
Abstract
Background: About 84% of the agriculture, fishing, and forestry occupational sector is comprised of farmers. This sector is at high risk for suicide in the United States. Recent disasters and trade upheavals may make farmers and their families more vulnerable to depression and suicide. This review focused on the risk for depression and suicide among United States’ primary farm operators and their families. Methods: A systematic search of the literature published between January 2000 and June 2019, using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) methodology was conducted. Results: A total of 30 articles met full inclusion criteria. Seventeen reports emanated from the midwest. Twenty studies used a cross-sectional design, primarily assessing a convenience sample or random stratified sample from a limited geographic area. We discovered only one intervention evaluation study. Depressive symptoms were assessed as part of the studies, but it was not the major focus. A variety of instruments measured depressive symptoms, with the Centers for Disease Control Epidemiologic Studies—Depression (CES-D) Scale used more frequently than other scales. Thirteen studies focused on the relationship between pesticide/chemical exposure and depression or suicide risk. Increased stress, poor physical health, compromised financial position, and previous injury were among the leading indicators of depression. Conclusion/Application to Practice: The limited number of studies that was discovered identified the need for more robust science where the risk for depression and suicide is the primary focus of the study and for intervention studies grounded in science. Occupational health providers should be vigilant about farm exposure and be aware of factors that may influence depressive symptoms of workers who operate farm establishments.
Background
America’s agricultural industry contributes 389 billion dollars to the U.S. economy (U.S. Department of Agriculture National Agricultural Statistics Service [USDA NASS], 2019a) and rests on the decisions of its 2.7 million primary producers (USDA NASS, 2019b). About 96% of U.S. farms are owned and operated as family farm enterprises (U.S. Department of Agriculture, 2019). While attention has focused on reducing physical injuries among producers, far less emphasis has been placed on their mental health. The purpose of this review was to examine the scientific literature related to depressive symptoms, depression, and suicide among primary farmers and their families in the United States. Mental health and mental disorders remain challenging in rural areas, both in terms of residents seeking help and in resources to provide that help (Gamm et al., 2003; Rural Health Information Hub, 2018; Weingarten, 2018).
Farmer suicide is not a recent manifestation, but with the rising rates of suicide in the general U.S. population across all age groups (Curtin et al., 2016), the 2016 Center for Disease Control and Injury Prevention’s report on suicide rates by occupation brought national attention to the issue (McIntosh et al., 2016; Peterson et al., 2018). According to these reports, persons working in the agriculture, forestry, and fishing (AgFF) sector exhibited one of the highest suicide rates: 44.9 and 32.2/100,000 in 2012 and 2015 compared to the general occupational rate of 17.3/100,000. About 84% of the AgFF sector is comprised of farmers (Bureau of Labor Statistics, 2017). Several state-specific reports confirmed these grim statistics using various databases. Browning et al. (2008) reported on the increased suicide during 1990 to 1998 of White male farmers in Kentucky, North Carolina, and South Carolina compared to the White male general population of those states. Similar reports were borne out by Stallones et al. (2013) in Colorado. Evidence from Georgia (Lavender et al., 2016) and national level (Ringgenberg et al., 2018; Tiesman et al., 2015) added to the robust knowledge that farmer suicide is a sustained epidemic. Ringgenberg et al. (2018) noted that the suicide rate of farmers and ranchers was 3.5 times that of the general population.
Despite the high suicide rate, the National Surveys on Drug Use and Health 2008 to 2013 reported that suicide ideation among AgFF employed workers, ages 16 to 64, was the lowest among all occupational groups at 1.3% in the past year (Han et al., 2016). How can this discrepancy between ideation report and actual suicide be rationalized? Perhaps part of the answer lies in the culture of agrarianism, where mental health still retains a social stigma (Weingarten, 2018). The values of agrarianism include achievement, group conformity, independence, fundamentalism, and keeping the family farm, all potential barriers to seeking help. In addition, the stigma associated with suicide in rural areas may lead to an underreporting of suicide (Timmermans, 2005). Ringgenberg et al. (2018) noted that suicide rates were highest in the west and lowest in the south, which coincidentally is the heart of the “Bible Belt,” where religious beliefs carry social sanctions on mental health issues and for suicide.
What leads farmers and ranchers to engage in agriculture? The agrarian imperative postulated by Rosmann (2010) claims that the drive for land acquisition and production is embedded in the genomes of the DNA and may be strengthened through generations of farming. If the farming practice is unsuccessful, the ensuing stress leads to negative health outcomes, including depression and behavioral health problems. Cole (2010) refutes the imperative, suggesting instead that it is the physical and social environments, including access to economic, cultural, and social capital that shape the outlook of the farmer. Both stances have merit. Human actions and responses are framed within internal and external contexts and are not easily parted. The debate about the agrarian imperative is but one facet of the challenges to farmers’ mental and behavioral health. There remains little progress to address the psychological health challenges that manifest among primary farmers or their families. During the Farm Crisis of the 1980s, several programs were developed (Rosmann, 2008) which delivered primary care or support, but these programs ceased or at the very best were severely underfunded, and little evaluation was done as to their success.
The bulk of the literature on farmers’ mental health focuses on migrant and seasonal farmworkers, or on farmers in other nations. While we acknowledge the importance of this work, we also note that primary farmers and their families in the United States may experience unique occupational factors that influence their mental health; yet scant research has focused on this population to address their mental health issues. The purpose of our report is to present this body of literature, identify gaps in the science, and to outline the next steps needed to decrease the epidemic of farmer suicide.
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) methodology was followed to conduct this review (Moher et al., 2009). The following criteria were established for the literature review: (a) published in 2000 to June, 2019; (b) focused on primary farmers or their family household members within the United States; (c) addressed the topic of depressive symptoms, depression, suicide, or mental health of farmers and/or their families; and (d) published in English. The review was limited to published, peer-reviewed research articles, and the article had to meet all the criteria (see Figure 1 for the systematic review process).
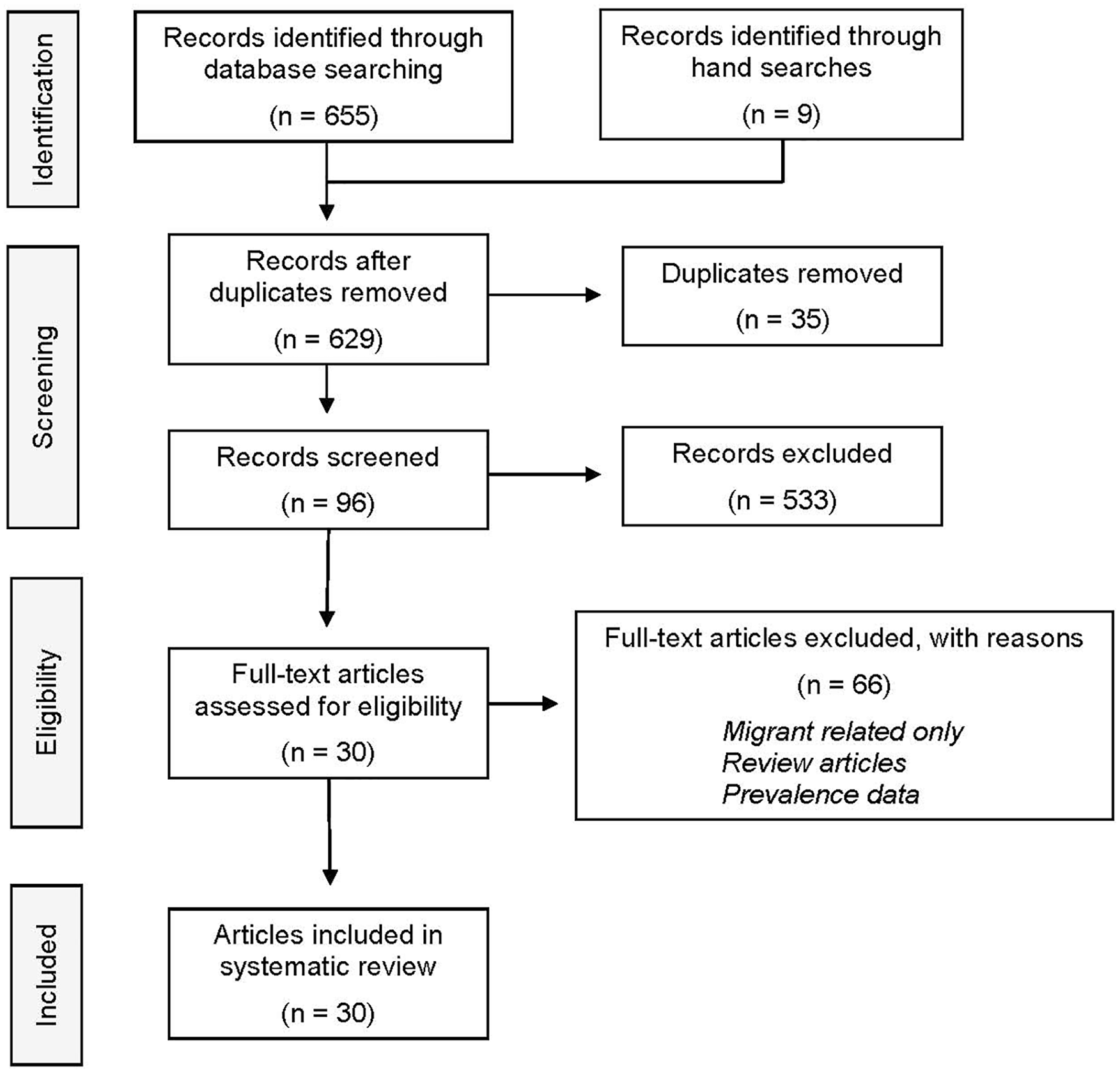
PRISMA systematic review process.
The term “primary farmer” is inclusive of various terminologies used to describe persons in charge of the farm operation. Principle farm operator, agricultural producer, farmer, and rancher are also common terms used to describe a primary farmer. For this report, any of these terms were acceptable.
Searches were conducted in PubMed, SafetyLit, and Google Scholar and the U.S. Department of Agriculture’s online access database (AGRICOLA) using keywords and/or phrases of mental health, depression, stress, and suicide among the agricultural community within the United States. Supplemental Table 1 describes the searches by keywords and phrases in the order in which the searches were implemented. Titles and abstracts/brief synopses of the identified articles were examined by both authors to determine the relevance of these results.
Searches through PubMed and SafetyLit generated 255 articles. The Google Scholar search returned more than 18,000 articles. The Google Scholar database sorts the data by relevance and lists 10 articles per page. We reviewed the first 40 pages of results (400 articles). In the first 22 pages, we found only 34 articles that possibly met our eligibility criteria. No articles relevant to our review were discovered from pages 23 to 40 and the search ceased. As a result, our initial pool of articles contained 655 articles (255 from PubMed/SafetyLit + 400 from Google Scholar). No articles were discovered from AGRICOLA.
A large proportion of the articles included studies that were conducted in other countries, did not focus on the topics of interest, or did not center on farmers or their families, resulting in 122 articles. After removing 35 duplicates, 87 articles underwent further examination. We discovered nine additional articles by hand searching two journals known to the authors to publish on agricultural health and safety issues but obscure in the aforementioned search engines, bringing the total number of articles for further consideration to 96. Reference lists from those articles were examined for additional publications, but none were identified. Following a closer review of the 96 retained articles, 66 were excluded because they focused solely on migrant workers, only mentioned prevalence estimates, or reflected review articles, leaving 30 articles meeting the eligibility requirements which are listed in Table 1.
Summary of Literature on U.S. Primary Farmer and Farm Household Residents Depressive Symptoms by Focus, Study Type, Location, Year, Sample Size, and Key Findings (n = 30)
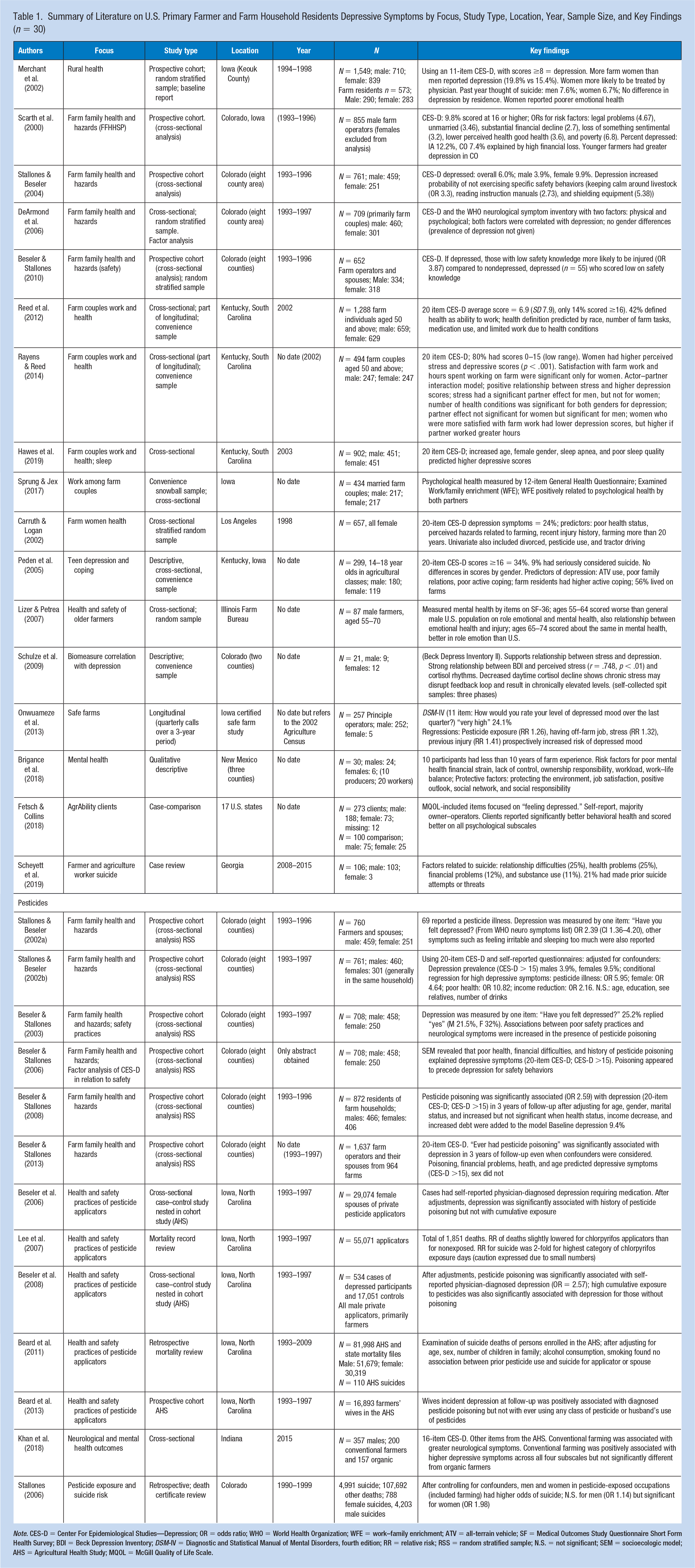
Note. CES-D = Center For Epidemiological Studies—Depression; OR = odds ratio; WHO = World Health Organization; WFE = work–family enrichment; ATV = all-terrain vehicle; SF = Medical Outcomes Study Questionnaire Short Form Health Survey; BDI = Beck Depression Inventory; DSM-IV = Diagnostic and Statistical Manual of Mental Disorders, fourth edition; RR = relative risk; RSS = random stratified sample; N.S. = not significant; SEM = socioecologic model; AHS = Agricultural Health Study; MQOL = McGill Quality of Life Scale.
Results
Among the 30 articles, the effects of the original National Institute for Occupational Safety and Health (NIOSH, 1991) funding of the Farm Family Health and Hazard Surveillance studies, funded between 1990 and 1996, were evident. Ten of the retained articles, all based in Colorado, evolved from studies funded through this research program. Eighteen of the articles resulted from three major studies. Geographically, 23 studies had a presence in the midwest, primarily Colorado and Iowa, with lesser numbers in the south and only one report from the west. No studies were discovered from the northeast United States. The biggest flurry of publications took place between 2006 and 2008, when eight articles were published, representing four distinct studies. In that time frame, six of the eight publications focused on pesticide exposures. Five studies were published between 2018 and 2019.
Study Designs and Sample Sizes
Of the 30 studies, 20 used cross-sectional data, 2 analyzed longitudinal data (Beard et al., 2013; Onwuameze et al., 2013), and 2 were case–control studies nested within a cohort panel (Beseler et al., 2006, 2008). Three retrospective review articles examined mortality and pesticide exposure (Beard et al., 2011; Lee et al., 2007; Stallones, 2006). One article relied on general death reviews (Scheyett et al., 2019). There was only one qualitative study (Brigance et al., 2018) and one case-comparison intervention evaluation study (Fetsch & Collins, 2018). It is important to point out that eight of the articles emanated from a single database in Colorado that included only eight counties. Led by Stallones and Beseler, six of these articles primarily examined associations between pesticide exposure and depressive symptoms.
Measures of Depressive Symptoms
Eight different tools were used to measure depressive symptoms. Fifteen of the studies used some form of the Centers for Disease Control Epidemiologic Studies—Depression Scale (CES-D). One study (Lizer & Petrea, 2007) used 10 items from the Medical Outcomes Study Questionnaire—Short Form 36 Health Survey (SF-36) to examine emotional and mental health. Sprung and Jex (2017) used the 12-item General Health Questionnaire, while Schulze et al. (2009) used the Beck Depression Inventory. Fetsch and Collins (2018) applied the McGill Quality of Life Scale, which includes subitems on depressive symptoms. Articles using the Agricultural Health Study (AHS) databases judged depression by a single item that asked if the participant had a physician-diagnosed depression. Onwuameze and colleagues (2013) used a single item from the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV): “How would you rate your level of depressed mood over the last quarter?” Two studies simply asked, “Have you felt depressed?” (Stallones & Beseler, 2002a) or “experienced sadness or depression” in the past year (Carruth & Logan, 2002).
Study Participants
Only four studies clearly identified the study sample as primary farmers or members of their households, but the study was retained if the implication was inherent that a substantial percentage of the sample was from primary farmers and not farm laborers. Members of the same household (usually referred to as farmer and spouse) comprised the sample for 18 of the articles, and in all but one of these (Sprung & Jex, 2017), they were part of a prospective cohort study. Just one study addressed adolescent depressive symptoms (Peden et al., 2005).
Gender Inclusion
Twenty-five of the reports included both genders in their analysis; three of the studies were heavily slanted toward male gender. Two of those involved chemical applicators, a job performed by nearly all males (Beseler et al., 2008; Lee et al., 2007); the other was a suicide chart review (Beard et al., 2011). Three samples were all female, two of which were the spouses of pesticide applicators (Beard et al., 2013; Beseler et al., 2006; Carruth & Logan, 2002). The reports of many of the studies noted that women were excluded from analyses due to small numbers or they were noted as spouses.
Suicide Ideation and Suicide
The report by Merchant and colleagues (2002) of adults in rural Iowa (1/3 of who were farm residents) noted that 7.6% of men and 6.7% of women had thought of suicide in the past year. Nine percent of adolescents (Peden et al., 2005) reported seriously considering suicide in the past year, but no difference by gender was observed. In the death chart reviews of Colorado residents, those persons in pesticide-exposed occupations (including farming) had higher odds of dying by suicide, which was significant for women (OR 1.98) but not for men (OR 1.14) (Stallones, 2006). Beard et al. (2011) found no association between pesticide exposure and suicide. A record review (Lee et al., 2007) of more than 55,000 male pesticide applicators noted a reduced relative risk (RR) for all causes of death for applicators but a two-fold risk for suicide among the highest category exposure days for one specific pesticide, chlorpyrifos. The review of farmer suicides in Georgia (Scheyett et al., 2019) noted that 21% of the deceased had made prior suicide threats.
Factors Affecting Farmers’ Depressive Symptoms and Suicide
Gender
Six studies (Beseler & Stallones, 2003; Hawes et al., 2019; Merchant et al., 2002; Rayens & Reed, 2014; Stallones & Beseler, 2002b, 2004) confirmed that women exhibited higher depressive symptoms scores compared to men in the study; no studies reported higher rates in men compared to women. Carruth and Logan (2002) noted that 24% of their all-female sample reported depression, while Scarth et al. (2000) reported a prevalence of 9.8% in their all male sample. Lizer and Petrea (2007) noted that men aged 55 to 64 scored worse than the general U.S. male population in emotional and mental health, but older participants scored about the same as the general population. Reports based on the AHS noted that only 3.0% of the male sample reported a history of diagnosed depression requiring medication (Beseler et al., 2008), compared to their wives in the study who reported a 7.1% prevalence (Beseler et al., 2006; Stallones & Beseler, 2002a). Scheyett et al. (2019) did not report depressive symptoms; however, more than 97% of their sample who died by suicide were men.
Financial decline
Financial decline was a significant risk for depressive symptoms in three reports (Beseler & Stallones, 2013; Scarth et al., 2000; Stallones & Beseler, 2002b) and showed an increasing but not significant trend in one prospective study (Beseler & Stallones, 2008). Scarth et al. (2000) noted that farmers in Iowa had a depressive symptom prevalence of 12.2% compared to Colorado residents with 7.4%. This difference was explained by the severe weather that had decimated much of the Iowa crops and thus, little income, yielding more insight into the precarious nature of farming and its effect on health. When this was taken into account, younger Colorado farmers had higher depressive symptoms scores. Brigance et al. (2018) listed financial strain as a major theme in their study of organic farmers. Financial problems were causative factors in 12% of Georgia suicide deaths (Scheyett et al., 2019).
Perceived health status
Perceived health status (PHS) was measured in several studies, usually using the National Health Interview Survey (NHIS) item: “How would you describe your health?” One study (Reed et al., 2012) examined predictors of health definition by several variables, including CES-D score. Health was defined as the ability to work by 42% of the sample. The CES-D score was not significant in predicting health definition; however, daily prescription use and the number of health conditions that limited farm work were significant predictors of higher CES-D scores, but not necessarily above the cut-off point of 15. Poor PHS was the leading predictor of depressive symptoms as reported by Stallones and Beseler (2002b) (OR 10.82) and was significant as reported by Scarth et al. (2000) (OR 6.8) and in the structural equational modeling reported by Beseler and Stallones (2006) using the CES-D score >15 cutoff. In a study on farm couples (Rayens & Reed, 2014), the number of health conditions was significant for predicting increasing CES-D scores in both the husband and spouse. Farm women (Carruth & Logan, 2002) who reported poor health also had significantly higher depressive symptoms (feelings of sadness or depression). Health problems factored heavily in suicide deaths in Georgia with 25% of the sample having physical health problems and 11% exhibiting substance abuse (Scheyett et al., 2019). Fetsch and Collins (2018) noted in their intervention evaluation that AgrAbility clients had better mental health indicators than nonclients with disabilities. AgrAbility is a program that supports farmers with any type of disability.
Previous injury
In studies that reported this factor, previous injury was found to be associated with depression (Carruth & Logan, 2002; Onwuameze et al., 2013). One descriptive study (Lizer & Petrea, 2007) reported a relationship between poor emotional health and injury among the male sample of older farmers.
Stress
Various measurements of stress were included in two articles. Among older farm couples (Rayens & Reed, 2014), women had higher perceived stress scores than their husbands. Stress influenced each person’s depressive scores; men were also influenced by their wife’s stress but not vice versa. Schulze et al. (2009) also noted a positive relationship between stress and depression for both genders. Stress was the leading indicator for depressed mood in one Iowa study (RR ≥ 3.09) (Onwuameze et al., 2013). Physical and mental stress factors were mentioned in the qualitative study (Brigance et al., 2018) in a more global sense.
Work satisfaction
Three studies enrolled farm couples and examined a variety of variables. Rayens and Reed (2014) reported that women’s symptoms were predicted by their level of farm work satisfaction and their own hours of working on the farm but inversely related to hours worked by their spouse. Farm work satisfaction did not play a significant role in predicting their husband’s depressive symptoms. In a related study, Reed et al. (2012) noted that 14% of their sample had a CES-D score greater than 15 and that was related to decreased farm work satisfaction. Sprung and Jex (2017) provided insight into the complexities of work satisfaction, work conflict, and work–family enrichment (WFE). WFE was positively related to both the husband’s and wife’s psychological health. Wife’s farm satisfaction was positively related to her own psychological health and that of her husband. Brigance et al. (2018) reported that organic farmers found their sense of environmental responsibility, pride in their work, and their job satisfaction were protective factors for their mental health.
Safety knowledge and behavior
Three publications from the Colorado FFHHSP (Farm Family Health and Hazard Surveillance Project) reported on the association between depression and safety knowledge or safety behavior. Stallones and Beseler (2004) reported that depression inhibited three specific safety behaviors, while a follow-up publication (Beseler & Stallones, 2010) noted that depressed farmers with low safety knowledge were more likely to be injured than compared to those without depression and low safety knowledge; while Beseler and Stallones (2003) reported positive associations between some poor safety practices, neurological symptoms, and depression.
Other factors
Other factors mentioned in the studies that were associated with depression included loss of something sentimental (Scarth et al., 2000), legal problems (Scarth et al., 2000), having an off-farm job (Onwuameze et al., 2013), perceived hazards related to farming (Carruth & Logan, 2002), farming more than 20 years (Carruth & Logan, 2002), tractor driving (Carruth & Logan, 2002), and neurological symptoms; that is, feeling irritable and sleeping too much (Khan et al., 2018; Stallones & Beseler, 2002a). Sleep apnea, poor quality of sleep, and increased body mass index (BMI) were associated with increased CES-D scores among men and women (Hawes et al., 2019). Among adolescents (Peden et al., 2005), all-terrain vehicle (ATV) use, poor family relations, and poor active coping were associated with higher depressive symptoms scores. Lack of external control was noted by Brigance et al. (2018) as a risk for poorer mental health.
Pesticides, depression, and suicide
Thirteen reports focused primarily on the association of pesticide use and depressive outcomes or suicide associated with pesticide exposure, of which six were from FFHHSP and five from the National Agriculture Health Study. Khan et al. (2018) focused on the neurological and mental health differences between male organic and conventional farmers with the underlying premise that organic farmers may have less exposure to pesticides and chemicals. That study did support significant differences in total, sensory, and behavioral outcomes and positive, but nonsignificant findings with all subscales of depressive symptoms. The other (Stallones, 2006) was a death certificate review of suicides in Colorado, which noted higher odds for suicide in pesticide-exposed occupations, including farming.
Reports from the Colorado FFHHSP study generally supported the association between pesticide poisoning, pesticide illness, and depression. Stallones and Beseler (2002a) noted that persons with a history of pesticide illness had increased risks of depression (odds ratio [OR] = 2.39) and increased irritability and excessive sleep in 3 years of follow-up. A follow-up report (Beseler & Stallones, 2003) discovered that 25% of the respondents affirmed depression, and positive associations between negative safety practices and neurological symptoms were increased in the presence of pesticide poisoning. Using the CES-D in that same cohort the OR for depressive symptoms was 5.87 for those with a history of pesticide illness, after adjusting for confounders (Stallones & Beseler, 2002b). A factor analysis of the CES-D in relation to safety (Beseler & Stallones, 2006) noted the role of pesticide poisoning in decreased attention to safety. Other significant factors were poor health and financial difficulties. A similar publication (Beseler & Stallones, 2013) that followed the same cohort for 3 years found an association between pesticide poisoning and depression that carried across time. Additional factors were negative finances, poor health, and increasing age, while other demographic factors were not associated with depression.
One study (Lee et al., 2007) focused on mortality of pesticide operators in the Agriculture Health Study who applied chlorpyrifos noting a significantly increased RR for suicide in the highest category of exposure days only, and particularly for small farmer operators within that category. Caution was advised due to small numbers of deaths analyzed. On the contrary, the risk for suicide among the overall study group was less than for the general population for those states.
Two publications (Beseler et al., 2006, 2008) used a nested case–control approach to examine depression among pesticide applicators enrolled in the AHS and their spouses. Among the applicators (nearly all male), a history of pesticide poisoning was significantly associated with depression, as was high cumulative exposure to pesticides. Among spouses (Beseler et al., 2006), depression was only associated with a history of pesticide poisoning. The strength of these studies is their robust sample size and continued surveillance. Finally, a review of suicide deaths from the AHS cohort (Beard et al., 2011) was compared to state mortality files for Iowa and North Carolina. After adjusting for a myriad of factors, no association was found between pesticide use and suicide for applicators or spouses.
Discussion
Where does this leave us? We know that suicide has reached epidemic proportions among farmers, yet little has been done to address the issue. This report highlights the paucity of attention to factor identification or the chain of events that results in depression and even to the deadly sequel of suicide. Despite the increasing evidence that U.S. farmers suffer disproportionate shares of depression and suicide, we found only these 30 reports that examined the risks for depressive symptoms and suicide among primary farmers or their families. More troubling is that 18 of these reports were based on only three research studies. The leading indicators of depressive symptoms seem to be the association with pesticide illness or pesticide poisoning, increased stress of any type, poor physical health, financial position, and previous injury.
In the general public, women are more likely to report being depressed than men (National Institute of Mental Health, 2017), and this was supported in our review. Only three studies in this review focused solely on women, and these were not necessarily primary farmers. In two of the studies, they were referred to only as spouses. This exclusion of women continues to be a challenge in agricultural health research despite the increasing numbers of women in agriculture and is troubling, given the growing numbers of suicides among adolescents, in particular, adolescent girls (Curtin et al., 2016). Women are entering farming as an occupation much more than in previous history, yet none of the reviewed articles focused on women as primary operators. Female farmers may have different risk factors for depression than their male counterparts (National Institute of Mental Health, 2017).
Measurement of depressive symptoms varied across studies making it difficult to compare them. This is not unique to this body of literature; however, it begs the question of the best way to measure such a sensitive topic, particularly using self-report. Depressive symptoms were not the primary focus of any of the studies reviewed but was embedded within a larger context, thus the depth of the examination was limited. Across the studies, depressive symptoms were measured from a single item to the more extensive 20-item CES-D Scale. Regardless of which instrument was used, it was evident that depressive symptoms or the self-report of “feeling depressed” was generally greater for farm residents than for comparison groups. Even the admission of “feeling depressed” runs counter to the literature that supports the stoic nature and reticence of rural populations to admit these feelings (Fraser et al., 2005; Rosmann, 2010). It seems almost a cry for help fixed within an anonymous or confidential questionnaire.
In times of farm economic disaster, such as in the 1980s, more attention was focused on supporting the agricultural population, but as economic recovery began, programs were defunded or scaled back. It is important to note that the research reviewed in this article was grounded in the 1990s and later, a time of relative prosperity in agriculture (Dimitri et al., 2005). Even so, the levels of depressive symptoms were high and the suicides did not subside but increased. Research has provided the evidence to reduce injury and unintentional death in production agriculture. Deaths involving tractors have plummeted, and children on farmsteads die in much fewer numbers since the Surgeon General’s 1989 call for improved agricultural health and safety and the robust program of research that ensued (Myers & Hendricks, 2010; National Children’s Center for Agricultural Health and Safety, 2017). Yet, suicide, a preventable death, is more than three times greater among farmers than the general public (Ringgenberg et al., 2018), a silent epidemic that is under-researched. The alarming rate of farmer suicide will only be stymied by interventions grounded in evidence-based practice guided by rigorous research.
The focus of this review was on research that can serve as the foundation for intervention trials. In the examination of the literature, we did find some evidence of programs to improve the mental/behavioral health of farmers, but most of these (like Rosmann’s project, Sowing Seeds of Hope (American Farm Bureau, 2009) ceased to exist after the major farm crisis in the 1980s or have not been evaluated for efficacy or effectiveness. One program (Dickens et al., 2014) reported on a promising intervention to reduce stress among Vermont dairy farmers, but the authors cautioned that their commentary merely pointed to the need for such interventions. That need continues and is even more critical today. The findings reported by Fetsch and Collins (2018) included in our review noted the improvement in quality of life and depressive indicators for farmers with disabilities who participated in the AgrAbility program. More studies like this can provide the needed evidence for interventions with larger farm populations that can improve their mental health.
The recent Farm Bill (Congressional Research Service, 2019) included language to address the continuing and mounting problem of mental health among rural and farm populations with a 10 million dollar budget to address this growing epidemic. Regional farm and ranch stress assistance networks are expected to be funded in the late 2019. These will include 24/7 phone hotlines and other resources to support farmers through their mental health struggles. Recent articles in the national popular press (Weingarten, 2018, 2019; Weingarten & Mulkern, 2017) have illuminated this problem for the entire nation to see, far beyond the fields of agricultural production. Hopefully, this attention will spur research focused on both the epidemiology of the problem and on interventions that may prevent or alleviate distress among our agricultural population. The Farm Bill budget is a first step but sustained funding for programs that are evidence based is crucial for positive outcomes among this highly vulnerable occupational group.
Limitations
The literature on this topic may be scattered across many disciplines. We searched the primary databases and enlarged our search by reviewing reference lists at the end of articles and by hand searching the table of contents of two journals known to publish much of the NIOSH-funded research. There may be other reports buried among more obscure journals or releases. Another major limitation is the definition of farmer. Primary farmer or primary farm operator are terms now used by the U.S. Census of Agriculture; however, the term “farmer” is much broader in the literature. We addressed this by reading each article thoroughly to decide if the report included respondents other than primary farmers or their immediate households. Also troubling is that reports on the AgFF occupational sector usually consolidate all three subsectors, making it difficult to gain a concise understanding of agriculture. The reality is that there is no perfect database for presenting the picture of farmers’ mental health and the outcomes of the myriad of factors that influence farmers’ stress, depressive symptoms, and the worst outcome of suicide.
Implications for Occupational Health Practice
Farming may not seem pertinent to occupational health nurses (OHNs) in most settings, but the reality is that more than half of the nation’s farmers also hold an off-farm job (USDA NASS, 2019b). Spouses of farmers also hold off-farm jobs. OHNs, particularly those in rural areas, should be cognizant of the mental health of farm families and ready to intervene in culturally appropriate ways. OHNs should also engage with primary care providers to better understand the total health of the farmers. Many places of employment now provide total health care on-site. Working together as a team will enhance the overall well-being of the farmers and their families. As new programs evolve from federal funding, OHNs can bolster their resources using the new tools that will be made available from these programs. OHNs can also offer suicide risk detection education in the workplace, so everyone in the workplace is better equipped to recognize risk and make appropriate referrals.
The first step in providing care for the farm and farm family is by knowing who among your clients is a member of a farm family. Becoming familiar with local agricultural commodities and local stressors that farmers face can underpin counseling and interventions such as farm appreciation day in the workplace, or working with human resources to provide flexible hours during period of planting or harvesting. Engaging in continuing education on mental health of farmers will provide the OHN with the knowledge to provide culturally appropriate care to this vulnerable population of workers.
Conclusion
Scant research on farmer depressive symptoms and suicide in the United States has been conducted. This review of the literature exposed gaps in the science that must be addressed, so effective interventions can be developed to help farmers, and their families cope with the unique occupational hazards to their mental health. OHNs should be at the forefront of the research and delivery of interventions to assist our farm population.
In Summary
Persons engaged in farming should be screened for depressive symptoms.
Women in farm households are at greater risk for depression than men.
Financial stress in farming is associated with increased depression and suicide.
Pesticide exposure and application may increase depressive symptoms.
Supplemental Material
Supplemental_Table_1 – Supplemental material for Risk for Depressive Symptoms and Suicide Among U.S. Primary Farmers and Family Members: A Systematic Literature Review
Supplemental material, Supplemental_Table_1 for Risk for Depressive Symptoms and Suicide Among U.S. Primary Farmers and Family Members: A Systematic Literature Review by Deborah B. Reed and Deborah T. Claunch in Workplace Health & Safety
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material is available online for this article.
Author Biographies
Deborah B. Reed holds the Good Samaritan Chair in Community Health Nursing. She is Professor Emeritus in the U.K. College of Nursing and is Kentucky’s agricultural health nurse in the U.K. College of Agriculture, Food, and Environment. She is the content expert and led the development of the manuscript.
Deborah T. Claunch has served as a research associate in the U.K. College of Nursing. She has functioned as project manager for five of Dr. Reed’s studies and collaborated with Dr. Reed in publications and presentations on research findings at state, national, and international conferences. She conducted the database searches and contributed to writing the manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.