
Abstract
With the rapid growth of the aging workforce, age-related conditions may negatively influence overall workplace safety and health among these workers and their employers. In this summary, we have outlined details about visual acuity, glare sensitivity, and contrast sensitivity, which are common age-related vision changes that can potentially affect their occupational safety. The occupational health nurse is well positioned to address these concerns by instructing aging workers about potential development of vision change and ensuring they receive the appropriate vision screening. By assisting employers to modify work environments to accommodate this population, the occupational health nurse can reduce the risk of injury, as well as positively impact the health of their aging workforce.
Keywords
Introduction
A 68-year-old worker presents to the occupational clinic complaining of right wrist and right knee pain after a recent fall in the warehouse. The worker describes descending a staircase in the warehouse and missing a step resulting in a fall. He explains lighting in the area was dim and he has recently noticed difficulty seeing in low lighting. Aging workers are at risk for falls in poorly lit environments. The purpose of this article was to describe the most common age-related visual changes, their potential effect on occupational safety, and mitigating strategies to be considered for application by occupational health nurses.
The National Institute on Aging’s 21st Century Strategic Directions for Research aims to improve aging for all Americans to maintain their independence, healthy lifestyles, and overall quality of life (National Institute on Aging Strategic Directions, 2016). With advances in medical technology and treatment modalities, the number of older adults in the United States (U.S.) will continue to grow at a rapid rate. According to the U.S. Census Bureau, roughly 50 million people (15%) of the population are aged 65 years and older. By 2030 and 2050, older adults will account for 70 million and 89 million, respectively (U.S. Census Bureau, 2017). As the annual number of older adults increases, the likelihood of America’s labor force participation among older adults will also increase (Collins & Casey, 2017).
In 2026, the Bureau of Labor Statistics projects the number of people in the workforce who are 55 years and older will represent roughly 25% of all American workers, which is approximately a 3% increase from 2016 (Bureau of Labor Statistics, 2017). Specifically, these trends will continue to increase with workers aged 65 to 74 years and 75 years and older, accounting for an annual growth of 4.2% and 6.7%, respectively (Bureau of Labor Statistics, 2017). These unprecedented workforce occurrences will more likely inform stakeholder (e.g.: policymakers, and businesses) future decisions regarding occupational preferences (setting, roles, size), labor force participation rates, and retirement conditions (Collins & Casey, 2017).
According to Crews, Chou, Stevens, and Saaddine (2016), an estimated 2.8 million people aged ≥65 years in the U.S. reported severe vision impairment such as being blind or impaired vision, with or without eyeglasses. Poor vision is a risk of injury and in particular falls in this population (Crews et al., 2016). A number of age-related conditions, such as macular degeneration, cataracts, diabetic neuropathy, glaucoma, dry eye, and low vision, may impair workers’ vision as they age, which could potentially affect the safety and health of this growing population (Nylén, Favero, Glimne, Fahnehjelm, & Eklund, 2014).
Common Visual Changes Associated With Aging and Associated Tests
Visual Acuity
Visual acuity degrades with aging, and degrades in a parallel manner. That is, as age increases, visual acuity worsens (Porto et al., 2016). Changes in visual acuity such as presbyopia, which is the inability to focus on close objects, is frequently experienced within the aging population (Katada et al., 2016). Although refractive changes in natural lenses and the use of outdated corrective lenses have been identified as related influencing factors contributing to visual decline in this group, other contributing factors may also be present in the older person. For example, the actual amount of light entering the eyes may be decreased in older workers due to the presence of cataracts (Eichenbaum, 2012). Moreover, it may be that there is a deterioration of perception of visual information in older individuals related to visual input signal strength and perceptual and cognitive processing (information degradation hypothesis; Monge & Madden, 2016).
Visual acuity is commonly measured in the occupational health setting and conducted using variations of standardized wall-mounted or movable charts such as the Snellen, Landolt C, Tumbling E, or less often, the Feinbloom, and Early Treatment of Diabetic Retinopathy (ETDR) charts. Visual acuity may also be measured using standardized charts mounted in a standing or wall-mounted light box (Elliott & Flanagan, 2007). Regardless of the measurement method used, it is critical that the occupational health nurses know the correct distance and procedures for the specific visual acuity testing method. It is also essential that visual acuity documentation includes that of each eye individually, both eyes, and whether or not the test was performed with corrective lenses.
Contrast Sensitivity
Contrast sensitivity is a measure of the ability of the visual system to discriminate an object from its background (Dorr, Lesmes, Lu, & Bex, 2013). Although contrast sensitivity declines in healthy aging individuals (Karatepe, Köse, & Eğrilmez, 2017), it is also comorbid with age-related eye diseases. Common conditions associated with aging are also associated with decline in contrast sensitivity. Among these conditions are macular degeneration, cataracts, and glaucoma (Bowling, 2016; Carr et al., 2016). There are many ways to measure contrast sensitivity, including grating charts (VisTech or FACT charts), letter charts (Pelli-Robson, MARS), and computer- and tablet-based assessments (Dorr et al., 2013; Richman, Spaeth, & Wirostko, 2013). However, these measures are not commonly part of an occupational health nursing assessment. Instead, the occupational health nurses should elicit from employees whether or not they are having difficulty distinguishing backgrounds, such as determining the leading edges of steps in a staircase. If so, the worker should be referred to an ophthalmologist for further testing.
Glare Sensitivity
Glare occurs when light is scattered on the retina, also known as straylight (Van den Berg, 2017). Two human responses to glare may occur including discomfort glare, which is the feeling of discomfort when directly exposed to bright light (e.g., headlights, spotlights), as well as disability glare, or the actual reduction in visual acuity related to light scattering on the retina after exposure to bright light (Van Den Berg, Franssen, & Coppens, 2009). Objective measures of disability glare may be achieved with the use of several different types of instruments. As with contrast sensitivity measures, the measures of glare sensitivity are not done in the occupational health setting. Thus, appropriate assessments and referrals for additional testing among employees with glare condition difficulties are essential.
Visual Accommodations in the Aging Workforce
The occupational health nurses and employers can assist aging workers with visual accommodations in the workplace, particularly with visual acuity, a common problem in aging workers. Presbyopia is one of the most common changes in visual acuity for aging workers (Nylén et al., 2014). Suggestions for presbyopia are workplace magnifiers, directional lighting, computer screen magnifiers, as well as enlarging numbers and texts to a 12-point font minimum with a dark print and a light background (Phillips & Miltner, 2015; Rogers et al., 2011). Safety glasses with bifocal lenses are available to assist workers with presbyopia (Perry, 2010). Workers with untreated presbyopia can lead to eyestrain and headaches, which in turn leads to lost productivity, an average of US$2,100 a year (Mowbray, 2013). It is important for workers to acknowledge this change in vision and ask for possible accommodations with presbyopia. Older workers can have a reduced field of vision, so signs should be at eye level, as older workers may not see a sign unless in their direct field of vision (Perry, 2010). Visual acuity can be an issue for older workers who operate machinery and forklifts in dark areas like a warehouse, so adequate lighting is important. Aging drivers have difficulty not only in static acuity but also in tracking moving objects, which increases the risk for a motor vehicle accident (Perry, 2010). An employer should recommend routine eye exams for aging workers not only for acuity but also for age-related diseases such as cataracts to prevent injuries and motor vehicle accidents.
For contrast sensitivity, optimizing lighting is important particularly in stairwells or in dark areas like a warehouse. Color contrasting treads and marking changes in levels of surfaces like steps should be administered to reduce the risk of slips, trips, and falls (Rogers et al., 2011). Poor lighting can hide hazards like objects on the ground, spills, and uneven flooring causing injury. It is also important to have uniform lighting and eliminate areas where lighting goes from brightly lit to dim; these sudden changes in lighting increase the risk for sensitivity and can result in falls (Phillips & Miltner, 2015).
Older workers can be more sensitive to glare than younger workers (Rodriguez-Acosta, Pratt, Olsavsky, & Morgantown, 2016). Glare sensitivity is a normal result of the aging process of the eye, so accommodating changes in glare is beneficial for aging workers physically and psychologically (Nylén et al., 2014). Moreover, glare can only be tolerated in short intervals and prolonged exposure may be distressing for the worker (Nylén et al., 2014). Providing window shades can reduce direct light, as well as installing light diffusers and variable light sources for glare sensitivity (Rogers et al., 2011). Perry (2010) suggested removing glare by putting carpets over polished floors, providing adjustable light sources for younger and older workers, as well as being cautious using reflective paints in the workplace that cause a glare. Workers looking at computers may benefit from anti-glare screens (Phillips & Miltner, 2015). Glare sensitivity can also be an issue in older drivers. Older drivers may be more sensitive to the sun and headlights. A driver may need a change in their work schedule, particularly if they drive in the early morning hours, at dusk or night if glare during these times is an issue (Rodriguez-Acosta et al., 2016).
It is important to remember that not only are these visual accommodations beneficial for aging workers, but for all workers to prevent injuries and provide a safe working environment. Visual acuity changes, contrast sensitivity, and glare sensitivity can occur in younger workers as well, so addressing these issues is beneficial for all workers.
Implications for Occupational Health Nurses
Workers with visual impairment may hesitate to request accommodations for many reasons. They may experience fear with appearing ineffective, receiving negative responses from employers and fellow employees, fear of discrimination for requesting and receiving accommodations, and possible job loss. (Dong, Warner, Mamboleo, Guerette, & Zalles, 2017). It is crucial that occupational health nurses take leadership in promoting healthy and safe work environments that embrace the value of aging workers in the work setting (White, Burns, & Conlon, 2018). Facilitating understanding of legal and ethical importance to make reasonable accommodations in the workplace may decrease potential discrimination behaviors reflected by coworkers and supervisors. Encouraging implementation of universal design principles when determining appropriate accommodation techniques can improve work life for employees of all ages and abilities (Matt, Fleming, & Maheady, 2015).
Research
Research focused on assessment of employer and worker knowledge of Americans with Disabilities Act (ADA) mandates regarding visual accommodations may identify deficits requiring instruction to improve accommodation processes. In a systematic review by Gould et al. (2015), it was identified that many employees needing work accommodations did not have adequate knowledge of individual rights that applied to them under ADA law, thus hindering their ability to advocate for themselves. Opportunities exist to conduct studies further investigating strategies to mitigate workplace biases toward employees receiving accommodations, including those for visual impairment due to aging. In a study conducted by MacDonald-Wilson, Fabian, and Dong (2008), the main barrier identified by employees with visual challenges that prohibited them from requesting accommodations was the negative stance of the employer. Exploring barriers and facilitators to accommodation of aging workers may reveal areas requiring improvement including adjustment of accommodation processes and successful facilitation strategies. In a study conducted by Kensbock, Boehm, and Bourovoi (2017), participants revealed that their managers lacked understanding of their condition that required accommodation, and they felt more supported by their coworkers than their employers. Addressing concerns of supervisors, coworkers and the accommodated worker could enhance communication and acceptance by all parties, resulting in team cohesiveness and successful continuation of employment for the accommodated worker.
Investigation is necessary to determine best practices for motivating acceptance and inclusion of aging workers with low vision and other disabilities in the occupational setting. Further examination of successful methods for application of universal design techniques may prove useful when determining appropriate duties for older workers with visual impairment.
Education
It is crucial to provide workers, health care staff, and plant management with information about employee rights under the ADA (1990) and instruction concerning accommodations available to aid specific low-vision conditions. Providing these educational tools could assist workers to determine whether requesting visual accommodations is appropriate for their needs (Tompa et al., 2015). In addition, providing this education to all employees could improve cohesiveness of fellow workers of aging individuals that are being accommodated for low vision. Improving physical examination and worksite assessment skills used to determine appropriate accommodations for visually impaired employees is important for occupational health nurses and workplace management. The ADA specifies that reasonable accommodations should be made for workers with disabilities to remove barriers that impede ability to perform functions essential to their job (MacDonald-Wilson et al., 2008). In addition, the ADA specifies that the accommodations made should not result in “undue hardship for the employer” (ADA, 1990). Understanding specific details of daily operations in the workplace is important for all who provide occupational care to patients and who assist in determining work accommodations. Occupational health nurses should seek to master assessment techniques and interpretation of results of visual screening. Tools and equipment employed to assess visual acuity must be used skillfully to achieve quality results. In addition, accurate interpretation of results is crucial when determining whether an aging employee can safely perform their job with accommodations. It is beneficial for the occupational health nurses to maintain a professional collaborative relationship with an eye care provider, for consultation when vision testing results vary from accepted parameters. Seeking a culture of diversity in the workplace that includes older workers and those with disabilities, and building an environment of inclusiveness may play an important role in worksite success (Kensbock et al., 2017). Embracing accommodated older workers and the important work they contribute to the mission of the organization is essential for a healthy occupational environment. When employers accommodate needs of employees with disabilities, awareness of benefits and value that providing reasonable accommodation also extends to the workplace should be emphasized (MacDonald-Wilson et al., 2008). Gould et al. (2015) conducted a review of ADA employment research revealing that employer’s knowledge of ADA compliance was basic leaving room for individual interpretation of the mandates regarding accommodation. In turn, the review disclosed that for individuals with disabilities, a lack of knowledge of their rights under ADA affected the ability to petition for themselves. Careful instruction is needed to help aging workers utilize accommodations to the fullest potential. Streamlining return to work processes including the acquisition of equipment necessary for accommodations can assist to return the aging worker to a productive employment status in a timely manner.
Practice
Because adequate visibility and lighting are significant factors affecting vision in aging workers, it is important to assess the quality of these features when planning visual accommodations. Standard lighting combined with adaptable lighting can provide higher illumination levels to accommodate vision in older workers (Van Bommel & van den Beld (2003). There are 11 different components to be considered when providing suitable ergonomic lighting. No one assessment or tool provides all information needed to determine the “best lighting” for an interior environment. One assessment tool, the Ergonomic Lighting Indicator (ELI) is a 5-scale, 38-item questionnaire used by designers when seeking feedback to guide lighting design. The tool collects both objective and subjective data related to visual lighting quality information including visual performance, view, visual comfort and vitality and control. Administering this tool before and after initiation of lighting enhancement for older workers could provide measurable information to evaluate improvement of individual vision for work in the environment (Kruisselbrinka, Dangola, & Rosemanna, 2018). Furnishing glare screens for computer monitors can reduce the effects of decreased contrast sensitivity experienced by many older workers. Use of ultraviolet (UV) protective sunglasses for employees who work outdoors or in sunlight, and for those who operate machinery, may serve to decrease discomfort glare. It is important to note that most visual changes caused by aging develop slowly, and many individuals may not realize the degree of change that has occurred over time without regularly scheduled visual testing for comparison. Promoting annual evaluation by an eye specialist is important for all workers aged 65 and older and for any worker with established ocular disease (Nylén et al., 2014). Consideration of referral to an ophthalmologist for vision evaluation and recommendation of reasonable visual accommodations for the workplace may be an alternative in some occupational settings (Table 1).
Visual Accommodations for Workers
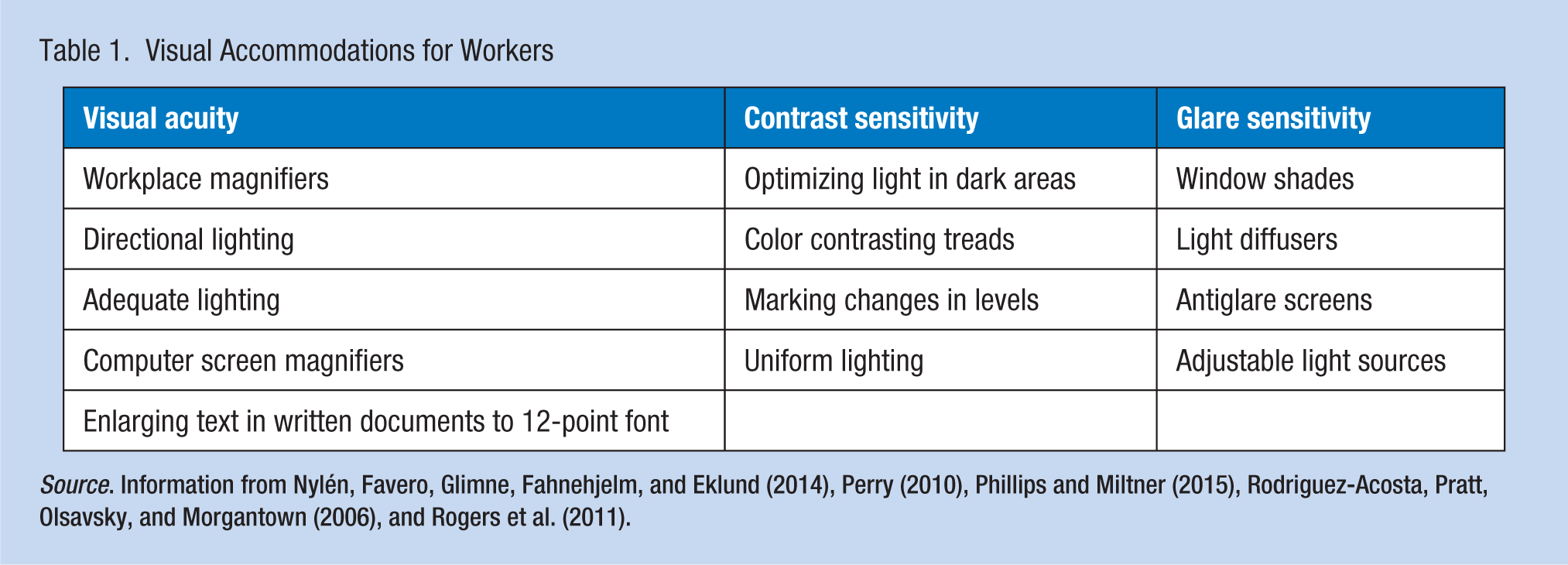
Source. Information from Nylén, Favero, Glimne, Fahnehjelm, and Eklund (2014), Perry (2010), Phillips and Miltner (2015), Rodriguez-Acosta, Pratt, Olsavsky, and Morgantown (2006), and Rogers et al. (2011).
Conclusion
Age-related vision changes are common in the aging population. Visual acuity, glare sensitivity, and contrast sensitivity are common challenges experienced by aging workers. The occupational health nurse may be the first health care provider to recognize visual changes and identify potential accommodations. Occupational health nurses should be skilled to conduct effective visual screening, interpret test results, and make recommendations for visual accommodations in aging workers.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Deep South Center for Occupational Health and Safety Grant (T42OH008436).
Author Biographies
Stephanie Hammond is an assistant professor at the University of Alabama School of Nursing. She is an adult nurse practitioner with years of experience in occupational health and safety.
Pamela G. Bowen has an active program of research, which focuses on physical activity as a lifestyle behavior to manage and prevent chronic conditions associated with inactivity. Her funded projects have emphasized multilevel (individual- and system-level) approaches to increase and promote physical activity as a strategy to improve overall health outcomes.
Melanie Gibbons Hallman has been a leader in emergency services for over 39 years, actively serving as an emergency nurse practitioner for the past 24 years. She served as clinic director of a large municipal occupational health clinic providing urgent and occupational health services for 15 years. She is currently a coordinator of the Emergency Nurse Practitioner subspecialty at the University of Alabama at Birmingham School of Nursing.
Karen Heaton is an associate professor and director of the PhD and Occupational Health Nursing programs at the University of Alabama at Birmingham School of Nursing.