
Abstract
Workplace bullying is associated with a host of negative outcomes for the worker who is the target of bullying, as well as for the organization where the bullying occurs. Moreover, we know that rates of bullying are particularly high in health care settings; however, we are less familiar with the factors that may reduce workplace bullying in hospitals. Thus, this study was conducted to determine whether the humor orientation styles of individuals, including nurses working in hospitals, as well as their managers’ leadership styles, can influence perceptions of bullying in the workplace. Using data from 459 workers employed in a large hospital in the Southern United States, we examined associations between the Multidimensional Sense of Humor Scale, which has four dimensions, as well as the Multifactor Leadership Questionnaire, with three leadership substyles, and their associations with the risk of being bullied. We observed that one of the four humor subscales, Humor Appreciation, did affect perceptions of bullying in the workplace. The other three, Humor Recognition, Humor Production, and Humor for Coping, did not. However, the leadership styles of managers did affect reports of negative acts. In fact, transformational leadership was associated with 22% of the variance in reports of decreased bullying activity. This work is consistent with previous work on the importance of leadership styles for creating positive work environments, particularly in hospital settings. Given these findings, we offer suggestions for leaders to further improve nursing communication.
Introduction
In the 1970s, scholars, lawyers, and the general public began to wrestle with the phenomenon of “sexual harassment” (Baker, 2007). Although behaviors that constituted harassment had been part of work culture, perhaps since the beginning of organizing itself, the labeling of the behavior created a new awareness of the negative acts, as well as the ability to do something about it (Jones, 2006). Much like sexual harassment, workplace bullying is a long-standing problem; yet only in the 1980s did scholars even begin to critically examine worker mistreatment labeled as “mobbing” (Leymann, 1990) or “bullying” (Adams, 1992). Einarsen (1999) defined bullying as “systematically subjected to aggressive behavior from one or more colleagues or superiors over a long period of time” (p. 16). Namie and Namie (2009) argued that workplace bullying is repeated, health-harming, verbally abusive behavior. The conduct is threatening, humiliating, and intimidating; it is work-related sabotage, or a combination of these.
The importance of workplace bullying has been established across the world, including countries as diverse as Scandinavia (Einarsen, 1999), the United States (Lutgen-Sandvik, 2006, 2008), Greece (Karatza, Zyga, Tziaferi, & Prezerakos, 2017), Australia (Hutchinson, 2014), and Korea (Oh, Uhm, & Yoon, 2016), and the results are quite consistent. Hoel and Beale (2006) found that approximately 10% of workers in the United Kingdom report workplace bullying within 6 months of employment, and 25% report bullying occurrences within a 5-year time frame. In the United States, nearly half of the adults in the workplace experience bullying behaviors during their career, which is an estimated 71.5 million workers (Namie & Lutgen-Sandvik, 2010).
Studies show that workplace bullying is associated with poor mental health, high levels of absenteeism, and low levels of workplace productivity (Tye-Williams & Krone, 2015). Emotional symptoms further include low self-esteem, hostility, nervousness, hypersensitivity, and social isolation (Matthiesen & Einarsen, 2001; Matthiesen & Einarsen, 2004). Physical symptoms include loss of strength, chronic fatigue, sleeplessness, and stroke and even suicide (Namie & Namie, 2009). These problems are not insignificant; victims of prolonged workplace bullying can mimic or exceed the levels of stress found in persons diagnosed with post-traumatic stress syndrome (Nielsen & Einarsen, 2012) and even escalate to thoughts of suicide (Lutgen-Sandvik & Tracy, 2012). Although the deleterious individual effects of bullying make it worthy of study, research demonstrates that the costs far exceed the personal harm to victims. Organizations find that there are numerous organizational concerns with bullying, including burnout or turnover, which can be quite costly in terms of money, and time spent training new employees (Tracy, Lutgen-Sandvik, & Alberts, 2006).
Bullying in Health Care
In nursing, it is estimated to cost up to 125% of nurse’s annual salary to replace a nurse who has left their job (Stagg & Sheridan, 2010). These numbers can be quite substantial to organizations considering that in 2007, over 40% of those who were bullied left their jobs as a result of the bullying, an estimated 21 million people leaving their jobs (Stagg & Sheridan, 2010). Giorgi et al. (2016) suggested that bullying is particularly expensive for health care organizations given the psychological and physical health impact on nurses, and argue that the low autonomy and high workloads for health care workers contribute to the high rates of bullying. In a meta-analysis of 136 articles that included work from 38 countries, and over 151,347 health care workers (predominantly nurses), Spector, Zhou, and Che (2014) found that 23% of nurses had been bullied in the prior 6 months, 47% had been bullied in the prior year, and 70% had been bullied at some point in their careers. Thus, if bullying leads to job dissatisfaction and turnover, the resulting expenses can be staggering.
There are other indirect organizational expenses related to bullying and employee and patient health. Research shows that nurses who are victims of bullying have decreases in their cognitive abilities, as well as in their ability to interact with large numbers of patients (Laschinger, Grau, Finegan, & Wilk, 2010), and that in hospitals, bullying is associated with verifiable illnesses and workplace absenteeism (Kivimäki, Elovainio, & Vahtera, 2000), which can substantially affect both continuity and quality of care. Glambek, Skogstad, and Einarsen (2018) found that that the impact of bullying can disrupt a nurse’s feeling of job security for 2 years, thus making the nurse feel vulnerable and unsafe in his or her work environment. This could lead to workers seeking employment elsewhere. This distraction and lack of commitment can have additional important consequences; bullying among nurses has been significantly related to both emotional distress and medical errors (Wright & Khatri, 2015). Given that lives are literally on the line, the relationship to medical errors is particularly problematic. This is not surprising given MacIntosh, Wuest, Gray, and Cronkhite’s (2010) finding that targets of bullying find less satisfaction in their work and are less committed to their jobs and patients.
Theory
Although research has verified that bullying is an ongoing, troublesome workplace behavior, particularly in health care, much less work has sought to explore the factors that mitigate perceptions of bullying. For example, why do some people experience bullying more than others? Furthermore, why does workplace bullying flourish in some environments and not others? This study explored two aspects that may contribute to how and why those differences in bullying experiences exist, including an individual’s sense humor and the leadership they experience from their supervisor.
Humor
Given that bullying creates informal power inequities, it is important to look at a tool that can be used to deal with bullying informally, as well. It is a common belief that people use humor to alleviate stress, as well as use it as a coping mechanism (Butler, Hoedemaekers, & Russell, 2015; Williamson, 2007). Research indicates that people frequently use humor to deal with anxiety (Wanzer, Booth-Butterfield, & Booth-Butterfield, 2005); it can “moderate the effect of life stressors” (Avtgis & Taber, 2006, p. 14) and can directly affect a person’s level of depression (Porterfield, 1987). Given the positive benefits of using humor to deal with stress, researchers have suggested that organizations can use humor to help employees have more positive work experiences (Deal & Kennedy, 2000).
Examining how humor operates in work relationships, Radcliffe-Brown (1965) argued that humor reduces tension and conflict, particularly between individuals who must coordinate work activities for the success of a larger goal, even if that teamwork is antithetical to individual goals. Thus, humor may reestablish power for a victim by highlighting their ability to take control of a situation and/or minimize the negative impact of the aggression, thus decreasing the control of the bully in the situation (see Mulkay, 1988; Thorson & Powell, 1991; Thorson & Powell, 1993).
Thorson and Powell (1991) found that humor has several components. First, there is humor recognition: the ability to see humor in various situations. Second, there is humor appreciation: the ability to enjoy humorous events and people, life’s absurdities, and oneself as a humorous person. Third, there is humor production, which is the ability to generate humorous moments through strategies such as telling jokes and funny stories. Finally, there is coping humor: when humor is used as an adaptive mechanism, such as being able to laugh at problems and/or deal with difficult situations.
Given these varying elements of humor, it is important to determine if some areas of humor are more important to understanding and responding to bullying than others. Thus, this research sought to more fully explore the relationship between people’s orientation toward humor and reports of bullying. We hypothesized that all of the dimensions of humor will be related to reports of decreased bullying, with the exception of humor recognition. Simply being able to identify humor does not mean that the employee will appreciate the intended meaning, or accept the bid for lightheartedness—in fact, they might see through the veiled attempt at using humor for an aggressive act. However, appreciation might lead to further acceptance, production might lead to engagement with the humorous activity, and coping might be a strategy to deal with potentially negative acts.
Leadership
Noon and Blyton (1997) noted that though humor can be used to release tension about power inequity, it can also be a dysfunctional form of escape by allowing people to laugh at the problem, while not challenging the problem itself. Although individual differences, such as humor, might affect perceptions of bullying, it is clear that employees’ negative behaviors are also an organizational phenomenon that may need to be dealt with on a larger scale. Stohl and Schell (1991) argued that organizational members, who cause problems for others, are typically the products of dysfunctional group norms. Some organizations’ norms might enable bullying (see Keashly & Neuman, 2002; Salin, 2003) while laying the blame on individuals. In fact, Salin (2003) argued that bullying can only emerge in cultures that allow it to occur, with components such as power imbalances, tolerated aggression, and workplace dissatisfaction, all contributing to the culture of bullying.
Despite the negative effects of bullying, research does indicate that positive leadership in the organization can mitigate the behavior. Goodboy, Martin, Knight, and Long (2017) found that supervisors who allow workers some control over task completion, seek ways to reduce work strain, and provide appropriate levels of work-related support can reduce perceptions of workplace bullying. Given the significant interpersonal and organizational outcomes associated with workplace bullying, this research seeks to explore the variations in leadership styles that may support or inhibit the development of bullying behaviors in the workplace.
Not all leadership is good leadership. Fox and Spector (2002) found that poor organizational leadership, including low levels of communication about tasks and expectations, affected coworkers’ interactions. For instance, laissez-faire, or hands-off, leadership creates frustration in groups and can escalate tension (Einarsen, 1999). Olsen, Bjaalid, and Mikkelsen (2017) argued that negligent leadership can lead to workplace stress and divisive worker relationships, such as isolating and excluding coworkers. Einarsen, Raknes, and Matthiesen (1994) found that dissatisfaction with leadership was strongly related to bullying behaviors in the workplace and that poor leaders allow victims to be vulnerable. Skogstad, Einarsen, Torsheim, Aasland, and Hetland (2007) found that employees with poor leaders experienced bullying significantly more than those who had more constructive leadership in their organization. Within health care settings, these results are consistent with extant research: Anderson (2015) found that nurses who often struggle with competing work demands and poor leadership often feel unsupported and turn to aggression toward their coworkers in an attempt to manage their workload and alleviate frustration. Thus, it is important to explore positive forms of leadership that can eliminate or reduce vulnerability to bullying and improve coworker relationships.
Transformational leadership
In recent years, one of the most commonly studied leadership models is Bass’s concept of “transformational leadership” (Avolio, Bass, & Jung, 1999; Bass & Avolio, 1993). In their conceptualization of leadership, there are three primary types of leadership: transformational leadership, transactional leadership, and management-by-exception (MBE). Transformational leaders are charismatic and inspirational with their subordinates, and they challenge them to do their best work in a positive and individualized way (Bass & Avolio, 1993). Employees of transformational leaders respect and trust their supervisors. Also, the employees feel that their emotional needs are being met. Aldoory and Toth (2002) showed that employees prefer transformational leadership. Thus, it is likely that this type of leadership will lead to more positive supervisor/subordinate and coworker relationships, and lead to fewer instances of workplace bullying.
Transactional leadership
Although not as effective as transformational leaders, transactional leaders are more common in organizations. They provide rewards for good performance, watch for aberrant behaviors, and intervene when issues arise, yet they avoid making controversial decisions (Bass, 1990). According to Bass, transactional leadership often leads to mediocrity. Transactional leaders lack the charisma and ability to motivate employees to look beyond their individual goals and focus on the larger organizational needs. Yet, Dussault and Frenette (2015) looked at the work environment and found both transactional and transformational leaders can be beneficial in creating a workplace environment that is not conducive to bullying activities.
Management-by-exception (MBE)
Even less effective than transactional leadership is MBE. Although part of the theory of transformational leadership, MBE is not technically leadership, but rather poor management; it lacks initiative and goal setting. In fact, those who use MBE take action only when there is evidence of something not going according to plan in the organization (Bass, 1985).
Given this research on leadership, transformational leaders should create positive climates where bullying does not have an opportunity to develop, whereas transactional leaders leave some room for anti-bullying success, and MBE managers might provide fertile ground for hostile behaviors. Thus, we posit that the transformational style leadership will result in less reports of bullying than either transactional and MBE leadership, while the transaction style leadership will result in fewer reports of bullying than MBE.
Method
Study Participants and Recruitment
Workers from a hospital located in the southern region of the United States were invited to participate through an employee newsletter distributed by human resources via email. In a short text box describing the study, they were told that researchers at a local university were examining workplace bullying and that all information collected would be completely confidential. They were also told it would take approximately 15 minutes of their time. In the newsletter, they were given a web address to a SurveyMonkey questionnaire and no identifiable information was asked. They were able to complete the survey in the privacy of their own home or office.
Instrumentation
Following a series of demographic questions such as age, race, gender, and occupation, participants were asked to complete the Multidimensional Sense of Humor Scale (MSHS) developed by Thorson and Powell (1993). The MSHS is a 24-item, 5-point Likert-type scale, from “strongly agree” to “strongly disagree,” with all items loading at .50 or higher. The scales, used as continuous variables, encompassed four subscales: Recognition of Humor, Production of Humor, Appreciation of Humor, and Using Humor as a Coping Mechanism. An average score from each subscale was used. A low score indicates a high level of humor in a particular area. In other words, an average of 1 on a subscale would mean that a participant thought they strongly agreed they used humor in that way for every item. Thorson and Powell (1993) reported an overall alpha reliability coefficient of .92 for the scale; the alpha in this sample was .90. Subscale reliabilities ranged from .88 to .94.
The second measure was Bass’s Multifactor Leadership Questionnaire (MLQ). The MLQ is a widely used five-factor measuring tool to identify three styles of leadership as discussed above: Transformational Leadership, Transactional Leadership, and MBE (a non-management style). Leadership styles are measured using a 5-point Likert-type scale from “frequently” to “not at all.” Thus, being “high” in the leadership style is represent by a low number.
Transformational leadership is identified by questions that indicate a manger inspired subordinates, or provided a clear vision. Items included samples such as “Specifies the importance of having a strong sense of purpose.” Transactional leadership is more traditional management, and is represented by staying within organizational regulations, and can be seen in items such as “Is effective in meeting organization requirements.” MBE is represented by not acting until necessary with items such as “Fails to intervene until problems become serious.” The subscales were constructed as continuous variables.
We did not specify who counted as the supervisor, but rather let the participants answer with the supervisor of their choosing. Overall, this questionnaire was found to have a Cronbach’s alpha of .86 (Muenjohn & Armstrong, 2008). The subscale alphas range from .85 to .93 in this study. An average score for each subscale was used.
The final measure was the Negative Acts Questionnaire–Revised (NAQ-R) that measures a person’s experience as the target of 22 bullying behaviors, such as “Gossip or rumors have been spread about you” and “Being exposed to an unmanageable workload,” as well as questions about physical aggression. Responses are measured on a Likert-type scale from “never” (1) to “daily” (5), thus measuring both the negative acts and the frequency of those acts. The scores were averaged across the 22 bullying behaviors. The higher the average score, the more likely the person was experiencing bullying. Cronbach’s alpha for the NAQ-R was .93. It was used as a continuous variable in analysis.
Data Analysis
The data analysis was conducted using IBM SPSS 24.0. We first conducted descriptive statistics to describe the study sample including frequencies for categorical variables (e.g., race, occupational group, gender, employment status) and means and standard deviations for continuous (e.g., years of age, length of hospital employment). We then conducted ordinary least squares (OLS) regression to examine the relationships between the participant’s humor orientation and their reports of being bullied. We ran a second analysis of the workers’ reports of their manager’s transformational leadership style and the worker’s risk of being bullied. For the linear regression models, beta estimates, both standardized and unstandardized, were calculated, as well as the explained variance expressed as the R-squared estimates. Results were considered statistically significant when p < .05.
Results
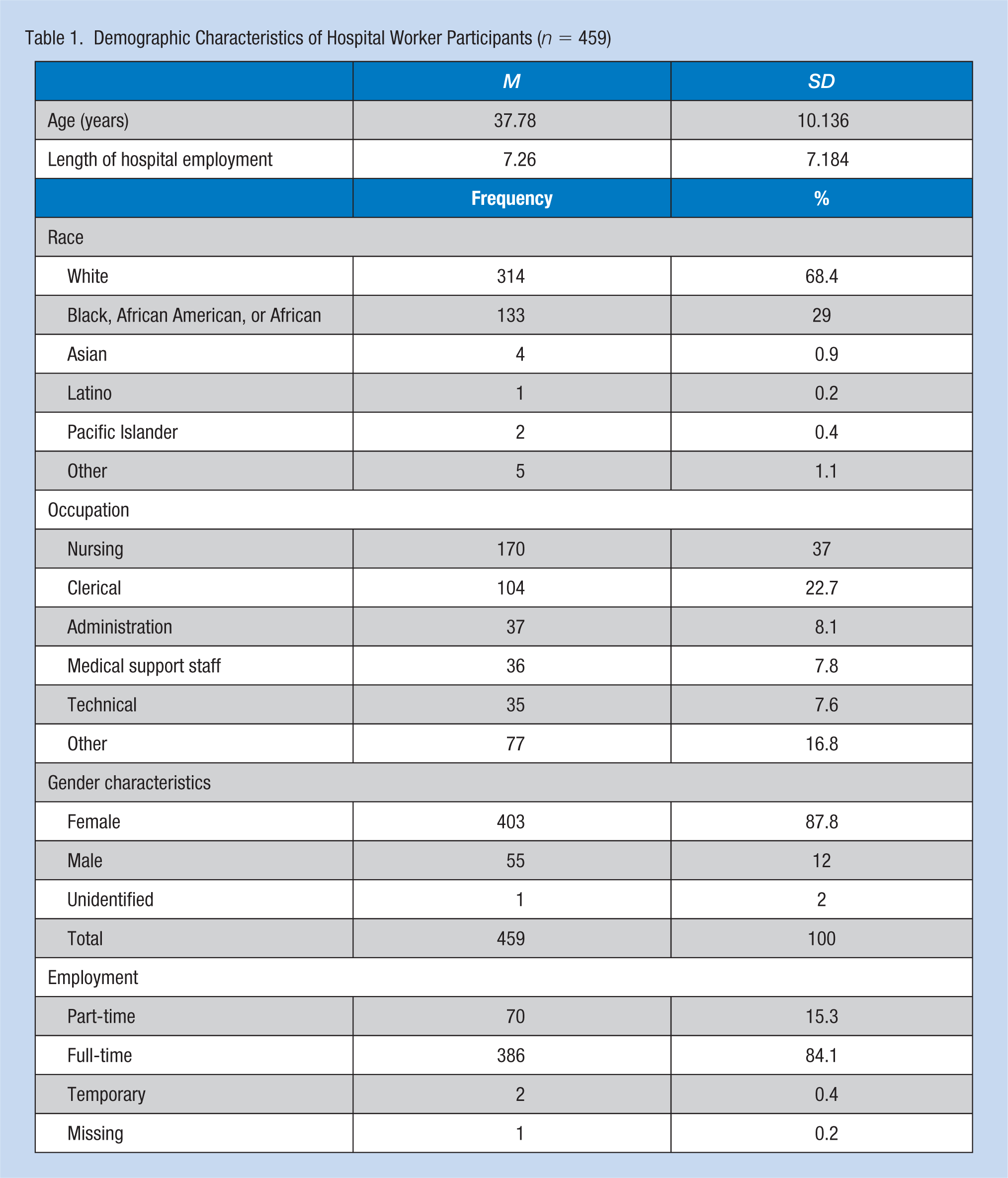
A total of 459 subjects (female = 87.6%, male = 12.4%) participated in this study. Refer to Table 1 for participant demographics. The age of participants varied from 20 to 66 years (M = 37.3, SD = 10.14). Occupations in the hospital varied: 170 (37%) were nurses, 104 (22.7%) were clerical, and the remainder identified as administration, doctors, educators, support staff, or technical staff. The majority of participants were White, non-Hispanic (69.1%), while African Americans were the next highest group represented (27%). The employees had been at the hospital for an average of 7.26 years, with a range of 2 weeks to 38 years.
Demographic Characteristics of Hospital Worker Participants (n = 459)
Our first set of hypotheses explored the relationships between people’s sense of humor and their reports of bullying in their hospital. As noted in Table 2, only one form of humor orientation, humor appreciation resulted in fewer negative acts, β = −.15, t(317)= −2.65, p = .009, was confirmed. The unstandardized beta (−.149) tells us that for every .149 increase in the humor appreciation scale, there is a 1-point decrease in the NAQ-R scale. There were no statistically significant relationships between recognition, humor production, humor for coping, and the reports of bullying acts.
Linear Regression Analysis of the Worker’s Humor Orientation and Manager’s Leadership Styles on Worker’s Risk of Being Bullied
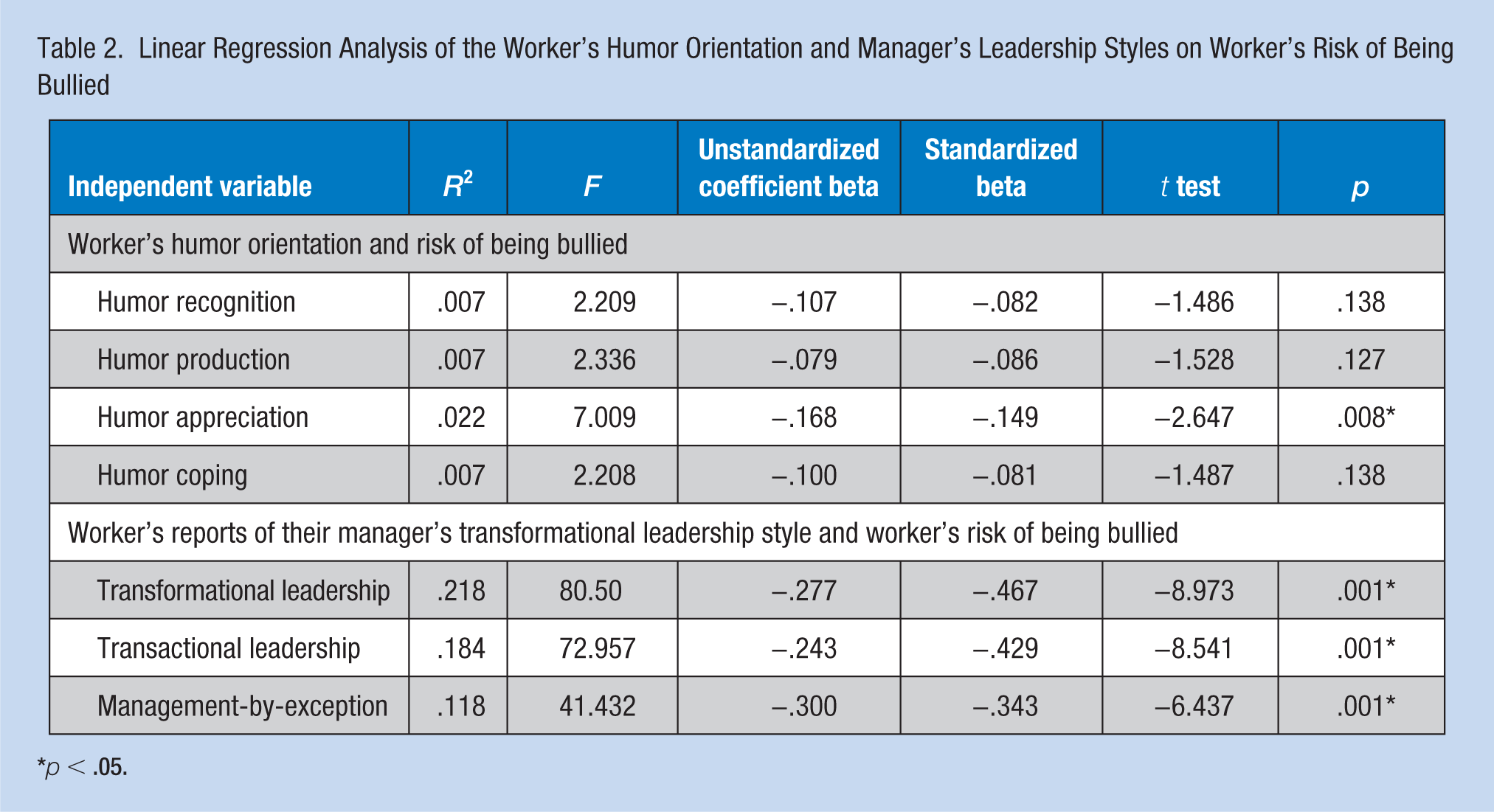
p < .05.
We then turned to an examination of hospital employees’ perceptions of their supervisor’s leadership behaviors. We predicted that both transformational and transactional leadership styles would result in fewer reports of bullying than MBE. As predicted, transformational style leadership was associated with the least amount of negative acts reported, β = −.47, t(294) = −8.97, p = .000, R2 = .22. The unstandardized beta (−.467) suggests that it was followed by the transactional style leadership, β = −.43, t(330) = −8.85, p = .000, R2 = .18, and finally the MBE style leadership, β = −.34, t(317) = −6.64, p = .000, R2 = .12. Note that there was a negative, significant relationship for each style, though transformational leadership accounted for 22% of the variance.
Discussion
The goal of this work was to examine the ways in which people process the messages they receive, as well as examine organizational cultural factors that can contribute to, or diminish, bullying practices.
Workplace bullying is an ongoing and significant problem that affects the productivity and emotional and physical health of employees (Tye-Williams & Krone, 2015). This study helped us better understand more about how an individual difference, such as humor orientation, as well as an organizational difference, such as leadership practices, may affect people’s experiences of bullying. First, humor is comprised of varying factors, including an ability to recognize humor as well as appreciating humor, being able to generate humor, and the ability to use humor to cope with difficult situations. Results indicate that people who are higher in humor appreciation report fewer acts of bullying, though no other form of humor predicted bullying reports.
Individuals who appreciate humor are less likely to see bullying comments or behaviors as bullying; simply recognizing humorous situations, using humor for coping, and not being able to produce humor jokes or make others laugh do not relate to perceptions of decreased bullying. This finding needs to be further researched to better understand the role of humor in bullying perceptions. Mills and Carwile (2009) argued that teasing is an ambiguous act that challenges people while maintaining a potential “out” through joking or humor, while bullying is a purely negative act. Perhaps the humor appreciation contributes to people’s ability to make humorous attributions about ambiguous acts, thus labeling them “teasing” or “joking” rather than bullying. It is also possible that individuals who are predisposed to appreciate humor are more likely to see humor in potentially aggressive or bullying acts and, thus, respond in ways that make the bully less likely to continue. However, there was no evidence in these data that humor production contributed to fewer reports of bullying activities, so that is unlikely. Humor production deals with how funny a person is, or perceives himself or herself to be; thus at this time, there is no evidence that humorous people are buffered from bullying more than non-funny people. Furthermore, using humor to cope with negative situations, or trauma, does not affect a person’s ability to see the negative acts when they occur, nor are they more likely to assign hostile meaning to potentially ambiguous situations.
Although Humor Appreciation is the only humor subscale that affected perceptions of bullying, and albeit in a statistically minor way, organizational leadership style plays a much clearer role in health care workers’ perceptions of bullying. These data imply that the underlying processes of reducing negative acts may be most effectively tackled with strong, involved, and charismatic leadership styles. First, among three leadership styles, the transformational style was the most effective in reducing negative acts. Its R2 was the largest, accounting for 22% of the variance in decreased reporting in bullying activities, which indicates that its relationship with fewer negative acts was the strongest among three leadership styles.
Leaders who involve their members, use positive interaction styles, and create long-term visions with their employees create an environment where bullying is less likely to become challenging. These findings further support Stohl and Schell’s (1991) notion that problematic behaviors do not develop in a vacuum but are representative of the culture in which they are embedded. In addition, our finding support Dussault and Frenette’s (2015) study of leadership styles and the environments they create, yet have taken the results a step further to include health care employees, an important group whose professional successes and failures can quite literally influence others’ lives. Given that workplace bullying is an increasingly important issue for both health care employees and their employers, multi-viewed approaches to better understanding the problem can be useful.
Limitations and Future Directions for Research
This study has several limitations that need to be considered. First, the sample is limited to those working in a hospital, many of them in high stress positions. Future studies could examine other high stress positions, such as first responders, to see if these results generalize to other stressful occupational settings, as well as explore other, less stressful, workplace settings. Future research can also examine the differences between occupations within hospitals.
Furthermore, a closer look at sex and gender roles is very important. This study, given the sample, was predominantly female (nearly 88%), thus is hard to generalize to both sexes. Moreover, although the NAQ is the most widely used scale to measure bullying, it only measures whether particular bullying behaviors have occurred and the frequency of the behavior. It does not measure how much the behaviors troubled the target. Thus, something that happens daily might be insignificant, while something that only happens occasionally might be more hurtful.
Implications for Occupational Nursing Practice
As we continue to wrestle with workplace bullying, it is important to consider how organizational culture and climate contribute to these negative acts to determine how to minimize them. Hospitals are high stress environments where lives are quite literally on the line. Thus, it is important to examine what contributes to effective nursing practices, and occupational nurses are poised to be at the forefront of these issues given their additional training focused on the promotion of health and well-being, when we know how bullying undermines the well-being of nearly everyone bullied—as well as bystanders and patients of bullied caregivers.
These findings can assist occupational health nurses to identify transformational leadership style characteristics to help create more positive work environments, which will in turn reduce mental and physical work–related strains. It is not enough just to promote good nurses but to recognize and foster good leaders with the ability to motivate others with shared vision and ideals to move the organization forward. Leadership selection, training, and mentorship for nursing managers should be ongoing. Supporting leaders can help foster and create a better climate for all hospital employees.
Clinical skills alone do not create good leaders, nor should they be the sole criteria for promotion. Hospitals need to develop ways to identify nurses skilled in communication and conflict management skills, who are able to create cohesion among their peers, and can develop camaraderie in tough situations. It is important to nurture the skills of those individuals who can work across teams, and specialty groups, as well. Thus, upper level management need to consider real ways to prevent episodes of workplace bullying through effective leadership, as well as discussions about the importance of group norms in organizational culture. With the stresses of a hospital and immediate patient needs, it is often easy to forget the importance of climate and culture that ultimately can affect patient care. The variance accounted by transformational leadership highlights leadership is truly not just about nurses managing tasks and running shifts, or serving as liaisons between doctors and other staff, but also managing and motivating people—creating a vision and culture that permeates a work climate for all employees. Once selected and trained, with ongoing support, leaders can be encouraged to involve their staff by remaining open and positive, while creating lasting positive cultures to enhance a collegial and civil workplace, to reduce bullying.
Finally, given the pervasiveness of bullying in hospitals, health care organizations should encourage anonymous reporting of bullying behaviors, and be willing to follow-up with interventions to help bystanders intervene and targets defend themselves. Like sexual harassment, bullying needs clear reporting processes, ongoing training to sensitize employees to the issues, and empower victims and bystanders to speak-up. According to the American Association of Occupational Health Nurses (AAOHN; 2018), occupational health nurses have the “combined knowledge of health and business that they blend with health care expertise to balance the requirement for a safe and healthful work environment with a ‘healthy’ bottom line.” Given that very definition, occupational health nurses are uniquely poised, from the inside of health care, to address bullying within hospitals as a critical safety threat facing the profession that can be overcome with effective communication, leadership training, and organizational support.
Conclusion
It is often easy to tell adult victims of bullying “to deal with,” or “be the bigger person,” but the reality is that victims of bullying suffer short-term and long-term mental and physical health consequences. In hospitals, where the health of patients is the priority, administration cannot overlook or minimize the importance of negative behaviors that undermine the employees’ health, as well as their ability to serve patients. This study reveals that there may be a predisposition to humor appreciation that helps some people receive potentially negative acts without assigning a negative valence, other humor orientations do not affect perceptions of bullying activities, and even if they did, there are no established training programs for humor styles. However, hospitals may be able to affect rates and perceptions of bullying with better selection and training of supervisors to maximize the transformational leadership styles used to interact with staff, and occupational nurses may be uniquely qualified to help implement such initiatives. Bullying, like sexual harassment, will not magically disappear; however, with administrative attention, reporting avenues, and stronger leadership, it may diminish. If staff are not distracted by their own health issues stemming from bullying, they can better serve and care for their own patients.
Applying Research to Practice
Bullying in hospitals can be reduced through effective and encouraging leadership. Administrators need to focus on selecting managers with strong communication skills and leadership potential, then train those supervisors to communicate openly with their teams, facilitate conflict management, and develop cohesive climates that foster support and teamwork. It is not enough to promote technically skilled employees and hope they have the requisite people skills to lead others.
Furthermore, hospitals should have clear anti-bullying policies in place, including clear reporting channels and consequences, and they should begin training all employees to recognize bullying and learn to help targets through effective bystander intervention behaviors. Bullying can only flourish in cultures where it is tolerated.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Carol Bishop Mills is an associate professor and Graduate Coordinator in the Department of Communication Studies at the University of Alabama. Her research focuses on interpersonal and health communication, with a focus on bullying and teasing across the lifespan.
Marieke Keller is a PhD student at The University of Alabama. Her interests lie in organizational communication and intercultural communication.
Alexa Chilcutt is an assistant professor at the University of Alabama where she serves as the Director of Public Speaking at the University of Alabama’s College of College of Communication and Information Sciences. Her research focuses on organizational impression management, leadership and team dynamics.
Mark D. Nelson is Dean of the College of Communication and Information Sciences at The University of Alabama. His research interests are in small group communication and leadership.