
Abstract
Background: Managing the safety climate in health care is a promising tool for improving employee and patient safety in the health care work environment. Gaps in the theoretical and conceptual underpinnings of safety climate, as well as the evidence base for its practical application in health care remain. The purpose of this study was to evaluate the number of work injuries occurring in health care work units and associated safety climate beliefs. Methods: A retrospective analysis was conducted utilizing organizational staff survey data collected by a large medical hospital in the Midwest in 2015. Employees (n = 32,327) were invited to identify safety climate perceptions via survey. Injuries, days restricted, and days absent were identified through the Hospital’s Occupational Safety and Health Administration (OSHA) log. Zero inflated negative binomial regressions used injuries as dependent variables and safety climate perceptions as independent variables. Findings: In all, 23,599 employees completed the survey (73% response rate) across 1,805 employee work units which were defined as groupings of employees reporting to a single supervisor. We found that there was an association between fewer injuries and health care workers indicating that they share responsibility for compliance with safety rules and procedures (relative risk [RR] = 0.98, 95% confidence interval [CI] = [0.98, 0.99]). Conclusion/Application to Practice: This study supports the use of a safety climate measure to assess working units’ perceptions of employee safety. A continued focus on the health and safety of employees who interact directly with patients is warranted, as well as employees who do not provide direct patient care.
Health Care Worker Perception and Injury
According to the International Labor Organization (ILO), an estimated 2.7 million people die every year from work-related injuries and diseases, and the burden of poor workplace safety causes an estimated loss of 4% of the world’s annual gross domestic product (GDP; ILO, 2018). More than three decades ago, the concept of “safety climate” was introduced as a principal consideration in creating and maintaining safe work environments, and is defined as “shared employee perceptions of the priority of safety . . . at their organization” (Zohar, 1980, p. 96), or as “a snapshot of the prevailing state of safety in the organization at a discrete point in time” (Huang, Ho, Smith, & Chen, 2006, p. 425). This concept has proven useful in defining and improving workplace safety behaviors and injuries across multiple industries (Amponsah-Tawiah & Mensah, 2016; Beus, Payne, Bergman, & Arthur, 2010).
Health care workers continue to experience one of the highest number of nonfatal workplace injuries (Bureau of Labor Statistics, 2019; Dressner, 2017). Health care workers face a broad range of risks including: blood-borne pathogens, workplace violence, exposures to chemicals and hazardous drugs, physical demands, latex and other allergens, infectious diseases, and shiftwork, to name a few (Dressner, 2017). Previous work by Yassi and colleagues suggests a positive association between improved health and safety of health care workers and patient safety when utilizing a comprehensive approach to safety climate (Yassi, Lockhart, Buxton, & McDonald, 2010). Organizational policies, practices, and managerial customs help create a climate that can enable active, as well as latent errors that predispose to the occurrence of employee injuries, and accordingly to suboptimal patient care (Beus et al., 2010; Cheyne, Cox, Oliver, & Tomás, 1998; Christian, Bradley, Wallace, & Burke, 2009; Colla, Bracken, Kinney, & Weeks, 2005; Cook, Slade, Cantley, & Sakr, 2016). In this context, an assessment of the employee safety climate at the work unit level is a useful step toward improving both employee and patient safety.
Conceptual Framework
Studies suggest a connection between employees’ perceptions of organizational safety climate factors and the occurrence of employee injuries (Amponsah-Tawiah & Mensah, 2016; Gyekye, 2005; John & Anthony, 2001; O’Toole, 2002). Beus and colleagues (2010) found that perceived management commitment to workplace safety is an important determinant of workplace injury prevention. Kiani and Khodabakhsh (2014) noted that supervisors are seen as one of the key elements in health and safety management at the workplace in ensuring safety compliance and preventing worker injuries. In addition, Yule, Flin, and Murdy (2006) demonstrated that employees conformed to safety rules and procedures when they perceived that the action of their supervisor were fair and consistent with organization safety policies. In addition, previous inquiry demonstrated that employees’ perceptions of the work safety systems were strongly associated with job injuries (Christian et al., 2009). For example, Hoffmann and colleagues (2013) noted that employees had a more positive perception of their work safety climate when participation and responsibility involved the entire practice team, and a team perception of safety was found to be a consistent variable predicting a positive safety climate.
The literature supports the importance of safety climate, yet there remains an ongoing debate in the literature concerning the relative importance of factors characterizing positive safety climates (Halligan & Zecevic, 2011). Most authors agree that management and coworker commitment to safety practices are two factors that are critical to the employee safety experience (Christian et al., 2009; Cook et al., 2016; Hayes, Perandan, Smecko, & Trask, 1998; Huang et al., 2006; Sawhney & Cigularov, 2019). Our current study focused on these two factors of safety climate and their possible association with work-related injuries and subsequent injury outcomes. Those who are injured can return to work immediately with little to no change in their work duties, be restricted in the work duties they can perform, or lose time from work for a period of time due to inability to perform work-related tasks. Therefore, while the primary focus of this research was to evaluate the number of injuries occurring in different units, and the associated safety climate beliefs, it is an important next step to evaluate the number of days restricted and absent experienced in a work unit and to determine if safety climate perceptions are likewise associated. Findings may have potential application to occupational health nursing practice by guiding efforts to promote worker safety and realizing organizational cost-savings through reduction in injury-related loss of employee productivity (Sokas et al., 2013).
We hypothesized that greater perceived personal responsibility was associated with a reduction in injuries, days restricted and days absent. More specifically, that work units which rated unit members’ personal responsibility for complying with employee safety rules and procedures more positively experienced a lower number of employee injuries compared with units rating unit members’ personal responsibility lower. In addition, that work units which rated unit members’ personal responsibility for complying with employee safety rules and procedures experienced a lower number of employee days restricted from work, as well as days absent, compared with units rating unit members’ personal responsibility lower. In addition, we hypothesize that work units which rated their supervisor’s response to employee safety concerns more positively would experience a lower number of employee injuries, restricted and lost work days compared with units rating their supervisor less positively.
Methods
Data Sources
This was a retrospective analysis that utilized organizational staff survey data collected by a large medical hospital in the Midwest in 2015. The hospital had three facilities, direct and non-direct patient care units that employed more than 32,000 employees. The survey was electronically administered to all (32,327) of the hospital’s employees for purposes of learning their perceptions and satisfaction of their work environment. Due to human resource restrictions, characteristics of employees were only available per work unit level. This retrospective research study was approved by the Mayo Clinic Institutional Review Board (Rochester, MN).
Covariates
Data provided from the hospital system’s Human Resources department for unit characteristics included work unit, employees’ average age, gender, total number of employees, and average length of service for employees and supervisors. In addition, work units were classified based upon a review of employee job titles, job tasks and functions as providing direct patient care, or no direct care (e.g., those who work in finance or office space).
Safety Climate
Safety climate was measured using two items developed by a management consultant company used by the study hospital (Mercer, 2019) and included the following: “My immediate supervisor responds as quickly as possible when employee safety problems are discovered,” and “Where I work, everyone takes personal responsibility for complying with employee safety rules and procedures.” For both measures, the response was scored on a 5 point Likert-type scale, where 1 = complete disagreement, 2 = disagreement, 3 = neither disagree or agree, 4 = agreement and 5 = complete agreement to the question. For both questions, we created dichotomous variables that combined 1 to 3 for no agreement and 4 to 5 for agreement. At the work unit level, these dichotomous variables provide an indication as to the percentage of the work unit that agrees with each statement.
Injury Reports
Using Occupational Safety and Health Administration (OSHA) log recordability injury criteria, information was gathered about employee injuries, illnesses, days missed from work, and days restricted to other duties (OSHA, 2019). We created outcome variables of injury counts, days absent, and days restricted by summing the number of injuries, days absent and days restricted reported for each work unit. We created continuous count variables for total number of injury, days restricted and days absent, as well as categorical variables of injury (zero injuries, one injury, or more than one injury), restricted (0 days absent, 1 to median days absent, and median plus 1 day absent) and absent (0 days restricted, 1 to median days restricted, and median plus 1 day restricted).
Data Analysis
For this study, the unit of analysis was the work unit which was categorized as direct patient care or non-direct patient care. Characteristics of the work unit, safety climate responses and injuries, restricted days and days absent were analyzed using mean and standard deviations for continuous variables and frequencies and percentages for categorical or binary variables. The primary dependent variable was the number or counts of injuries each unit experienced. Secondarily, we reviewed the number of days absent and the number of days restricted occurring within the work unit. Descriptive associations were examined using ANOVA and Kruskal Wallis to compare groups based upon the number of injuries, days absent, and days restricted identified. For multivariate analysis, we used statistical analysis appropriate for count data based on our continuous data for number of injuries, number of days absent and number of days restricted. Each of our outcome variables demonstrated overdispersion and required the use of negative binomial regression, which corrected for excess variability in count data (Long & Freese, 2006). In addition, each of the variables contained a large percentage of zero counts requiring zero inflation correction (Alfò & Maruotti, 2010; Goetzel et al., 2010; Spaulding, Zhao, & Haley, 2014). As a result, we utilized three separate zero-inflated negative binomial models to model the dependent variables of interest: (a) number of injuries, (b) number of days restricted, and (c) number of days absent. Zero-inflated negative binomial models provide the ability to assess overdispersed count data that also has too many zeros to fit a normal negative binomial distribution assumption (Long & Freese, 2006). As such the model contains two parts which allow for the data to be assessed in two groups allowing for model assumptions to be met and the full extent of the data to be used (Alfò & Maruotti, 2010). The first part of the model consisted of a negative binomial regression that assessed the count information while excluding zero counts. Associated risk estimates were expressed as a relative risk (RR) and 95% confidence intervals (CIs). The second part of the model assessed the odds of not experiencing any injuries (0) versus experiencing one or more injuries (1), which were expressed as odds ratios (ORs) and 95% CIs. To account for varying numbers of employees in work units, as well as the increased opportunities for injuries, days absent or days restricted to occur due to this work unit size difference, we used the number of employees in the work unit as the offset term in all models. As this analysis occurred at the unit level, variables were assessed for multicollinearity. Based on this evaluation, employee age, and length of service were identified as highly correlated by bivariate correlation analysis, as well as variance inflation factor scores; therefore, to reduce bias from multicollinearity, age was not included to the model. All statistical analyses were performed using SAS Version 9.4 (SAS Institute Inc.).
Findings
Table 1 contains the working unit characteristics included in this analysis. A total of 23,599 employees, across 1,805 work units completed the survey with a response rate of 73%. Direct patient care units compared with non-direct patient care units had a greater mean number of employees (22.88 vs. 13.97), were more largely made up of females (73% vs. 65%), were younger (mean of 43.78 vs. 46.30), had a larger average supervisor length of service (mean of 19.51 vs. 17.36 years).
Work Unit Characteristics, Safety Climate Responses, Injuries, Days Restricted, Days Absent by Direct Patient Care Work Unit Responsibility (N = 1,805)
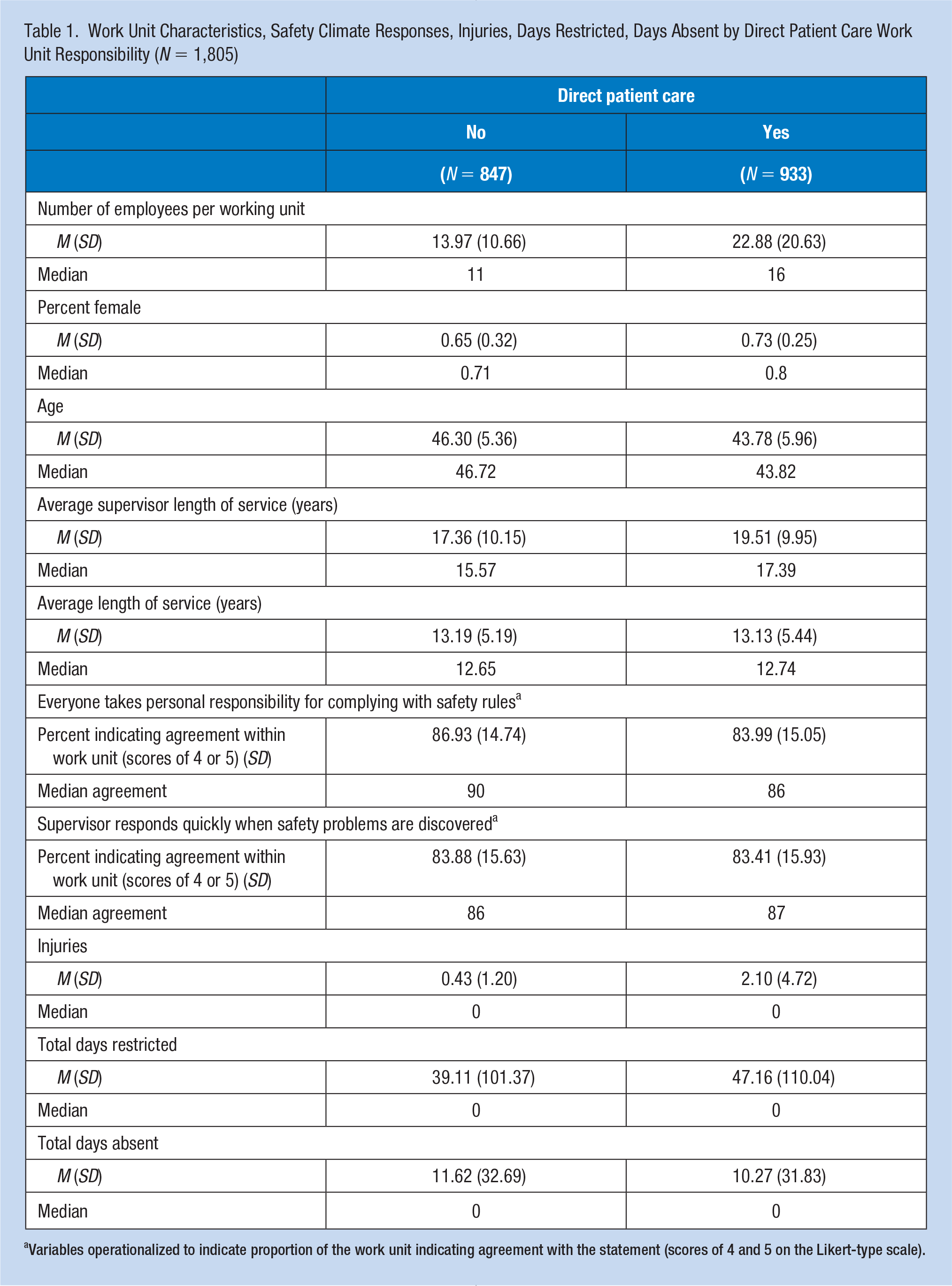
Variables operationalized to indicate proportion of the work unit indicating agreement with the statement (scores of 4 and 5 on the Likert-type scale).
Direct patient care units had a lower percent agreement score (i.e., the percent of individuals within the work unit endorsing agreements scores of 4 or 5) associated with the question “Everyone takes personal responsibility for complying with safety rules” compared with non-direct care units (83.99% vs. 86.93% agreement). However, there was little difference in scores associated with the question “My supervisor responds quickly when safety problems are discovered” (83.41% vs. 83.88% agreement). In addition, direct patient care units had a higher mean number of injuries (2.10 vs. 0.43), total days restricted (47.16 vs. 39.11), and a lower number of days absent during the study period (mean of 10.27 vs. 11.62).
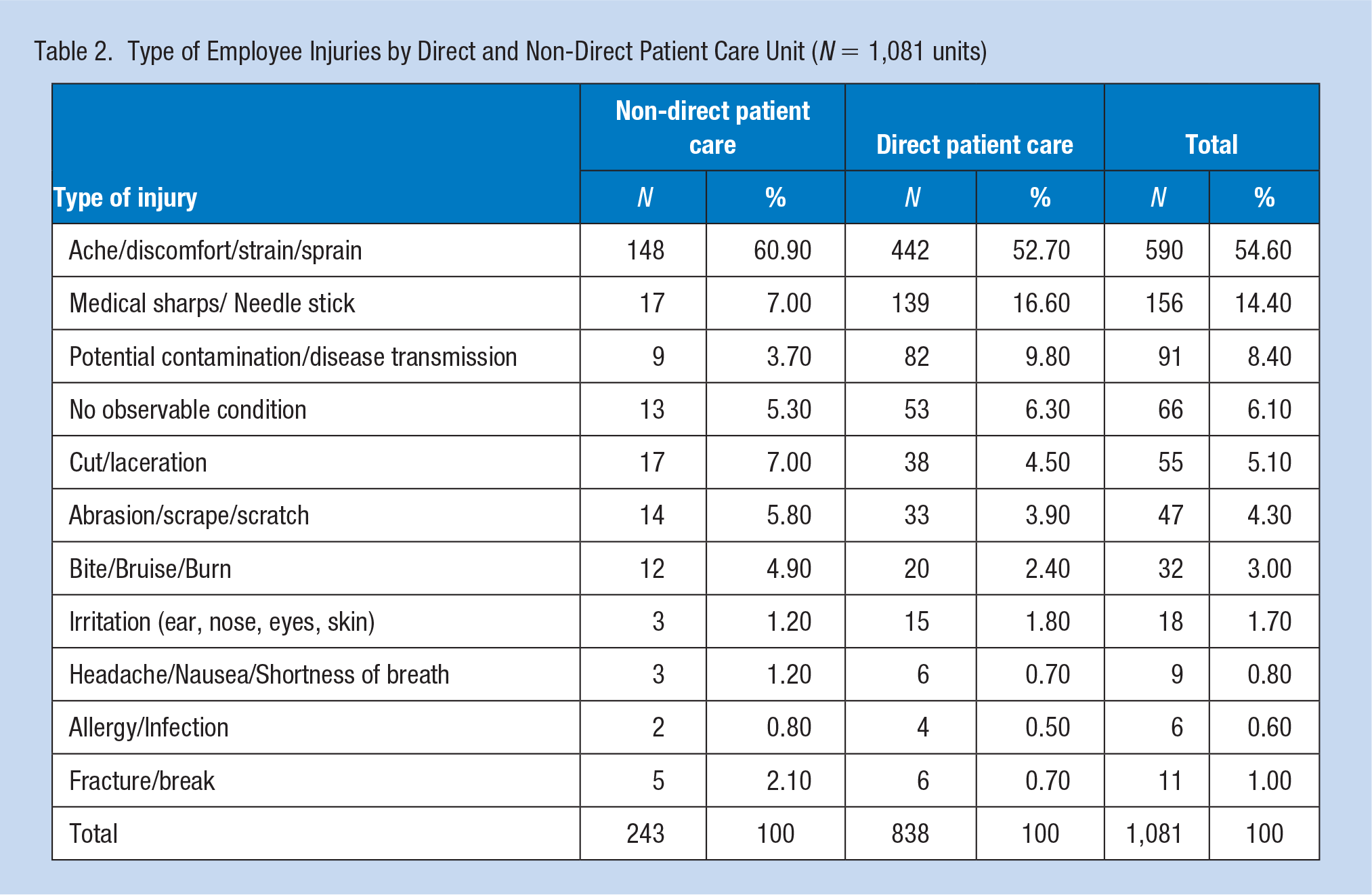
Table 2 describes the types of injuries and illnesses experienced by the employees. Injuries resulting in aches, discomfort, strain, and sprain were the most common reported injuries in both non-direct patient care units (60.9%), and direct patient care units (52.7%). For both groups, sharps and needle stick injuries (14.4%) were the second most common injury, however, direct patient care units experienced 16.6% of all injuries as needle sticks or medical sharp injuries, whereas only 7% of the injuries in non-direct patient care units (e.g., laboratory, custodial) were from needles or sharps. Direct patient care employees experienced 9.8% or more than twice as many potential contamination/disease transmission occurrences as non-direct patient care staff at 3.7%. Less frequent, but together totaling 28.3% of the injuries for non-direct patient care staff and 20.8% for direct patient care employees were other types of injuries including cuts/lacerations, abrasions/scrapes/scratches, bites/bruises/burns, and symptoms such as headache/nausea/shortness of breath, allergy and infection, as well as fractures/breaks.
Type of Employee Injuries by Direct and Non-Direct Patient Care Unit (N = 1,081 units)
As seen in Table 3, 56.1% of units providing direct patient care did not have any employee injury, whereas 49.4% had no days absent and 50.0% had no days restricted. On average, units more likely to report no injuries had a greater positive perception of the supervisory response (84.6% with no injury, 83.5% with one injury, and 79.4% with more than one injury), as well as greater perception of responsibility for everyone complying with safety rules (87.7% with zero injuries, 83.7% with one injury, and 77.5% with more than one injury). Similarly, units with no days absent also had a greater positive perception of the supervisory response (84.0 with no days absent, 79.1 with 1-17 days, and 78.0 with 18 or more days absent), as well as a greater perception of responsibility for complying with safety rules (86.0 with no days absent, 79.6 with 1-17, and 75.4 with 18 or more days absent). Finally, the same pattern emerges when considering days restricted. Units with no days restricted had a greater positive perception of the supervisory response (83.9 with no days restricted, 78.5 with 1-92 days, and 80.8 with 92 or more days restricted), as well as a greater positive perception of responsibility for complying with safety rules (86.1 with no days restricted, 78.5 with 1-92 days, and 78.3 with 93 or more days restricted).
Working Unit Characteristics and Safety Climate Perceptions by Number of Injuries, Days Absent, and Days Restricted (N = 1,805 units)
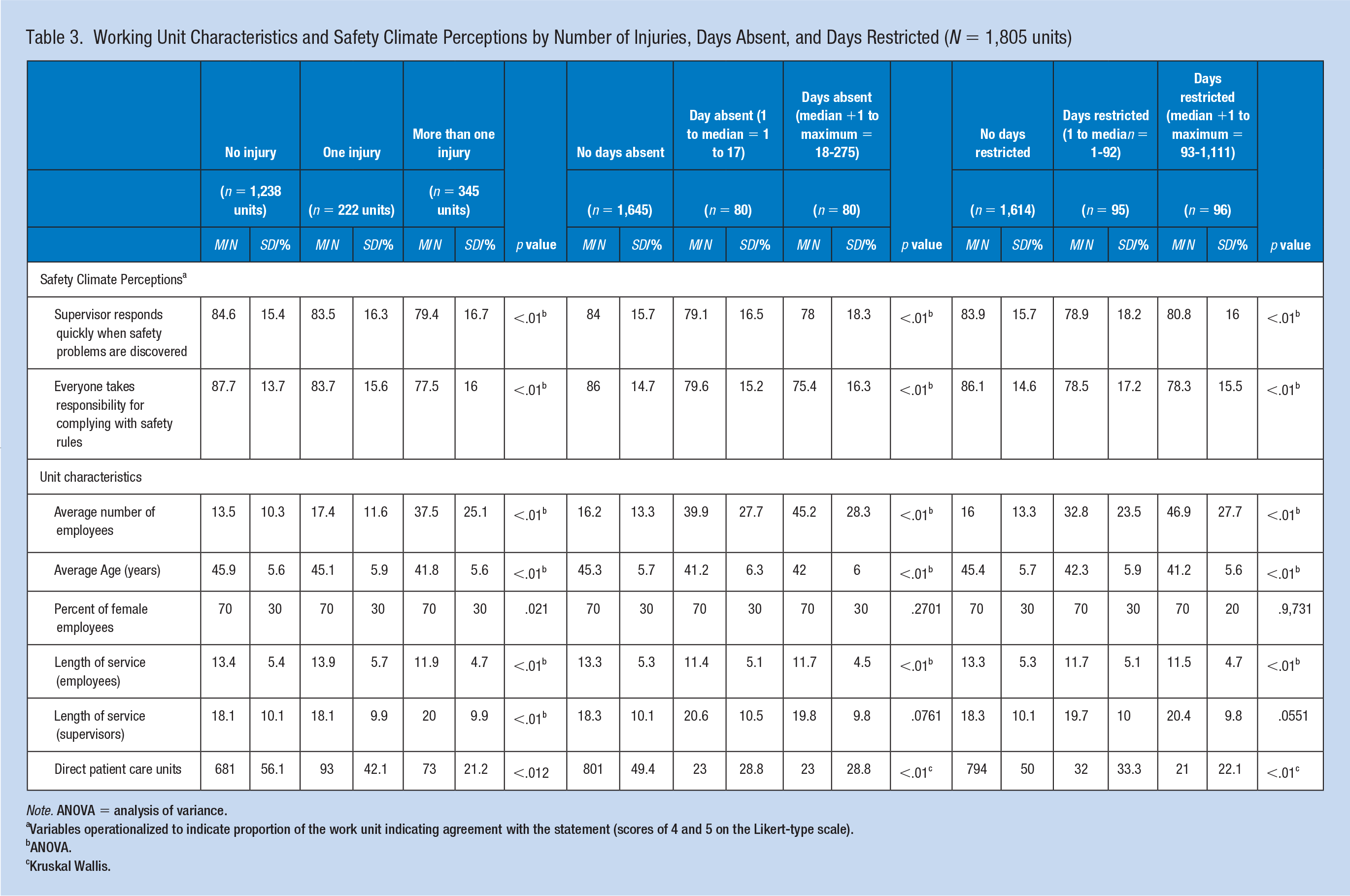
Note. ANOVA = analysis of variance.
Variables operationalized to indicate proportion of the work unit indicating agreement with the statement (scores of 4 and 5 on the Likert-type scale).
ANOVA.
Kruskal Wallis.
In Table 4, results of the multivariable analysis predicting number of injuries showed that after adjustment for differences in unit characteristics, units who perceived positive indications regarding everyone taking responsibility for complying with safety rules and procedures had lower risk of employee injuries RR = 0.98 (95% CI = [0.98, 0.99]) and higher odds of being in the certain zero (no injury) group OR = 1.06 (95% CI = [1.03, 1.09]) per unit change. In contrast, there was no significant difference of injuries observed among units that positively perceived prompt supervisor response to safety concerns RR = 1.00 (95% CI = [0.99, 1.00]) and OR = 0.99 (95% CI = [0.97, 1.01]), indicating a rejection for our hypothesis that perceived supervisors’ response to safety concerns is associated with a lower number of employee injuries.
Zero Inflated Negative Binomial Analysis of the Association Between Safety Climate Perceptions and Injuries
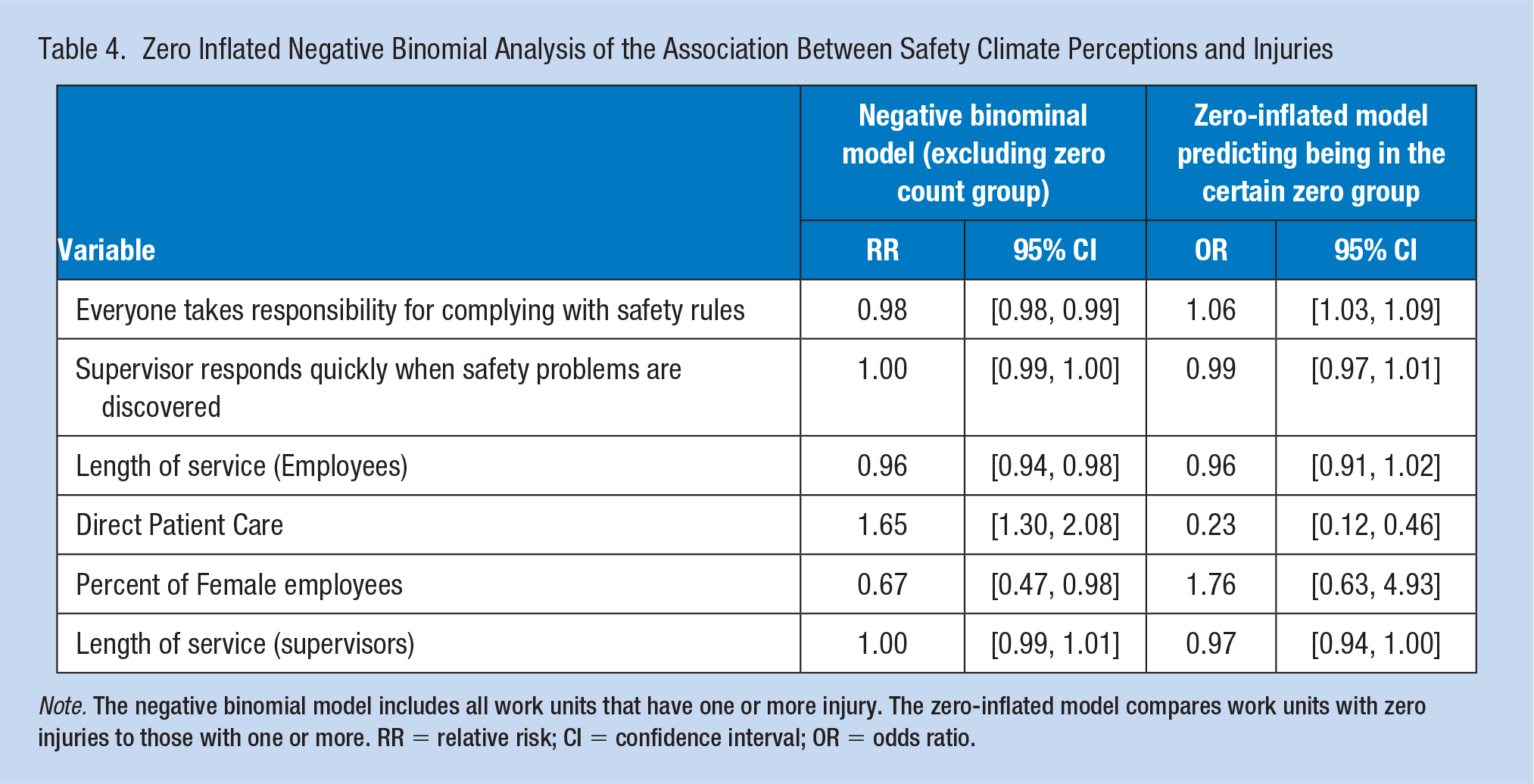
Note. The negative binomial model includes all work units that have one or more injury. The zero-inflated model compares work units with zero injuries to those with one or more. RR = relative risk; CI = confidence interval; OR = odds ratio.
We also observed that employees with greater length of service were at reduced risk of experiencing an injury (RR = 0.96; 95% CI = [0.94, 0.98]). Employees with direct patient care responsibilities had an increased risk (RR = 1.65; 95% CI = [1.30, 2.08]) compared with non-direct patient care employees, and had reduced odds of being in the certain zero (no injury) group OR = 0.23 (95% CI = [0.12, 0.46]).
The results of the multivariable models predicting days absent and restricted (Table 5) showed that units who perceived positive indications regarding everyone taking responsibility for complying with safety rules and procedures had higher odds of being in the certain zero group, that is, those who had no days absent OR = 1.04 (95% CI = [1.02, 1.06]) or no days restricted group OR = 1.03 (95% CI = [1.02, 1.04]). In contrast, there was no significant difference of injuries observed among units that positively perceived prompt supervisor response to safety concerns for days absent RR = 1.00 (95% CI = [0.98, 1.01]) and OR = 1.01 (95% CI = [0.99, 1.02]) nor days restricted RR = 1.00 (95% CI = [0.99, 1.01]) and OR = 1.00 (95% CI = [0.99, 1.01]).
Zero Inflated Negative Binomial Analysis of the Association Between Safety Climate Perceptions and Days Absent and Restricted
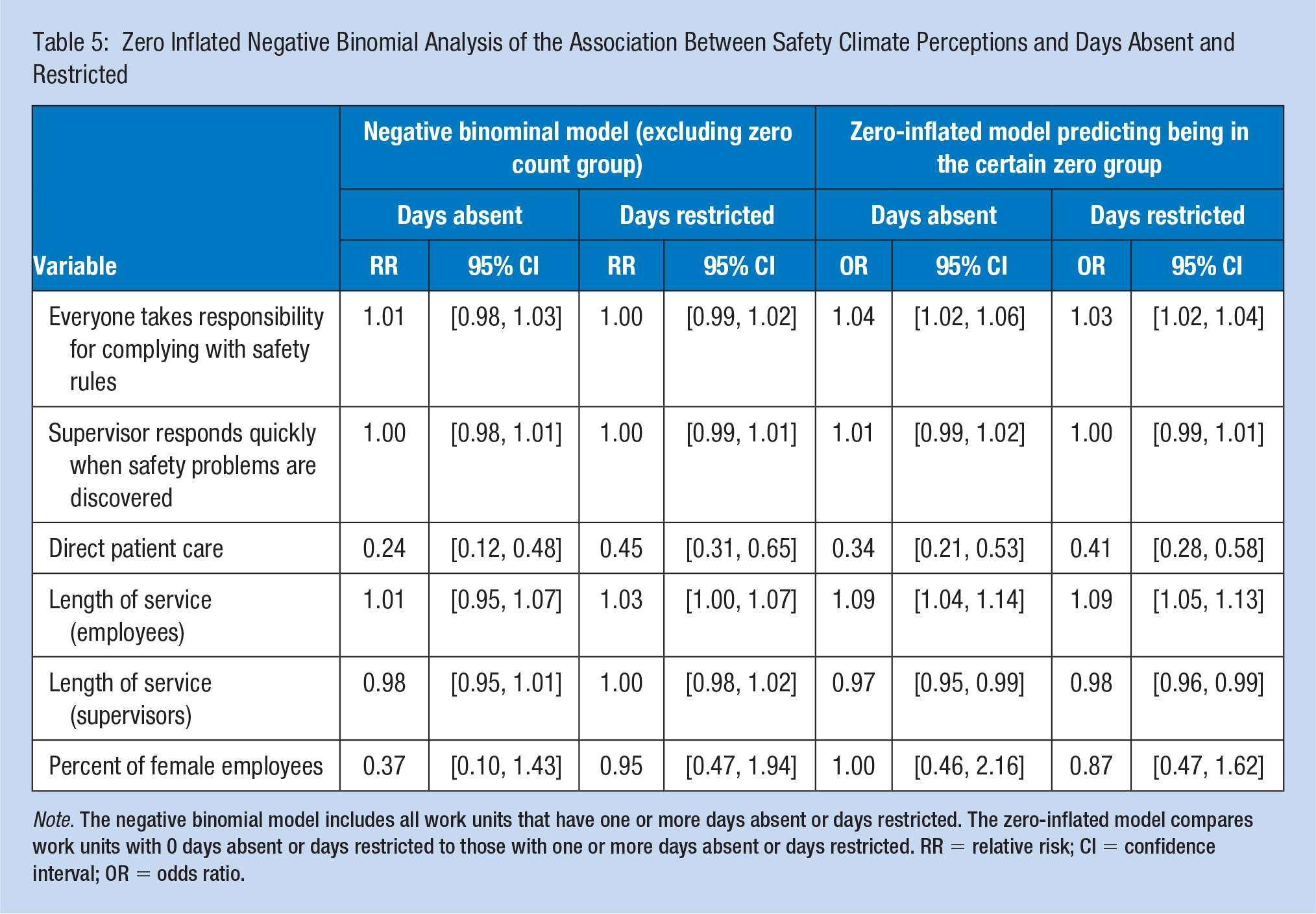
Note. The negative binomial model includes all work units that have one or more days absent or days restricted. The zero-inflated model compares work units with 0 days absent or days restricted to those with one or more days absent or days restricted. RR = relative risk; CI = confidence interval; OR = odds ratio.
We also observed that employees providing direct patient care were at less risk of having a greater number of days restricted RR = 0.45 (95% CI = [0.31, 0.65]), and also had reduced odds of being in the certain zero group (i.e., those in the no days restricted group) OR = 0.41 (95% CI = [0.28, 0.58]). Also, units providing direct patient care had a reduced risk of having a greater number of days absent RR = 0.24 (95% CI = [0.12, 0.48]) compared with non-direct patient care employees, and decreased odds of being in the certain zero group (i.e., no days absent) OR = 0.34 (95% CI = [0.21, 0.53]).
In addition, work units which had employees with greater lengths of service were at increased odds of being in the certain zero group (those that didn’t have any days absent nor days restricted) OR = 1.09 (95% CI = [1.04, 1.14]) and OR = 1.09 (95% CI = [1.05, 1.13]), whereas units which had supervisors with longer lengths of service had reduced odds of being in the certain zero group (those that didn’t have any days absent nor days restricted) OR = 0.97 (95% CI = [0.95, 0.99]) and OR = 0.97 (95% CI = [0.96, 0.99]).
Discussion
A hospital work unit’s perception of safety may provide indications that appropriate protocols are followed or that concerns about safety are being addressed by the work unit’s supervisor or those working in the unit. This study provides important caveats to previous research. First, previous research has indicated a relationship between supervisor response to safety issues and the number of injuries, but the current study did not replicate these findings, thus not supporting our hypothesis that work units which rated their supervisor’s response to employee safety concerns more positively would experience a lower number of employee injuries (Cook et al., 2016; Tucker, Ogunfowora, & Ehr, 2016). This may reflect the current study’s focus on perceptions of personal responsibility rather than assessing actual compliance with safety practices and policies. When those within a work unit take responsibility to comply with safe work practices, or at least it is perceived that there is a common expectation for taking personal responsibility to do so, the frequency of injury is decreased. Previous inquiry by Christian and colleagues (2009) confirms that peer networks, accountabilities, and cultures provide strong influence on the patterns of individual behavior and adherence to policies within organizations. Being surrounded by individuals perceived to value or uphold safety policies likely result in a positive feedback loop promoting those behaviors.
Previous inquiry has demonstrated that management and supervisory support is crucial in the creation of safe environments and safety cultures (McGonagle et al., 2016; Tucker et al., 2016). We do not believe the results of this study necessarily conflict with these findings and may provide some indication concerning the amount of influence and authority supervisors have at different locations. Acceptance of personal responsibility for complying with safety rules and policies is in large part due to messaging, education, and accountability measures implemented broadly by the organization, as well specifically by supervisors for each work unit. Whether organizational or supervisory actions are the most effective varies with supervisory interest and commitment, as well as the organizational priority and resourcing. For example, at the supervisory level, variation in how new workers are oriented to their work and how mission and safety imperatives are expressed are critical.
When considering the association between safety climate and days absent and days restricted there is mixed support. In both cases, there is a positive relationship between perceptions of personal responsibility within the unit and having no days absent and no days restricted. However, this relationship is not carried over into units that have any days restricted or any days absent. One explanation, and a unique aspect of this study, is the differences between employees providing direct patient care and employees who do not provide direct patient care. Previous inquiries looking at safety culture tend to not differentiate employee care responsibilities or focus primarily on clinical staff (Cook et al., 2016; McGonagle et al., 2016; Weaver et al., 2013). Within health care settings, employee injuries can and do occur throughout the organization, in both clinical and nonclinical environments, and in association with both random and systematic process failures (Bell et al., 2008; Clarke, Lerner, & Marella, 2007). This study indicates that direct patient care employees are at greater risk of an injury; however, they have less risk of experiencing restricted work or absence from the job. The reduced risk of lost or restricted days may be an artifact of the specific pattern of injuries commonly seen in the clinical environment or differences in how impairments due to injuries are managed.
Direct care staff are at greater risk of injuries such as needle sticks, minor sprains and strains, and abrasions and cuts which, while significant in terms of the care givers’ mental and emotional health, will generally not prevent them from physically performing their job (Green & Griffiths, 2013). According to the Centers for Disease Control and Prevention (CDC) health care employees experience approximately 385,000 sharps injuries each year (CDC, 2015). The potential for needle sticks and cuts to cause infection with hepatitis B, hepatitis C, HIV and other blood-borne pathogens mandates up to 6 months of follow-up testing for the employee. Studies suggest that significant anxiety and depression are common sequelae, but recordkeeping and benefits practices make it highly unlikely that any subsequent lost or restricted work days due to mental health issues will be seen as associated with the initial injury (Green & Griffiths, 2013). As a result, the greater risk of injury will not be reflected in a proportionately greater number of days absent or restricted, even as the employee’s cognitive and emotional abilities are compromised.
Although this study supports a need to continue to focus on the health and safety of employees who interact directly with patients, it also provides emphasis for the need to focus on the safety of the employees who do not provide direct patient care. Impaired or absent support workers can result in less effective or efficient patient care (Needleman, Buerhaus, Mattke, Stewart, & Zelevinsky, 2002). The ability of direct patient care employees to effectively provide patient care depends upon support staff who are available to conduct and complete complementary and support tasks. Limited staffing, lean inventories, and complex management systems can make loss or impairment of knowledgeable non-direct care staff problematic. In addition to potential impacts on clinical care processes, organizational impacts may include less informed business decisions, interruptions or unreliable claim processing and remediation, or impaired information system maintenance and support. The risk of disruption is particularly true given the higher risk of days absent or restricted, with associated direct and indirect costs among non-direct care staff. Furthermore, the impact of absent employees is easily underestimated. Operational impacts and costs are often hidden, but include workload capacity backups, quality issues, maintenance, and work flow issues (Marinescu, 2007). Estimates of indirect financial costs of work injuries are challenging, but are commonly estimated to be 4 times the direct costs of medical care and disability pay (Manuele, 2011). The disruptive consequences of support staff injuries place greater stress on patient care staff, increasing the potential for preventable injury or patient experience issues.
Finally, it is worth noting that the relationship between employee injuries and patient safety is both direct and indirect. Unsafe environmental conditions, which are antecedents for employee injuries, are also potential antecedents for patient injuries as the clinical work environment and patient care environments are typically the same. When employees are injured during the course of their duties, and are unable to perform their usual tasks, quality of work, the cost of care, and patient outcomes can be compromised (Aiken, Clarke, Sloane, Sochalski, & Silber, 2002). Common management responses to loss of staff, such as replacement of experienced staff by less experienced staff can compromises care (Aiken et al., 2014). In addition, redistribution of physically demanding work, such as patient handling, to remaining staff may increase their risk of injury. The impact of injuries not resulting in missed or reassigned time is less obvious, but distraction may increase the frequency of cognitive errors, and the emotional toll can result in staff disability at a later date (Memon, Naeem, Zaman, & Zahid, 2016).
Limitations
There are several study limitations worth considering. First, this is a cross-sectional study utilizing secondary data. As a result, there are aspects of the data, and nuances associated with interpreting the data that limit the ability to draw more concrete associations between the dependent and independent variables. In addition, the survey data utilized for this study does not provide the opportunity to evaluate other important measures or conceptual dimensions of safety culture. Similarly, the limitations of OSHA reporting when studying injuries are well known and have been summarized elsewhere (Fagan & Hodgson, 2017). The primary limitation relevant to this study is the extent of underreporting. The validity and reliability of the data is a limitation of the study, we believe the strengths of the study are not greatly affected by these issues. In addition, the work unit level evaluation also may contribute to some misclassification of direct versus non-direct care employees. However, utilization of work unit level data does provide strong indication as to the beliefs and behaviors of a group of individuals who share similar backgrounds and work tasks. As a result, assessment of safety beliefs and injuries within these groups does provide a solid foundation on which to review associations. Furthermore, the size of the population and breadth of work unit types and work responsibilities provide a unique opportunity to evaluate safety culture and injuries within an organization while still allowing for important nuances to be fleshed out such as provision of direct patient care.
Conclusion
Our findings suggest that greater agreement concerning a work unit’s responsibility to comply with safety rules and procedures is associated with fewer injuries. Furthermore, this study finds that employees providing direct patient care are at greater risk of injury, as well as more likely to be restricted or absent from work than employees working in non-direct patient care units. Employees in non-direct patient care units are, however, at greater risk of having a larger number of days restricted or absent from work when injured. These results point toward the need for organizations to assess and actively manage the organizational, supervisory, work group, and, ultimately, the employee’s personal commitment to safety.
Implications for Occupational Health Practice
This study suggests that it is important for occupational health professionals to have an understanding of the role of safety climate in preventing occupational injuries. Safety climate assessments at the unit level can provide important information regarding shared perceptions of peer beliefs about safety, as well as the nature of leadership and organizational support for safety (Hofmann, Burke, & Zohar, 2017; Zohar, 1980). This study indicates that unit perception of accountability for injury prevention is an important aspect of workplace safety (Christian et al., 2009). In addition, as previous authors have indicated, a holistic approach to safety which includes personal and supervisory support for processes and protocols focused on safety provides better adherence to safe work practices than a more coercive strategies (Yassi & Hancock, 2005; Yassi et al., 2010). In pursuing high reliability care, excellent care outcomes, outstanding patient experience, as well as a safe workplace workers, employee perceptions of safety and supervisors’ responses concerning safety, are areas of opportunity in which occupational health professionals can effectively intervene.
Commitment to clarifying and communicating supervisor and employee responsibilities can help foster a climate of safety and is likely to encourage both groups to play a more active role in ensuring workplace safety (Kiani & Khodabakhsh, 2014). Training that incorporates supervisors as well as work teams or work units may provide for better communication and understanding of safety protocols and responsibilities (Weaver et al., 2013). Furthermore, application of established harm reduction measures such as education on how to recognize and mitigate safety problems and safety self-assessments to staff concerns may serve to help reduce the likelihood of employee injury.
We acknowledge that different strategies may be appropriate depending upon the work environment (Sokas et al., 2013). Managers and frontline supervisors are directly responsible for the safety, health, and well-being of their employees in both direct care and non-direct care areas. Better understanding of the particular risks and injuries common in both areas will provide both managers and employees working in those areas additional knowledge concerning prevention, and risk mitigation (Yule et al., 2006). This understanding can also help to tailor needed training, and evaluations of work processes. For instance, in non-direct patient care settings, education or interventions concerning overuse injuries or poor ergonomics associated with work stations may prove to be a fruitful, particularly if both supervisors and staff are educated on identifying and applying appropriate resources to reduce risks or remedy poor processes. Likewise, in direct patient care settings, supervisors and staff will likely need training or resources that will prevent slips and falls, poor lifting habits, and patient engagement and emotional de-escalation skills.
Finally, studies such as this are important in identifying areas which promote or inhibit safety behaviors. Future assessments could take evaluations further by defining available resources, amount of training, and specific types of injuries to better identify specific needs for injury prevention (ceiling mounted lifts, nonslip flooring, more ergonomically appropriate work stations), needed educational interventions, or improved processes and procedures that limit injuries or help develop stronger cultures of safety through enhanced organizational support. By better understanding the nuances of the injury data occurring throughout the facility, a more focused opportunity to intervene and create a more a safe environment is possible (Bell et al., 2008).
Applying Research to Occupational Health Practice
Our findings suggest that the higher proportion of a work unit’s employees who believe it is their responsibility to comply with safety rules and procedures, the fewer occupational injuries. Furthermore, this study finds that employees providing direct patient care are at greater risk of injury, as well as more likely to be restricted or absent from work than employees working in non-direct patient care units. This study suggests that it is important for occupational health professionals to have an understanding of the safety climate in the units with which they work. Safety climate assessments at the unit level can provide critical information regarding shared perceptions of peer beliefs about safety as well as the nature of leadership and organizational support for safety. In pursuing high reliability care, employee perceptions of safety and supervisors’ responses concerning safety, are areas of opportunity in which occupational health professionals can intervene.
Footnotes
Acknowledgements
This study was made possible by support from the Robert D., and Patricia E. Kern Center for the Science of Health care Delivery.
Ethical Approval Statement
Retrospective research study was approved by Institutional Review (IRB ID: 16-008960).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Duaa Aljabri, PhD, is an assistant professor of health services policy and management at the College of Public Health, Imam Abdulrahman Bin Faisal University, Saudi Arabia. She earned her PhD from the University of South Carolina. She worked as a research fellow at Mayo Clinic Florida. Her research interest is focused on health services evaluation and improvement.
Andrew Vaughn, MD, MPH, is an occupational physician with a special interest in the how healthcare workforce safety enables safe, effective patient care. He recently served as Director of Employee Health and Safety for Mayo Clinic in Rochester, Minnesota, and previously as Global Medical Director for Eastman Kodak.
Matthew Austin, CIH, is the Occupational Safety Administrator at Mayo Clinic, providing strategic and operational support to Mayo Clinic’s integrated clinical practice, education, and research initiatives. He is a Certified Industrial Hygienist (CIH) and received his Bachelor of Science in Industrial Hygiene–Environmental Toxicology from Clarkson University; a Master of Science in Public Health in Environmental Sciences and Engineering from the University of North Carolina-Chapel Hill; and a Master of Science in Management from Rensselaer Polytechnic Institute.
Launia White, BS, has been working as a statistical program analyst at the Mayo Clinic since 2014. She is an expert in data retrieval, data manipulation and data organization.
Zhuo Li has been working as a biostatistician in Mayo Clinic for over 10 years by applying statistical, computer, and scientific expertise to the design, implementation, analysis, interpretations, and reporting of clinical research projects including retrospective studies and clinical trials. She is proficient in the use of SAS and R, and has a strong background in statistical theory and application.
James Naessens, MPH, ScD, is a Professor of Health Services Research at Mayo Clinic. Dr. Naessens also serves as the scientific director of the Robert D. and Patricia E. Kern Center for the Science of Health Care Delivery at Mayo Clinic Florida. For the last decade, he has worked extensively on quality measurement and improvement.
Aaron Spaulding, PhD, is an Associate Professor of Health Services Research at Mayo Clinic. As a health services researcher in Mayo Clinic’s Division of Health Care Policy and Research, as well as the Mayo Clinic Robert D. and Patricia E. Kern Center for the Science of Health Care Delivery, he conducts research related to the outcomes, quality, and value of health care.