
Abstract
Objective
Sleeping habits may greatly impact the prevalence of functional dyspepsia (FD). This study examined relationships between aspects of sleep impairment and FD.
Methods
This prospective study included university student volunteers. Following enrolment, FD was diagnosed based on the Rome IV criteria, dividing participants into an FD group or controls. The FD group was further subdivided into long-term (disease course >6 months) and short-term (disease course 3–6 months) FD groups. Participants completed the Pittsburgh Sleep Quality Index (PSQI), the Rome IV Diagnostic Questionnaire for Gastrointestinal Disorders in Adults, and a visual analogue scale (VAS).
Results
Out of 418 participants in total, sleep quality, latency, and duration, habitual sleep efficiency, sleep disturbances, sleep medication use, daytime dysfunction, and PSQI scores were higher in the FD groups versus controls. Components of PSQI scores emerged as risk factors, and were higher in the long-term versus short-term dyspepsia group. Moreover, these components were positively correlated with frequency/severity of postprandial distress syndrome and early satiation. Total PSQI scores were positively correlated with VAS scores.
Conclusion
Several PSQI components are associated with FD occurrence, symptom frequency, and symptom severity.
Introduction
Functional dyspepsia (FD) is highly prevalent worldwide, with a prevalence that varies between regions. For example, in Western countries the prevalence of FD ranges between 10% and 40%, and in Asia, it ranges between 5% and 30%.1,2 Although FD rarely leads to mortality, it can strongly affect quality of life,3,4 however, an effective treatment to manage this disease remains unavailable. 5 The first Rome classification system for functional gastrointestinal disorders was published in 1990, and subsequently the Rome I, Rome II, and Rome III classifications were published in 1992, 1999, and 2006, respectively. 6 With publication of the Rome IV classification in 2016, the definition of FD was further clarified. 7
Sleep impairment is a common medical issue within the general population worldwide, and previously published studies have demonstrated a strong association between sleep impairments and functional gastrointestinal disorders, such as FD and irritable bowel syndrome.8,9 For instance, in one study, 68% of patients with FD reported poor sleep quality. 10 Studies that include self-reported sleep and gastrointestinal symptoms often measure sleep impairment using the Pittsburgh Sleep Quality Index (PSQI), a well-validated measure of perceived sleep quality. Components of the PSQI include subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medication, and daytime dysfunction. 11 However, the question of whether sleep impairment is independently associated with the development of FD remains unresolved. Additionally, the relationship between facets of sleep impairment risk factors and the physical symptoms of FD also remains unknown.
The aim of the present study was to identify risk factors of sleep impairment and development of FD, and to identify how sleep impairment may contribute to gastrointestinal symptoms in patients with FD.
Participants and methods
Study population
This prospective study was conducted at Xi’an Medical University, Xi’an, Shaanxi, China, between January 2018 and October 2018. Individuals interested in participating were recruited from the student population of Xi’an Medical University, through flyers, emails, and student unions. Participation in this study was voluntary, and questionnaires and study information were anonymized. Individuals were informed that participation would not affect course grades, and participants were compensated with a free health consultation provided by the researchers. 12 The study was approved by the Institutional Ethics Committee of Xi’an Medical University (Xi’an, Shaanxi, China; approval date, 8 July 2017). Written informed consent was obtained from all participants before beginning the study, and the study was compliant with relevant Equator network guidelines.
Participants completed questionnaires, including the Rome IV criteria that was used to diagnose FD. Participants also underwent examinations including electrocardiogram, abdominal ultrasound, X-ray scan, and routine blood tests in order to exclude other diseases. For analysis, participants were subdivided into those with or without FD.
Students who volunteered to participate in the study were included unless they met the following exclusion criteria: other organ system disease that may affect the study results, current pregnancy, currently lactating, or unwilling to participate.
Questionnaires
The PSQI, Rome IV Diagnostic Questionnaire for Gastrointestinal Disorders in Adults, and a visual analogue scale (VAS) were used in the study. All participants were given the approved PSQI, which is a 19-item self-rated questionnaire measuring perceived sleep quality. The PSQI differentiates between poor and good sleep quality by considering seven components: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medication, and daytime dysfunction over a one-month period. Answers are scored based on a 1–4 Likert-scale, where an overall sum ≥5 indicates poor sleep quality. 11
The Rome IV Diagnostic Questionnaire for Gastrointestinal Disorders in Adults was used to classify FD gastrointestinal symptoms. Questionnaires were also administered to measure postprandial distress syndrome and epigastric pain syndrome, including postprandial fullness, early satiation, epigastric pain that had occurred in the last 3 months, and to establish the time duration of the disease. 13 Postprandial fullness was evaluated on a scale including little impact on daily life, affecting diet and daily life but not sleep, and seriously affecting sleep. Early satiation severity was evaluated as mild, moderate, or severe.
The VAS was used to measure severity of epigastric pain, and comprised a 10-cm scale, with marks for numbers ranging from 0–10, with 0 indicating no pain, 1–3 indicating mild pain, 4–6 indicating moderate pain, 7–9 indicating severe pain, and 10 indicating pain so severe as to be unbearable. 14
Specialist doctors (ZPH, SML, TS and YYZ) used a standard explanation to describe the tests, so that the participants were able to complete the questionnaires independently, without external interference, and with a time restriction of completion within 30 min from the start of the test. The doctors then calculated the PSQI and VAS scores from completed questionnaires.
Statistical Analyses
All statistical analyses were performed using SPSS software for Windows, version 17.0 (SPSS Inc., Chicago, IL, USA). Continuous variables are presented as mean ± SD and categorical variables are presented as proportions and percentages. Student’s t-test was used to compare continuous variables, and χ2-test of independence was used to compare categorical variables. Multivariate logistic regression analysis and Spearman’s correlation coefficient test were also conducted. A two-sided P-value < 0.05 was considered to be statistically significant.
Results
Prevalence of FD
According to the formula of sample size estimation used in medical research (N = Z21–α/2(1–p)/ε2p), the average prevalence of FD in Asia is approximately 20%. Therefore, a sample size of at least 308 participants was required for the present study.1,2
A total of 418 participants were enrolled into the study, and comprised 130 male and 288 female participants aged 18–25 years (mean age, 20.97 ± 1.07 years). Among the participants, 145 (34.69%) were diagnosed with FD, including 40 (27.6%) males and 105 (72.4%) females. There was no statistically significant difference in the proportions of males and females with or without FD (P = 0.269).
Sleep impairment and incidence of FD
All PSQI score components (i.e. subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medication, and daytime dysfunction), and PSQI total scores, were significantly higher in the FD group than in the control group (all P < 0.05; Figure 1).
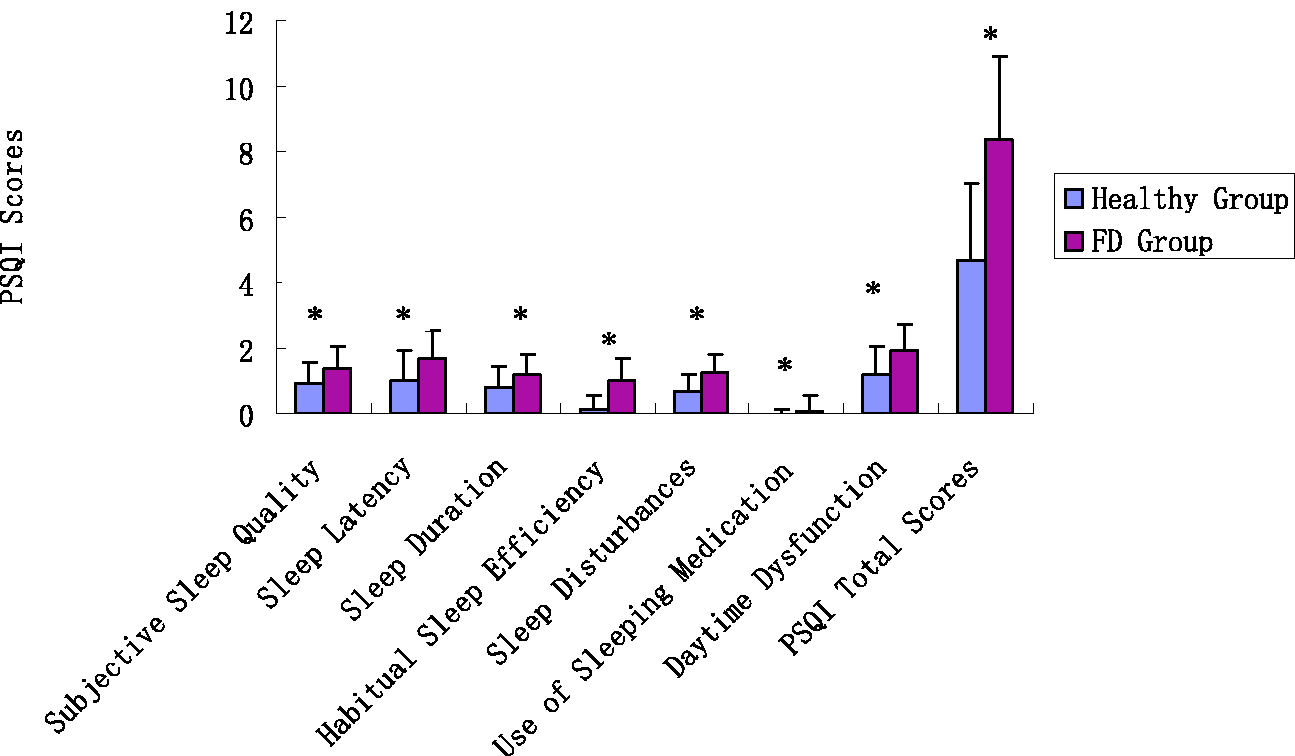
Pittsburgh Sleep Quality Index (PSQI) scores between healthy adults (n = 273) and those with functional dyspepsia (FD, n = 145). All PSQI score components (subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medication, and daytime dysfunction), and total PSQI score, were higher in the FD group versus healthy controls. *P < 0.05, FD group versus healthy controls.
Moreover, multivariate logistic regression analysis showed that subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleep medication, daytime dysfunction, and total PSQI scores, were significant risk factors for FD (all P < 0.05; Table 1).
Multivariate logistic regression analysis of sleep impairment risk factors for functional dyspepsia.
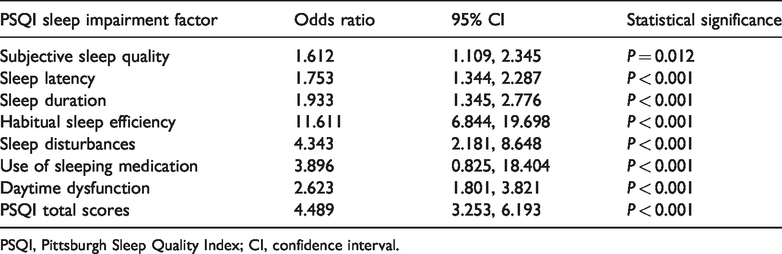
PSQI, Pittsburgh Sleep Quality Index; CI, confidence interval.
Sleep impairment and development of FD
The FD group was further subdivided into two groups according to the duration of FD gastrointestinal symptoms: Long-term FD, defined as FD gastrointestinal symptoms lasting more than 6 months (n = 55); and short-term FD, defined as FD gastrointestinal symptoms lasting 3–6 months (n = 90).
In the long-term FD group, PSQI scores for subjective sleep quality, sleep latency, sleep disturbances, use of sleeping medication, daytime dysfunction, and PSQI total score were all higher than in the short-term FD group (all P < 0.05; Figure 2). There was no statistically significant between-group difference in PSQI scores for sleep duration and habitual sleep efficiency (P > 0.05).

Pittsburgh Sleep Quality Index (PSQI) scores between adults with long-term functional dyspepsia (FD, n = 55) and those with short-term FD (n = 90). In the long-term FD group, PSQI scores for subjective sleep quality, sleep latency, sleep disturbances, use of sleeping medication, daytime dysfunction, and PSQI total score were all higher in the long-term FD group versus the short-term FD group (all P < 0.05). There were no statistically significant between-group differences in PSQI scores for sleep duration and habitual sleep efficiency.
Sleep impairment and gastrointestinal symptoms of FD
The gastrointestinal symptoms analysed included postprandial fullness and early satiation (defined as postprandial distress syndrome), and epigastric pain (defined as epigastric pain syndrome). PSQI scores, including subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleep medication, daytime dysfunction, and total scores were all higher in participants with gastrointestinal symptoms compared with the control group (all P < 0.05; Figure 3).

Pittsburgh Sleep Quality Index (PSQI) scores between adults with functional dyspepsia gastrointestinal symptoms and healthy controls: (A) PSQI scores between adults with postprandial fullness (n = 101) and healthy participants (n = 273); (B) PSQI scores between adults with early satiation (n = 92) and healthy participants (n = 273); and (C) PSQI scores between adults with epigastric pain (n = 58) and healthy participants (n = 273). *P < 0.05 versus healthy controls.
Regarding postprandial distress syndrome (postprandial fullness and early satiation), various aspects of sleep quality were further evaluated using Spearman’s correlation coefficient. Subjective sleep quality, sleep latency, sleep disturbances, daytime dysfunction and total scores were positively correlated with the frequency of postprandial fullness (all P < 0.05; Table 2). Additionally, subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, daytime dysfunction, and total scores were positively correlated with the severity of postprandial fullness (all P < 0.05; Table 2). Subjective sleep quality, sleep disturbances, and total scores were positively correlated with the frequency of early satiation. In addition, subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, daytime dysfunction and PSQI total scores were all positively correlated with the severity of early satiation (all P < 0.05; Table 2).
Correlation between components of sleep impairment and postprandial distress syndrome symptoms (postprandial fullness and early satiation).

PSQI, Pittsburgh Sleep Quality Index; NS, no statistically significant correlation (P > 0.05).
Regarding epigastric pain syndrome, sleep disturbances were positively correlated with the frequency of epigastric pain. Subjective sleep quality, sleep latency, sleep duration, sleep disturbances, daytime dysfunction and PSQI total scores were all positively correlated with the VAS scale for pain severity (all P < 0.05; Table 3).
Correlation between components of sleep impairment and epigastric pain syndrome.
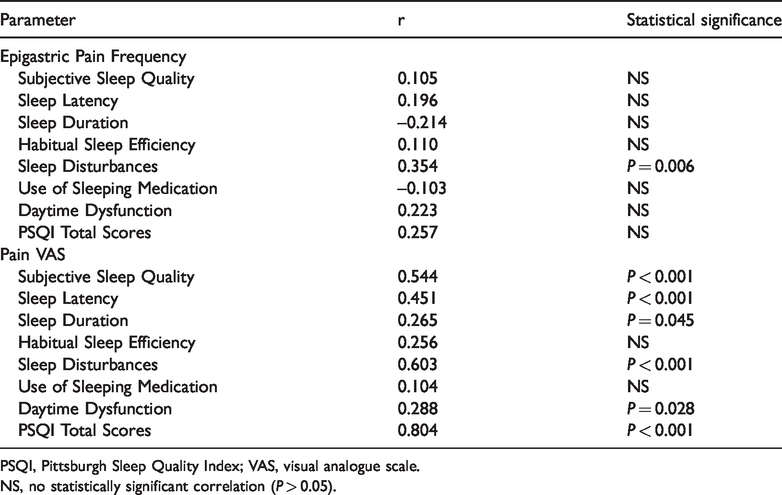
PSQI, Pittsburgh Sleep Quality Index; VAS, visual analogue scale.
NS, no statistically significant correlation (P > 0.05).
Discussion
Functional dyspepsia is a functional gastrointestinal disorder characterized by the absence of organic changes. The underlying mechanism of FD remains unknown, but it is a very common ailment in the global population,15,16 with a prevalence that varies between 7% and 45% worldwide.17,18 A large-scale study in France concluded that the prevalence of FD was about 15–21%, 19 while in Korea, the prevalence of FD is thought to be approximately 46.5%. 5 In China, multicentre FD prevalence studies are lacking. In the present single-centre young adult study population, the prevalence of FD was found to be 34.69%, which is within the range reported by previously published studies.4,20
Sleep impairments severely affect quality of life in adults, and functional gastrointestinal disorders, including FD and irritable bowel syndrome, are common clinical diseases, often accompanied by sleep disorders.21,22 Associations between poor sleep quality and functional gastrointestinal disorders have been evaluated in previous studies.23,24 Correctly identified and promptly managed sleep impairments may greatly improve gastrointestinal symptoms and quality of life in patients with FD. 21 However, whether sleep impairment is independently associated with the development of FD, and the relationship between sleep impairments and FD gastrointestinal symptoms, remains unknown.
The PSQI is a self-rated questionnaire measuring an individual’s recent history of sleep quality and duration during the last month, and has been well validated and widely used for measuring sleep impairment in patients with functional gastrointestinal disorders.11,25–27 In the present study, sleep impairments were confirmed to be common in patients with FD, similar to the findings from previous studies.8,28,29 Additionally, subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleep medication, and daytime dysfunction were found to be worse in patients with FD than in control participants. In patients with longer-term FD (more than 6 months duration), subjective sleep quality, sleep latency, sleep disturbances, use of sleeping medication, daytime dysfunction, and PSQI total score were found to be significantly higher than in those with shorter-term FD, suggesting that factors relating to sleep quality deteriorate with the development of FD. As observed in the present study, subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleep medication, and daytime dysfunction were all risk factors for FD. FD has an impact on the sleep-wake cycle and causes poor sleep quality, and conversely, poor sleep strongly promotes the development of FD. 30 Since the gut-brain axis has feedback loops that may influence sleep regulation pathways through immune activation, intestinal permeability, and enteroendocrine signalling, any disturbances in these processes may also contribute to impaired sleep quality in patients with FD. 31
In the present study, sleep impairment was also found to be positively correlated with specific FD symptoms, including postprandial distress syndrome and epigastric pain syndrome, in terms of both their frequency and severity. Gastrointestinal symptoms such as postprandial fullness, early satiation, epigastric pain in postprandial distress syndrome and epigastric pain syndrome, were found to be associated with decreased subjective sleep quality, prolonged sleep latency, shortened sleep duration, and decreased habitual sleep efficiency. Recent studies have also confirmed that both rapid eye movement sleep and slow wave sleep in patients with FD are decreased.32,33 As cytokines may modulate the sleep-wake cycle, sleep disturbances may upregulate proinflammatory cytokines, such as tumour necrosis factor-α, interleukin-1 and interleukin-6, which can have a profound impact on FD symptoms.34–36
The results of the present study may be limited by several factors. The study was conducted at a single centre with a relatively small sample size of volunteers, which may have introduced some sample bias and may limit the generalisability of the present findings. Further studies are required to validate the present results.
In conclusion, the present study found that sleep impairments, evaluated on the basis of subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleep medication, and daytime dysfunction, are common in patients with FD. Subjective sleep quality, sleep latency, reduced sleep duration, habitual sleep efficiency, sleep disturbances, increased use of sleeping medication, and daytime dysfunction were found to be risk factors of FD. Sleep impairment was also positively correlated with the frequency and severity of FD gastrointestinal symptoms, including postprandial distress syndrome and epigastric pain syndrome. These results suggest that FD may be prevented by ameliorating sleep impairments.
Footnotes
Acknowledgements
We should like to thank Prof. Hui-Min Wang for his assistance in this study.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by a grant from the Guangzhou key medical discipline construction project fund to Zhen-Peng Huang.