
Abstract
The increasing demand for health coaches and wellness coaches in worksite health promotion and the marketplace has resulted in a plethora of training programs with wide variations in coaching definitions, content, attributes, and eligibility of those who may train. It is in the interest of public awareness and safety that those in clinical practice take the lead in this discussion and offer a reasonable contrast and comparison focusing on the risks and responsibilities of health coaching in particular. With the endorsement of the American Association of Occupational Health Nurses (AAOHN), the National Society of Health Coaches, whose membership is primarily nurses, discusses the issue and states its position here.
Keywords
Introduction
As health care reform in the United States steadily moves the pendulum from sickness and disease to wellness and prevention, new interventions have arisen in the name of coaching to guide and thus improve the life, health, and health risk of individuals. Although a number of “coaching” types and modalities exist, for example, health, wellness, personal, and life coaching, health coaching and wellness coaching have received substantial attention and are considered to be most closely associated with affecting positive health behavior change.
Herein lie the questions that have arisen among health care providers and health professionals. Is there a difference between health coaching and wellness coaching? If so, what is this difference? Should there be a difference? What should the qualifications be for those providing these services? What are the risks and responsibilities involved? What should the patient/client expect to gain from enlisting such services? This discussion seeks to answer these questions and to move the debate toward a higher degree of resolution from which to frame a consensus definition of health coaching, and to guide practice and research.
Background
Active health promotion through lifestyle changes emerged in the 1950s and spawned the wellness movement in the 1970s (J. W. Miller, 2005) in worksite health promotion. The term wellness was generally accepted to indicate a state of well-being, the absence of illness. Large automotive companies were some of the first to institute employee wellness programs (Yen, Edington, McDonald, Hirschland, & Edington, 2001). As wellness continued to evolve, the term also expanded in the early 2000s to include coaching individuals to maintain healthy lifestyles.
As health care costs continued to spiral upward, it was recognized during this same this time that individuals with chronic conditions and health risk(s) could possibly benefit from coaching, with the focus being not only on wellness but also on the health of the individual. With this shift, the term health coaching was spawned. Articles about health coaching were evident as early as 2000 and have increased all the more since 2008 (Olsen, 2013).
Differentiation of Health Coaching From Wellness Coaching
The National Society of Health Coaches (NSHC) has long supported the premise that health care professionals are best suited to guide or coach individuals with chronic conditions and those with moderate to high health risk (C. Miller, 2014). Olsen (2013) stated from an extensive review of the literature that health coaching primarily falls within a nursing scope of practice, with nurses being the most commonly cited professionals administering health coaching and evaluating its effectiveness.
Kreisberg (2015) distinguished health coaching from wellness coaching in this way: “Health coaches work with persons who are struggling with health issues that are often chronic. Wellness coaches orient more to prevention and continued wellness. In the medical marketplace, it’s health, not wellness, coaches who are being hired.”
It will require more research to build a widely accepted consensus about health coaching as differentiated from wellness coaching in part due to the explosion of coaching in the marketplace that has caused the lines to blur for some.
In addition, online “dictionaries” and “encyclopedias” have added to the menagerie of definitions, and understandably so, as these resources allow any individual to add personal thoughts and biases to the construct as it exists on the web.
Importantly, it is the clinical professional who has the responsibility, liability, and an oath to protect the best interest of the patient/consumer with regard to health care and, in this developing field, to ensure that the public receive health coaching from qualified individuals who are best suited to safely guide them. With this concept of health coaching and its difference from wellness, the following definitions are framed.
Health Coaching and Wellness Coaching Defined
Health coaching is the use of evidence-based skillful conversation, clinical strategies, and interventions to actively and safely engage clients in health behavior change to better self-manage their health, health risk(s), and acute or chronic health conditions resulting in optimal wellness, improved health outcomes, lowered health risk, and decreased health care costs (Huffman & Miller, 2015).
Wellness as defined by Mirriam-Webster (Wellness, 2016) is the quality or state of being healthy; or in good health, especially as an actively sought goal. Manderscheid et al. (2010) for the Centers for Disease Control and Prevention define wellness as the degree to which one feels positive and enthusiastic about life. It can therefore be reasoned that wellness coaching is guidance and inspiration provided to otherwise “healthy” individuals who desire to maintain or improve their overall general health status, which often includes smoking cessation, increased physical activity, eating well, and general weight management.
Attributes of Health Coaching
Although research about health coaching continues to determine the efficacy and effectiveness of various interventions and who should provide these interventions, individuals who wish to provide health coaching services or simply use health coaching skills in the care of clients/patients are faced with a dilemma. Which coaching education and training allows them to gain the appropriate knowledge and skill to guide patients/clients to achieve the best or most appropriate health outcomes possible, either within a patient–provider coaching relationship or the simple use of health coaching skills in a brief clinical encounter at the point of care?
The following attributes of health coaching are derived from clinician coaching practices (Huffman, 2014; J. W. Miller, 2014; Olsen & Nesbitt, 2010), from a systematic review of 284 peer-reviewed articles in health care literature by Wolever et al. (2013), and from a concept analysis of 215 articles conducted by Olsen (2013). These attributes are mentioned in varying degrees and collectively provide the most complete compilation the NSHC has to date. These attributes are
client-centered, self goal-directed process
health-focused, evidence-based practice interventions for those with chronic conditions and/or moderate to high health risk(s)
health teaching
client autonomy
client empowerment and self-discovery
collaborative partnership
client engagement
motivational interviewing
health outcomes measurement
client accountability
nurses most commonly cited as health coaches
evaluating its effectiveness
Health Coaching Qualifications and Skills
The NSHC strongly takes the position that health coaching be no less than evidence-based and conducted by licensed/credentialed health care professionals who have the clinical education and training to safely guide patients/clients with acute or chronic conditions or moderate to high health risk. (see Figure 1)
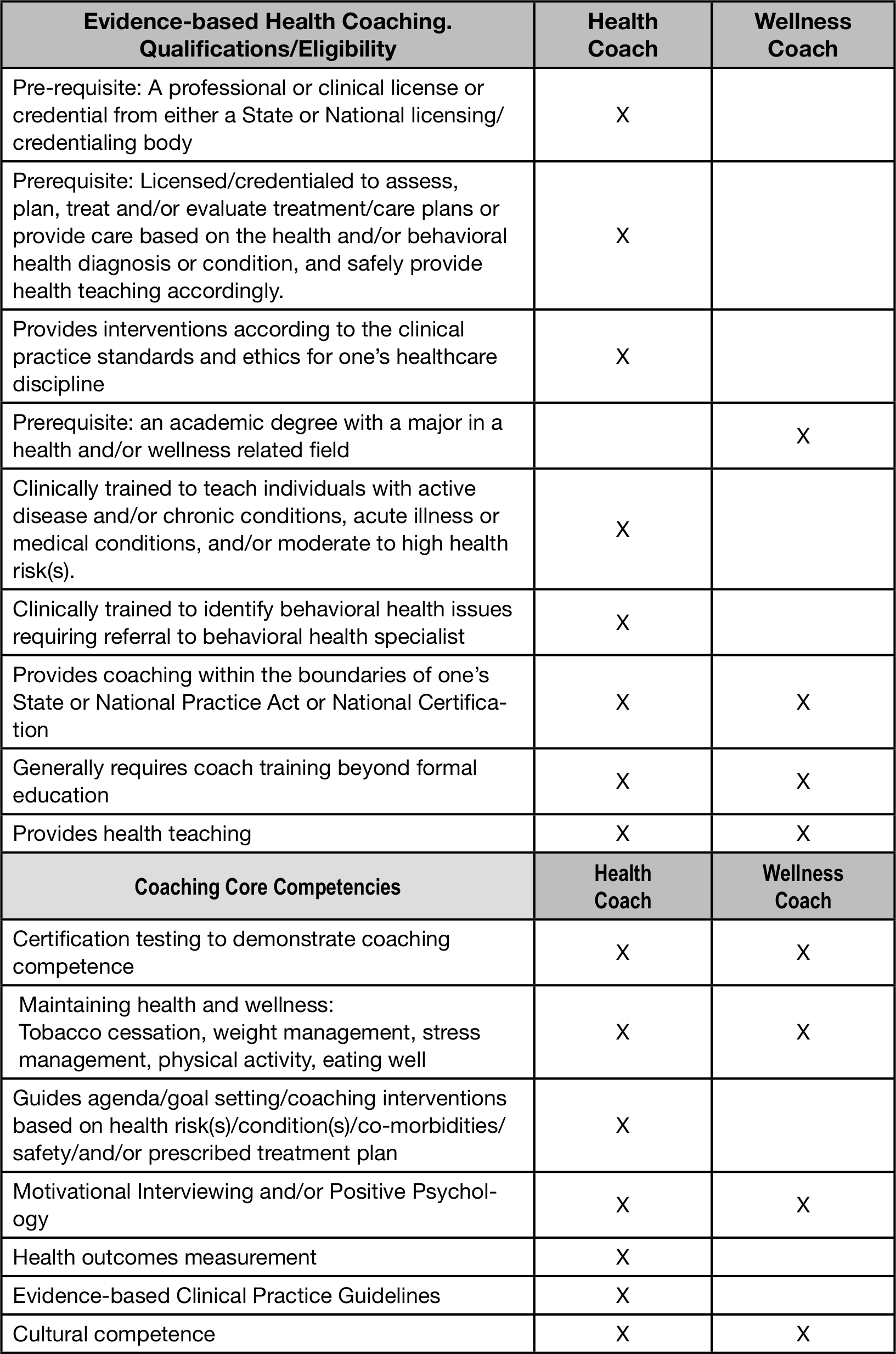
Health coach qualifications and skills.
By virtue of health care professionals’ active, unencumbered licenses/credentials, which guide health management or medical/nursing interventions within their professional scope of practice, they have accountability and liability for their professional clinical actions. This is especially critical in the interest of consumer awareness and safety.
Recently, the state of Florida passed regulations limiting who may conduct nutrition counseling or teaching due to questionable nutrition-related business practices by non-credentialed individuals. Other states have followed suit. The Center for Nutrition Advocacy (2016) is leading this movement. Health coaching should be no different, given the widespread, explosive business interest driven by the marketplace.
Health Coach Certification is considered an appropriate and acceptable method of recognizing knowledge and skill attainment in the core competencies of evidence-based health coaching. However, a lack of consensus about who is qualified to test for this credential and what the educational content for the credential should be still exists.
The NSHC limits the pool of qualified individuals to those with an active/unencumbered clinical license/credential to assess, treat, implement, and/or evaluate outcomes. See NSHC’s Position Statement.
Core competencies for health coaches are based on theoretical principles, science, clinical practice, concept applications, and skills competency. Patients/clients identify their own specific concerns to be the focus throughout the coaching relationship, regardless of whether the relationship is sustained or brief.
Conclusion
The interest in the use of “coaching” to guide others to achieve optimal health and wellness has skyrocketed within the past 5 years. This interest has resulted in individuals and organizations of all types promoting their health coaching and wellness coaching training and/or certification programs to meet the marketplace demand.
The distinction between health coaching and wellness coaching definitions, health coaching attributes, and coach qualifications, risks and responsibilities offered by the NSHC comes at a critical time. The purpose is multifold:
To simplify an otherwise endless plethora of health coaching attributes that sees no end for the foreseeable future
To simplify a framework for research, thereby shortening the timeline to establish health coaching and wellness coaching effectiveness and gain consensus for each.
And most importantly, to enhance public awareness and safety during practice and the research process in a responsible meaningful way.
It is prudent for clinical health care providers and especially those in worksite health promotion to take the lead in affirming and publicizing the difference between health coaching and wellness coaching. NSHC’s position has gained much interest and is supported by the American Association of Occupational Health Nurses (AAOHN).
Spirit of the health coaching relationship and 50/50 patient/provider partnership in health
Patient/client engagement through motivational interviewing and empathy
Guiding the agenda and goal setting
Communication style
Cultural competence
Active listening
Mindfulness
Facilitating behavior change
Evidence-based practice interventions for wellness, prevention, and chronic health conditions
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biography
Melinda H. Huffman is a co-founder of the National Society of Health Coaches. She is a cardiovascular clinical nurse specialist and certified health coach. She is a nationally known speaker, writer, author, and consultant on evidence-based health coaching, creating a 50/50 patient/provider partnership in health, and chronic condition management. She conducts onsite CoachClinics nationwide.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.