
Abstract
Keywords
“Participants had an expectation to be valued as human beings and engaged in a two-way dialogue about their care.”
Healthy aging is viewed as a desirable goal for the aging process.1-4 Reflecting this, there is no shortage of terminology to describe healthy aging. Building on Rowe & Kahn’s “successful aging model” (1997), 5 recent additions have included “optimal aging,” 6 “productive aging,” 7 “harmonious aging,” 8 and “active aging.” 9 Depp and Jeste’s 2006 review of English-language, peer-reviewed studies that defined “successful aging” in adults over age 60 identified 28 papers with 29 definitions. 10 By 2016, there were over 3000 new scientific articles dedicated to “healthy aging.” 11 While there are distinctions between these terms and their definitions, there is an underlying agreement among researchers and healthcare professionals that healthy aging is complex and multifactorial.12-14 It encompasses physical and psychosocial well-being, as well as social connectedness, adaptation, and meaning.15,16
The extensive literature related to lifestyle medicine (LM) demonstrates that it plays a crucial role in promoting healthy aging through its focus on health behaviors that prevent, treat, and reverse chronic diseases.17-20 However, this published research has focused on clinical outcomes, rather than patient expectations related to lifestyle medicine. Despite the abundance of literature on healthy aging, including the role that lifestyle medicine plays in supporting it, there is a dearth of information about what patients want from their healthcare providers to age healthily throughout their lifespan. A search of the PubMed, Google Scholar, JSTOR Life Science Collection, EBSCO, Sage Journals, and APA PsychInfo databases using a combination of the keywords “lifestyle medicine, healthy aging, patient expectations,” and/or “patient-centered care” found papers related to how lifestyle medicine supports physical, mental, and social well-being20-23; papers focused on shared decision-making between patients and physicians related to disease treatment 24 ; and papers discussing broader perspectives on patient-centered care.25-27 However, none of the studies examined patients’ expectations of how their healthcare providers might support them to age in a healthy way.
Our study aimed to address this gap by exploring the overarching research question: “What do you want from your healthcare provider to age in a healthy way?” While this question wasn’t explicitly focused on lifestyle medicine, its broad and open-ended nature allowed us to uncover whether—and to what extent—participants, unprompted, value lifestyle-based interventions and how much they want their providers to connect them with such approaches. This paper examines these desires from a life course perspective, viewing healthy aging as a continuum across years rather than focusing solely on participants age 65 and older. 28 Understanding patients’ expectations for healthy aging is crucial as it can significantly impact healthcare delivery and patient outcomes.29-31 Research has shown that whether or not their expectations are met can influence patients’ satisfaction with care and their overall health outcomes.29-31 Additionally, aligning healthcare practices with patients’ expectations can lead to more personalized and effective interventions, resulting in better adherence to healthcare providers’ advice. 32
Methods
This study received ethics approval from the Indiana University Review Board (#22140) and the North Dakota State University Review Board (#22410). After completing an online intake form, all eligible participants reviewed and signed an informed consent document before being enrolled in this study.
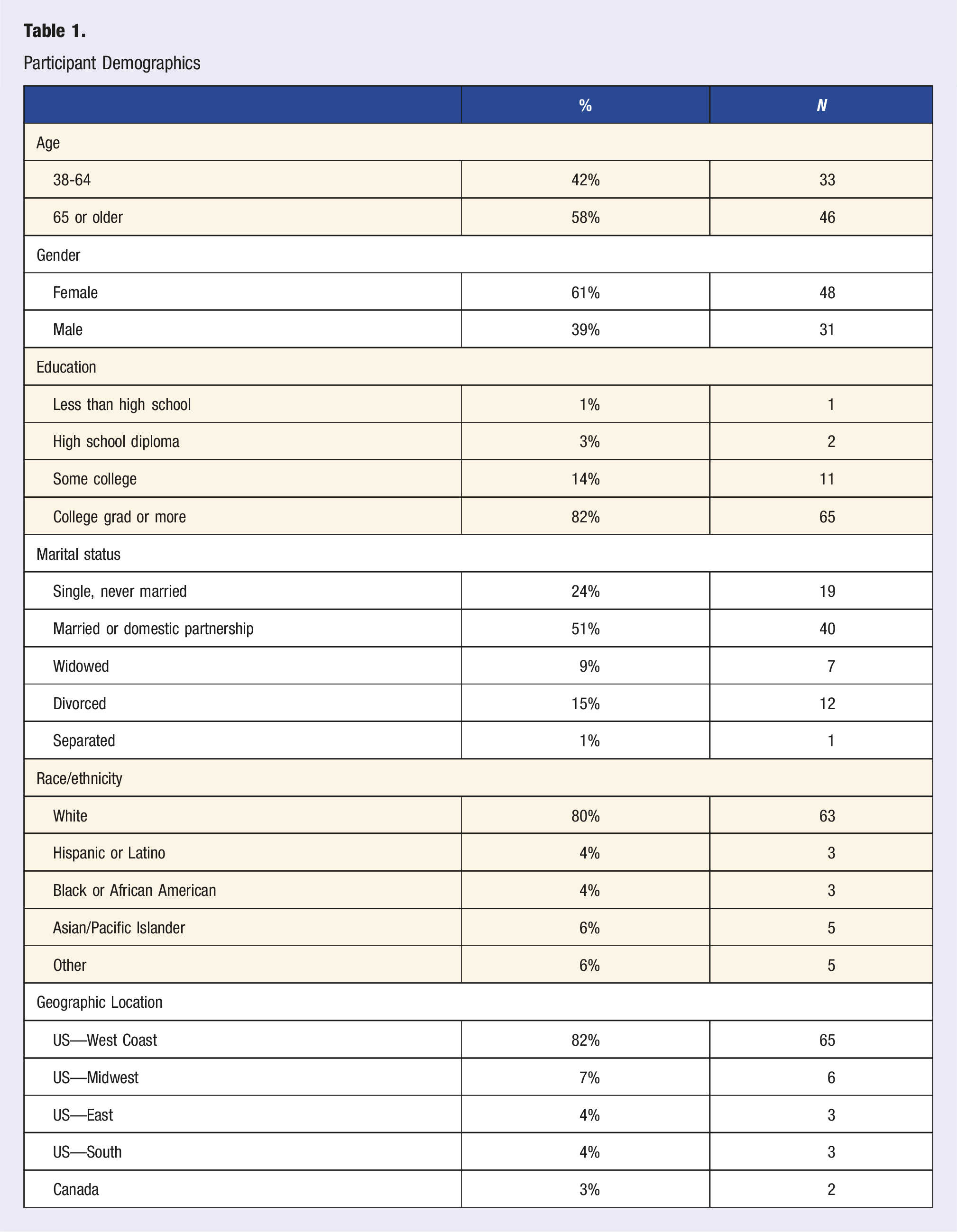
Participants
Participant Demographics
Recruiting Strategy
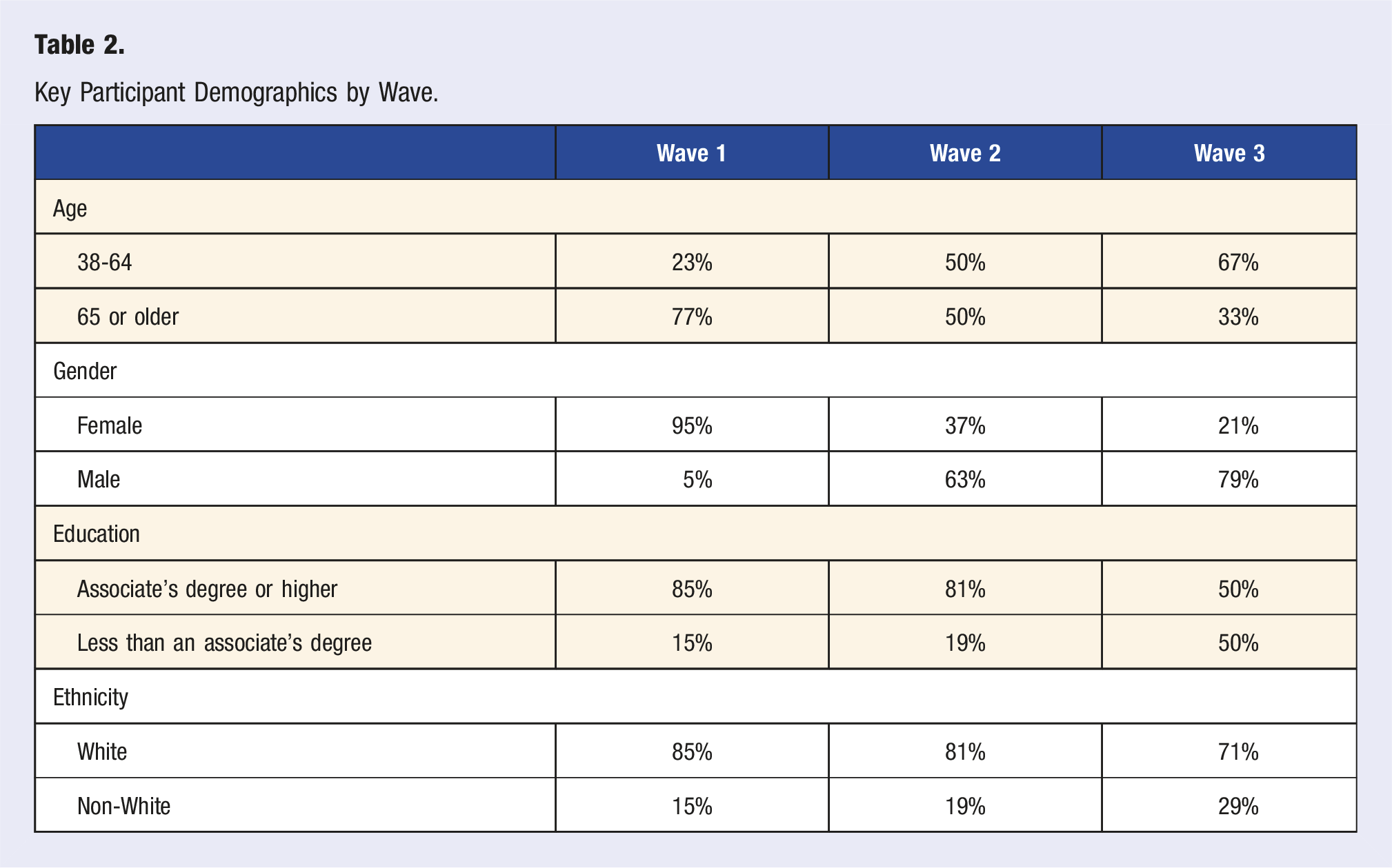
We recruited participants in three waves over a 7-month period using a combination of sampling techniques to capture a wide range of perspectives. In the first wave (Wave 1), we used purposive sampling 33 to recruit individuals from a mailing list of approximately 600 people who subscribed to a healthy aging newsletter. Purposive sampling is widely used in qualitative research to ensure the selection of information-rich sources (i.e., participants) who will provide the most relevant and plentiful data for addressing the study topic. 33 Within the first wave, a total of 47 people completed the study enrollment form, 39 provided informed consent, and 39 enrolled and participated in the scheduled Zoom-based focus groups. The participants who engaged in the Wave 1 focus groups were predominantly white (85%), female (95%), age 65 or older (77%), and had an associate’s degree or higher (85%).
Key Participant Demographics by Wave.
Procedure
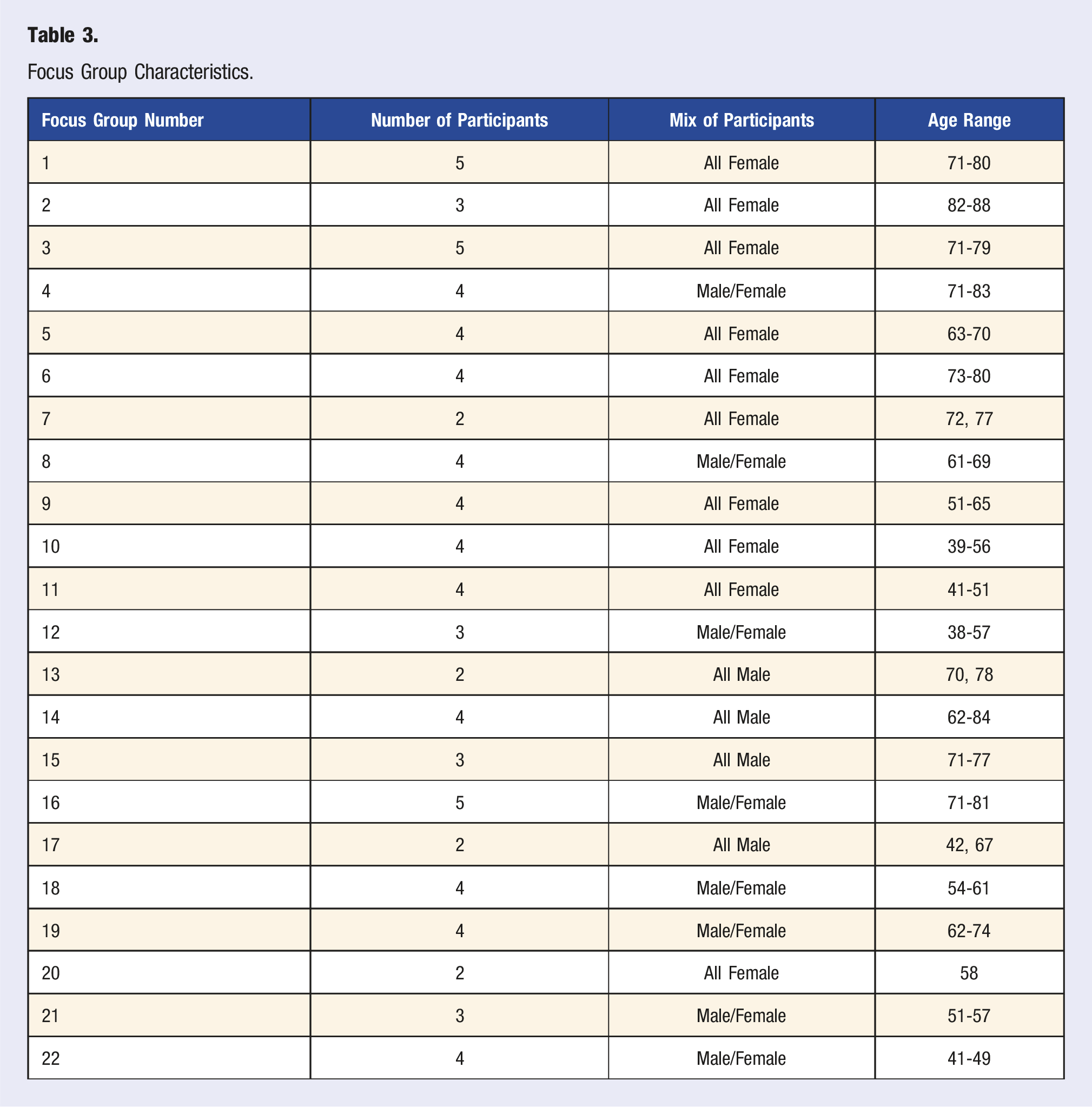
Data were collected during one-hour focus groups conducted by researcher S.D. via Zoom and attended by participants via a personal device (e.g., a personal computer or phone). We selected a focus group format, used extensively in public health research, 37 to bring fresh perspectives through the mutual exchange of ideas, opinions, and critical questioning among participants. 38 Focus groups also provided an opportunity to learn what participants value based on their priorities and experiences, and in their own vocabulary, without the constraint of interviewer/interviewee questions and answers.38,39 The discussion flowed smoothly with minimal disruption or redirection.
Focus Group Characteristics.
All focus group discussions were recorded using Zoom’s audio and video recording software. These audio files were transcribed using Rev.com’s AI-assisted transcription to produce an initial 328-page document of single-spaced data in Microsoft Word. After transcription, S.D. performed minimal editing to correct obvious AI errors. The video files and minimally edited focus group transcripts were uploaded to MAXQDA software, version 24.8, for coding and analysis.
Data Exploration and Analysis
Our analysis focused on examining similarities in responses across all three waves of male and female participants and noting divergent opinions and experiences across the three waves. Data exploration began with a review of the Microsoft Word transcript. Researcher S.D., who holds a graduate certificate in qualitative research and inquiry methods, trained researcher T.U. in the Braun and Clark reflexive thematic analysis process. Together, we applied reflexive thematic analysis to identify key themes in the open-ended responses to the three study questions. In addition, our analysis was guided by feedback from Dr. Jessica N. Lester, Professor of Qualitative Methodology in the School of Education at Indiana University, Bloomington.
Working from the transcripts, researchers S.D. and T.U. independently conducted “unmotivated looking,” 42 an inductive approach emphasizing openness to emerging patterns and phenomena. We each recorded our observations in a summary matrix, organized by focus group, and specific to each of the three guiding questions posed in every session. We then reviewed each other’s matrix entries and developed descriptive codes, first independently and then collectively, aiming to identify a broad range of meanings from more explicit to inferential interpretations. 43 After an initial code set was agreed upon, researcher S.D. applied these codes to the transcripts using MAXQDA software, version 24.8. Multiple codes were assigned to most text segments. In an iterative cycle of verbal and written exchanges, we refined the codes through discussion, debate, and modification. This process culminated in 28 primary codes, which provided a robust and confirmable interpretive structure for the data. (The complete codebook is available from the first author, S.D.).
We grouped the codes into categorical sets to form preliminary themes. S.D. and T.U. then iteratively examined these themes alongside the supporting data, seeking overarching patterns across age, gender, and participant group (e.g., those recruited in Wave 1, 2, or 3). During this refining process, which included deliberation, disagreement, and ultimately arriving at consensus, we further honed the themes and their definitions, focusing on finding commonalities across the groups. This ultimately produced three key themes and supporting subthemes that were consistent across participants in the three waves.
Reflexivity/Validity
We conducted this research within an interpretive framework, understanding that two perspectives would inherently shape our findings: (1) the participants’ viewpoints, informed by their personal interpretations of their experiences, and (2) our perspectives as researchers, which are shaped by the biases, assumptions, and preconceptions that we, as researchers, bring to the research process. 44 One such bias was our existing knowledge of lifestyle medicine, which required us to be vigilant during analysis to avoid inadvertently over-focusing on themes related to this area unless the data supported this. Because reflexive practices were central to our approach, we used memoing and weekly debriefing to reflect critically on our interpretations, noting variability in participant narratives and identifying divergent examples to highlight cases that challenged our initial expectations. 45 Our findings are presented from a strengths-based perspective, which offers opportunities for constructive action rather than focusing on deficits in the current healthcare system, such as limited access to physicians.46,47 While some participants expressed frustration related to physician access, our research is not focused on this aspect.
Findings
Themes, Subthemes, and Supporting Quotes.
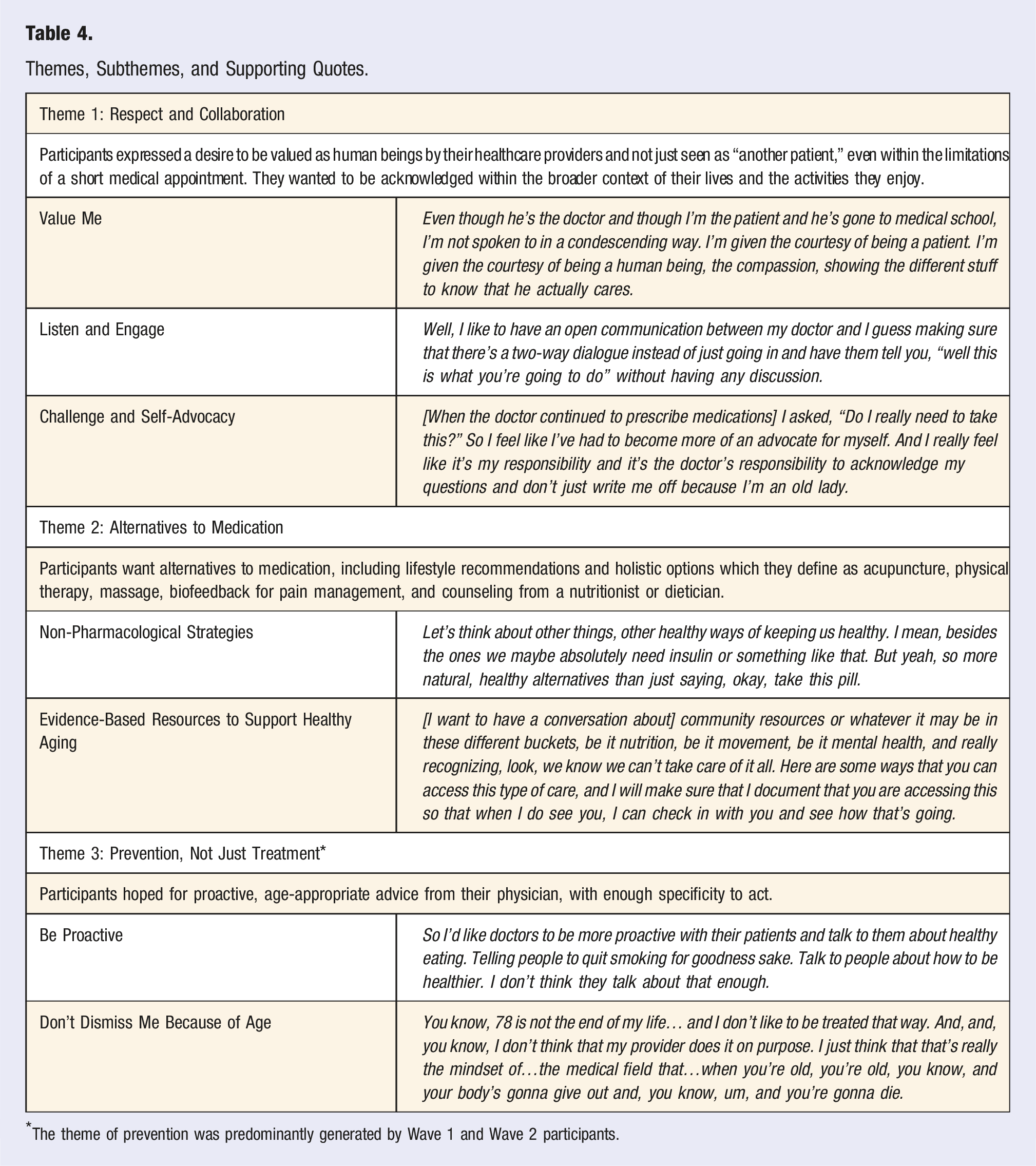
*The theme of prevention was predominantly generated by Wave 1 and Wave 2 participants.
To enhance transparency and provide context for each subtheme, we have documented the frequency of occurrence across focus groups and the total number of participant comments (e.g., n = 10 focus groups, 30 comments). For clarity, we have condensed some verbatim comments using ellipses and provided summaries in brackets to maintain the essence of participants’ narratives while ensuring readability. The selected quotes represent a diverse mix of ages, genders, and participants across all three waves.
Theme 1: Respect and Collaboration
Participants expressed a desire to be valued as human beings by their healthcare providers, rather than being seen as “just another patient.” This encompassed wanting genuine respect and collaboration, as well as being able to comfortably challenge or question the healthcare provider’s authority when it was in their best interest. While the theme of respect and collaboration is not directly tied to achieving healthy aging, participants felt that being valued as a person was fundamental to a positive patient/provider relationship, including supporting them in aging in a healthy way. This perspective established a foundational standard for how participants expected to be treated by their healthcare providers, setting the stage for more comprehensive and nuanced discussions regarding healthy aging.
Value Me
A frequent subtheme was the desire to be valued as a human being and not just to be treated for an illness (n = 16 focus groups, 30 comments). Participants emphasized that “it’s nice to feel that person cares rather than you’re just a 10-minute slot in their day” (Participant #11, female, age 71). Participants wanted to be acknowledged within the broader context of their lives and the activities they enjoy. They sought healthcare providers who genuinely cared about them, recognized their value as a person, and were invested in their healthy aging. As one stated: Like if my knee hurts, I would go to a doctor who knows about knees, but I would want him to see me as a whole person and to figure out how my problems with my knees affect my whole life. (Participant 10, female, age 79)
Listen and Engage
Participants expressed the desire to be heard and to engage in a two-way dialog with their healthcare provider (n = 14 focus groups, 31 comments) instead of “just going in and having them tell you, ‘Well, this is what you’re going to do,’ without having any discussion” (Participant #63, male, age 61). Participants praised healthcare providers who did not dismiss their concerns but genuinely listened and encouraged them to participate in decision-making related to medications, treatment, or follow-up care. “Being heard” was of utmost importance to participants, many of whom expressed concern that their healthcare providers were “just trying to shoot off their message” (Participant #42, female, age 47).
Participants also described the limits on appointment time as a reason for healthcare providers not listening or engaging. As one participant said: “And it just felt like you wouldn’t dare ask a question because that would take minutes and they don’t have minutes” (Participant #66, male, age 54). The desire for engagement and dialogue was fueled, in part, by patients conducting their own internet-based research related to health, well-being, and medical conditions and wanting to discuss their findings with their providers (n = 15 focus groups, 32 comments). Participants’ reasons for doing their own research varied and included wanting to be a proactive partner with their healthcare provider and a lack of trust that their provider would provide a solution, especially related to a chronic condition. Their reasons also included finding alternative treatments that their healthcare provider might not have offered, which is also related to Theme 2. Participants expressed hope that their healthcare providers would be open to receiving this information, while acknowledging that this was not often the case. [Being proactive about my health] means having the partnership with my doctor, going and talking and knowing what you're talking about, what the options are out there. Sometimes doing some of the legwork myself and just kind of running it past them, but you also have to find someone who's willing to listen when you do that. Someone who is going to actively consider where you're coming from. Because if they can help me base my healthcare off of what works for me best and what my situation is and not just what they think they should be prescribing, I'm going to have a better health outcome. (Participant #73, male, age 57.)
Participants underscored the importance of being heard and actively involved in their healthcare decisions to enhance their personal health outcomes, particularly as they increasingly drew upon internet-based resources to guide these discussions.
Challenge and Self-Advocacy
Participants acknowledged questioning or challenging their healthcare providers and not automatically accepting the advice provided (n = 5 focus groups, 18 comments), which many felt was the norm for prior generations. I just think that we need to question our doctors more, which I don't think is going to be pleasant for doctors. We have to reset expectations. We have to reset our engagement. I just don't think as these younger generations, unlike our parents, our grandparents, we can't just think, oh well the doctors are gods and everything they say is right because it doesn't work like that anymore. (Participant #34, female, age 53)
The concept of questioning healthcare providers was tied to self-advocating for the course of treatment that participants thought best, although the phrase “self-advocating” was used primarily by Wave 1 and Wave 2 participants. In contrast, some Wave 3 participants expressed this as “fighting for” what they thought was best. Self-advocacy was connected to having a sense of control and was based on information shared by others, one’s own research, and/or a lack of trust in one’s healthcare provider. One participant described this sense of distrust as: I’ve heard stories at a Mayo Clinic where some doctors have made mistakes and I mean, we have to be our own advocates and we have to research and speak up like you said, you had to do [it] because they're not going to do it. So we have to take control of ourselves and hopefully find some good doctors that you can talk to. (Participant #24, female, age 80)
Theme 2: Alternatives to Medications
Participants expressed the desire for alternatives to medication, including lifestyle-related recommendations that would help them age in a healthy way.
52
In response to the two opening questions posed at the start of each focus group session: “What is one thing you love to do?” and “What is healthy aging?” participants shared lifestyle behaviors they were already practicing. Participants reported engaging in physical activity (n = 21 focus groups, 76 comments); social activities (n = 19 focus groups, 90 comments); healthy eating (n = 18 focus groups, 28 comments); activities to promote mental well-being (n = 12 focus groups, 23 comments); getting sufficient sleep (n = 6 focus groups, 8 comments); and avoiding drugs and alcohol (n = 4 focus groups, 5 comments). Despite having disabilities and chronic diseases, participants acknowledged trying to maintain behaviors that contribute to healthy aging. As one stated: Well, I walk using a cane and I pretty much persevere through it because at the store, that's kind of my exercise and I do my darnedest and never have to use the sit down cart because [I’d] much rather walk because I feel okay, yeah, it's going to be painful, but I just keep doing it and I'm trying to use less Tylenol. (Participant #72, female, age 58)
Engagement in these health-promoting behaviors was associated with an expectation for information about non-pharmacological treatments to support healthy aging., Participants wanted healthcare providers who, instead of leading with medication advice, would “be a little more accepting of those kinds of treatments that don’t necessarily rely on popping pills” (Participant #73, male, age 57).
Non-Pharmacological Strategies
Participants wanted their healthcare providers to provide alternatives to medications (n = 12 focus groups, 38 comments). While they recognized that some prescription medications were necessary, many felt that providers rarely discussed other options unless patients already knew to ask about them. What I would like a doctor to do is to offer alternatives. You know, I had a bone density test…and the drugs that are available right now are not anything I'm willing to do. So, when my doctor said, oh, I think it's time to start this drug, I looked at her and I said, what else can I do? Because I'm a hundred percent certain I am never going to take that drug. And all of a sudden, I get a list of all these things I can do that doesn't include taking a pill. But why could that not have been offered to me as an alternative? She wouldn’t have even offered if I hadn't had as much knowledge about that particular drug. (Participant #4, female, age 75.)
Participants also wanted suggestions of alternatives related to lifestyle behaviors, and guidance on how to adopt these behaviors, paired with appropriate follow-up. Beyond general advice like “exercise more,” they hoped their providers would check in with them, offering both encouragement (“It’s good you’re going to the garden”) and accountability (“What’s keeping you from going hiking or walking?”) (Participant #64, male, age 60). One pre-diabetic participant said he needed a “kick in the pants” to remind him that “I need to take care of this now” (Participant #46, male, age 38). Expectations related to follow-up were based on the belief that their healthcare providers would recall and reinforce earlier discussions related to lifestyle behaviors.
Participants expressed a desire for “holistic” or “natural” options as an alternative to medications (n = 7 focus groups, 11 comments). They did not have a specific definition for these terms, but mentioned acupuncture, physical therapy, massage, biofeedback for pain management, and counseling from a nutritionist or dietician. Participants’ concerns were centered on physicians’ unwillingness to consider these methods (or provide referrals) and the limited availability and high out-of-pocket costs of holistic services. One participant described this as: [It’s not] just giving us meds. Let's think about other things, other ways of keeping us healthy. I do appreciate the fact that [my healthcare center] does have acupuncture, and they have the dietician, so they do have more homeopathic avenues of care, but sometimes it can take a long time to get in to see them. So more natural, healthy alternatives than just saying, okay, take this pill. (Participant #72, female, age 58).
Participants expressed a need to conduct their own research on alternative strategies and bring these findings to their healthcare providers. This reinforced the findings in Theme 1 regarding self-advocacy. Participants appreciated the need for some prescriptions but hoped for greater openness, accessibility, and regular encouragement from their healthcare providers when considering non-pharmacologic approaches.
Evidence-Based Resources to Support Healthy Aging
Participants expressed a desire for connection and access to resources to support healthy aging (n = 10 focus groups, 32 comments). While wishing for more time with their healthcare providers, they also acknowledged the practical constraints of brief medical appointments. Within these limitations, participants valued healthcare providers who act as trusted advisors, directing them to evidence-based information and connecting them to a broader network of resources for achieving healthy aging.
Some participants acknowledged that, although they conducted their own research, including research on lifestyle-related alternatives, they were unsure about what to believe. But see, I could easily Google…75 different diets that people will swear are going to make me healthy for many, many, many, many years. And they're not, who knows? Some of that information is really valid, but…how can I assess what's good and what's bad? (Participant #31, male, age 61).
Participants did not expect their healthcare providers to “know it all,” but rather to provide them with access to vetted information. They also wanted this information earlier in their life stage to help them prevent disease and age-related decline. Give us tools, podcasts, information, books, any such information would be helpful. Help me prevent it, just like my pre-diabetic situation, so I would have known years ago what I could have done to prevent this. (Participant #35, female, age 58)
Building on their desire for evidence-based information, participants sought referrals to allied health professionals (e.g., nutritionists, registered dietitians, physical therapists, clinical exercise specialists) who had been vetted by their healthcare providers. Participants wanted resources who would proactively foster healthy aging and help avert functional decline, not simply treat a medical condition such as diabetes or post-surgery recovery. As one participant said: I want one stop where I get off the bus here and they point me to all of those things [I may not know I need.]. I may not know that I need to see a nutritionist. I may not know that I need to see an exercise professional. I don't expect my doctor to be the expert on all those things. But I want somebody kind of playing traffic cop. (Participant #31, male, age 61).
Some participants acknowledged the importance of additional resources while simultaneously describing barriers to access, especially related to cost. As one participant stated: “If we have limited income, what else is out there and available for us?” (Participant #79, male, age 40). Participants also described the importance of connection to others who had experienced similar challenges—that is, to “hear other people’s voices and how they’ve navigated the system” (Participant #77, female, age 49).
These insights about evidence-based resources reflect participants’ dilemma of conducting their own research, yet feeling overwhelmed by conflicting advice. Participants also highlight the value of physician-vetted referrals to allied health professionals who can extend the care model, while acknowledging barriers, particularly cost and accessibility.
Theme 3: Prevention, Not Just Treatment
Participants sought proactive, age-related information that would help prevent disease and disability. However, the word “prevention” was used primarily by Wave 1 and Wave 2 participants (n = 9 focus groups, 25 comments); it was only mentioned once by Wave 3 participants (n = 1 focus group, 1 comment). Participants who discussed prevention hoped for proactive, age-appropriate advice from their healthcare providers that was specific enough to guide them to take action.
Be Proactive
Participants who talked about prevention said they did not want to be “laden with medications to cure something that we could have prevented when we were in our thirties, forties, and fifties” (Participant #35, female, age 58). Similar to the finding in Theme 2, in which participants expressed “not knowing what we don’t know,” participants hoped that their healthcare providers could help them consider the actions they needed to take, and at what life stage, to help them age in a healthy way. I want a doctor who says, ‘Okay, at this age, here are the things you need to be thinking about.' And I don't care if he or she tells me that every single year. Here are the things that are going to change your life, that are going to expand your health span if you focus on these. And my doctors over the years have said things like, you need to eat well and exercise. We all know that. But I don't know what that means. Why is that important at this age? (Participant #31, male, age 61).
As noted in Theme 2, participants did not expect healthcare providers to “know it all” or “do it all” but to be aware of important age-related preventative strategies and provide guidance, even if that meant a referral to another provider. Rather than a one-size-fits-all approach, participants hoped that their healthcare provider would “understand, in our stage of life development, we may have different needs, desires, and certainly different physiology” (Participant #2, female, age 75) and advise accordingly.
Don’t Dismiss Me Because of Age
Both younger and older participants felt “dismissed” by their healthcare providers due to their age, although this sentiment was only expressed by the Wave 1 and Wave 2 focus group members (n = 9 focus groups, 10 comments). Older participants felt that their health issues were dismissed as a natural part of aging, diminishing the perceived importance of preventative measures. This was expressed by a participant who described her provider’s perspective as: “Oh, honey, it’s just because you’re older,” instead of having her provider “really listen to the issues and what I want to do” (Participant #29, female, age 69). Conversely, younger participants felt their concerns were not taken as seriously because of their youth and overall good health, leading to their providers making less proactive efforts to support them in healthy aging. A younger woman expressed being similarly dismissed due to her age: So they look at someone like maybe any of us like, oh, you're fine. There's nothing wrong with you. You're young, you're healthy. Yeah. Well, compared to the heart attack in the waiting room waiting to happen, yeah, I am pretty healthy, but I also want more, I want to be able to prevent stuff. (Participant #37, female, age 45).
Discussion
This qualitative study examined the expectations of a diverse group of men and women, aged 38-88, regarding what they want from their healthcare providers to help them age in a healthy way. Three broad themes were generated from 22 focus groups with 79 total participants: (1) Respect and Collaboration, (2) Alternatives to Medication, and (3) Prevention, Not Just Treatment. This research addresses notable gaps in existing literature, where concepts such as “healthy aging” and “patient-centered care” are well-defined but fail to capture patients’ perspectives on the specific support they expect from healthcare providers to achieve healthy aging. Furthermore, this study identifies a gap in the literature on lifestyle medicine. These studies focus on the ability of lifestyle medicine to prevent, treat, and reverse chronic disease17-20 and to support healthy aging,48-50 but do not reflect patients’ expectations of their healthcare providers to help them age in a healthy way.
The expectations shared by study participants underscore a shift from the traditional deferential patient-healthcare provider dynamic toward a model in which patients are respected as partners in their care.29,51 Participants had an expectation to be valued as human beings and engaged in a two-way dialogue about their care. This finding is consistent with a 2024 study by Rathert et al., which found that patients’ top criteria for a patient-physician relationship were “feeling heard,” having shared power and shared deliberation, and having the full presence, trust, respect, and emotional support of one’s physician. 27 Although this expectation for respect and collaboration is not exclusively linked to aging, participants said that this support was essential to their achieving healthy aging. This is understandable, given that older adults may not feel as valued as they did when they were younger 52 and often perceive themselves to be “expendable and disposable,” especially in terms of healthcare. 53 Patient-centered research shows that—across the range of patient ages—respectful and collaborative relationships enhance patient satisfaction, empower patients to engage actively in their care, enhance compliance with both lifestyle and medication recommendations, and improve health outcomes.29,31,54,55
When describing their ideal type and degree of collaboration with healthcare providers, participants emphasized the importance of questioning physicians when necessary and advocating for what they believed to be the best course of action. This advocacy was often informed by their own internet-based research, reflecting the growing accessibility of health information online. Such participant-driven research is unsurprising within the context of an “infodemic” fueled by increasing consumer interest in holistic approaches, self-care, and preventative care, and wide access to online information. 56 Currently, 93.1% of the US population has internet access, 57 enabling individuals to explore a wide range of topics, including disease definitions, symptoms, diagnoses, medications, alternative therapies, and the role of lifestyle choices in maintaining health. Since the advent of “Dr Google” in 2010 and the introduction of tools like ChatGPT in 2022, an estimated one-third to 70% of patients in the U.S. now search the internet before consulting their physician, often using this information to prepare for their appointments.58,59 Despite their internet-based research, participants in our study admitted to being confused about what to believe and sought guidance from their healthcare provider as to what alternative strategies were most effective. This highlights the crucial role of healthcare professionals in guiding patients to reliable, evidence-based resources that support informed decision-making.67,68
Although the term “lifestyle medicine” was not explicitly mentioned by participants during the focus group discussions, nor did the researchers specifically ask about lifestyle medicine, two of the study’s themes, Alternatives to Medication (Theme 2) and Prevention, Not Just Treatment (Theme 3) highlight patients’ interest in lifestyle medicine practices to support healthy aging. Study participants were clear that they wanted the type of treatment options that lifestyle medicine provides, including non-pharmacological alternatives and lifestyle guidance, particularly related to nutrition and physical activity.
Participants also expressed a desire for their healthcare providers to recommend options such as acupuncture, physical therapy, and biofeedback for pain management that align with the principles of integrative medicine. 60 This holistic approach to healthcare combines conventional medical practices with evidence-informed complementary and alternative therapies to address the interrelated physical, mental, emotional, social, spiritual, and environmental aspects of health. 60 When making recommendations, healthcare providers should be aware that many complementary and alternative therapies, such as acupuncture, may not be covered by patients’ health plans, making them out of reach for many.61,62 Other therapies may not be a realistic option, that is, for those who lack access to transportation and those with mobility challenges, similar to other access to healthcare. 63
Building on their interest in alternatives to medication, participants emphasized the need for preventive strategies to support healthy aging. It’s worth noting that the word “prevention” came up frequently among Wave 1 and Wave 2 participants but was only mentioned once by a Wave 3 participant. Participants who discussed prevention wanted clarity on which health behaviors—practiced at specific points in life—would help them age well and avoid chronic diseases or disabilities that could limit them later. Participants weren’t looking for vague advice like “eat better” or “exercise more.” Instead, they sought specific, actionable guidance tailored to their life stage. This aligns with recent studies highlighting the demand for personalized, life-stage-specific guidance in preventive care.64,65 The desire to age in a healthy way was expressed by participants of all ages. The validity of this aspiration is supported by research indicating that adopting healthier lifestyle behaviors earlier in life can significantly reduce premature mortality and enhance quality of life throughout the lifespan.48-50,66,67
Participants commented that their healthcare providers were not offering age-related preventive strategies. They also acknowledged that they did not expect their providers to have the expertise or time to “do it all.” Instead, participants expressed a desire for referrals to evidence-based resources, community providers, and other professionals who could offer lifestyle counseling and proactive guidance aimed at helping them maintain good health rather than merely treating disease.68-70
Concerns were also raised about being “dismissed because of my age,” particularly regarding preventive options. While previous studies have documented dismissive attitudes toward older adults in healthcare settings, 71 a novel finding in our study was that younger, healthy adults reported similar experiences of being dismissed based on their age. Both older and younger adults felt that preventive treatments were overlooked because they were perceived as either “too old” or “young and healthy.” This suggests that the issue may not be specific to the patient’s age but may instead reflect broader systemic gaps in the understanding of the impact and value of lifestyle medicine across the lifespan.64,65
Implications
Assuming participants are representative of the patient population in general, the findings of this study have significant practical implications. These include improving healthcare providers’ understanding of, and ability to meet, patient expectations and supporting patients of all ages in healthy aging. Across the lifespan, participants sought to be actively involved in achieving their own healthy aging, and they expected their providers to support this. This points to an opportunity for healthcare providers to support patients in having better health outcomes by aligning their practices to deliver patient-centered care that meets patients’ expectations. This would include fostering active patient involvement in achieving healthy aging and expanding access to allied health professionals and community partners who are cost-effective and support prevention via lifestyle medicine. These collaborative approaches can improve patient outcomes and address the limitations in the time that healthcare providers have to spend with patients.
For lifestyle medicine practitioners, this study highlights the growing demand for evidence-based lifestyle guidance in conjunction with conventional treatments. With the increasing burden of chronic disease, the therapeutic use of lifestyle changes emphasizing nutrition, physical activity, stress management, and other behaviors should serve as a cornerstone of care. 72 Scalable models, such as reimbursable group medical visits (GMVs) that incorporate education about and practice of lifestyle medicine alongside clinical care, and community-engaged lifestyle medicine (CELM) programs, such as clinical/community partnerships where patients are referred to community-based programs, offer promising solutions to support sustained behavior change.68,70,73,74 Further research is needed to explore how evidence-based strategies such as these can effectively enhance healthspan and longevity.
Strengths and Limitations
This study has strengths that enhance its contribution to understanding patients’ expectations of healthcare providers in supporting healthy aging across the lifespan. The diverse participant sample, which included representation from both genders (male/female), a 50-year age range, and varied demographics, strengthens the generalizability of the findings. Focus group discussions provided rich, detailed narratives that offered comprehensive insights into patients’ perceptions and feelings about the role of healthcare providers in promoting healthy aging. The moderator posed just three open-ended questions, which enabled the participants to engage deeply in the discussion. The small number of participants in each group supported thoughtful and thorough discussion of each of the three questions. The use of reflexive thematic analysis and multiple rounds of review and discussion between the researchers helped avoid bias in interpreting the focus group discussions. However, several limitations should be considered when interpreting these findings. The sample consisted primarily of English-speaking, educated individuals who were engaged in their health, which may have introduced bias in their expectations regarding healthy aging. Additionally, although the study included a relatively large sample, the thematic analysis primarily focused on identifying commonalities, thereby limiting the exploration of nuanced differences among subgroups. Furthermore, demographic data collection was intentionally limited to reduce barriers to participation. This constraint restricted the ability to conduct more granular analyses and may limit the generalizability of the findings to diverse subpopulations.
Future research should aim to address these limitations by collecting more comprehensive demographic and contextual data, as well as employing targeted sampling strategies. This would enable deeper exploration of how factors such as socioeconomic status, health status, and insurance coverage influence patients’ expectations of healthcare providers in supporting healthy aging throughout the lifespan.
Conclusions
This study provides valuable insights into patients’ expectations of healthcare providers in supporting healthy aging across the lifespan. Regardless of age, participants emphasized the importance of respectful, collaborative relationships with their providers, a desire for evidence-based alternatives to medication, and access to proactive, age-appropriate preventive strategies. These findings highlight a shift toward patient-centered care models that prioritize shared decision-making and the integration of lifestyle-based interventions. Addressing these expectations has the potential to improve patient outcomes, enhance satisfaction with care, and promote healthy aging across diverse populations.
Footnotes
Acknowledgments
Jessica N. Lester, PhD, Heather Fuller, PhD, Michaela Hayes, MHSA, and Noriah S. Zaragoza, BS
Author Contributions
Conceptualization, S.D.; research, S.D. and T.U.; analysis, S.D. and T.U.; writing—original draft preparation, S.D., writing—review and editing, S.D. and T.U.; supervision, S.D. All authors have read and agreed to the published version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Data Availability Statement
Our data file with de-identified data is stored in the OSF data repository at OSF.IO.