
Abstract
The labor force participation rate for adults aged 55 years and older has increased nearly 10% over the past two and a half decades. As workers age, they frequently experience increased chronic health conditions and impaired sleep, which may negatively influence their self-rated health (SRH) and work performance. This study aimed to examine the associations between nonrestorative sleep (NRS) and work performance (i.e., difficulty concentrating or having lower productivity at work) and associations between demographic and sleep characteristics with SRH in middle-aged workers. We conducted a secondary data analysis among working middle-aged adults 50 to 65 years of age (N = 392) from the 2008 Sleep in America Poll. Respondents frequently reported impaired sleep such as frequent insomnia symptoms, NRS, and short sleep duration. Nonrestorative sleep was associated with decreased work performance such as trouble organizing work, doing work over due to mistakes, and lower productivity. Nonrestorative sleep and short sleep duration were significantly associated with lower SRH. Strategies for the early detection of impaired sleep and implementation of interventions to improve sleep may improve SRH and work performance in working middle-aged adults.
Introduction
The workforce in the United States is aging. In 2017, an estimated 27 million workers were 55 years of age or older, constituting approximately 22% of the total workforce for 2017 (Bureau of Labor Statistics, 2018). Over the past 25 years, the labor force participation rate of individuals above the age of 55 (the percentage of those who are working or actively looking for work) has increased by approximately 10%, whereas the rate for younger age groups has remained nearly constant (Bureau of Labor Statistics, 2018).
With aging, there is an increase in chronic health conditions, disabilities (Paez, Zhao, & Hwang, 2009), and impaired sleep (Mai & Buysse, 2008). Such conditions can adversely affect individuals’ perceptions of their overall health status, including their self-rated health (SRH). A recent study reported that middle-aged adults, aged 55 to 64 years, showed an increase in the proportion reporting their health as fair or poor using a standard SRH scale (Idler & Cartwright, 2018). Self-rated health is a good indicator of actual health status (Office of Disease Prevention and Health Promotion, 2018), and poor SRH should not be considered a benign condition. Decreased SRH during middle age predicts frailty, morbidity, and mortality in older age (DeSalvo, Bloser, Reynolds, He, & Muntner, 2006; Galenkamp et al., 2013; Huohvanainen et al., 2016).
Impaired sleep can result from various impairments such as sleep disorders (e.g., insomnia or sleep apnea) or sleep deprivation (inadequate sleep duration). A hallmark of impaired sleep is nonrestorative sleep (NRS), the feeling of waking up unrefreshed, or not feeling sufficiently rested after sleep (Roth et al., 2010). Nonrestorative sleep frequently accompanies sleep disorders (American Psychiatric Association [APA], 2013), and daytime sleepiness is a potential indicator of NRS (Zhang, Lam, Li, Li, & Wing, 2012). Impaired sleep is associated with poorer SRH (Chasens, Twerski, Yang, & Umlauf, 2010; Kitamura, Nakatani, & Nakata, 2014; Silva-Costa, Griep, & Rotenberg, 2015). Moreover, although some studies report NRS improves with age (Ohayon & Roth, 2001; Wakasugi et al., 2014), the prevalence of NRS in middle-aged adults (aged 50-69) remains high (estimated 16%-31%; Wakasugi et al., 2014). Two other common sleep disorders, sleep apnea, a disorder characterized by pauses in breathing during sleep (National Institute of Neurological Disorders and Stroke [NINDS], 2018b), and insomnia, characterized by difficulty in falling and maintaining sleep (APA, 2013), also increase with age (Edwards et al., 2010; Mai & Buysse, 2008). Of note, previous studies that examined NRS and common sleep disorders did not focus exclusively on middle-aged workers (50-65 years); thus, better understanding of sleep characteristics in this population is necessary.
In addition to the effects on SRH, impaired sleep is associated with negative work performance such as sickness absences (Hui & Grandner, 2015; Rahkonen et al., 2012) and work-related injuries (Uehli, Miedinger, et al., 2014). A systematic review and meta-analysis of 27 studies found that impaired sleep increased the risk of being injured at work by 1.62 times (Uehli, Mehta, et al., 2014). In addition, negative effects of impaired sleep on lower self-rated work performance (Hui & Grandner, 2015) and impaired work productivity (Roth et al., 2010) were found, although these studies did not focus on middle-aged workers.
Given the increasing trend in the aging workforce, it is essential to gain a better understanding of how impaired sleep among these workers is associated with their SRH. Such studies may help identify potential areas for intervention to improve their overall health. Study results may expand employers’ awareness about their aging workers. Results may prompt individuals to change their behaviors to reflect a healthy lifestyle and may contribute to promoting healthy work environments (Musich, McDonald, & Chapman, 2009). The aims of the current study were to (a) examine the associations between NRS and work performance and (b) examine the associations between sociodemographic and sleep characteristics and SRH in middle-aged workers aged 50 to 65 years.
Method
Design and Sample
This secondary data analysis used data collected during the National Sleep Foundation’s (NSF) 2008 Sleep in America Poll that surveyed adults working outside the home at least 30 hours a week. The brief survey, developed by experts in occupational sleep medicine, included questions used in previous NSF surveys and questions taken from validated questionnaires. The methodology is fully described in the 2008 Sleep in America Poll: Summary of Findings (NSF, 2008). A random sample of telephone numbers was purchased by the NSF, and trained interviewers conducted the interviews. Quota sampling was used to achieve a nationwide, representative sample (N = 1,000; NSF, 2008); there was a 17% response rate. In these analyses, we examined a subsample of middle-aged working adults aged 50 to 65 years (N = 392). The sampling error of the data for the entire sample was estimated to be 3.1 percentage points with a 95% confidence interval (CI); however, the NSF acknowledged that a larger sampling error may have occurred in subsamples. The original survey used verbal informed consent and deidentified data (NSF, 2008). The institutional review boards at the University of Pittsburgh and Georgia State University approved the study.
Measures
SRH
Self-rated health was evaluated with a single question, “In general, how would you rate your current overall health?” with Likert-type responses of 1 (poor), 2 (fair), 3 (good), 4 (very good), and 5 (excellent). Responses were considered both as a continuous variable and dichotomized as either good, very good, and excellent or fair and poor (Zajacova & Dowd, 2011).
Sleep measures
To assess insomnia symptoms, three survey items were used that are reflective of the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; APA, 2013) criteria for insomnia including difficulty in initiating sleep, difficulty in maintaining sleep continuity, and early morning awakening with inability to get back to sleep. Frequency of these three symptoms over the past month was measured on a scale ranging from 1 (never), 2 (rarely), 3 (a few nights a month), 4 (a few nights a week), and 5 (almost every night or every night). Responses were tallied to create an insomnia symptom frequency index with scores ranging from 3 to 15. Scores ≥12 indicated insomnia symptoms frequently occurred at least multiple nights a week.
Nonrestorative sleep was assessed with the single-item, “how often over the past month did you wake up feeling unrefreshed,” using a scale ranging from 1 (never), 2 (rarely), 3 (a few times a month), 4 (a few times a week), to 5 (almost every night or every night). According to the DSM-5 (APA, 2013), NRS is a nonspecific symptom that frequently accompanies sleep disorders.
Daytime sleepiness was measured using the questions taken from Epworth Sleepiness Scale (ESS) that were included in the survey (ESS, α = .88; Johns, 1992). The eight-item ESS evaluated the propensity to fall asleep during the day. Scores range from 0 to 24, with a score >10 indicating excessive daytime sleepiness. Responses to the ESS were evaluated as both a continuous variable and dichotomized as either normal or excessive daytime sleepiness.
Sleep duration was assessed by questions that asked how long (hours and minutes) the respondent normally slept on days worked and on days not worked. Average sleep duration was then calculated as ([sleep duration days worked × 5] + [sleep duration days off × 2]) / 7. Short sleep duration was operationalized as obtaining less than 7 hours a night and dichotomized as “<7 hours” or “≥7 hours” (Hirshkowitz et al., 2015).
Respondents were also asked whether they had ever been diagnosed by a doctor and whether they were currently receiving treatment for sleep apnea, restless leg syndrome (a disorder that produces uncomfortable sensations in the legs that can potentially disrupt sleep; NINDS, 2018a), insomnia, or shift–work disorder. Shift–work disorder is defined by the DSM-5 in persons who work shifts outside of a normal daytime schedule as excessive sleepiness at work and difficulty in sleeping when at home (APA, 2013).
Work performance
Respondents were asked to provide the average number of hours worked per week and whether their work schedule allowed them to obtain enough sleep (yes/no) and their average total daily commute time to and from work (in minutes; NSF, 2008). They were asked to indicate the frequency, over the past month, with which they had difficulties concentrating at work, organizing work, avoided interactions with others, became bored at work, had to repeat work due to mistakes, had reduced productivity, or failed to finish assigned tasks. These items were measured on a scale ranging from 1 (never), 2 (rarely), 3 (a few nights a month), 4 (a few nights a week), to 5 (almost every night or every night). Responses to the work performance questions were dichotomized as either infrequent (1 [never], 2[rarely], and 3 [a few days a month]) or frequent (4 [a few days a week] and 5 [every day or almost every day]).
Demographic and health characteristics
As reflected in Table 1, information on age, sex, education, race, marital status, and whether there were children below 18 years in the household (yes/no) was collected. Because of the fairly homogeneous sample, education was dichotomized in the analysis as either high school or less or more than high school. Self-reported height and weight were used to calculate body mass index (BMI; kg/m2). A BMI ≥ 25 is considered overweight and ≥30 is considered obese (National Heart, Lung, and Blood Institute, 2018). Participants were asked whether they were currently being treated for heart disease, high blood pressure, diabetes, heartburn or gastroesophageal reflux disease, arthritis, depression, or anxiety disorder. Responses were combined together to indicate total number of health conditions.
Demographic and Clinical Characteristics of Middle-Aged Workers (N = 392)

Note. This is a subsample from the National Sleep Foundation (2008) Sleep in America Poll (N = 1,000). NRS = nonrestorative sleep.
n = 389.
n = 391.
n = 380.
n = 388.
n = 351.
n = 367.
Analysis
SPSS version 24.0 (IBM; Armonk, NY, USA) was used to analyze the data. Descriptive statistics included means and standard deviations for continuous variables, and frequencies and percentages for categorical variables. For descriptive analyses, differences between continuous outcomes were examined using t tests and chi-square tests, or Spearman correlations were used for categorical outcomes. Binary logistic regression was used to measure the potential impact of NRS on work performance such as having to do work over due to mistakes, lower productivity, trouble organizing work, experiencing difficulties concentrating, becoming impatient with others, avoiding interactions with others, and becoming bored while at work. Multivariate logistic regression was used to measure the potential impact of sex, education, total hours worked/week, insomnia symptoms, NRS, and sleep duration on SRH (good to excellent/fair to poor). For both analyses, odds ratios (ORs) and 95% CIs were calculated.
Results
Table 1 describes the characteristics of the sample of 392 participants. The majority (88%, n = 345) reported their health as excellent, whereas only 1.8% (n = 7) characterized their health as “poor.” The group was fully employed with almost half (44.4%, n = 174) who worked more than 40 hours a week, and 25% of the sample reported an average of 50 or more hours each week. With regard to sleep, 18% (n = 70) reported frequent insomnia symptoms; 54% (n = 212) reported one or more insomnia symptoms at least a few nights per week; 45% (n = 180) had frequent NRS; and 12% (n = 44) had excessive daytime sleepiness. Although most respondents (90.2%, n = 353) felt their work schedule allowed them time to obtain adequate sleep, nearly 45% (n = 165) slept less than 7 hours per night. More than 90% (n = 353) of the sample was not currently being treated for any of the four listed sleep disorders.
Associations between the variables of SRH, age, BMI, NRS, insomnia, sleep duration, and daytime sleepiness are depicted in Table 2. There were no significant differences by age, race, or marital status in frequency of NRS, short sleep duration (<7 hours per night), or SRH; however, women were more likely to report NRS (p < .006) and persons with less than a high school education were more likely to report short sleep duration (p < .017). Lower (worse) SRH was associated with impaired sleep, including NRS, more frequent insomnia symptoms, and short sleep duration. Age was not significantly associated with any of the variables. Higher BMI was significantly associated with more daytime sleepiness, and increased hours worked had a modest but significant association with decreased sleep duration.
Associations Between SRH, Age, BMI, Hours Worked, and Sleep Among Middle-Aged Workers (N = 392)
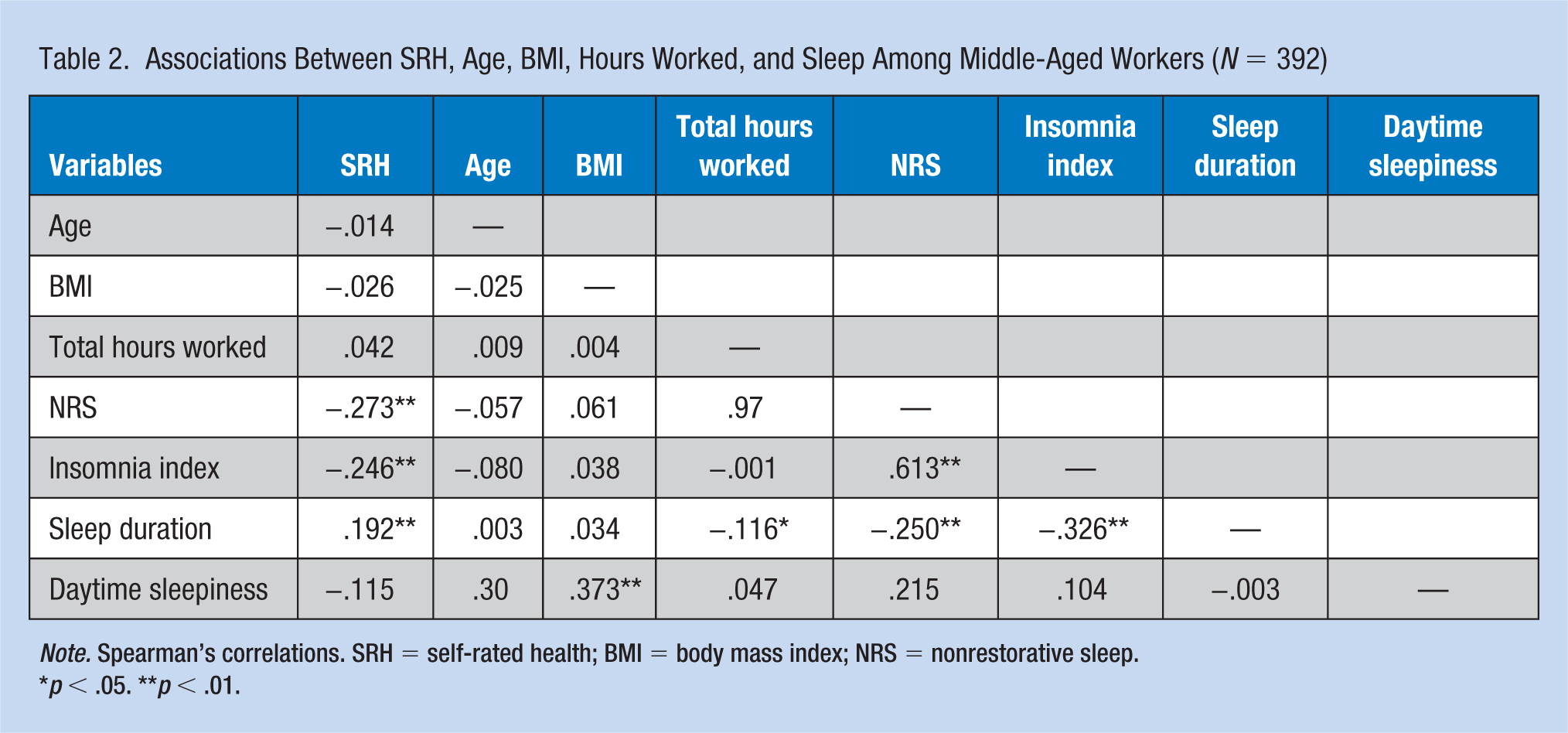
Note. Spearman’s correlations. SRH = self-rated health; BMI = body mass index; NRS = nonrestorative sleep.
p < .05. **p < .01.
Participants who worked more than 40 hours a week were more likely to report NRS (OR = 1.51, 95% CI = [1.01, 2.25], p = .046) but did not report lower SRH (OR = 0.90, 95% CI = [0.49, 1.65], p = .722) compared with those who worked 40 hours or less a week. Those persons with longer commutes to and from work (1 hour or more) were significantly more likely to have NRS (OR = 1.85, 95% CI = [1.16, 2.95], p = .010) compared with those with shorter commutes (less than 1 hour). Impaired work performance (difficulties concentrating, trouble organizing work, impatience with others, avoidance of interactions with others, becoming bored, doing work over due to mistakes, and lower productivity) occurred more frequently (p < .05; see Table 3) among those with NRS compared with those with restorative sleep.
Odds of Impaired Work Performance and Nonrestorative Sleep Among Middle-Aged Workers: Unadjusted ORs and 95% CI
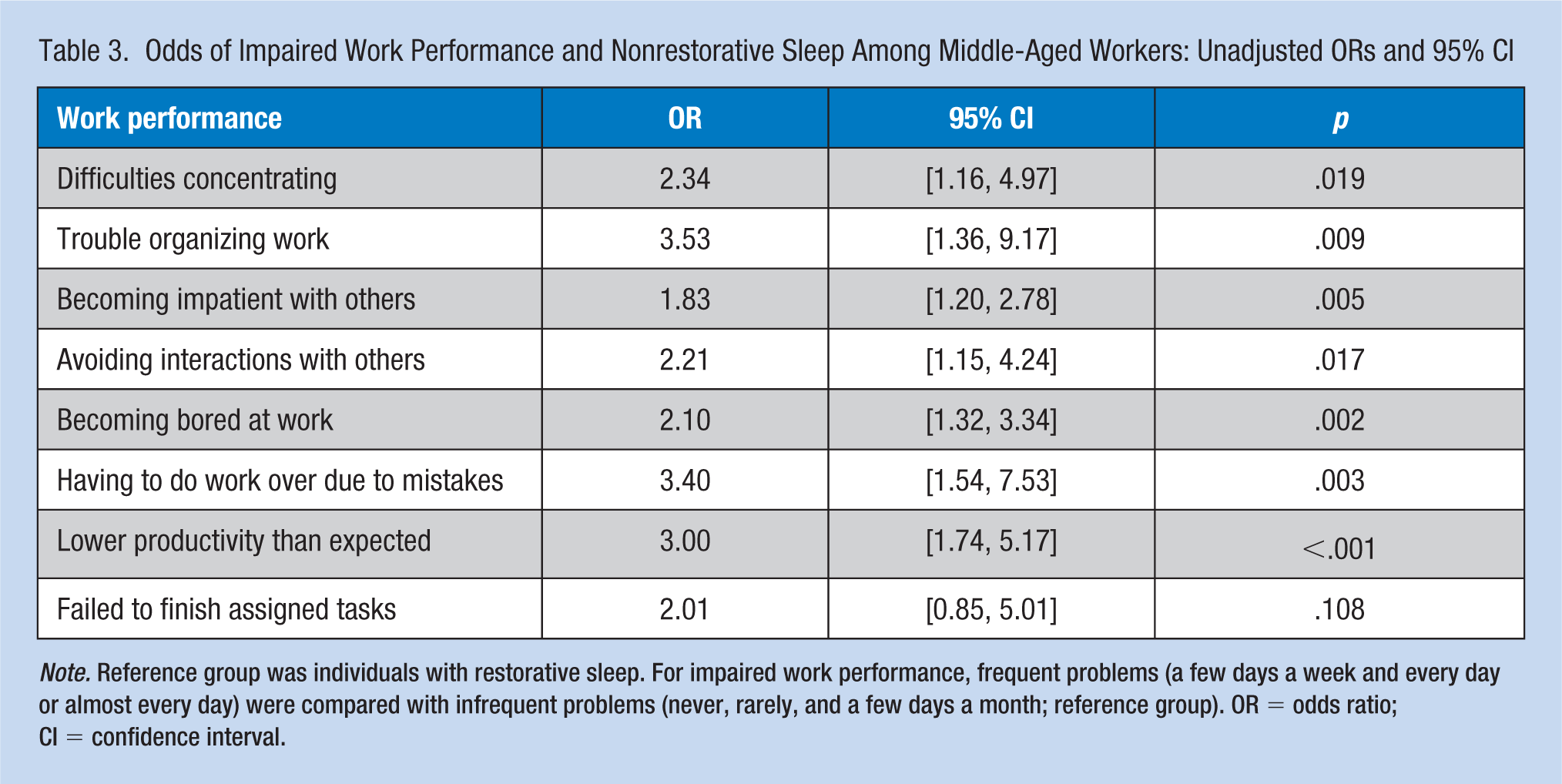
Note. Reference group was individuals with restorative sleep. For impaired work performance, frequent problems (a few days a week and every day or almost every day) were compared with infrequent problems (never, rarely, and a few days a month; reference group). OR = odds ratio; CI = confidence interval.
In the fully adjusted model, persons with NRS had more than 2.5 times the risk of lower SRH (OR = 2.52, 95% CI = [1.09, 5.78], p = .03) and those with short sleep duration (<7 hours/night) had more than 2.6 times the risk of lower SRH (OR = 2.62, 95% CI = [1.24, 5.50], p = .01) after adjusting for all other variables (sex, education, hours worked/week, and insomnia symptoms) in the model (see Table 4). Sex, educational level, working more than 40 hours a week, and insomnia symptoms were not statistically significant in predicting SRH.
Unadjusted and Adjusted Associations Between Sleep Measures and Fair-to-Poor SRH Among Middle-Aged Workers
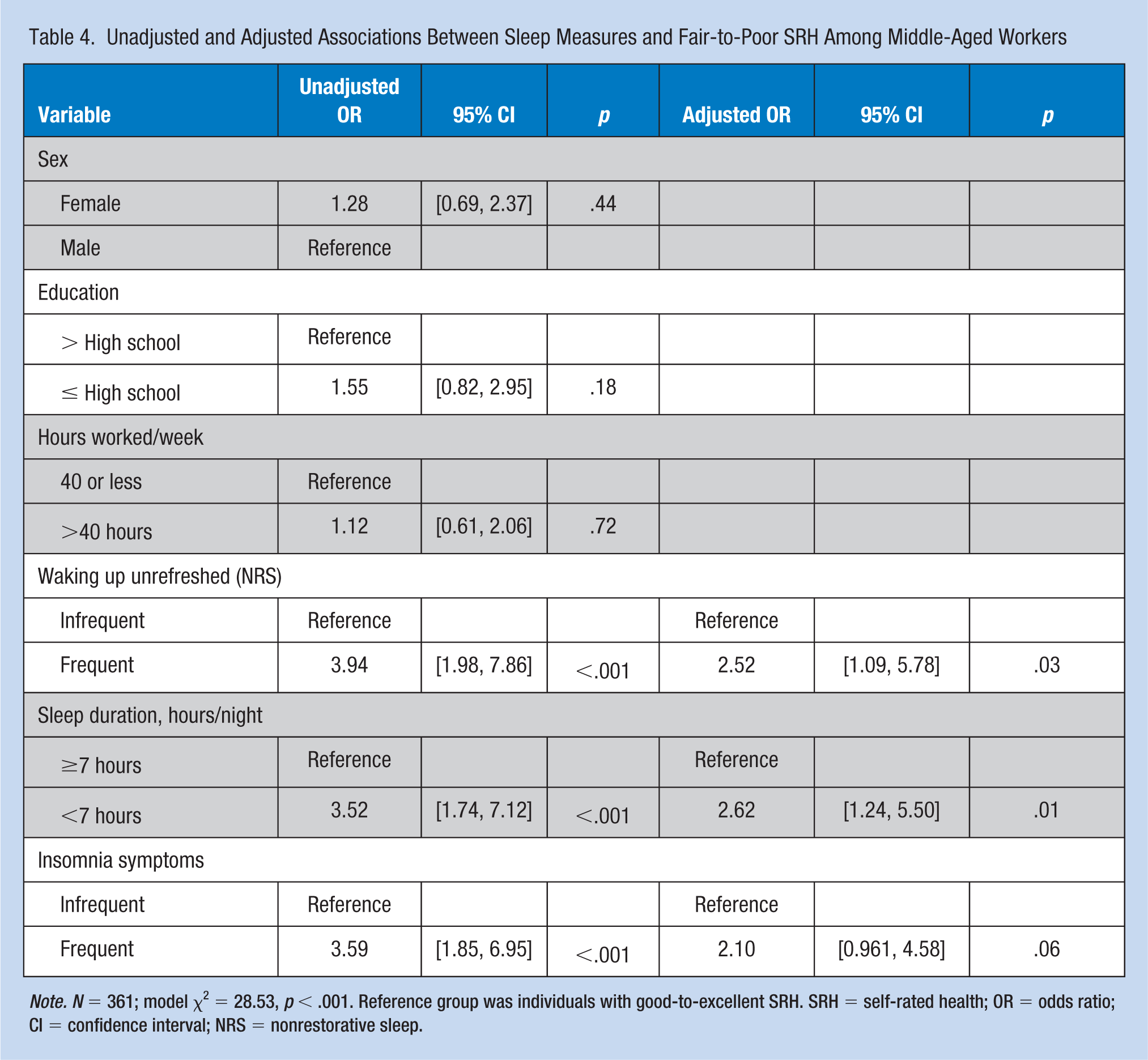
Note. N = 361; model χ2 = 28.53, p < .001. Reference group was individuals with good-to-excellent SRH. SRH = self-rated health; OR = odds ratio; CI = confidence interval; NRS = nonrestorative sleep.
Discussion
This study revealed a very high occurrence of frequent NRS in the sample (46%) and that NRS was significantly associated with more frequent negative work performance and worse SRH in middle-aged workers between the ages of 50 and 65 years. This finding of NRS prevalence is in stark contrast to two large-scale studies that reported the prevalence of NRS as 8.9% to 25% in adults ≥18 years old (Wakasugi et al., 2014; Zhang et al., 2012). The findings regarding the role of NRS on work performance are consistent with the findings from previous studies. Sleep loss is known to negatively affect capacity and work effort (Engle-Fiedman, 2014), and poor sleep hygiene is known to yield increased psychological strain, less self-control, and less work engagement (Barber, Grawitch, & Munz, 2013).
A notable minority of the sample (12%) reported fair-to-poor SRH. Previous work has shown that, compared with those with excellent SRH, those with poor SRH had a twofold higher risk of mortality (DeSalvo et al., 2006). In addition, SRH provides an indicator of cognitive function, and poorer SRH status may predict cognitive decline in older adults (Bendayan, Piccinin, Hofer, & Muniz, 2017). It has been recently reported that the predictive validity of SRH for mortality appears to be growing stronger over the past decade, and may be linked with a person’s ability to better assess his or her own health due to improved access of health information (Schnittker & Bacak, 2014).
These findings highlight the relationship between impaired sleep and poor SRH in this sample. Although this relationship has been reported in other studies, most focus only on sleep duration without a measure of sleep quality (Silva-Costa et al., 2015), and only a few reported a positive association between sleep quality and SRH in middle-aged adults (Hublin, Lehtovirta, Partinen, Koskenvuo, & Kaprio, 2017). A recent study reported worse SRH with insomnia symptoms in workers; however, their sample was not focused on the middle-aged worker (Kitamura et al., 2014). Among the current study’s sample, few respondents reported treatment for insomnia; however, more than half had one or more insomnia symptoms occurring at least a few times/week, which is higher than the estimate by Roth (2007) of 30% of the population. In addition, nearly half of this sample did not obtain the recommended 7 to 9 hours of sleep/night (NSF, 2015), which is similar to previous studies (Liu, Wheaton, Chapman, & Croft, 2013; Stamatakis, Kaplan, & Roberts, 2007).
It remains unclear whether the responsibilities of work combined with impaired sleep, chronic health conditions, and increasing age affect SRH. However, Taloyan, Leineweber, Hyde, and Westerlund (2015) found a twofold increase (95% CI = [1.51, 2.64]) for suboptimal SRH in workers aged 51 to 60 years, compared with workers aged 20 to 30 years, after adjusting for sex, age, income, and marital status. In comparison with the makeup of the workforce 50 years ago, workers are staying employed longer, which creates a challenge for most employers in keeping aging workers healthy (Anderson, 2015). To improve NRS and SRH in the aging workforce, early detection of and interventions for impaired sleep are essential for maintaining productivity and promoting healthy aging in this population (NSF, 2010).
This survey likely overrepresents Caucasians; however, the sample broadly reflects the age, gender, educational and marital status, and somewhat overweight condition of the middle-aged workforce in the United States. The survey methodology may have resulted in a biased sample, in which persons with poorer sleep were more likely to respond. Additional limitations of this study include the cross-sectional design, the use of self-reported and secondary data, and the fairly homogeneous sample regarding race and education. Although snoring and increased BMI are risk factors for sleep apnea, there was no objective measure of the presence or severity of sleep apnea or data regarding treatment for sleep apnea. Thus, snoring and the diagnosis of sleep apnea were not included in the models. Furthermore, important factors that may affect sleep in the aging workforce were not collected, including time spent working within the home or caring for yet older family members. Future studies could examine these factors, and examine how the working population compares with those who are not working outside the home.
Implications for Occupational Health Nursing Practice
It is important for occupational health nurses to recognize that working middle-aged adults frequently have inadequate sleep and that sleep disorders (i.e., sleep apnea and insomnia) are higher in this age group. Despite the growing body of literature regarding sleep health and the impact of impaired sleep on overall health, health practitioners ask fewer than half of patients about their sleep (NSF, 2010). In addition, only about 30% of patients are discussing their sleep with health care providers (Ye, Keane, Hutton-Johnson, & Dykes, 2013). The occupational health nurse may start the discussion with a simple sleep assessment that includes questions on sleep duration, sleep latency (the amount of time it takes to fall asleep), nighttime awakenings, use of any sleep aids, falling asleep in unplanned situations during the daytime, and being told that they snore or hold their breath during sleep. This study suggests that an additional aspect of sleep health assessment ought to include asking whether patients are experiencing NRS, waking up feeling unrefreshed after a night’s sleep, a nonspecific but important symptom of impaired sleep.
Occupational health nurses should be aware of several tools that are available to assess many of the symptoms associated with either impaired sleep or potential sleep disorders (Luyster et al., 2015). The Pittsburgh Sleep Quality Index is a well-established questionnaire to assess quality of sleep (Buysse, Reynolds, Monk, Berman, & Kupfer, 1989). The Epworth Sleep Questionnaire (Johns, 1992) can be used to evaluate for excessive daytime sleepiness. The Berlin Questionnaire may be useful in screening for possible obstructive sleep apnea (Netzer, Stoohs, Netzer, Clark, & Strohl, 1999). These tools are not intended for actual diagnosis but are used to establish risk of impaired sleep. If an actual sleep disorder is suspected, proper referral to a sleep specialist is in order.
Occupational health nurses can also provide education regarding effective sleep hygiene (routine around preparing for sleep), which could improve impaired sleep. Recommendations for healthy sleep hygiene include consistent bed times and wake times, a dark and relaxing bedroom, a comfortable bed, avoidance of using the bed for things other than sleep or sex, avoiding large meals before bedtime, and avoiding caffeine or nicotine several hours prior to bedtime (NSF, 2018). Resources available include the healthy sleep guide from the U.S. Department of Health and Human Services, National Heart, Lung, and Blood Institute: http://www.nhlbi.nih.gov/files/docs/public/sleep/healthy_sleep.pdf.
Conclusion
This study found that impaired sleep was highly prevalent, and that NRS was significantly associated with more frequent poor work performance and worse SRH in middle-aged workers aged 50 to 65. Interventions to improve sleep and decrease NRS not only may improve productivity and work performance but also may improve SRH, a predictor of morbidity and mortality. These results increase the awareness of impaired sleep in the aging workforce and highlight the need for occupational health nurses to address sleep health as an aspect of promoting a healthy work environment.
Applying Research to Practice
As the average age of worker continues to increase, the health of the aging workforce is essential to address due to factors such as this population’s increase in chronic health conditions and sleep impairment. Impaired sleep is reported to affect SRH, an important predictor of overall health. However, the association between NRS, a key feature of impaired sleep, and SRH is poorly understood, especially in the aging worker. Middle-aged workers frequently reported impaired sleep such as insomnia symptoms, NRS, and short sleep duration. Nonrestorative sleep was associated with decreased work performance. Also, NRS and short sleep duration were predictors of worse SRH. To increase SRH, the early detection of factors associated with impaired sleep and interventions to improve sleep are important for health promotion in the aging workforce.
Footnotes
Acknowledgements
The NSF has the official acknowledgment, see the original Poll. Dr. Matthew J. Hayat, PhD, for his contributions to statistical analysis.
Ethical Approval
Institutional review board (IRB) numbers: PRO14110222 (University of Pittsburgh) and H15246 (Georgia State University).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this work for last author: K24 NR016685. The other authors declare there was no funding for this work.
Author Biographies
Ashley Helvig Coombe, PhD, RN, CNE, is an assistant clinical professor in the Nell Hodgson Woodruff School of Nursing at Emory University, Atlanta, Georgia, and holds an appointment as affiliate member in the Georgia Center for Diabetes Translation Research. Her research involves young adults at risk of type 2 diabetes, focusing on sleep health.
Fayron Epps, PhD, RN, is an assistant professor at Georgia State University School of Nursing, is an affiliate faculty with the Gerontology Institute, and she completed her postdoctoral fellowship with the National Hartford Center of Gerontological Nursing Excellence. Her program of research involves evidence-based practices for promoting quality of life for African American adults living with dementia and their family caregivers.
Jiwon Lee, PhD, RN, MPH, is a clinical assistant professor in the Byrdine F. Lewis College of Nursing and Health Professions at Georgia State University, Atlanta, Georgia. Her research interests focus on the role of stress and sleep on psychological and physical health outcomes in families of children with developmental disabilities.
Mei-Lan Chen, PhD, RN, received her master’s degree in nursing from Taipei Medical University and earned her PhD degree in nursing from the University of North Carolina at Greensboro. Her primary area of research focuses on the development of theory-based physical activity programs and lifestyle interventions to reduce health disparities in older adults.
Christopher C. Imes, PhD, RN, is an assistant professor in the Acute and Tertiary Care Department at the University of Pittsburgh, School of Nursing. His research interests include examining how sleep, physical activity, and dietary habits affect wellness and cardiovascular health and the development of health promotion interventions.
Eileen R. Chasens, PhD, RN, FAAN, is an associate professor in the School of Nursing at the University of Pittsburgh and has a history of funding from the National Institutes of Health (NIH) including grants awarded by the National Heart, Lung, and Blood Institute (NHLBI), the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), and the National Institute of Nursing Research (NINR).The focus of her research is the effect of sleep disorders and daytime sleepiness on management of chronic disease.