
Abstract
The integration of health coaching in workplace interventions has increased over the past several years. However, the tasks and the qualifications of the coaches have not been clearly defined. The objective of this qualitative study was to assess workplace stakeholders’ expectations regarding a health coach. Systematic field notes of 11 meetings and 14 semi-structured interviews with stakeholders of a workplace intervention, including employees, company doctors, and representatives of health insurances, were analyzed according to the structured content analysis. Stakeholders reported that the main aspect of a health coach’s work should be the motivation of clients (workers) to achieve their internally developed goals. Regarding the coach’s competencies, personal, methodological, and social skills were desired. They also expected that the health coach use a range of different approaches to develop contacts and, in terms of content, focus on physical activity. These findings provide a step toward establishing criteria for professional health coaching and an evidence-based curriculum for coach training.
Introduction
Health coaching is associated with a client-centered education method which aims to motivate individuals to achieve self-determined health-promoting goals and to improve self-management (Butterworth, Linden, & McClay, 2007; Palmer, Tubbs, & Whybrow, 2003; Wolever et al., 2013). In recent years, the integration of health coaching in lifestyle intervention has emerged as a promising approach to initiate behavioral changes and to improve health (Hill, Richardson, & Skouteris, 2015; Kivelä, Elo, Kyngäs, & Kääriäinen, 2014). This has led to the development of health coaching interventions for both rehabilitative and preventive settings (Dejonghe, Becker, Froboese, & Schaller, 2017) and to the proliferation of international peer-reviewed articles on health coaching (Sforzo et al., 2017).
The number of people working as health coaches has risen, and their qualifications and working methods vary markedly (Wolever et al., 2013). Although efforts to introduce certification programs exist, field-wide standards have yet to emerge. Indeed, there is still much room for improvement when it comes to the establishment of clear accreditation criteria and recognized professional associations (Collins et al., 2018; Johnson, Saba, Wolf, Gardner, & Thom, 2017; Jordan, Wolever, Lawson, & Moore, 2015; Kivelä et al., 2014; Olsen & Nesbitt, 2010; Thom et al., 2016; Wolever et al., 2013).
The workplace is considered a promising setting for the implementation of health coaching (Cheng & Chan, 2009; Duijts, Kant, van den Brandt, & Swaen, 2008) as the challenges in work life have increased due to the lengthening of working lifetime and the shortage of skilled employees. As a consequence, health promotion is considered of utmost importance (Rongen, Robroek, van Lenthe, & Burdorf, 2013; van Rijn, Robroek, Brouwer, & Burdorf, 2014; Varekamp & van Dijk, 2010).
In Germany, the relevance of the workplace setting is underscored by the new Preventive Health Care Act (July 2015), which strengthens the field of workplace health promotion (e.g., by requiring collaboration among providers; Federal Ministry of Health, 2017). An example of a workplace lifestyle intervention in collaboration with different social security agencies and companies is the preventive intervention of the German Pension Fund Rhineland (2013). Designed for employees with health-related risk factors, this intervention promotes a health-oriented lifestyle through a behavior-oriented lifestyle intervention and the assignment of a health coach. However, neither the working methods nor the necessary qualifications of such a coach are clearly defined. Little is known about the expectations of the different stakeholders involved in the intervention process, such as participants, providers, and representatives of funding agencies. Based on this, there is a need to establish conceptual and operational clarification in the field of health coaching. The objective of the present qualitative study was to identify and analyze the expectations of different stakeholders regarding the necessary competencies and working methods of a health coach in an occupational health setting.
Method
This qualitative study was part of a project titled “AtRisk” which was approved by the German Sports University Cologne Ethics Committee. AtRisk was a project pertaining to primary prevention and health promotion (Schaller, Alayli, et al., 2016). More specifically, the AtRisk-project evaluated a workplace-related intervention of the German Pension Fund Rhineland (Schaller, Dejonghe, Alayli-Goebbels, Biallas, & Froboese, 2016). The intervention targeted employees who were at risk of chronic diseases, such as those showing initial signs of possible musculoskeletal, internal organ, or mental impairment that was noticeable at work, but was not yet formally diagnosed as a disease—for example, an office worker who had occasional backaches that negatively affected their work performance, but had not been formally diagnosed with chronic back pain. One component of the intervention was a behavior-oriented lifestyle intervention, which mainly took place in ambulatory rehabilitation centers. Another integral component of this complex intervention was the work of a health coach, who supported the employees individually with improving their lifestyle. The coaches were employees of special coaching companies or of the rehabilitation centers. The German Pension Fund, German Statutory Health Insurances, and employers cooperated in this intervention. More details about the intervention’s conceptual guidelines (German Pension Fund Rhineland, 2013) and/or the protocol of the AtRisk-project can be found elsewhere (Schaller, Dejonghe, et al., 2016).
The purpose of this study was to clarify the function of a health coach by assessing the expectations of the stakeholders of the workplace intervention of the German Pension Fund.
Study Setting and Population
To answer the research question, a qualitative study was employed. The study participants were stakeholders of the workplace intervention, including the following: employees with health-related risk factors, company doctors, representatives of the human resources departments of cooperating large companies in different sectors, representatives of the cooperating rehabilitation centers (directors, therapy managers, and therapists), representatives of involved social insurance agencies, and health coaches. To guarantee confidentiality, the exact number of the different participants is not provided. Systematic field notes of 11 meetings and 14 semi-structured interviews were conducted.
Study Design
This qualitative study consisted of systematic field notes of meetings followed by semi-structured interviews, which was chosen because it facilitated an in-depth exploration of an unanticipated issue and generated a detailed perspective (Ritchie, Lewis, McNaughton, & Ormston, 2014). The purpose of the meetings was to get to know the stakeholders of the workplace-related intervention (e.g., health coaches, representatives of the rehabilitation centers, company doctors) with the aim to acquire them as participants for the AtRisk-project. An additional aim was to gain information about the current status of the intervention and learn the advantages and disadvantages of using a health coach.
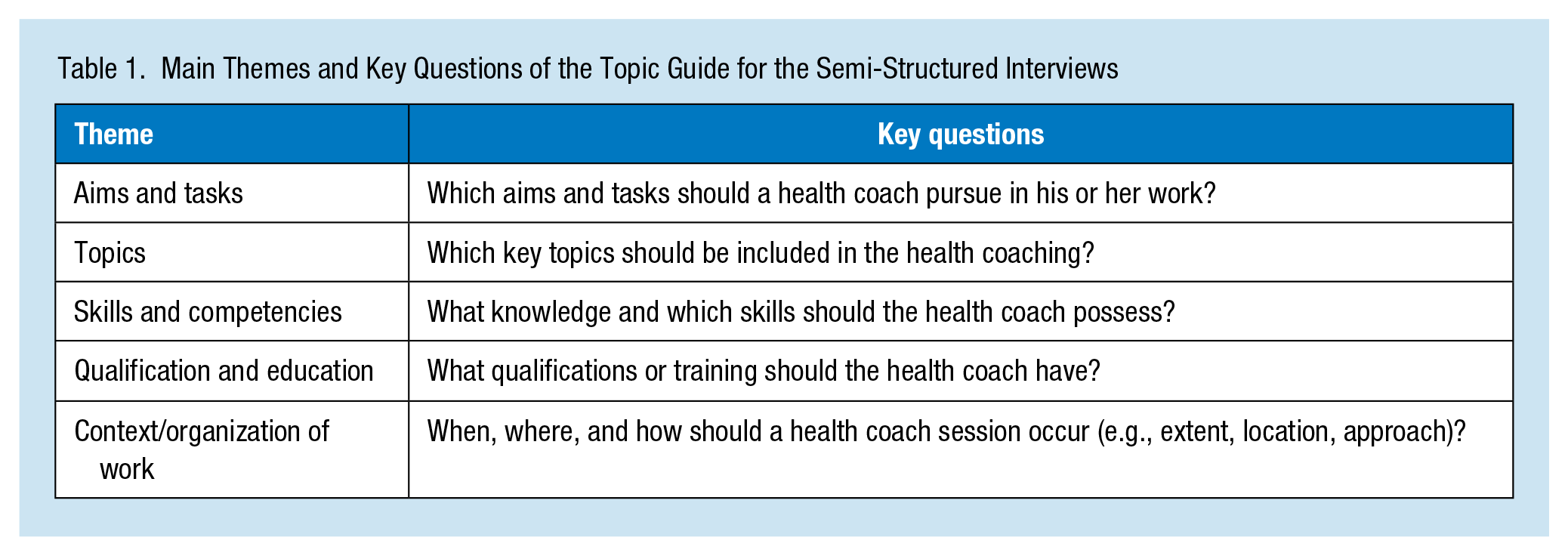
For the semi-structured interviews, two researchers developed a topic guide for structuring the interviews based on the phases “collecting,” “check,” “sort,” and “subsume” (Helfferich, 2011). Checked against the criteria proposed by Kruse (Kruse, 2015), the topic guide consisted of open-ended questions grouped into four categories: opening questions, introductory/transition questions, key questions, and ending questions. A pretest was undertaken with bachelor students (studying “sport and health in prevention and therapy”) who were not involved in the study. According to the results of the pretest, the topic guide was adjusted. Table 1 provides an overview of the main topics and key questions included.
Main Themes and Key Questions of the Topic Guide for the Semi-Structured Interviews
Recruitment
When identifying participants for the meetings and the interviews, the researchers relied on a German Pension Fund Rhineland steering committee that assembled stakeholders from the workplace intervention to share their experiences. During one session with the steering committee, the researchers presented plans for the AtRisk-project and afterward recruited potential participants for the current study via email. Employee participants of the intervention were not members of the steering committee and were, therefore, recruited through the cooperating companies and/or intervention providers. Recruitment continued until the researchers felt that data saturation was achieved (Ritchie et al., 2014).
Data Collection
Data collection included 11 meetings and 14 interviews with key stakeholders. In 11 meetings, a total of 22 participants were visited between April 2015 and May 2016. During these meetings, the researchers asked participants about the advantages and disadvantages of using a health coach in the intervention of the German Pension Fund.
For purposes of facilitating the discussion between the researchers and the participants, the researchers developed a topics list and a systematic protocol for recording the field notes. Study researchers conducted the meetings and took notes based on the discussions. The researchers always met the participants at their places of work. After the meetings, the lead author summarized the notes, which were then checked by the project lead.
Between April 2015 and May 2016, 14 interviews were conducted. Before starting the interviews, the researchers provided written details of the study to all participants, and they gave their written informed consent to be interviewed. If the participants agreed, the interviews were audio recorded. During all the interviews, two researchers were present: One led the conversation following the topic guide, whereas the other took notes.
The meetings and the interviews were conducted in German, and the included passages were professionally translated into English.
Data Analysis
The audio-recorded interviews (n = 12) were transcribed verbatim according to the rules of Kuckartz (2014) and then double checked to minimize errors. Two participants did not agree to audio recordings of their interviews; for these, the researchers relied on their written notes. The structured field notes of the meetings were also included. All written documents were anonymized via codes.
Data analysis followed the structured content analysis proposed by Kuckartz (2014), which is similar to the analysis of Mayring (2015). This method consisted of a concurrent deductive and inductive approach. As a first step, the researchers identified main categories, which were mostly based on the main topics of the guide. Next, they formulated subcategories inductively within an analytic framework (system of categories). For each category, they selected an example of the data, determined a definition, and developed a coding rule. They then grouped common themes and issues into main categories and subcategories. One researcher coded the data, while a second researcher scrutinized the data. Contentious issues were resolved by discussion. The software MAXQDA 12 (VERBI Software GmbH, Berlin) was used to analyze the data.
Results
During 11 meetings, a minimum of one and a maximum of three participants were present, with a total of 22 participants (10 females, 12 males). Most of the meetings included representatives of the rehabilitation centers (n = 7).
Moreover, the 14 semi-structured interviews were conducted with nine female and five male participants. At least one participant from each of the following groups was interviewed: employees, company doctors, representatives of the human resources departments of cooperating companies, representatives of the cooperating rehabilitation centers, representatives of the involved social insurance agencies, and health coaches. The age of the participants ranged between 29 and 64 years.
Health Coach: Aims and Tasks
Nearly all participants said that the main aim and role of the health coach should be to help employees improve their quality of life and achieve health-oriented goals. They stressed that these goals should be realistic and at least partially self-determined. The health coach should be a companion who is able to enhance the motivation of the employees for a sustainable lifestyle change. It was reported that coach’s clients (the worker) should be ultimately empowered to achieve their goals. Therefore, “help to self-help” was commonly identified as a task: There are family problems, children, and spouse, whatever. There are also times of ups and downs at work [ . . . ]. But I believe that it is most important that the participants [the worker] be motivated again and again to stay with it, not to lose sight of their own objectives, to do something together with them and thus to also lead them a little way out of their sorrowful state. I believe that this is the main task of the health coach [ . . . ]. (Human resources department employee) Thus, the health coach should be able to see every individual, with their specific characteristics, and to let them know that they possess an amazing potential. That each participant is therefore not going somewhere to get something but that they themselves possess a huge scope for development. [ . . . ] And in this way, I see the health coach as a companion. (Social insurance agency representative)
The interviewers also suggested that coaches should exert pressure on employees who lack sufficient motivation: One can’t motivate everyone with “come and join us,” but one can apply enough pressure such that at some stage they will do something. (Employee)
The data indicated that a health coach should act as a role model for a healthy lifestyle. Hence, health coaches should themselves lead health-conscious lives while conveying information and know-how in an easy-to-understand manner. Some participants observed that the support of the coach is necessary to identify individual needs. There was a sense that health coaching should be based on a client-centered approach: Thus, I think the task of transferring the information is already one which has a higher priority [ . . . ]. Here, a health coach can therefore exert a really big influence on the individual because they can adjust themselves to every individual. (Human resources department employee) She must be able to participate in everything which she also requires of us. Let’s say if she talks about nutrition then I assume that she has also had experience in dealing with nutrition and has not just read about it somewhere on the Internet shortly before. If one talks about sport and differing types of sport activities then she should also know something about it. (Employee)
In one company, the participants demanded that the health coach should be able to promote a group dynamic and build an associated team spirit. For them, a heath coach should have an overview over a group of employees as well as work with individuals. A coach should be connected and engaged with the involved participants, represent the interests of the clients, and act as a link between the various interest groups: He certainly ought to also assume the role of a process manager, or something similar, that when difficulties arise, [ . . . ], he acts as spokesman for his group’s members and represents the interests of his group’s members. (Social insurance agency representative)
Health Coaching: Topics
With regard to the thematic focus on health coaching, most of the participants believe that the emphasis should depend on the individual, although they also believe that individual behavior and environmental changes should be considered in all cases: In fact, the topic is determined by the person who is sitting in front of you. (Health coach)
The researchers identified four central workplace issues. In order of priority, these were (a) physical activity, (b) nutrition, (c) relaxation, and (d) addiction (especially to nicotine). Overall, the participants mostly listed only shallow topics and did not go into the details. Slightly more detailed statements were made regarding nutrition, inter alia, the focus on weight reduction, regarding stress while focusing on shift workers, and regarding physical activity in the topics on strength and endurance training: Thus, it should be someone who can anticipate the needs for all fields. Someone who knows about both nutrition and psychology as well as physical activity. (Provider representative) I also know [ . . . ] that 50% of the people having nutritional goals can then be divided again into eating better and into reducing weight. (Social insurance agency representative) Of course, that which is really important; important from our view point, is what I’ve always described as psychomental stress. People do a whole lot of overtime [ . . . ]. And it’s extremely important to be able to deal with the stress at work. (Company doctor)
Health Coach: Skills and Competencies
Therefore combining therapeutic knowledge with pedagogic skills already guarantees success. (Social insurance agency representative)
Regarding the skills and competencies of a health coach, the participants frequently mentioned the concept of hard and soft skills and their combination. Most participants only alluded to the hard skills and focused on the soft skills. The researchers inductively grouped the soft skills into three categories: personal, methodological, and social.
Regarding the personal soft skills, nearly all the participants identified the need for a coach who is authentic and able to motivate. Further personal soft skills should be good self-management, friendliness, show a zest for life, and have had life experience.
The methodological soft skills of mediation and problem-solving were also seen as desirable.
Ideally, coaches should also display organizational talent and good management skills and possess a conceptual overview of the intervention: Solving problems. We keep having talks about problem-solving issues. That is, one has to be able to endure it and, at times, also be able to cope with adverse situations. (Social insurance agency representative)
Most of the statements focused on social soft skills. Nearly all participants said that the health coach should be empathic. Further social soft skills and abilities that were cited included the following: effective relationship management, ability to create a team spirit, good communication and conversational skills, knowledge of human nature, and the ability to approach other people in an open-minded way: Of course, he must be very empathic because he must succeed in being close to and demonstrating great openness towards the participants. Yet, one opens up in private [ . . . ]. Well, if the health coach is not successful in being close and building trust, then he will also not be accepted and will not accomplish anything. (Human resources department employee) I think that a good health coach is characterized by knowing both what he is particularly good at and also where his shortcomings are. And then, to whatever point he takes someone, they can say, now at this point I need support. (Social insurance agency representative)
Health Coach: Qualification and Education
The general statements were heterogeneous regarding the perceived qualification and education of a health coach in a workplace setting. For some participants, the qualifications and education of a health coach were largely unimportant: That’s difficult to answer. It is an interdisciplinary set of skills and is therefore difficult to say. There is no training that embodies this skill-set. (Human resources department employee) For this reason, I don’t think about a specific training. However, I think one must also demonstrate a very high level of commitment. And also be prepared to familiarize oneself with other topics which lie outside the narrow training course. (Company doctor)
Yet most participants answered the question by naming completed vocational trainings which are not preferred, for example, artisan or an administrative employee, or by naming concrete vocational trainings. Many said that a health coach should have been educated in a physical activity field such as sports science or physiotherapy. Others wanted the health coaches to have pedagogical training: Thus I would just find [ . . . ] that the pedagogic basic requirements are important. In my opinion, a sport therapist [ . . . ] as well as a psychologist, or an educator actually fulfils these requirements. (Provider representative)
Besides the wish for a completed special vocational training, the participants demanded an additional training for a health coach: A second conclusion would be that I’d also like to see a health coach with dual qualifications. I’d also like a university graduate with perhaps an additional qualification in coaching or with a vocational training. (Social insurance agency representative) One could then provocatively say that we’ll discuss this again in a few of years if this exists as a training; that one is then trained. Thus one has a basic training, pedagogical, or sport-therapeutic, or whatever, and then trains as a health coach. (Provider representative)
While answering the question, many participants spend a long time thinking about their responses. Quite a few sought for a clearer definition of what constitutes an education as a health coach: Here, one should perhaps also look again at what abilities they provide. Perhaps one must more clearly define who is suitable and who isn’t. (Provider representative)
Context of Health Coaching Sessions
This theme covers the when, where, and how health coach sessions occur. According to the extent, the statements of the participants were heterogeneous and ranged from one contact every 2 weeks to one per 3 months. The answers were not formulated very precisely and the question was quickly passed over. Potential locations for the work of health coaches included companies, fitness studios, rehabilitation centers, and employees’ home. It was desirable that the health coach becomes active not only in one setting but also in different settings.
The style of engagement of the coach and mode of delivery of the coaching were discussed by the participants. It is possible for a health coach to provide input through individual and group coaching, face-to-face or by telephone and email. Participants mentioned individual and group meetings most frequently. Many expressed the view that a health coach should offer both individual and group options, although they emphasized group meetings in particular. Their responses describe the advantages and disadvantages of each approach: Thus, it should also be possible to have individual discussions so that one also establishes personal ties because, in individual discussions, one also experiences things [ . . . ], which one would simply not believe that one can experience. (Company doctor) One already knows the phenomenon of group dynamics. And that is exactly what it is. Thus the group members are motivated when they have this fixed appointment and when they know they will run into others here. Thus it operates sure enough via the group. This regular participation. (Health coach)
Also, according to the use of the new social media as a communication channel for a health coach, participants gave various statements: I believe that the electronic communication will be used more and more. That is, the use of modern media to keep in contact. That will certainly be the future or the trend for the future. (Social insurance agency representative) Although we live in the 21st century, nevertheless not everyone has a mobile phone let alone an Internet connection. (Employee)
Discussion and Conclusion
According to our findings, the participants agreed that a health coach in the workplace setting should motivate the employees to achieve individualized, internally developed goals and sustain a health-oriented lifestyle modification. The work of a health coach should be to provide information about physical activity, nutrition, and reducing substance addiction. Many participants also desired that health coaches possess personal, methodological, and social soft skills and that they use a range of approaches to work with clients. It was also highlighted that one aim of the health coach’s work is the long-term maintenance of the client’s lifestyle modification. As the success of a lifestyle intervention is assessed by its sustainability, long-term behavior modification is, in general, also a prior intervention aim (Berendsen, Kremers, Savelberg, Schaper, & Hendriks, 2015).
For the most part, our results align with the broad scope of health coaching definitions and descriptions (Butterworth et al., 2007; Palmer et al., 2003; Wolever et al., 2013). However, the variety of described requirements and expectations shows how complex the role of the health coach is. The heterogeneity of this broad research field has been summarized in several reviews (Hill et al., 2015; Kivelä et al., 2014; Olsen & Nesbitt, 2010; Sforzo et al., 2017). Accordingly, there is still much need for uniform accredited standards defining the training requirements and skills of heath coaches. In the United States, the National Consortium for Credentialing Health and Wellness Coaches (NCCHWC) developed training and education standards and signed an agreement with the National Board of Medical Examiners about developing a national board certification. In 2017, the NCCHWC was renamed the International Consortium for Health & Wellness Coaching (ICHWC; 2018) and tasked with creating new international standards (Jordan et al., 2015). To our knowledge, such consortia do not exist outside the North American continent. In Germany, for example, certifications of health coaches are omnipresent but heterogeneous. The stakeholders’ views in the present study reinforced just how important a standard curriculum for health coach education in the workplace setting is.
Regarding the manner of work, most participants preferred a mix of approaches. This is in line with the results of Kivelä et al. (2014), who concluded that the intervention’s effectiveness improves when the program integrates a combination of different approaches. The integration of technology is positive because of the accessibility of the participants and because of the potential to improve health behaviors (Davies, Spence, Vandelanotte, Caperchione, & Mummery, 2012). Group coaching can create a greater sense of responsibility for health-related goals and is more cost-effective (Armstrong et al., 2013). Participants in the present study reported that interpersonal face-to-face contact was of major importance. Ma et al. (2013) also identified face-to-face contact as the most important component. According to the optimal duration of a health coaching intervention, our findings and those of the current literature are heterogeneous. Olsen and Nesbitt (2010) identified a program duration of 6 to 12 months as one of four key features for effective health coaching, but there are also effective, half-day interventions (Cheng & Chan, 2009).
With regard to the thematic focus on health conditions, our findings appear to contradict current knowledge. The different participants in our study did not mention disease-related topics (Olsen & Nesbitt, 2010; Wolever et al., 2013). They did stress behavioral and environmental changes. The enumerated four topics of the participants corresponded with the area of activity of prevention in Germany (GKV-Spitzenverband, 2017). Also, the frequency of naming the topics is comparable with the frequency of the participation in prevention measures (Schempp & Strippel, 2016). The thematic focus on physical activity received particular emphasis, indicating its importance.
Contrary to the findings of Kivelä et al. (2014) and Wolever et al. (2013), the participants in our study did not mention medical training as a health coach qualification. This is probably due to our focus on workplace settings and on employees who display risk factors but do not have chronic diseases. Nevertheless, the participants preferred special professions, especially academics and mentioned degrees related to sports and movement. Also, to become certified by the ICHWC only a few practitioners are eligible to apply. For example, persons with at least an associate’s degree (Jordan et al., 2015).
With regard to the skills, the results were striking because the participants mainly talked about the soft skills of ideal health coaches. A possible reason for this may be that people are more satisfied with the personal rather than the professional quality of a therapist (Mahapatra, Nayak, & Pati, 2016). If the literature about health coaching mentioned soft skills, these are quite similar to our findings (Collins et al., 2018; Jordan et al., 2015). Nevertheless, the description of the coach in the method of health coaching interventions focuses mainly on the hard skills (Cheng & Chan, 2009; Duijts et al., 2008; Strijk, Proper, van Mechelen, & van der Beek, 2013). Remarkably, qualitative analyses normally show that different stakeholders have differing opinions regarding quality in the field of health care (Grande & Romppel, 2010; Hudelson, Cléopas, Kolly, Chopard, & Perneger, 2008). The current study does not completely confirm these findings because no striking differences were found between the participants regarding the recommendation of a health coach. Only the employees had, at times, differing opinions. To improve the standards and quality of health coaching, feedback from clients and other consumers must be taken into account (Nilsen, Myrhaug, Johansen, Oliver, & Oxman, 2006).
A strength of this study is its use of participants with differing and diverse interests. The qualitative approach offered an opportunity to carry out an in-depth exploration of an unanticipated and complex issue. Here, it is possible to clarify the understanding and to form a detailed personal view (Ritchie et al., 2014). Another strength is the focus on the workplace setting. Health promotion related to chronic disease in employment age and the associated reduction of early retirement and increase in employability are relevant to the wider economy and the society in general (Rice, Lang, Henley, & Melzer, 2011; von Bonsdorff, Huuhtanen, Tuomi, & Seitsamo, 2010). Finally, health coaching accreditation, job content of a health coach’s role, and their working style are all timely and socially and politically relevant.
However, some limitations need to be acknowledged. This was a small-scale exploratory study. It includes a small number of interviews and observations in selected workplaces. These can limit broad generalizations. This study was undertaken in the context where the researchers were already associated with some of the participants who had already cooperated in another part of the AtRisk-project. In addition to this, it was difficult for some of the participants to talk about their wishes regarding the requirement of a health coach because they already knew persons who had acted as a health coach.
Conclusions and Implications
This study determined what different stakeholders desire regarding the aims, tasks, skills, qualifications, methods, and thematic focus of workplace health coaching. The findings can be seen as an important step in establishing criteria for health coaching professional development. Standards for health coaching are necessary: An evidence-based curriculum will improve the quality in this field and thereby legitimate its financing. To reduce the heterogeneity in the field of health coaching, more setting-specific and target-group-specific exploratory studies should be conducted. Further interviews, especially with a diverse range of participants/employees, should be performed.
Implications for Occupational Health Nursing Practice
Occupational health nurses considering the use of health coaches in their organization should know that their role in the workplace setting is to promote healthy behaviors (e.g., physical activity). In addition, the health coach should have personal, methodological, and social skills. When appointing people as health coaches, employers should make sure that the selected person has the skills identified by this study. Moreover, it is useful to always consider the clients’ expectations so that the work of the health coach can be tailored individually to the needs of the clients and to the requirements of the workplace.
Applying Research to Practice
When planning a health coach intervention, it is useful to consider the clients’ expectations so that the work of the health coach can be tailored to the needs of the target work group. A health coach should have personal, methodological, and social skills, such as authenticity, problem-solving competencies, and empathy.
Footnotes
Acknowledgements
The authors wish to acknowledge all stakeholders for taking part in this qualitative study.
Ethics Approval and Consent to Participate
The main study (“The AtRisk-study”) was approved by the German Sport University Cologne Ethics Committee (reference number: 93/2015).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Federal Ministry of Education and Research (BMBF; Grant Number: 01EL1425A).
Author Biographies
Lea A. L. Dejonghe is a PhD student of the German Sport University Cologne and was a research assistant of the Institute of Health Promotion and Clinical Movement Science.
Bianca Biallas is a research assistant in the Institute of Health Promotion and Clinical Movement Science (German Sport University Cologne).
Lorna McKee is part of the Health Services Research Unit and holds a joint position with the University of Aberdeen Business School.
Kevin Rudolf is a PhD student of the German Sport University Cologne and a research assistant of the Institute of Health Promotion and Clinical Movement Science.
Ingo Froböse is head of the Institute of Health Promotion and Clinical Movement Science and of the Center for Health through Sport and Movement (German Sport University Cologne).
Andrea Schaller was professor of the IST University of Applied Science (Düsseldorf) and is now head of the working group physical activity-related prevention research (German Sport University Cologne).