on it. I wasn’t thinking about why I was eating it, I was just thinking that I should eat it, or needed to, in the frame of mind that I was in . . . it’s that panic feeling and then not knowing when you’re going to be able to eat again. (Medical/Surgical)
Nurses perceived the need for quick energy to perform their best during long shifts. Fast, high-caloric foods and caffeine were commonly used during busy workflows and during slow workflows to ward off boredom or sleepiness: Third shifters are known to gain more weight than day shifters because 3 or 4 in the morning, its carb frenzy! I mean, your body is like “carb! carb! carb!” . . . you think you are doing good and then, you just need that pick-me-up, and then its carbs. (Medical/Surgical)
Shift work encroached on personal time, especially when working several long shifts in a row, and it inhibited the nurses’ ability to shop, cook, and pack food for work. Due to a total lack of options and a higher degree of difficulty in purchasing healthy foods while at work, 100% of the nurses cited bringing meals and snacks as being the best strategy to healthy dietary practices. However, even when able to bring healthy foods, there were barriers in the workplace to eating it. The abundance of tempting foods, social aspects of free food, boredom with the same packed lunch, and the inability to take a break were reasons why bringing healthy foods from home did not guarantee consumption. Still, nurses recommended bringing a variety of healthy, quick, and easy foods to increase the likelihood that they would be consumed.
The challenge in a hospital environment, where the nurse is confined for 12 hours, was that eating healthfully was often the “hard” choice. When asked how easy or difficult it was to eat healthfully during a shift, all responded with the sentiment: If I don’t pack something, I would say that it’s very difficult. That’s again due to availability, cafeteria’s only open very limited time, can’t go far away, usually your choices in the vending machine are junk. (Emergency Department)
Discussion
Hospital-based nurses were able to identify workplace influences on their eating habits. Hospitals are unique environments that pose distinct challenges to maintaining and improving employee health. Shift work and busy workflows, often present in hospitals, were major contributors to unhealthy dietary practices by nurses. Nursing responsibilities, which are unique and constant, influenced dietary behaviors. Beyond feeling obligated, nurses are in fact legally required to remain with patients and address needs (South Carolina Law, n.d.). The role of the bedside nurse, in this way, is different from any other discipline on the treatment team. For example, while medical doctors have a legal obligation to the patients’ health care, the nurse is responsible to address all immediate needs, including physical, emotional, and spiritual, and are expected to remain in close proximity at all times, ensuring quick response. The nursing responsibilities that require nurses to stay in close proximity to the patients affect what, when, and how the nurse eats.
The hospital food environment posed particularly challenging barriers to healthy eating. The abundance of unhealthy foods that were accessible nearby, 24/7, and oftentimes for free, combined with the lack of healthy food options, required nurses to bring food from home if they wanted to eat healthfully. The challenge with bringing healthy meals and snacks to work is the time required for their planning and preparation. The nursing workforce is approximately 93% female, and even though family dynamics have changed with time, women still retain the majority of household activities (U.S. Department of Health and Human Services, Health Resources and Services Administration, 2010; U.S. Department of Labor, Bureau of Labor Statistics, 2016). Shift work and family responsibilities restrict personal time to the degree that having to plan and prepare healthy meals becomes exceedingly burdensome. For nurses exhausted from hospital shift work, the healthy choice quickly becomes the difficult choice.
Given that nurses are the most numerous of health care professionals in hospitals, workplace dietary interventions should first target the food-choice barriers specific to nurses. Location, price, and availability of healthy foods are all important barriers for nurses that if addressed could improve the hospital food environment for all. Shift scheduling may be preferred by administrators and staff, but the many side effects of shift work should be considered when developing policies on breaks and food environments. Adequate time for obtaining healthy foods and the uninterrupted opportunity to eat properly should be of primary focus. Furthermore, nurses are typically involved in patient mealtimes and often provide dietary education. Improving nurses’ knowledge and personal-dietary practices could improve efficacy of patient counseling (Esposito & Fitzpatrick, 2011).
Strengths and Limitations
In this study, the participant demographics reflected the proportions found in the national hospital-based nursing population, except for race. The sample was predominantly White, therefore may not reflect some cultural variations. A body mass index average of 28.4 in this sample, reflected previous findings that nurses were overweight at similar rates to that of the general American population (Han et al., 2011; Krussig et al., 2012). The mix of day/night shift nurses and different practice settings in the sample strengthened the findings by providing a wider understanding of the varying experiences of nurses in hospitals. All participants worked in South Carolina, limiting the transferability to culturally and socioeconomically different locations.
Implications for Occupational Health Practice
Poor dietary practices put the nursing workforce at risk for illness, and the unique barriers that exist for hospital shift nurses were highlighted here. Although each nurse has individual preferences that affect eating choices, there are common experiences in the workplace that contribute to and perpetuate one another, continuing the never-ending cycle of harmful dietary practices. Any break in the chain has the potential to improve nurses’ dietary behaviors. Key interventions that offer potential to improve dietary practices could include (a) Change the workplace food environment using toolkits and guidelines for healthier hospitals available from the Centers for Disease Control and Prevention (2017); (b) Hospital leadership support in making nurses’ health a priority through resource allocation to ensure that nurses have duty coverage to take breaks, and through offering non-food incentives or changing the types of free foods offered; (c) Offer workplace wellness programs that are flexible and accessible to shift workers to include nutrition education and counseling offered on or near nursing units; and (d) Workplace wellness programs focused on success in the workplace as opposed to during personal time (e.g., recipes for quick, healthy meals/snacks, and sell healthy packed to-go meals 24/7).
Free food was cited as a driving influence in making unhealthy food choices, yet little research has explored this concept. Future research should explore free food in the workplace, including its prevalence, quality, and effects. The prevalence of unhealthy hospital food environments also needs to be evaluated to appreciate the gravity of the problem. Interventions that specifically target nurses’ dietary practices need to be implemented and tested. Research, in particular, on environmental interventions that address the many barriers experienced by hospital shift nurses, is needed. This study identified several predominant influences on dietary behaviors that nurses experience in the hospital setting, which should inform those interested in improving the dietary health of nurses.
Applying Research to Occupational Health Practice
This exploratory study provides an understanding of workplace influences on dietary behaviors for hospital-based RNs in the Southeast United States. Nurses face many barriers to healthy dietary practices in hospitals, particularly related to the food environment, nursing role, and shift work. The hospital food environment is predominantly unhealthy, including frequently offered free junk foods, which inhibits nurses from making healthy food choices. The nursing role is unique to other disciplines and restricts the distance and time nurses can spend away from patients. Shift work imposes various additional barriers related to physical, mental, and emotional well-being, which all impact dietary behaviors. Workplace interventions that target these barriers are needed to improve nurses’ dietary behaviors and promote health in the nursing workforce.
Supplemental Material
WHS_Supplemental_File_1_1 – Supplemental material for Hospital and Shift Work Influences on Nurses’ Dietary Behaviors: A Qualitative Study
Supplemental material, WHS_Supplemental_File_1_1 for Hospital and Shift Work Influences on Nurses’ Dietary Behaviors: A Qualitative Study by Cynthia Horton Dias and Robin M. Dawson in Workplace Health & Safety
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: C.H.D. received no financial support for the research, authorship, and/or publication of this article. R.M.D. was supported by the National Heart, Lung, and Blood Institute (NHLBI)/National Institutes of Health (NIH) (1 K23 HL133596-01A1). The views expressed in this manuscript are those of the authors and do not necessarily represent the views of the NHLBI/NIH.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
Cynthia Horton Dias is a hospital staff nurse in South Carolina and PhD Candidate and Jonas Scholar 2018–2020 at the University of South Carolina. Her research interests include workplace food environments, improving population dietary behaviors, and preventing chronic disease through diet.
Robin M. Dawson is an assistant professor and director of the Smart Start Nursing Program at the University of South Carolina. Her multi-level program of research is focused on understanding the context and processes of communication, as well as the development of practical and innovative interventions designed to facilitate optimal patient–provider communication.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.