
Abstract
Occupational burnout has been linked to the delivery of lower quality of care in some health care professions, including with turnover intentions and absenteeism in emergency medical services (EMS) workers. Thus, studies that identify factors associated with burnout may be integral to optimizing quality and workforce engagement among EMS professionals. A survey was conducted to assess social support outside the workplace, coping styles, and occupational burnout in a cohort of EMS providers from Minnesota. Surveys were returned by 217 providers (54% response), of which 167 had provided data on burnout, social support, and coping styles and were included in the analysis. The mean age was 41 years, 62% were male, and the prevalence of burnout was 17%. After adjustment for age and EMS tenure, the odds of burnout was higher among those characterized as socially isolated as compared with providers who were integrated socially or moderately integrated (odds ratio = 3.52; 95% confidence interval = [1.13, 10.98]). Common coping responses included planning, positive reframing, and active coping, while behavioral disengagement and denial were rarely used. Lack of social networks outside the workplace and frequent use of self-blame, food, or substance use as coping strategies were associated with burnout. Conversely, social integration and use of religion and instrumental support to cope with stressors were associated with reduced burnout.
Introduction
Individuals in human services professions are vulnerable to stress-related disorders and professional burnout, occupational health (Johnson et al., 2006), particularly emergency responders (Hegg-Deloye et al., 2014; van der Ploeg & Kleber, 2003), who are routinely exposed to high levels of emotional and physical stress as a result of providing acute care in the uncontrolled prehospital setting. Most studies on the occupational hazards of emergency responder worked have focused on law enforcement officers or firefighters, but a number of reports have documented similar physical and mental health risks in emergency medical services (EMS) providers, including being at increased risk for posttraumatic stress disorder (PTSD), obesity, disordered sleep, fatigue, and musculoskeletal problems (Berger et al., 2012; Hegg-Deloye et al., 2014; Sterud, Ekeberg, & Hem, 2006; van der Ploeg & Kleber, 2003).
Occupational burnout in EMS is attributed to a number of factors including performance in potentially hazardous environments, repeated exposure to trauma, the physical demands of the occupation, the strains of shift work, and the organizational stressors spawned by the hierarchical cultures prevalent in EMS (Boudreaux & Mandry, 1996; van der Ploeg & Kleber, 2003). Social support and coping styles are also thought to influence mental well-being in this group (Bennett et al., 2005; Donnelly & Siebert, 2009; Sterud, Hem, Lau, & Ekeberg, 2011). Burnout has been linked to lower quality of care delivered in other health care professions (Leiter, Harvie, & Frizzell, 1998), and with absenteeism and intention to the leave the profession in EMS providers (Crowe et al., 2018). Thus, identifying and addressing factors that increase risk of burnout is imperative for optimizing quality and workforce engagement among EMS professionals.
A survey was administered in a single EMS agency to (1) determine the prevalence of burnout, (2) describe coping behaviors and the degree of social connectedness among providers, and (3) examine whether coping behaviors and social connectedness are associated with burnout in our agency.
Method
This cross-sectional survey was conducted at Allina Health EMS, the prehospital emergency services provider of Allina Health, a not-for-profit health care system in Minnesota. The ambulance service provides 911 dispatch, advanced life support, basic life support, and scheduled medical transport in approximately 100 communities in and around Minneapolis–St. Paul, Minnesota. The agency employs paramedics, emergency medical technicians (EMT), medical dispatchers, and support staff and responds to about 110,000 calls annually across an 1,800 square mile service area. Two-member ambulance crew configuration for all 911 response is indiscriminately paramedic–paramedic or paramedic–EMT (i.e., configuration is not selected based on severity of the call) so exposures and work environment are considered identical for the two certification classes of field providers and they have been analyzed in aggregate (hereafter paramedics).
Data Collection
In 2012, a 167-item survey was emailed to all agency employees (n = 479) regardless of role. The survey included assessments of burnout and a variety of variables including demographics, social support, and coping style. The study protocol was approved by the Allina Health Institutional Review Board with voluntary completion of the survey constituting informed consent.
Burnout was measured using the 22-item Maslach Burnout Inventory–Health Services (MBI) version (Maslach, Jackson, & Leiter, 1996) which is considered the current gold standard for measuring work-related burnout. The MBI quantifies three dimensions of the burnout syndrome: emotional exhaustion (nine questions), depersonalization (five questions), and personal accomplishment (eight questions). Survey items are stated as job-related feelings such as “I feel emotionally drained from my work.” Respondents indicate how often they feel this way about their job using the following responses: 0 = never, 1 = a few times a year or less, 2 = once a month or less, 3 = a few times a month, 4 = once a week, 5 = a few times a week, 6 = every day. These responses yield the following ranges for the subscales: emotional exhaustion = 0 to 54, depersonalization = 0 to 30, and personal accomplishment = 0 to 48. Work-related strain is reflected by high scores on the emotional exhaustion and depersonalization dimensions and low scores on the personal accomplishment dimension. In addition to continuous dimension measures, cut-points based on normative United States (U.S.) data were used to define low, moderate, and high values on each scale (i.e., for emotional exhaustion, ≤16 = low, 17-26 = moderate, ≥27 = high; for depersonalization, ≤6 = low, 7-12 = moderate, ≥13 = high; for personal accomplishment, ≤31 = low, 32-38 = moderate, ≥39 = high; Maslach et al., 1996; Schaufeli & Van Dierendonck, 1995). For purposes of this analysis, burnout was deemed present in subjects with a high emotional exhaustion (i.e., ≥27) or high depersonalization (i.e., ≥13) score; the personal accomplishment score did not figure into the definition. This definition has been used by others (Schaufeli, Bakker, Hoogduin, Schaap, & Kladler, 2001; Thomas, 2004), though approaches to dichotomously defining burnout are not consistent (Dyrbye, West, & Shanafelt, 2009).
Social connectedness was measured using the Berkman-Syme Social Network Index (BSNI; Berkman & Syme, 1979). The BSNI is a validated 11-item questionnaire that evaluates the respondent’s current social connections in four areas: marital status, sociability (number of close relatives/friends and frequency of contact), affiliation with a religious community or congregation, and membership in other organizations/clubs. The BSNI asks the respondent to indicate things like whether they have a spouse/partner, whether they have a close friend or confidant they can share personal or health problems with, how many relatives and friends they feel close to, the number of relatives and friends they see at least once a month, and whether they belong to social or recreational groups such as churches, volunteer groups, fitness/sports clubs, or other community groups. The final score is used to characterize an individual’s level of social support as socially isolated, moderately isolated, moderately integrated, or socially integrated.
Items from the COPE Inventory (Carver, Scheier, & Weintraub, 1989), its shortened form, the Brief COPE (Carver, 1997), and two items to assess food coping (Tsenkova, Boylan, & Ryff, 2013) were used to ascertain how individuals generally respond to stressful events. Statements such as “I let my feelings out” and “I look for something good in what is happening” are provided and respondents indicate the degree to which they usually exhibit the behavior or way of thinking when they experience stressful events in their life. Responses of 1 (I do this a lot), 2 (I do this a medium amount), 3 (I only do this a little) and 4 (I usually don’t do this at all) are used to create subscales corresponding to specific coping approaches (e.g., denial, venting). In this application, a total of 24 survey items were used to assess use of the following 12 coping responses: planning, positive reframing, active coping, use of instrumental support, use of emotional support, religion, self-blame, food, venting, substance use, behavioral disengagement, and denial. The response values of two paired statements reflective of each of the coping responses are summed and reverse coded so that the score representing frequency of use of the coping responses ranges from 2 (rarely responds this way) to 8 (responds this way a lot). For purposes of our analyses, a subscale score of 6, 7, or 8 constituted frequent use, while a score of 2, 3, 4, or 5 indicated infrequent use. While some coping styles are thought to be functional and others dysfunctional, the inventory is used strictly to describe general coping style and not to characterize that style as “positive” or “negative.”
Demographic items on the survey included age, gender, relationship status (single/not in a committed relationship, married/partnered), and parental status (yes, no). Respondents indicated their current position as Paramedic–Field Staff, Paramedic–Supervisor/Manager, Dispatcher, Paramedic–Support staff, interfacility transfer personnel, or other. The first three categories (i.e., Paramedic–Field Staff, Paramedic–Supervisor/Manager, and Dispatcher) were used to identify clinicians who routinely provide 911 response, and the current analysis included only providers in these three roles. EMS tenure reflects the number of years providing 911 response and/or direct patient care as a paramedic or dispatcher. Respondents also designated their primary work setting as either metropolitan or non-metro/rural. Per the agency’s coverage area at the time of the survey, metropolitan did not include any distinctly urban areas.
Data Analysis
Means, frequencies, and proportions were calculated to describe characteristics of the study participants and burnout measures. De-identified, aggregate human resources data were used to compare characteristics of the respondents with those of the agency as a whole at the time of survey. Social support categories and the proportion of respondents who were frequent users of each of the coping responses were examined overall and stratified by gender, with gender differences assessed using a chi-square test. Univariate and multivariate logistic regression models were used to compute odds ratios (ORs) and 95% confidence intervals (CIs) for burnout in categories of social support, and the odds of burnout associated with frequent use of each of the 12 coping responses. Covariates in the adjusted models included age, gender, and EMS tenure. Stata version 14.1 (StataCorp LP, College Station, TX, USA) was used for analyses.
Results
At the time of the survey, 399 employees regularly provided 911 response, 217 of whom returned the survey (54% response). Among the 217, n = 167 had complete data for the MBI, BSNI and COPE portions of the survey and were used in analysis. The average age was 41, 62% were male, and 57% had 10+ years of EMS experience (Table 1). The distributions of age, gender, years in current position, and primary work setting among respondents closely reflected the distributions of those attributes in the agency as a whole (data not shown).
Characteristics of Emergency Medical Services Study Participants
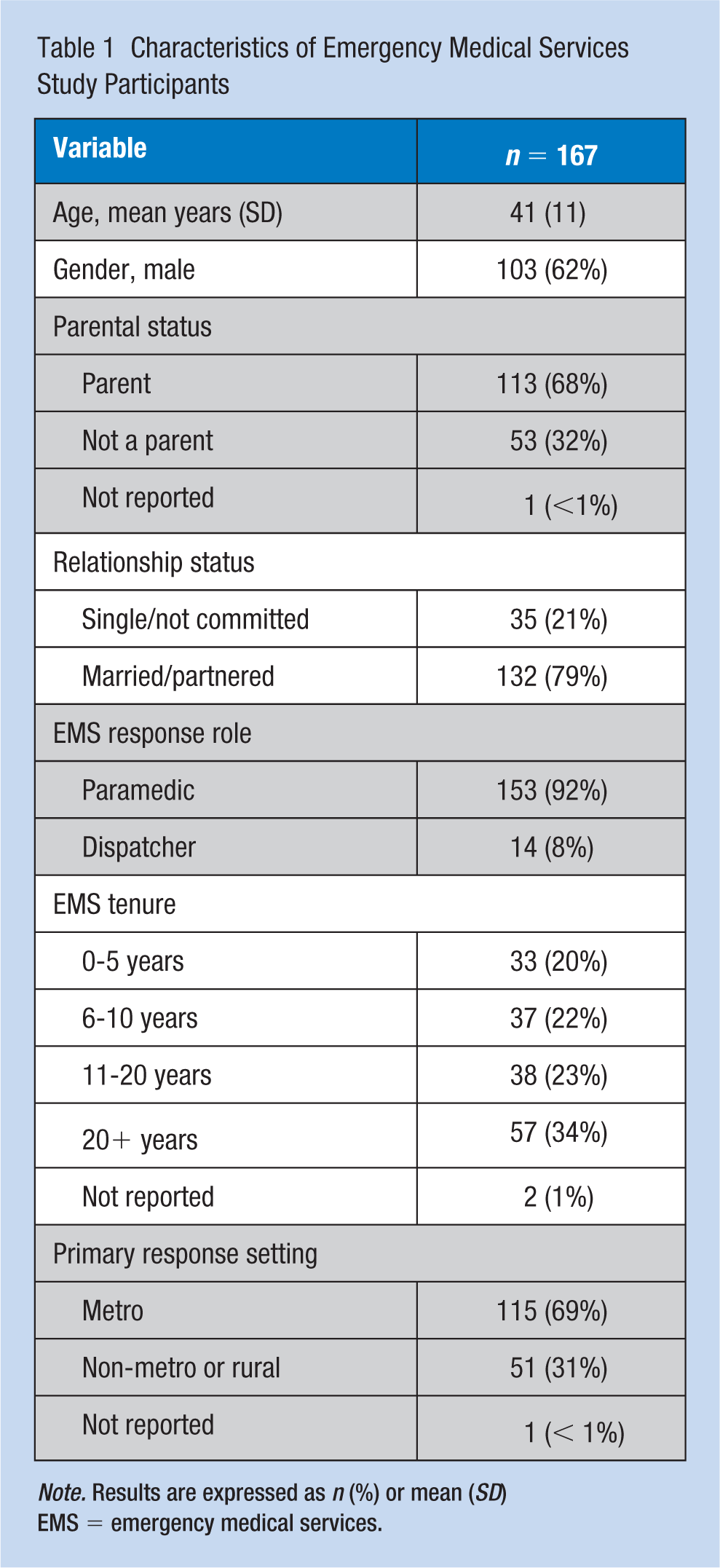
Note. Results are expressed as n (%) or mean (SD) EMS = emergency medical services.
The overall prevalence of professional burnout was 17% (Table 2). Using cut-points derived from a normative U.S. sample, 6% and 14% of respondents scored high on the emotional exhaustion and depersonalization subscales, respectively, while 59% scored low on personal accomplishment.
Prevalence of Burnout and Burnout Subscale Measures (n = 167)
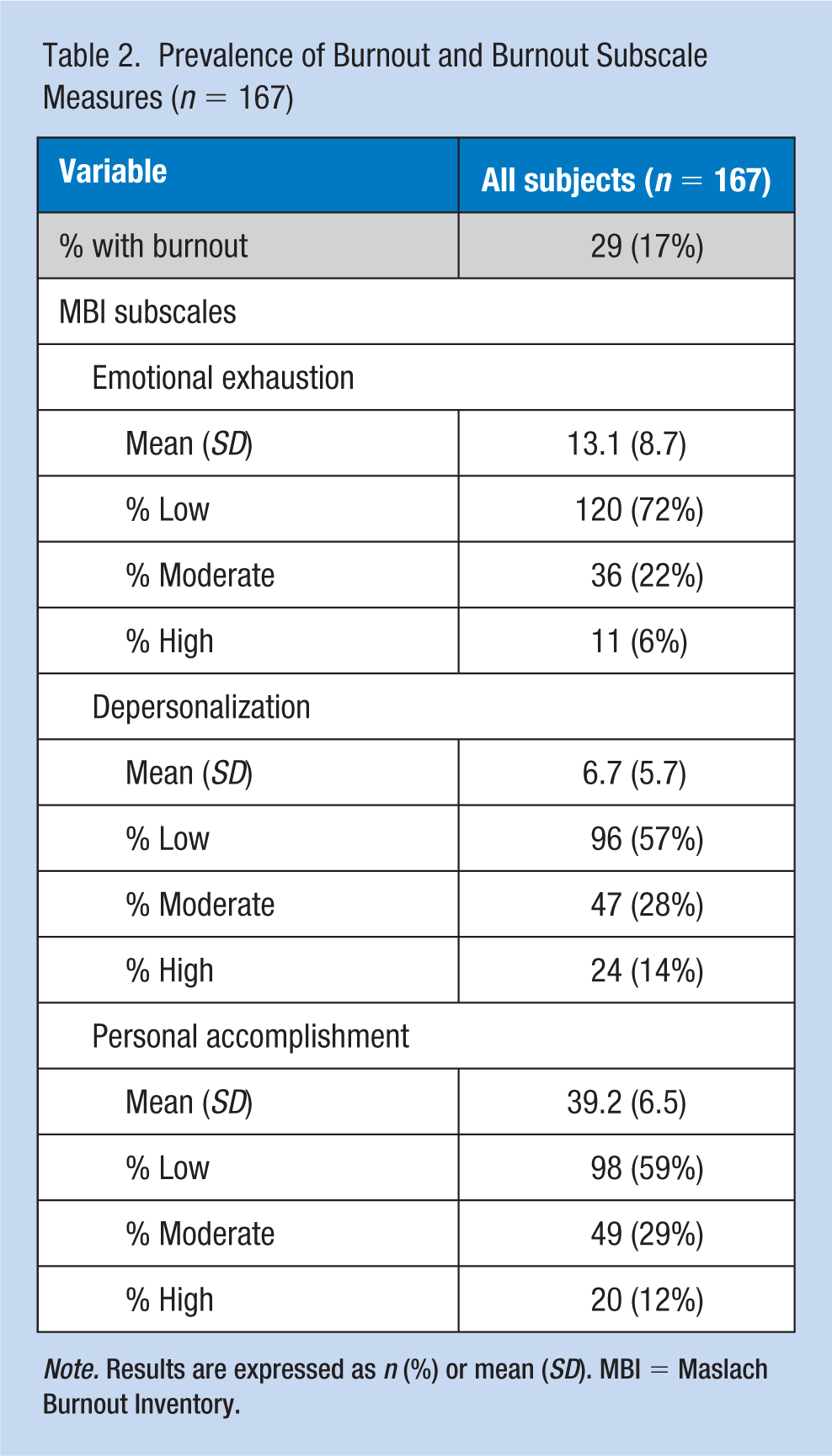
Note. Results are expressed as n (%) or mean (SD). MBI = Maslach Burnout Inventory.
Nearly a quarter of respondents were characterized as socially integrated, while 15% were socially isolated (Table 3). There was no significant difference in the distribution of social support by gender. The coping strategies most commonly used by providers included planning, positive reframing, active coping, and use of instrumental and emotional support. Instrumental support refers to assistance from others that is tangible (e.g., help with transportation, child care, housekeeping) while emotional support refers to the more intangible efforts by others that make us feel valued and cared for (e.g., providing reassurance or positive feedback, discussing feelings). Only 8% of providers acknowledged that they frequently use substances to cope, and virtually no respondents indicated they frequently used behavioral disengagement or denial. Female providers were more likely to report frequent use of instrumental support, emotional support, and venting than their male counterparts.
Level of Social Support and Use of Coping Responses Among Emergency Response Workers, Overall and Stratified by Gender
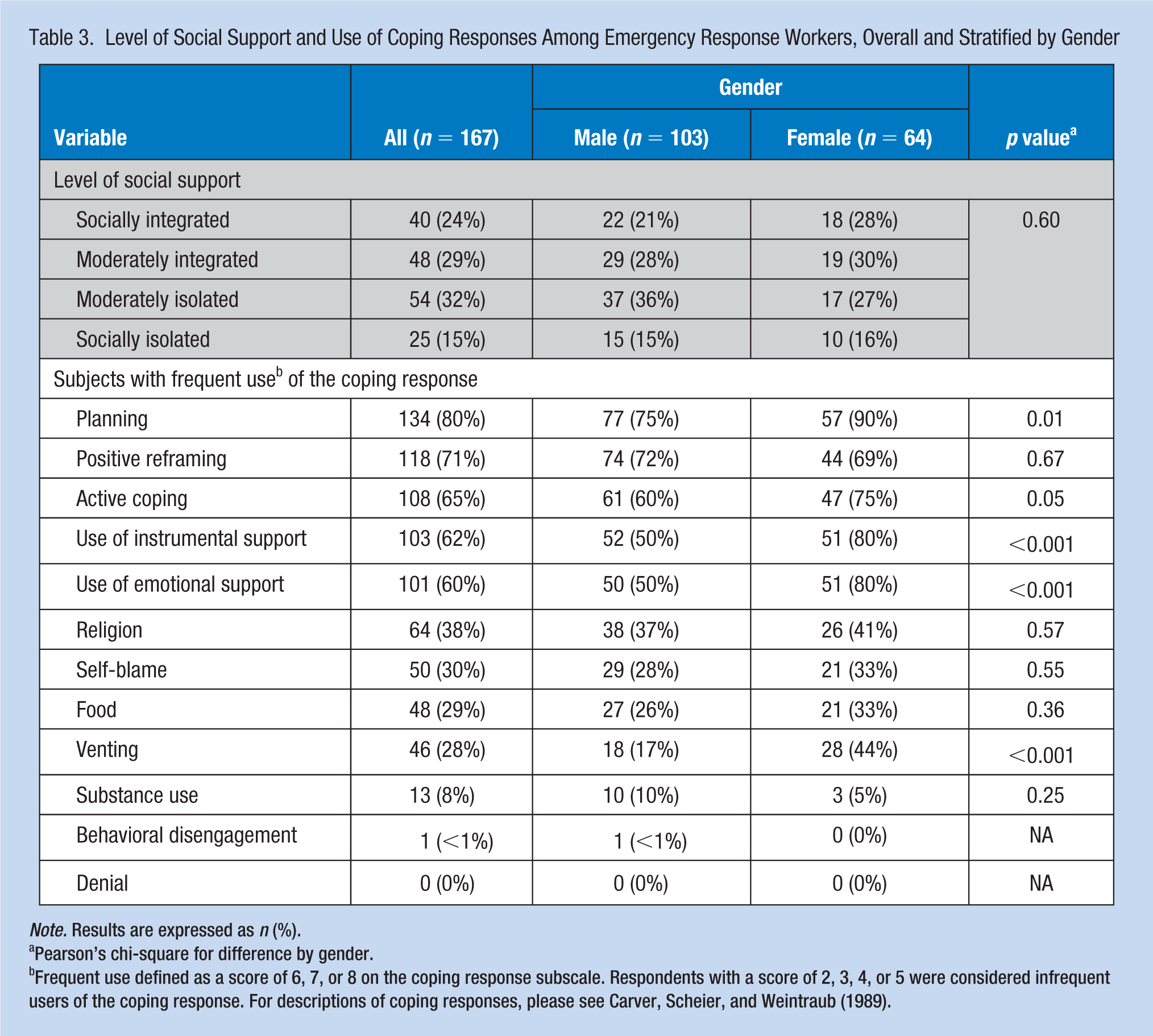
Note. Results are expressed as n (%).
Pearson’s chi-square for difference by gender.
Frequent use defined as a score of 6, 7, or 8 on the coping response subscale. Respondents with a score of 2, 3, 4, or 5 were considered infrequent users of the coping response. For descriptions of coping responses, please see Carver, Scheier, and Weintraub (1989).
The prevalence of burnout increased monotonically as social isolation increased (p for trend = .005; Table 4). Providers characterized as socially isolated had an increased odds of burnout compared with respondents who were integrated or moderately integrated (OR = 4.39; 95% CI = [1.54, 12.52]), and this finding persisted after adjustment for age and years in EMS (OR = 3.52, 95% CI = [1.13, 10.98]).
Crude and Adjusted Associations Between Level of Social Support and Risk of Burnout Among Emergency Medical System Workers (n = 167)
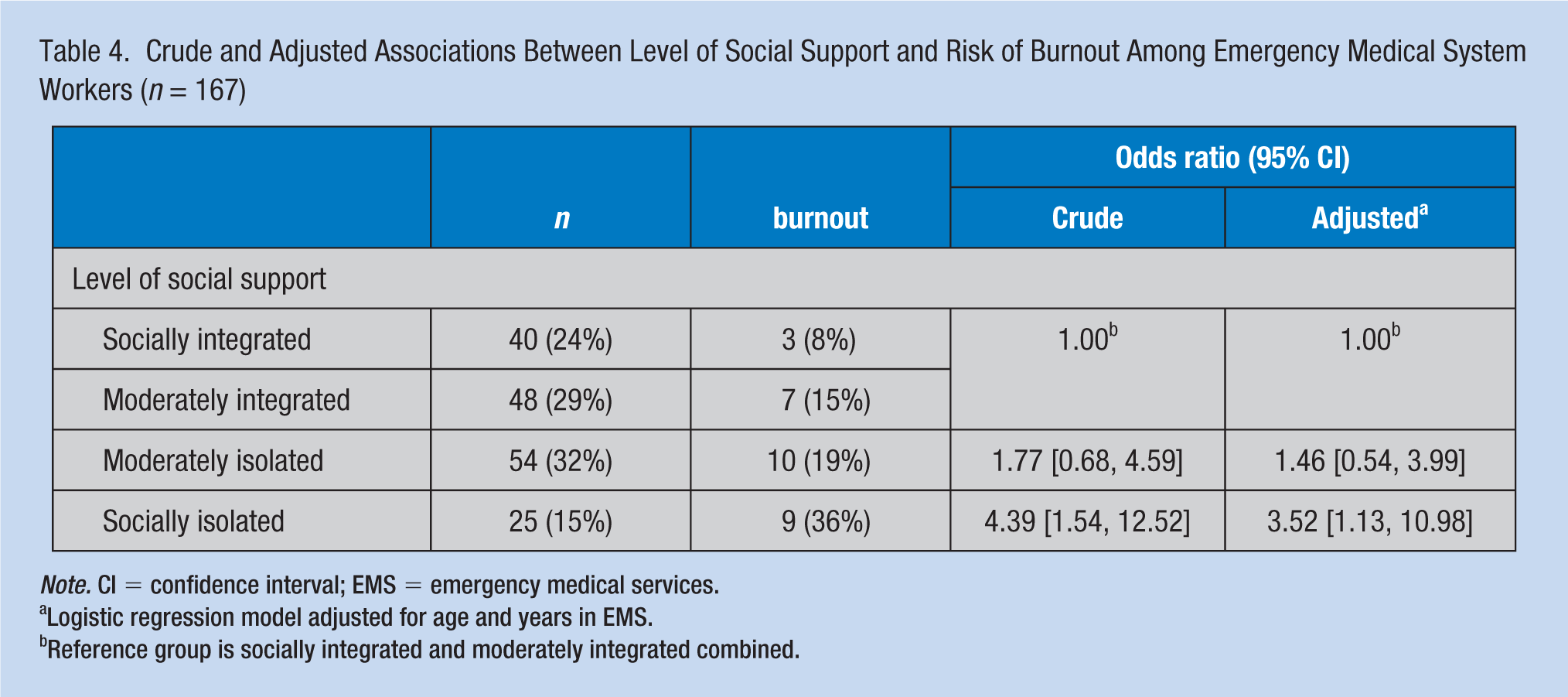
Note. CI = confidence interval; EMS = emergency medical services.
Logistic regression model adjusted for age and years in EMS.
Reference group is socially integrated and moderately integrated combined.
Providers who reported using religion, emotional support, and instrumental support with high frequency had a decreased odds of burnout when compared with those who reported using these strategies infrequently, while the odds of burnout was higher among those who regularly engaged in self-blame, or relied on food or substances to abate work-related stress (Table 5). With the exception of the use of emotional support, these associations remained after adjustment for age, gender, and years in EMS. The association between burnout and the coping strategies of behavioral disengagement and denial could not be evaluated due to rarity of use in this population.
Association Between Frequent Versus Infrequent Use a of Coping Responses and Burnout: Logistic Regression
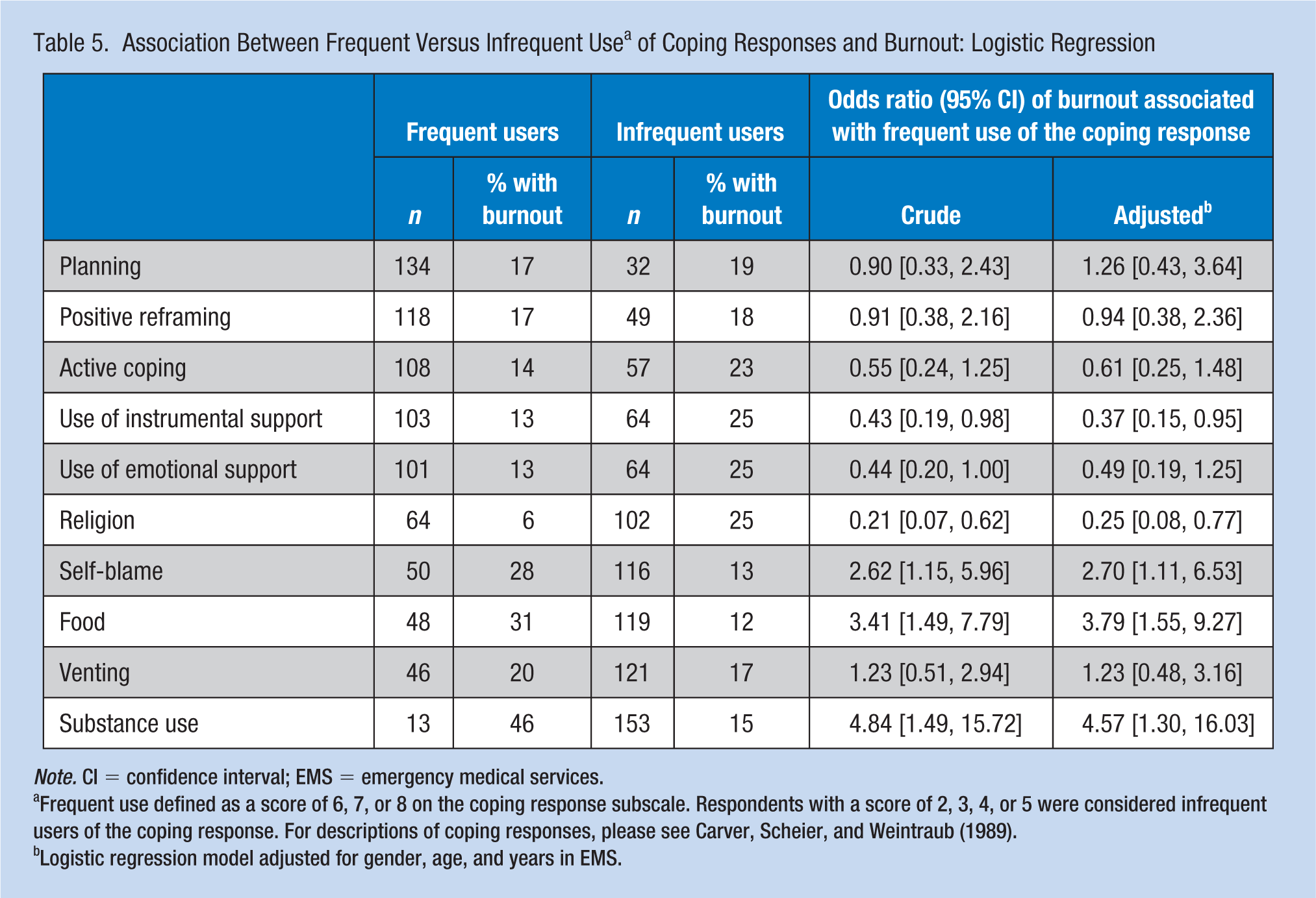
Note. CI = confidence interval; EMS = emergency medical services.
Frequent use defined as a score of 6, 7, or 8 on the coping response subscale. Respondents with a score of 2, 3, 4, or 5 were considered infrequent users of the coping response. For descriptions of coping responses, please see Carver, Scheier, and Weintraub (1989).
Logistic regression model adjusted for gender, age, and years in EMS.
Discussion
Occupational burnout has been documented extensively in emergency medicine physicians (Arora, Asha, Chinnappa, & Diwan, 2013; Bragard, Dupuis, & Fleet, 2015) and nurses (Adriaenssens, De Gucht, & Maes, 2015), but less is known about the prevalence and determinants of burnout in EMS clinicians, particularly those practicing in the U.S. Two recent surveys conducted in U.S. paramedics/EMTs found burnout was associated positively with turnover intentions and absenteeism (Crowe et al., 2018; Fragoso et al., 2016), so empirical studies to uncover correlates of burnout are integral to combating growing concerns around retention in the profession (Patterson et al., 2010). The findings of this study suggest social isolation outside the workplace is associated with burnout independent of age, gender, and years in the EMS profession, and that frequent use of self-blame, food, and substance use as coping strategies were also associated with an increased odds of burnout. Coping strategies associated with lower levels of burnout included religion and use of instrumental support.
Prior studies of social support in EMS responders have primarily focused on support received in the workplace and suggest that a supportive work environment may have a positive impact on recovery after traumatic incidents and mental well-being (Gouweloos-Trines et al., 2017; Revicki & Gershon, 1996; Shakespeare-Finch & Daley, 2017; Sterud, Hem, Ekeberg, & Lau, 2008; van der Ploeg & Kleber, 2003). The current study is distinct in that the measure of social support used here reflects personal relationships and interactions outside the workplace. In the only previous study we identified that examined non-work-based social support specifically in EMS workers, Fjeldheim et al. (2014) found that poor social integration was predictive of PTSD in a cohort of South African paramedic trainees. Social support outside the workplace has been shown to be a critical resource for managing occupational stress in other emergency responder groups such as police officers (Evans, Pistrang, & Billings, 2013), firefighters (Corneil, Beaton, Murphy, Johnson, & Pike, 1999; Huynh, Xanthopoulou, & Winefield, 2013), and emergency medical dispatchers (Shakespeare-Finch, Rees, & Armstrong, 2015).
Results from a recent survey of 145 Canadian paramedics (Donnelly, Bradford, Davis, Hedges, & Klingel, 2016) suggested that consideration of non-work-based social support may be important in developing burnout management strategies. When asked “if you felt you were suffering from work-related stress, how likely would you be to go to the following for help?” The top response among the paramedics was “a family member or friend” (81%), followed by “your partner” (73%), “a coworker” (50%), “the employee assistance program/another therapist” (39%), and “a supervisor” (17%) (Donnelly et al., 2016). This preference for seeking emotional support for work-related stress from family and friends has also been documented in police officers (Evans et al., 2013). Based on these findings and those of the current work, the popular contemporary paradigm of offering and encouraging use of formalized work-based supports (e.g., peer-support groups, critical incident stress debriefings) to prevent psychological stress and burnout in EMS professionals may need to be complemented with efforts to promote social network building away from the workplace. However, the long hours and shift work inherent in EMS, and the tendency of EMS professionals to work more than one job may limit opportunities to build positive social connections away from work. The number of hours worked per week was not measured in this study and represents a potentially important confounder of the association between social support and burnout.
Several of the present findings about coping strategies used by EMS providers are consistent with previous reports. The infrequent use of denial has been reported in two prior studies of paramedics (Clohessy & Ehlers, 1999; Mishra, Goebert, Char, Dukes, & Ahmed, 2010), and may reflect the fact that with repeated exposure to critical incidents, denial becomes an incompatible response (i.e., EMS workers see traumatic events often enough that they are no longer able to react with thoughts of “this isn’t real”). The current finding that paramedics frequently respond to stressful situations with positive reinterpretation and reframing has also been documented previously in EMS workers (Clohessy & Ehlers, 1999; Mishra et al., 2010), as has the infrequent use of substance abuse as a coping behavior (Mishra et al., 2010). Extant studies have also described the predilection for female paramedics to employ venting or emotional expression in response to difficult situations more so than male paramedics (Clohessy & Ehlers, 1999; Kirby, Shakespeare-Finch, & Palk, 2011).
No prior studies could be identified that have specifically examined the association between coping styles and occupational burnout in EMS workers, but existing data on coping and its relation to posttraumatic stress symptomatology in paramedics (Donnelly, 2012; Holland, 2011; Kirby et al., 2011) might be extrapolated for comparison. Studies in paramedics from Australia (Kirby et al., 2011) and the U.S. (Holland, 2011) found that use of adaptive coping strategies (e.g., positive reframing, seeking support) were associated with enhanced posttraumatic growth and fewer posttraumatic stress symptoms, while maladaptive strategies (e.g., disengagement) were associated with negative posttraumatic responses. The use of alcohol in response to work-related stress has also been shown to exacerbate posttraumatic stress symptoms in EMS workers (Donnelly, 2012). More directly comparable to the current results are studies of coping styles and MBI-measured burnout in emergency department staff (Howlett et al., 2015) and medical residents (Doolittle, Windish, & Seelig, 2013). Several findings from those studies coincide with those of the current study, namely that self-blame is associated with increased burnout, while use of spirituality and positive reframing may have protective benefit.
Although the response rate here (54%) was comparable to response rates reported in other published studies of surveys in EMS personnel (40%-60%) (Bennett et al., 2005; Clohessy & Ehlers, 1999; Sterud et al., 2011; van der Ploeg & Kleber, 2003), there is always a concern that survey respondents were attitudinally or behaviorally different than those who chose not to participate. Burnout was only identified in 29 individuals in this study and the resulting small numbers in some subgroups created challenges in analysis and interpretation. External validity may be limited because this work was conducted in a single EMS agency, and the cross-sectional nature of this study limits conclusions about causality. In particular, temporality is unclear. For example, it is impossible to discern whether social support networks may diminish, or coping behaviors become more maladaptive as a result of burnout. The survey instrument used in this study did not include an assessment of work-based social support or collect data on number of hours worked per week, and both would have strengthened the analysis of social support. Coping responses were not examined by EMS tenure, but such an analysis would shed light on the intriguing question of whether those who remain in the profession long term have a coping profile that is distinct from those who are newer to EMS. A critical first step acknowledged by others (Holland, 2011; Howlett et al., 2015) is increasing self-awareness of individual coping styles through assessment and feedback to EMS providers, but further investigations are needed to determine whether EMS providers can be taught to engage coping strategies that have been shown to optimize well-being in the aftermath of stressful events, even if those strategies differ from their inherent coping style.
Implications for Occupational Health Nursing Practice
The role of EMS providers in the U.S. has evolved significantly with the introduction of emerging, field-ready technologies and the proliferation of gun violence and terrorism, and thus there is an urgent need to improve contemporary understanding of mental well-being across this integral part of our nation’s corps of emergency responders. To begin to address this need, leaders of EMS agencies should seek to implement systematic assessment with validated instruments that would promote dialogue and facilitate critical data gathering. Such initiatives would represent an important starting point within many organizations for both normalizing expression around stressors and altering the common perception among EMS providers that management is not concerned about their mental well-being and that agency support is inadequate (Alexander & Klein, 2001; Drewitz-Chesney, 2012; Gallagher & McGilloway, 2009; Regehr, Goldberg, & Hughes, 2002). As demonstrated by this study, EMS organizations can administer surveys that assess indicators of mental well-being including occupational burnout, perceived stress, PTSD symptoms, and suicidality, and also evaluate potential risk factors such as provider demographics, social connectedness, coping behaviors, organizational factors (e.g., perceived support), and exposure to critical incidents. Findings can inform the design and implementation of interventions, agency resources, and operational processes that appropriately support mental well-being. Specific to the current work, this might include identifying training and resources that promote the adoption of optimal coping strategies and the cultivation of positive relationships outside the workplace. Periodic re-administration of surveys can serve as a barometer for wellness and as a tool for examining the effects of interventions designed to promote provider wellness. Included in these efforts should be routine sharing of data and interpretations back with clinicians, and education that promotes awareness and encourages utilization of available resources.
Conclusion
Possessing strong social networks outside of work and using religion and instrumental support to cope with stressors may be associated with lower levels of burnout in EMS workers, while social isolation, and frequent use of self-blame, food, and substance use to cope may be associated with increased burnout. EMS agencies should consider conducting assessments to evaluate burnout in their employees and enhance provider awareness of coping responses. Additional studies that prospectively explore the relation between social isolation, coping responses, and burnout are needed.
Applying Research to Practice
This survey conducted in an EMS agency in Minnesota suggests social isolation outside the workplace is associated with burnout independent of age, gender, and years in the EMS profession. Frequent use of self-blame, food, and substance use as coping strategies were also associated with an increased odds of burnout. Coping strategies associated with lower levels of burnout included religion and use of instrumental support. Occupational health professionals practicing in emergency care systems should conduct surveys among their EMS providers to assess indicators of mental well-being such as occupational burnout, perceived stress, PTSD symptoms, and suicidality, and also evaluate potential risk factors including provider demographics, social connectedness, coping behaviors, organizational factors, and exposure to critical incidents. These baseline results should then be used to guide implementation of interventions, agency resources, and operational processes that appropriately support mental well-being. Identifying training and resources that promote the adoption of optimal coping strategies and the cultivation of positive relationships outside the workplace may be important. EMS provider well-being initiatives should include routine sharing of data with clinicians, and education that promotes awareness and encourages utilization of available resources.
Footnotes
Acknowledgements
The authors wish to thank the employees of Allina Health EMS for their participation in the survey.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Lori L. Boland, MPH, is a principal research scientist at Allina Health Emergency Medical Services in St. Paul, Minnesota, and with Care Delivery Research at Allina Health in Minneapolis, Minnesota.
Pamela J. Mink, MPH, PhD, is a principal research scientist with Care Delivery Research at Allina Health in Minneapolis, Minnesota
Jonathan W. Kamrud, NREMT-P, is the manager of EMS Analytics for Allina Health Emergency Medical Services in St. Paul, Minnesota and is also currently pursuing his Master of Science in Analytics at the Villanova School of Business.
Jessica N. Jeruzal, BA, is a research assistant with Allina Health Emergency Medical Services in St. Paul, Minnesota and is also pursuing her Master of Science in Health Services Research, Policy and Administration at the University of Minnesota.
Andrew C. Stevens, MD, is an emergency medicine physician and the Associate Medical Director of Allina Health Emergency Medical Services in St. Paul, Minnesota. He also serves on the American Medical Response INDYCAR Safety Team.