
Abstract
Asian Americans have a higher prevalence of developing type 2 diabetes mellitus (T2DM) compared with White Americans. A two-phase evidence-based project developed specifically for Chinese American employees at an urban catering company worksite was led by a registered nurse/certified diabetes educator. The purpose of this project was to (a) identify Chinese employees at risk for T2DM, and (b) develop and implement a customized diabetes prevention program in Chinese. In Phase 1, Chinese employees were screened for T2DM risk factors using a Chinese version of the Canadian Diabetes Risk Assessment Questionnaire (CANRISK). Thirty-five people, who represented 58% of the Chinese employees, were screened; two were newly diagnosed with T2DM, and two were newly diagnosed with prediabetes based on the screening scores, nonfasting blood glucose, and hemoglobin (Hb) A1c tests. In Phase 2, 23 Chinese employees were interviewed and their remarks were used to modify the National Diabetes Prevention Program (DPP). Six Chinese employees participated and completed the DPP. Risk scores, nonfasting blood glucose, and HbA1c were obtained and pre- and postprogram data were compared. Upon completion of the program, participants showed an average reduction of nonfasting blood glucose of 30 mg/dL (1.7 mmol/L), and a reduction of HbA1c by 0.32 points (3 mmol/mol). This evidence-based project emphasizes the importance of screening for diabetes in the worksite setting and using linguistically sensitive materials.
Keywords
The American Diabetes Association (ADA) recommends testing for type 2 diabetes mellitus (T2DM) and prediabetes in asymptomatic Asian adults beginning at 45 years of age (ADA, 2018a). At an international airline food service company in the urban Midwest in the United States, Asian Americans recently accounted for 30% of the employees. Due to cultural and language barriers, Asian Americans at this company had not been regularly screened for T2DM nor offered any formal diabetes prevention programs.
Literature Review
Immigration to the United States has grown significantly in the last two decades with Asians now accounting for 27% of all U.S. immigrants (Zong, Batalova, & Hallock, 2018). Compared with Whites, Asian Americans had a higher rate of diagnosed diabetes 7.4% versus 8.0%, respectively (ADA, 2018b). The rate of undiagnosed diabetes was 51% in Asian Americans, ranking the highest of all ethnic and racial subgroups (National Institutes of Health, 2015). In addition, the World Health Organization (WHO) has indicated that Asian Americans had a higher percentage of body fat than Whites of the same age, sex, and body mass index (BMI), and the proportion of Asian Americans with higher percentage body fat who had developed diabetes and cardiovascular disease occurred below the general population normal value of a BMI of 25 kg/m². Therefore, WHO suggested that a BMI of 23 kg/m² be used as the overweight cut-off point for the Asian population (WHO Expert Consultation, 2004).
Diabetes Screening
Because of the asymptomatic nature of the early stages of the T2DM and being unaware that hyperglycemia could have serious consequences, early screening and detection has been shown to be important steps to help people prevent and reduce disease-related complications (Dall et al., 2014; Griffin, Little, Hales, Kinmonth, & Wareham, 2000). A diabetes risk tool using age, gender, BMI, family history of T2DM, high blood pressure, and physical activity helped identify people at risk of developing diabetes and contributed to earlier detection of the disease (Dall et al., 2014; Griffin et al., 2000). Once identified as being at risk, individuals could be enrolled into diabetes educational programs, including programs delivered within the worksite, ensuring more favorable health outcomes (Dall et al., 2014; Griffin et al., 2000). Diabetes screening was found to be a feasible and acceptable approach when using a risk score calculated from screening tools that detect diabetes in high-risk populations such as Asian Americans.
Diabetes Prevention
The National Diabetes Prevention Program (DPP), which includes healthy eating, physical activity, stress reduction, and problem-solving skills, is a well-established and cost-effective program approved by the Centers for Disease Control and Prevention (CDC) in partnership with public and private organizations to reduce the growing problem of prediabetes and T2DM (CDC, 2018). The Diabetes Prevention Program Outcomes Study conducted from 2002 to 2013 was found to be effective in the prevention or delay of T2DM with lifestyle intervention in a high-risk population. At a 10-year follow-up, the rate of developing T2DM was reduced by 34% and the delay of T2DM was about 4 years when compared with a placebo group (National Institute of Diabetes and Digestive and Kidney Diseases, 2018). A study conducted by Yeh and colleagues (2016) further demonstrated that a culturally appropriate translation of the DPP curriculum into Chinese had a positive impact on Chinese immigrants who were at a high risk of developing diabetes, with participants averaging a 3.5% weight reduction over 6 months. It was also suggested that the revised DPP was acceptable and effective in facilitating lifestyle changes in Chinese immigrants (Yeh et al., 2016). These research findings provided evidence that diabetes risk screening had the potential for demonstrating the positive outcomes for detection, so that early intervention could be initiated for those with T2DM or those at risk for T2DM. These studies also indicated that effective and simple lifestyle interventions had a positive impact on diabetes prevention and the reduction or delay of the onset of T2DM.
Research has shown that ethnic disparities, racial and cultural differences, and language insufficiencies significantly impact the quality diabetes screening and care among Asian Americans (Kim, Ford, Chiriboga, & Sorkin, 2012; Richard, Alexandre, Lara, & Akamigbo, 2011). Therefore, we sought to employ these evidence-based screening and prevention strategies among Asian Americans. The purpose of this two-phase evidence-based project developed for Chinese Americans was to (a) identify Chinese employees at risk for type 2 diabetes, and (b) develop and implement a customized diabetes prevention program in Chinese.
Planning
Project Design
This evidence-based project was divided into two phases: Phase 1 was a cross-sectional study in which we identified Chinese employees who were at risk for T2DM, while Phase 2 involved the use of group interviews among Chinese employees with and without diabetes to explore diabetes education needs and interests. This information informed the development of a 12-week culturally tailored DPP, which was offered to the employees identified in Phase 1 who were at risk for T2DM. A pretest–posttest design was also conducted to compare and evaluate the effectiveness of the culturally tailored DPP among workers included in this second phase of the study.
Setting
The site chosen for this evidence-based project was an international airline food service company based in a large Midwest city in the United States. This company had a network of over 20 “kitchens” and more than 2,000 employees. Participants for this project were recruited from the organization’s midwest kitchen. At the time of the project, the midwest kitchen employed over 300 people, among whom 30% identified as Asian, 32% African American, 29% Hispanic, and 9% White. Of the Asian employees, 56% were Chinese and were predominately from mainland China. The majority were women who immigrated to the United States within the past 5 to 10 years. Their annual average wage was close to US$20K. The midwest kitchen operated 24 hours a day, 7 days a week, with three shifts. Employee shift times vary and could occur anytime across the 24-hour day. Most Chinese employees worked on the second shift and car-pooled to work, and many found speaking English difficult. Furthermore, Chinese employees were identified as either speakers of Mandarin or Cantonese and all read Chinese.
Of all kitchens within this company, only the midwest kitchen had an on-site nurse-managed health clinic (NMHC) that provided primary care and occupational health care services. The NMHC provided primary care to employees and had approximately 1,500 annual patient visits. The NMHC was affiliated with a large academic medical center, which helped to ensure the clinic’s mission to provide outstanding, cost-effective, on-site primary care and wellness services to their employees. However, employees from China were less apt to use the clinic compared with other ethnic groups, despite the fact that a telephone translation service was available at the clinic.
This evidence-based project was conceptualized and led by a registered nurse, who was a Certified Diabetes Educator, and was bilingual in Chinese and English. At this worksite setting, she identified the need for diabetes screening and implementation of a diabetes education program for Chinese employees. Chinese was the written language, and Mandarin was the spoken language, to facilitate learning and communication. The project was fully supported by the key stakeholders at the company. Institutional review board (IRB) at Rush University deemed that the review was not required for this evidence-based project.
Measures
This evidence-based project used several measures, including the Canadian Diabetes Risk Questionnaire (CANRISK), nonfasting blood glucose measure, and hemoglobin (Hb) A1c.
CANRISK questionnaire
The CANRISK questionnaire is a publicly available, free tool for assessing the risk of diabetes. There were 12 variables: age in years (<45 = 0 points, 45-54 = 7 points, 44-64 = 13 points, >65 = 15 points); gender (female = 0 points, male = 6 points); BMI in kg/m2 (<25 = 0 points, 25-29 = 4 points, 30-34 = 9 points, >35 = 14 points); waist circumference in inches (men: <37 = 0 points, 37-40< = 4 points, >40 = 6 points; women: <31.5 = 0 points, 31.5-35 = 4 points, >35 = 6 points); daily physical activity, in other words, doing some physical activity for at least 30 minutes daily (yes = 0 points, no = 1 point); eating vegetables or fruit daily (every day = 0 points, not every day = 2 points); history of hypertension (no = 0 points, yes = 4 points); history of elevated blood glucose (no = 0 points, yes = 14 points); birth of a large infant (no or NA = 0 points, yes = 1 point); family history of diabetes (points each for mother, father, brothers/sisters, children); ethnicity (White = 0 points, Black = 5 points, East Asian = 10 points, South Asian = 11 points); and level of education (some college or a college degree = 0 points, high school diploma = 1 point, some high school or less = 5 points).
The CANRISK questionnaire score ranges from 0 to 85. A score of 0 to 32 indicated a low to moderate risk of T2DM with no HbA1c follow-up needed; a score of 33 to 42 indicated a moderate to high risk of T2DM with an HbA1c test recommended every 3 to 5 years along with health care provider consultation; and a score of >43 indicated a very high risk of T2DM with a recommendation of an annual HbA1c test and health care provider consultation. The CANRISK scores were validated against diagnostic gold standard blood tests (fasting plasma glucose [FPG] and 2-hour oral glucose tolerance test) in predicting dysglycemia. Canadian Diabetes Risk Assessment Questionnaire was found to be a statistically valid tool when tested in a Canadian multiethnic population (Robinson, Agarwal, & Nerenberg, 2011). The CANRISK questionnaire had been translated into 13 different languages; the Chinese paper version was used for this project (Canadian Pharmacists Association, 2018). Recently, this instrument had also been validated in a Chinese population and with minor modifications was shown to be a reliable and valid tool for diabetes screening (Guo et al., 2018).
Nonfasting blood glucose and HbA1c
Nonfasting blood glucose was a simple blood test used to measure blood glucose levels at any time of the day; values vary depending on the last time food was consumed. The American Diabetes Association recommended nonfasting/random blood glucose levels between 80 and 180 mg/dL (4.4-10.0 mmol/L). If nonfasting blood glucose ≥200 mg/dL (11.1 mmol/L) with classic symptoms of hyperglycemia, T2DM could be diagnosed (ADA, 2018a). HbA1c was a glycated hemoglobin test that measured average blood glucose over the past 3 months. According to ADA diagnostic criteria for T2DM, an HbA1c value of ≥6.5% (48 mmol/mol) substantiated a diagnosis of T2DM, and a range of 5.7% to 6.4% (39-47 mmol/mol) substantiated a prediabetes diagnosis. HbA1c was a valid measurement for diagnostic testing of diabetes and the indication of diabetes control (ADA, 2018a).
Implementation
Phase 1
Phase 1 addressed the identified problem that Asian Americans had a higher prevalence of diagnosed and undiagnosed rate of T2DM, and Chinese employees at the midwest urban kitchen (where the project was conducted) had only been minimally screened for diabetes. First, the implementation of the paper-based Chinese version of CANRISK was used to address the identified language problem and to identify Chinese employees who were at risk for T2DM. To complete this questionnaire, in addition to obtaining subjective data, the project leader obtained height and weight to calculate BMI, and also obtained a waist measurement in inches for risk score calculations. Second, employees were tested for nonfasting blood glucose. If employees had a nonfasting blood glucose ≥200 mg/dL (11.1 mmol/L) or a CANRISK score ≥40, an HbA1c was also obtained to confirm the diagnosis of T2DM and prediabetes. The screening was conducted at the midwest kitchen on three separate dates and times.
Phase 2
To better understand the Chinese employees’ diabetes concerns and learning priorities, group interviews were conducted. Group interviews were conducted during lunch breaks for first shift employees and before the shift start for second shift employees. Three open-ended questions were asked in Chinese: “What are your concerns about diabetes?” “What would you like to learn about diabetes?” and “Give me one issue that most interests you about diabetes.” Their answers were collected, field notes were taken, and data were analyzed.
The data collected from the group interviews were used to adapt the DPP. A modified and tailored 12-week, DPP lifestyle modification course was developed based on the identified topics from Chinese employees. Screening results showed that the majority (83%) of Chinese employees who participated in this project had less than a high school education. Therefore, the educational materials were adjusted to use common words, the avoidance of medical vocabulary, breaking down long sentences to short phrases, and inserting pictures to facilitate learning. All educational materials were translated into Chinese.
After the development of the revised DPP, Chinese employees at risk for diabetes who were identified in Phase 1 were contacted either face-to-face or by phone conversation to participate in the program. The original plan to deliver the DPP was to use group sessions. However, because identified employees worked different shifts and days of the week, the course was adjusted to be delivered weekly on an individual basis. The 12-week course was delivered in Chinese by the project leader; educational materials in Chinese were handed out at each session to facilitate learning. The course was convened generally during the first shift’s lunch break or before the beginning of the second shift. The implementation of Phase 2 was completed in the summer of 2017. Postprogram data, including CANRISK scores, HbA1c, and nonfasting blood glucose, were collected.
Evaluation
Data Analysis
Sample demographics were described using frequencies. The preprogram and postprogram CANRISK scores, nonfasting blood glucose, and HbA1c results were compared and analyzed using paired t tests and correlational statistics. For the group interview data, the project leader reviewed her notes after each groups and then collectively after the completion of the group interviews. Data were analyzed and employees’ indicated topics and their learning priorities were identified.
Phase 1 Results
Table 1 includes the CANRISK screener and demographic characteristics of the employees (N = 35) screened in Phase 1. These employees represented 58% of all of the Chinese employees at the midwest kitchen. The participants were mostly (97%) female between the ages of 18 and 64 years. The majority (83%) had an educational level of high school or less. Slightly less than half (49%) were overweight with a BMI ≥25 kg/m2, 3 % were obese with a BMI ≥30 kg/m2, and 17% had a waist circumference of ≥35 inches, putting them at greater risk for T2DM. The results also showed 89% reported daily physical activity of >30 minutes, which meets the United States’s recommended physical activity guidelines of obtaining 30 minutes of aerobic physical activity 5 or more days/week (ADA, 2018a), and 94% reported eating vegetables or fruit daily. Other diabetes-related risk factors were identified, including 17% with a history of high blood pressure, 17% who had relatives who were diagnosed with diabetes, and 3% reported giving birth to a large baby weighing >9 pounds. The screening data showed a mean score of 26.9 (SD = ±9.7), which falls into the low- to moderate-risk category (score = 0-32), with 63% (n = 22) of participants scoring within this range. One third (34%) of the participants fell into the moderate- to high-risk category (score = 33-42), while 3% of the participants fell into the high-risk category (scores >43; Canadian Pharmacists Association, 2018).
Diabetes CANRISK Screening Scores (N = 35)
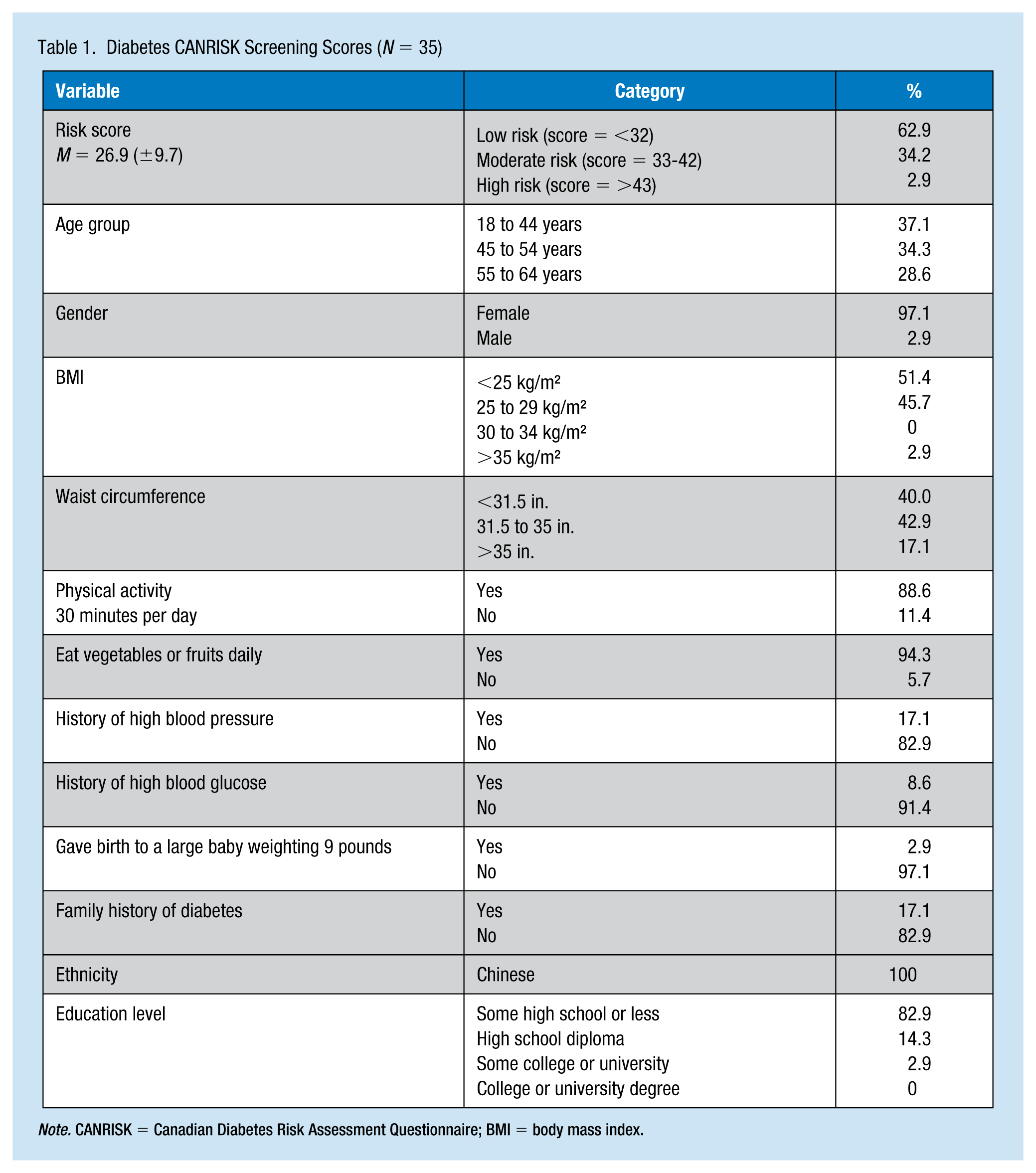
Note. CANRISK = Canadian Diabetes Risk Assessment Questionnaire; BMI = body mass index.
The average nonfasting blood glucose was 120.4 mg/dL (6.7 mmol/L; ±38.0). There were four participants (11%) with elevated HbA1cs. Concluding from the risk scores, nonfasting blood glucose readings, and HbA1c levels, two people (5.7%) were newly diagnosed with T2DM, and another two people (5.7%) were newly diagnosed with prediabetes.
Phase 2 Results
Group interview and adaptation of the DPP
Six groups of three to four participants (N = 23) were interviewed. Interviews lasted between 5 and 15 minutes. They were Chinese employees ranging from low- to high-risk categories for T2DM. During the group interviews, they asked questions including “What should I eat?” “What should I not eat?” “Is White rice bad for you?” and “Can I eat fruit?” Based on the feedback of the group interviews, the “diabetes meal plan” was identified as a priority topic for diabetes education. The project leader adapted the DPP to meet the needs of the employees. See Figure 1 for the topics covered in the 12 diabetes education classes, including a class on “Carbohydrate Counting and Chinese Menu Samples.”
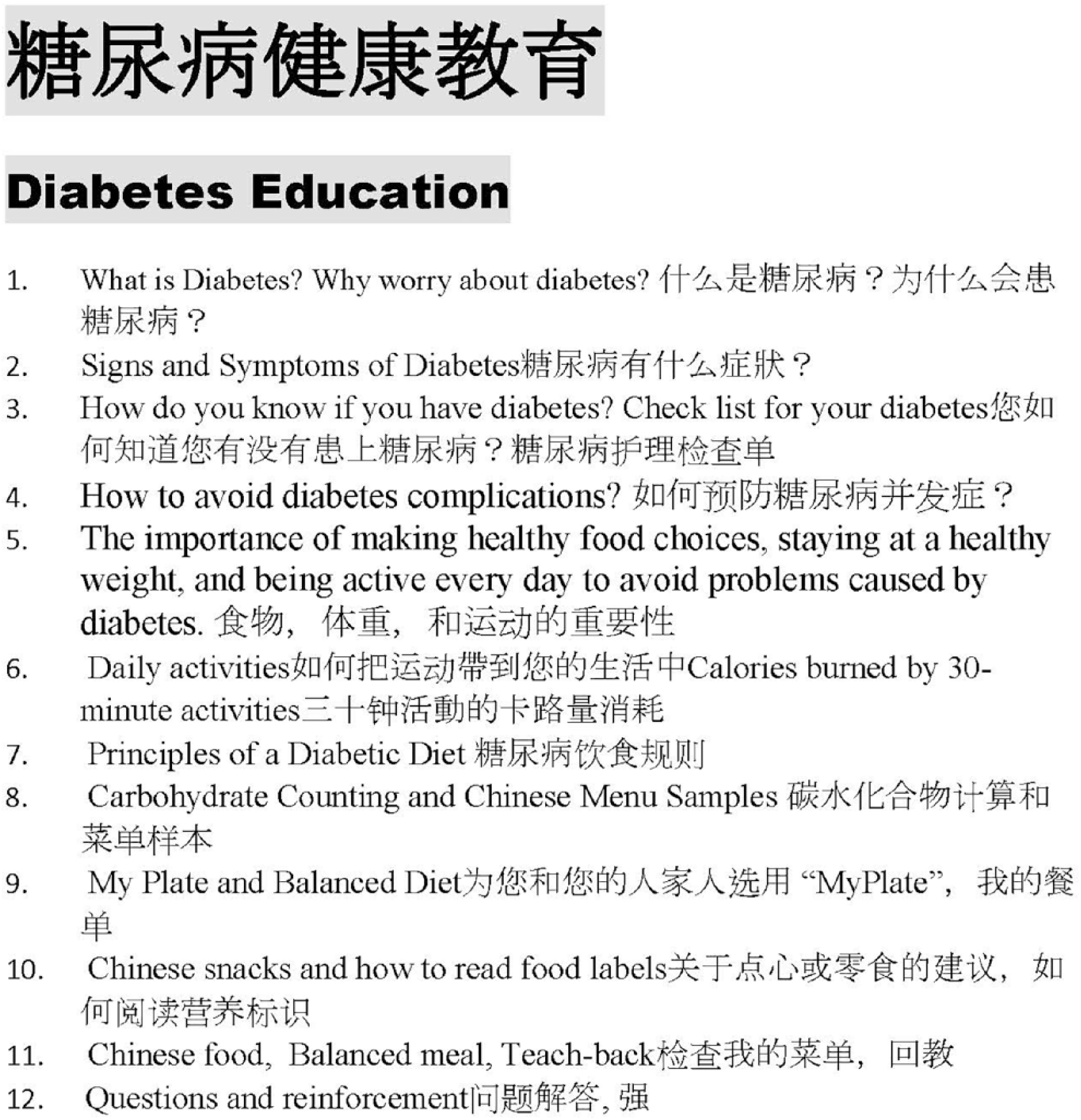
Diabetes educational weekly topics
DPP Participation
The DPP program was offered to the 12 employees who were at moderate to high risk for diabetes. The DPP program was also offered to one employee who already had a diagnosis of T2DM. Of these 13 employees, six (46%) were successfully recruited to take part in the DPP. Of these, two were newly diagnosed with T2DM, two were newly diagnosed with prediabetes, one had a moderate- to high-risk score with an HbA1c of 4.7% (28 mmol/mol), and one had preexisting T2DM with an HbA1c of 8.3% (67 mmol/mol). Of the six participants, five were female and one was male. The preprogram data for these six participants showed a mean risk score of 38.8 (±3.1), a mean HbA1c of 6.48% (47 mmol/mol; ±1.2), and a mean nonfasting blood glucose reading of 174.5 mg/dL (9.7 mmol/L; ±68.8). The six participants were given individual educational sessions, weekly, for 12 weeks. The 12-week sessions were successfully delivered in Chinese by the project leader with a 100% participation rate for all of the participants.
After the completion of the 12-week DPP course, postprogram data were obtained and compared with preprogram data (see Table 2). Figure 2 (pre- and postprogram results comparison) showed these data as a histogram. On the CANRISK, the mean postprogram total risk score was 49 (±10.3), which was increased by 10.2 points when compared with the preprogram data. In comparison with preprogram data, postprogram data showed BMI risk score was reduced by 0.83 points; the waist circumference was reduced by 1 point. The incidence of daily activity >30 minutes increased by 0.33 points and the consumption of vegetables or fruit daily was increased by 0.67 points. The postprogram data analysis also showed a mean HbA1c of 6.17% (44 mmol/mol; ±1.0) which was a reduction of 0.32 (3 mmol/mol), and a mean nonfasting blood glucose of 144.5 mg/dL (8.0 mmol/L; ±42.8), which was a reduction of 30 mg/dL (1.7 mmol/L).
Pre- and Postprogram Results of Diabetes Screening and Education Program Delivered in Chinese (n = 6)
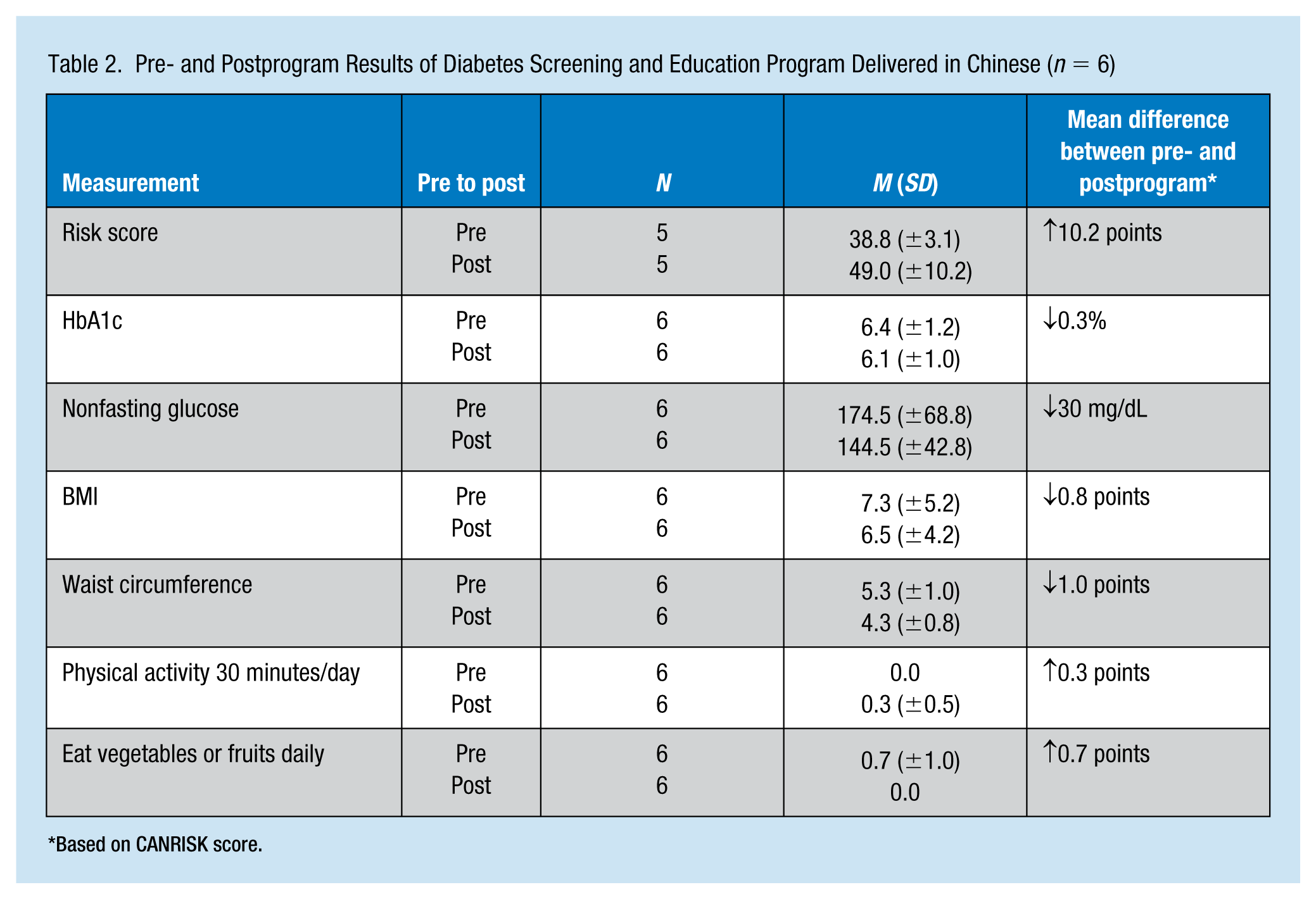
Based on CANRISK score.
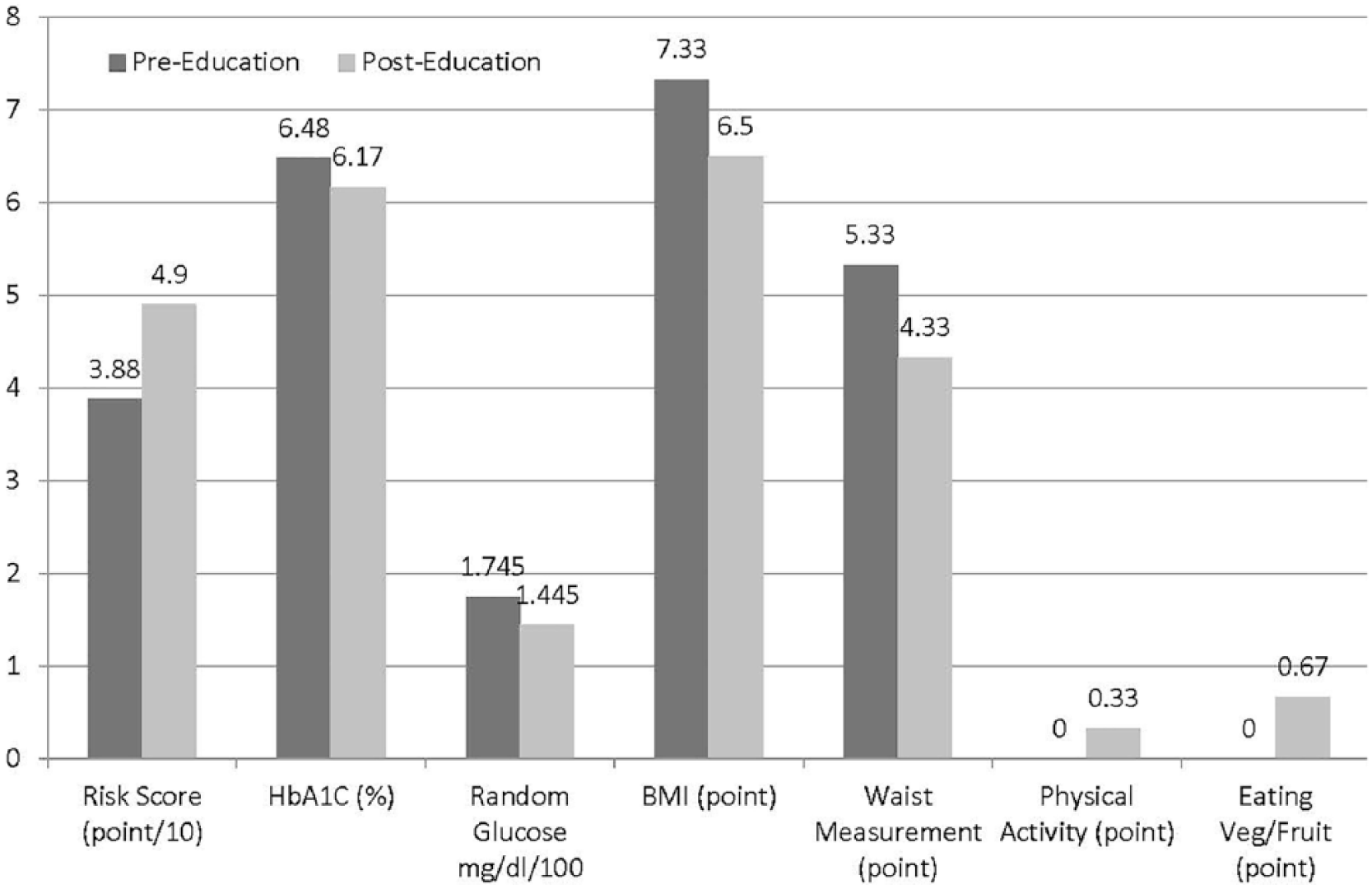
Pre- and postprogram results based on CANRISK scores.
Discussion
Results of this evidence-based project suggested the important role that the diabetes educator played in the worksite setting using linguistically sensitive materials for the screening and education of Chinese employees who were at risk for developing T2DM. By the end of this evidence-based project, more than half of the Chinese employees were screened and the prevalence of T2DM and prediabetes was identified. When compared with 8.0% of diagnosed diabetes in Asian Americans in the United States (ADA, 2018b), the 5.7% prevalence of T2DM and the 5.7% prevalence of prediabetes in Chinese employees were much lower than the predicted rate for this population; however, the sample size in our study was small. Also, at the time of the diabetes risk screening, 89% of the Chinese employees reported that their jobs required walking all the time. As the work required physical activity, it may have contributed to the lower prevalence of T2DM. For the four employees who were newly diagnosed with T2DM and prediabetes due to the diabetes screening, they were informed of their high blood glucose readings and they all participated in the DPP course. The health care providers at the NMHC were aware of their health conditions and a follow-up protocol was initiated after diagnosis.
By the end of this evidence-based project, participants had a better understanding of the impact of diet and physical activity on blood glucose and HbA1c. During the 12-week education sessions, participants became more familiar with the setting and function of the worksite-based NMHC and had increased their visits to the clinic for diabetes and other health-related problems. In addition, by emphasizing the availability and utilization of the telephone translation service, which includes Chinese to English interpretation, Chinese employees were more comfortable in continuing to come to the NMHC for their health care needs.
The results of this evidence-based project showed positive effects on the Chinese employees’ diabetes-related health outcomes evidenced by a reduction of HbA1c, nonfasting blood glucose reading, BMI, and waist circumference, as well as increased daily physical activity and daily vegetable or fruit consumption. These positive outcomes were compared over the 1-year period from the beginning of the diabetes risk screening to the end of the evidence-based project. When compared with research on individualized diabetes health coaching, an HbA1c reduction of 0.32% (3 mmol/mol; Sherifali, Viscardi, Bai, & Ali, 2016) was similar to the outcome of this project.
There were several strengths of this project. First, key stakeholders strongly supported the project. Second, the project leader was a certified diabetes educator and bilingual in Chinese and English. Third, the DPP was successfully modified and tailored to Chinese employees’ needs and was culturally and linguistically sensitive. Fourth, participants’ education level was taken into consideration when developing the DPP.
A limitation of this project was that the scores of the CANRISK screening tool may not be an ideal tool to use for pre- and posttest comparison because of pre- and postprogram awareness of high blood glucose. One of the questions on the CANRISK screening tool asked about the “history of high blood glucose.” As 83% of the participants were not aware of their high blood glucose at the time of the preprogram, they scored 0. However, some of the participants had become aware of their high blood glucose findings by the time of the postprogram, so they scored 14 points on this question, instead of 0. This awareness increased their CANRISK scores. As a result, participants who had a positive reduction on all modifiable objectives did not show a reduction in total risk scores. Moreover, as one of the participants had preexisting T2DM and was on multiple glucose lowering medications, the outcomes and effectiveness of the DPP could not be assessed with certainty. Another limitation was the modest sample size. Although the evidence-based project was effective in reducing diabetes risk factors in Chinese employees in this setting, the results may not be generalizable to the larger population.
Implications for Occupational Health Nurses
In this worksite setting, due to its multiple ethnicities, the bilingual registered nurse/certified diabetes educator served an important role in the health maintenance and disease screening and prevention of T2DM for the Chinese employees. As the successful results of this pilot project demonstrated, the company can continue to use the same concepts to screen and conduct disease prevention programs for other ethnic subgroups by incorporating their unique culture, language, and learning priorities. Occupational health nurses were part of a multidisciplinary team working closely with health care providers and other key stakeholders by contributing their expertise to reduce health inequalities and employee sickness absences, and therefore, reducing the overall health burden in the work place.
Conclusion
The project problem and purpose were identified based on the needs of the organization and aligned with the NMHC’s mission statement. The prevalence of T2DM and prediabetes among Chinese employees was examined. A culturally and linguistically tailored DPP was developed, implemented, and evaluated. The results of the project demonstrated effective reduction of risk factors for T2DM, namely, HbA1c, nonfasting blood glucose, BMI, waist circumference, and increased daily physical activity and increased daily consumption of vegetables or fruit. This evidence-based project was the first of its kind at this nurse practitioner run, worksite employee health clinic, offered for Chinese employees. It served as a basis for future health care outcome improvement projects for employees at this food service company. When approaching diabetes screening and education for Chinese Americans who speak Chinese, it was critical to use translated materials tailored to their educational level and health care needs, to be successful.
In Summary
Chinese employees at the midwest kitchen were screened for type 2 diabetes by using the Chinese paper version of CANRISK. The prevalence of diabetes and prediabetes was obtained.
The culturally and linguistically tailored diabetes prevention program (DPP) was developed and translated into Chinese and delivered in Chinese at the worksite for Chinese employees.
Chinese participants effectively reduced the risk factors of type 2 diabetes as a result of the modified DPP.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.