
Abstract
Introduction
Nurses are central to healthcare delivery, and their retention is a key factor associated with the quality of nursing care (QONC). Leadership style is considered one of the organizational factors related to nurses’ work outcomes.
Objectives
This study aimed to examine the associations between perceived nurse leaders’ transformational leadership style, nurses’ retention, and perceived QONC, as well as their relationships with selected demographic and professional characteristics among registered nurses working in selected hospitals in Jordan.
Methods
A cross-sectional design was used in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (2014) guidelines. Data were collected using the Global Transformational Leadership Scale, the Revised Casey–Fink Nurse Retention Survey, and the QONC questionnaire.
Results
Nurses reported moderate perceived levels of transformational leadership (Mean = 3.26 ± 0.054). The perceived level of nurse retention was satisfactory (Mean = 2.90 ± 0.026), while the perceived QONV ranged from moderate (Mean = 2.10 ± 0.044) to high (Mean = 1.48 ± 0.035). A strong, positive, and statistically significant association was found between perceived transformational leadership and nurses’ retention (r = 0.527, p < 0.01). Nurses with 16 years or more of experience in their current department reported significantly higher perceptions of transformational leadership than those with fewer years of experience (F = 2.46, df = 4, p = 0.045).
Conclusion
The findings demonstrate significant associations between perceived transformational leadership, nurse retention, and perceived QONC. These results suggest that transformational leadership is an important organizational factor related to nurses’ work perceptions and outcomes. Healthcare administrators and policymakers may consider emphasizing transformational leadership principles within leadership development and professional training programs and fostering supportive work environments aligned with these principles.
Introduction
In healthcare settings, directors, leaders, and executives can adopt various leadership styles, such as transformational leadership, to shape employees’ behaviors and attitudes, ultimately influencing nurse retention and the quality of nursing care (QONC) (Howard et al., 2023). This leadership approach is therefore essential in healthcare organizations, as it helps cultivate a positive work environment, strengthens nurse retention, and contributes to improved patient outcomes (Bonsu & Twum-Danso, 2018).
Transformational leadership is defined by its ability to inspire and motivate followers to exceed expectations through fostering creativity, collaboration, and personal growth (Hani et al., 2022). Effective leaders align their behaviors, beliefs, and values with organizational culture and norms, which can support or limit certain leadership approaches (Jamal, 2024). In nursing, transformational leadership is crucial for retention and care quality, as it cultivates an empowering environment that promotes professional development and collaboration (Collins et al., 2020). By providing a clear vision, recognizing contributions, and encouraging innovation, transformational leaders enhance job satisfaction and organizational commitment (Ferreira et al., 2020). This style also facilitates open communication and shared decision-making, strengthening teamwork, patient care standards, and safety, while reducing turnover intentions and improving overall nursing service quality (Labrague, 2024).
Transformational leadership centers on engaging with followers to elevate their motivation and morale (Al-Faouri et al., 2021) and is defined by four core components: individualized consideration, intellectual stimulation, inspirational motivation, and idealized influence (Park et al., 2019). In nursing, this leadership style inspires team members to uphold high moral and professional standards, strengthens commitment to organizational goals such as high-quality care, and fosters improved patient outcomes, including higher patient satisfaction (Ferreira et al., 2020). Transformational leaders build trust, anticipate staff needs, and provide essential support and resources, thereby enhancing nurse retention and improving the QONC (Hani et al., 2022).
Nurses’ retention refers to an organization's ability to maintain a stable nursing workforce through strategies that reduce turnover, promote job satisfaction, and support long-term commitment (De Vries et al., 2023). The QONC encompasses patient safety, effectiveness, responsiveness, satisfaction, and the overall care experience, measured through outcomes, adherence to best practices, and the ability to meet patients’ holistic needs (Salahat & Al-Hamdan, 2022). Although nurses play a vital role in healthcare, turnover continues to rise, influenced by factors such as leadership, work conditions, and opportunities for professional growth (Hani et al., 2022). Turnover patterns vary by setting, with rural nurses demonstrating higher turnover intentions compared to their urban counterparts (Sellers et al., 2019). The global nursing shortage leads to high turnover rates, with 12% to 64% of nurses planning to leave their jobs within the next year (Ulupınar & Erden, 2024). Turkey has the highest rate, ranging from 60.97% to 64.4%, while Italy (11.7%), Germany (14.0%), and Switzerland have the lowest (16.7%) (De Vries et al., 2023). Jordanian hospitals have a 36% total nurse turnover rate (Al-Faouri et al., 2021). As a result, inadequate nurse staffing leads to higher fatalities, readmissions, and lower quality of care (Park et al., 2019). With one-third of the current nursing workforce expected to retire within the next 10–15 years, a shortage of experienced nurses is anticipated, which may compromise patient care quality as less experienced graduates enter the profession (de Vries et al., 2024).
Review of Literature
Jordan's healthcare system is primarily public and private. The Ministry of Health (MOH) oversees 1,245 centers and 27 hospitals, which account for 37% of all beds. The military's Royal Medical Services operates 15 hospitals, contributing 24% of all beds, while the private sector provides 36%, distributed among 56 hospitals (MOH, 2023). Jordan's healthcare system, although relatively young, is recognized for delivering high-quality services. Over the years, numerous initiatives have been implemented to enhance patient care and improve healthcare outcomes. However, a significant research gap remains regarding the interrelationships between nurse leaders’ transformational leadership style, nurses’ retention, and QONC, particularly within the Jordanian context. While previous studies, such as Alloubani et al. (2019), found that private healthcare facilities provide superior QONC compared to public hospitals, limited research has examined how leadership styles influence nurse retention and QONC across different hospital sectors. Addressing this gap, the current study investigates the correlations among these variables, explores their relationships with nurses’ demographic and professional characteristics, and assesses differences based on these characteristics as perceived by registered nurses (RNs) working in selected hospitals in Jordan.
A Jordanian study found that non-transformational nursing leaders’ autocratic leadership may negatively impact QONC and increase nursing turnover, with 23% of nurses planning to leave within 12 months (Salahat & Al-Hamdan, 2022). To prevent staff loss, Jordan leaders and policymakers must implement retention initiatives and improve working conditions and nursing care quality.
Many international studies addressed transformational leadership and nurses’ retention (AbdELhay et al., 2025; Labrague, 2024), and transformational leadership and the QONC (Tsapnidou et al., 2024), but not the three variables together, which were measured in the current study. Transformational leadership is essential for efficient care delivery, especially in addressing nursing shortages and high turnover rates. Hence, this study examines transformational leadership style, nurses’ retention, and nursing care quality in Jordanian hospitals. Transformational leadership in healthcare promotes efficiency, reduces staff turnover, and cultivates a culture of recognition. Encouraging teamwork, creativity, and continuous professional development enhances patient care quality, improves patient experiences, and increases job satisfaction among healthcare staff (Tsapnidou et al., 2024).
The conceptual model used in this study is grounded in transformational leadership theory (Fischer, 2016), nursing retention theory (Cowden & Cummings, 2012), and the Donabedian structure-process-outcome framework (Tossaint-Schoenmakers et al., 2021). The study highlights that nurse leaders’ transformational leadership style positively influences nurse retention, which in turn enhances the QONC. Transformational leadership motivates and empowers nurses, improving job satisfaction, commitment, and a sense of belonging, which reduces turnover. Sample characteristics—such as age, experience, hospital type, and education—moderate nurses’ perceptions of leadership and retention. The model emphasizes the interconnectedness of leadership, retention, and care quality, showing that transformational leadership fosters cultural congruence, professional dedication, and a supportive work environment, thereby stabilizing teams, improving continuity of care, and enhancing clinical experience. By inspiring patient-centered care, transformational leadership can also directly impact QONC. Jordanian cultural values, including family orientation, collectivism, and respect for hierarchy, further strengthen the relationship between transformational leadership, nurse retention, and care quality, Figure 1.

The roles transformational leadership in nurses’ retention and the quality of nursing care.
Methods
Design
This quantitative study employed a descriptive, cross-sectional, correlational design. Through this design, data are gathered at one time from a wide range of participants (Flanagan & Beck, 2024). When using this design, variables are observed without being influenced. Gathering preliminary data can be done quickly and affordably. Also, this design was chosen for its relatively short-duration outcomes. However, this design is beneficial in addressing various types of study inquiries (Flanagan & Beck, 2024).
Research Questions
This study aims to answer the following research questions: 1) What are the levels of perceived nurse leaders’ transformational leadership style, nurses’ retention, and QONC as reported by RNs working in the selected Jordanian hospitals? 2) Is there a relationship between RNs’ perceptions of nurse leaders’ transformational leadership style, nurses’ retention, QONC, and the nurses’ demographic and professional characteristics in the selected Jordanian hospitals at the time of data collection? 3) Are there differences in RNs’ perceptions of nurse leaders’ transformational leadership style, nurses’ retention, and QONC based on their demographic and professional characteristics in the selected Jordanian hospitals?
Sample
The current study focused on Jordanian RNs working in selected hospitals, with a target population of RNs working in the selected hospitals who have direct communication and interaction with their nursing managers and can assess their leadership style. The accessible population in this study consisted of RNs working in the targeted hospitals who had direct interaction and communication with their nursing managers and were therefore able to evaluate their leadership style. These nurses were selected because their close professional relationship with their managers enabled them to provide accurate perceptions of transformational leadership practices. Data was collected from six large Jordanian hospitals, including two governmental hospitals, one military hospital, and three private hospitals. These hospitals were chosen for data collection due to their significant patient volume, accreditation status, comprehensive specialty coverage, bed capacity (over 150 beds), and high occupancy rates.
Inclusion/Exclusion Criteria
Nurses were selected using a convenience sampling technique. The inclusion criteria required participants who (1) hold at least a Bachelor of Science in Nursing (BSN) degree and (2) have at least 1 year of work experience in their current department. The exclusion criteria applied to individuals in administrative roles or other healthcare positions that did not involve direct patient care, as these roles were not relevant to assessing perceptions of transformational leadership and QONC. The sample size estimation was 175, as calculated using G*power software version 3.1.9.7. (Faul et al., 2009), based on a one-way analysis of variance (ANOVA) test with a medium effect size (25%), significance level (alpha = 0.05), and power of 80% on a confidence interval of 95%. However, a large sample size was collected to compensate for the electronic surveys’ expected low response rate and a convenience sample to enhance generalizability. The number of participants reached 322. The use of convenience sampling and online surveys via WhatsApp may bias the sample's representativeness. This methodology could lead to overrepresentation of technologically literate participants, while excluding those with limited internet access or less engagement in professional networks.
Instruments
A structured information sheet was designed to gather nurses’ sociodemographic data, including sex, age, educational background, total years of nursing experience, years of experience in the current department, hospital type, practice setting, and shift work schedule. Additional instruments used in the study are detailed below.
To evaluate the perceived level of transformational leadership among nurse leaders, the mean score was calculated. A tripartite classification approach was applied, using the formula: (highest score − lowest score) / number of categories = (5 − 1) / 3 = 1.33. Based on this, mean scores were interpreted as follows:
Section I includes 32 items measured on a 4-point Likert scale, where respondents indicate their level of agreement as follows: 1 = strongly disagree, 2 = disagree, 3 = agree, and 4 = strongly agree. These items are organized into four subscales related to the work environment:
Practitioners and nurse managers revised the Revised Casey-Fink Nurse Retention Survey after a pilot test with 60 oncology nurses (Buffington et al., 2012). The revised scale showed a Cronbach's alpha of 0.92, with reliability values for four subscales ranging from 0.76 to 0.93 (Buffington et al., 2012). Higher scores indicated satisfactory nurses’ retention, with a Cronbach's alpha of 0.95 in the current study.
Data Collection Procedures
This research was consistent with the Strengthening the Reporting of Observational Studies in Epidemiology (2014) guidelines. The study obtained approval from the university where the first author was studying and other relevant authorities before collecting data. The English version of the scales was used due to Jordan's official teaching language. The researcher visited targeted institutions, met nursing managers, and distributed the online survey link via the WhatsApp group to ensure the target sample could access the survey link. Data collection was started in May 2024 and ended in August 2024. Before analysis, the dataset was carefully checked for missing values. Cases with substantial missing responses were excluded, while minimal missing data were managed using appropriate statistical techniques, such as mean substitution, to maintain the integrity of the analysis.
The Pilot Study
A pilot study was conducted with 35 nurses to evaluate the questionnaire's clarity, suitability, and reliability for Jordanian healthcare settings. Internal consistency was confirmed using Cronbach's alpha, demonstrating that all three scales were reliable, and participants reported the questionnaire as easy to use, taking 15–20 min to complete. The survey was administered online via Google Forms distributed through WhatsApp groups, ensuring accessibility, voluntary participation, and anonymity. Measures such as cookie-based access, a unique QR code, and a customized Google Form were implemented to maintain confidentiality. The researcher coordinated with nursing managers and head nurses to explain the study and share survey access, while reminders were sent without exerting pressure to participate. The online format allowed participants to pause and resume the survey as needed. Data collection spanned approximately 3 months, during which the researcher monitored response rates and provided incentives for participation, ensuring that all responses remained confidential and devoid of personal identifiers.
Ethical Considerations
Ethical approval was obtained from the IRBs or ethics committees of the participating hospitals. The study protocol, including objectives, methodology, and consent procedures, was reviewed and approved prior to data collection. Nurses participated voluntarily, and consent was implied through completion of the online questionnaire. Data were anonymized, coded, stored in SPSS, and kept confidential on a password-protected Google Drive accessible only to the principal researcher.
Statistical Analysis
At a significance level of 0.05, the study used SPSS version 25 (IBM, 2019) to analyze data, check for accuracy, and align it with research questions. Descriptive and inferential statistics were used to report means, standard errors, frequencies, and percentages. Pearson and Spearman's rho correlations were used to answer questions, with Cohen's guidelines evaluating the strength of correlations (Faul et al., 2009). The study used inferential statistics of ANOVA or t-test to measure differences between groups based on overall mean scores and individual items (Faul et al., 2009).
Descriptive statistics, including means, standard errors, frequencies, and percentages, were calculated for all variables according to their measurement level. Pearson and Spearman's rho correlations were used to address research question two, based on overall mean scores to reduce type II errors. Correlation coefficients were interpreted in terms of significance, direction, and magnitude, with Cohen’s guidelines classifying correlations as weak (r < 0.30), moderate (r = 0.30–0.50), or strong (r > 0.50). Finally, to answer the third research question, inferential statistics of one-way ANOVA or t-test were used to measure the differences between groups based on the overall mean scores and individual items of the studied concepts. Inferential statistics of t-tests were used to compare the means of the two groups, the mean of a dependent continuous variable with two categorical independent variables (Polit & Beck, 2020). ANOVA was used to compare the mean of a dependent continuous variable with more than two categorical independent variables or groups (Faul et al., 2009). The reliability was reported for all instruments used in the current study.
Results
Sample Characteristics
The study recruited (n = 322) RNs, where most of them were females (n = 242, 75.20%). The highest age group was 30–39 years old (n = 191, 59.30%), while the lowest was 50 or more (n = 8, 2.50%). Most participants held bachelor's degrees in nursing (251, 78.00%), while 71 (22.00%) held a higher degree of education, such as a master's or PhD degree in nursing. About 26.70% of the participants have 6–10 years of experience in nursing (n = 86), while 5.00% had 1 year (n = 16), 16.80% of nurses had 2–5 years of experience in the current department (n = 54), while 10.60% had 1 year (n = 34). The participants were recruited from three types of hospitals: governmental hospitals (30.4%), military hospitals (39.2%), and private hospitals (30.4%). This distribution indicates a balanced representation across different healthcare sectors, with the highest proportion of participants working in military hospitals (Table 1).
Sample Characteristics (N = 322).

The Levels of Perceived Nurse Leaders’ Transformational Leadership Style, Nurses' Retention, and Quality of Nursing Care as Perceived by Registered Nurses Working in the Selected Jordanian Hospitals
The perceived nurse leaders’ transformational leadership style was rated at a moderate level, with an overall mean score of 3.26 (SE = 0.054). Item means ranged narrowly from 3.19 to 3.32, and the median response for all items was “three,” indicating that nurses most often selected “occasionally” or “sometimes.” The highest-rated behaviors were communicating a clear and positive vision of the future and treating and supporting staff as individuals. The lowest-rated behavior was encouraging new ways of thinking and questioning assumptions (Table 2).
The Levels of the Perceived Nurse Leaders’ Transformational Leadership Style (N = 322).

SE, standard error; CI 95.0%, confidence interval 95%.
The overall mean score of the perceived nurses’ retention was 2.90 (SE = 0.026), indicating a satisfactory nurses’ retention level. According to the nurses’ retention subscale, the highest mean score was for the schedule flexibility subscale (Mean = 2.95, SE = 0.037), which indicated higher satisfactory nurses’ retention, followed by the subscales of mentorship (Mean = 2.92, SE = 0.028) and recognition reward (Mean = 2.90, SE = 0.031). On the other hand, the lowest mean score was for the subscale of professional nursing roles (Mean = 2.84, SE = 0.023), indicating an unsatisfactory level of the perceived nurses’ retention, with the median equal to three for all items of the perceived nurses’ retention subscales (Table 3).
The Levels of the Perceived Overall Nurses’ Retention (N = 322).

SE, standard error; CI 95.0%, confidence interval 95%.
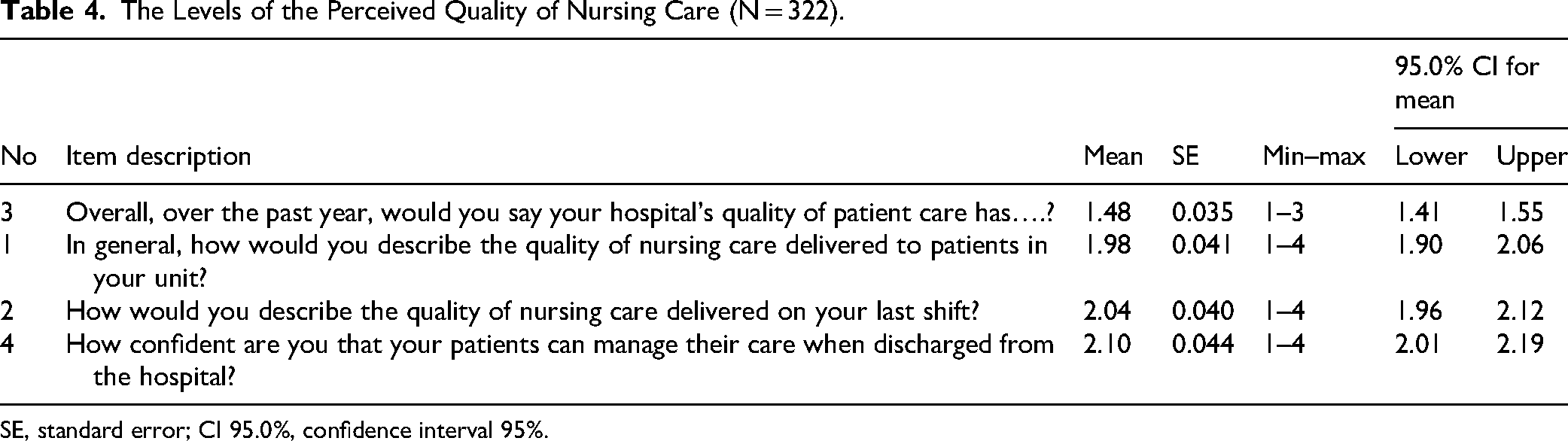
Healthy workplaces, effective leadership styles, quality improvement initiatives, and clearly defined organizational policies contribute to a satisfactory nursing experience. The QONC scale items demonstrated mean scores ranging from 1.48 to 2.10, reflecting moderate to high levels of perceived quality of care. The lowest mean score was observed for the third item, “Overall, over the past year, would you say the quality of patient care in your hospital has…?” (Mean = 1.48, SE = 0.035). This was followed by the first item, “In general, how would you describe the QONC delivery to the patients in your unit?” (Mean = 1.98, SE = 0.041). The highest mean score was recorded for the fourth item, “How confident are you that your patients can manage their care when discharged from the hospital?” (Mean = 2.10, SE = 0.044) (Table 4).
The Levels of the Perceived Quality of Nursing Care (N = 322).
SE, standard error; CI 95.0%, confidence interval 95%.
The Relationships Between the Perceived Nurse Leaders’ Transformational Leadership Style and Nurses’ Retention and the Quality of Nursing Care
As shown in Table 5, there was a statistically significant, strong positive correlation between the overall score of the perceived nurse leaders’ transformational leadership style and the overall score of the perceived nurses’ retention in the selected Jordanian hospitals (r = 0.527, p < 0.01). In terms of the correlations between the overall score of the perceived nurse leaders’ transformational leadership style and nurses’ retention subscales, there was a statistically significant strong positive correlation with the recognition-rewards subscale (r = 0.550, p < 0.01), a statistically significant moderate positive correlation with the professional nursing roles subscale (r = 0.402, p < 0.01), a statistically significant strong positive correlation score the mentorship subscale (r = 0.514, p < 0.01), and a statistically significant weak positive relationship with the scheduling flexibility subscale (r = 0.264, p < 0.01).
The Relationships Between the Perceived Nurse Leaders’ Transformational Leadership Style and Nurses’ Retention (N = 322).

Correlation is significant at the 0.01 level (two-tailed). r = Pearson correlation.
Spearman's correlation analysis showed that perceived nurse leaders’ transformational leadership style was positively and significantly associated with all indicators of the QONC. Weak but significant correlations were found with overall unit-level care quality and quality delivered during the last shift (r = 0.245 and r = 0.190, respectively; p < 0.01). Moderate positive correlations were observed for the perceived quality of patient care over the past year (r = 0.438, p < 0.01) and for nurses’ confidence in patients’ ability to manage their care after discharge (r = 0.408, p < 0.01).
The Relationships Between the Perceived Nurse Leaders’ Transformational Leadership Style, Nursing Retention, the Quality of Nursing Care, and the Sample Characteristics
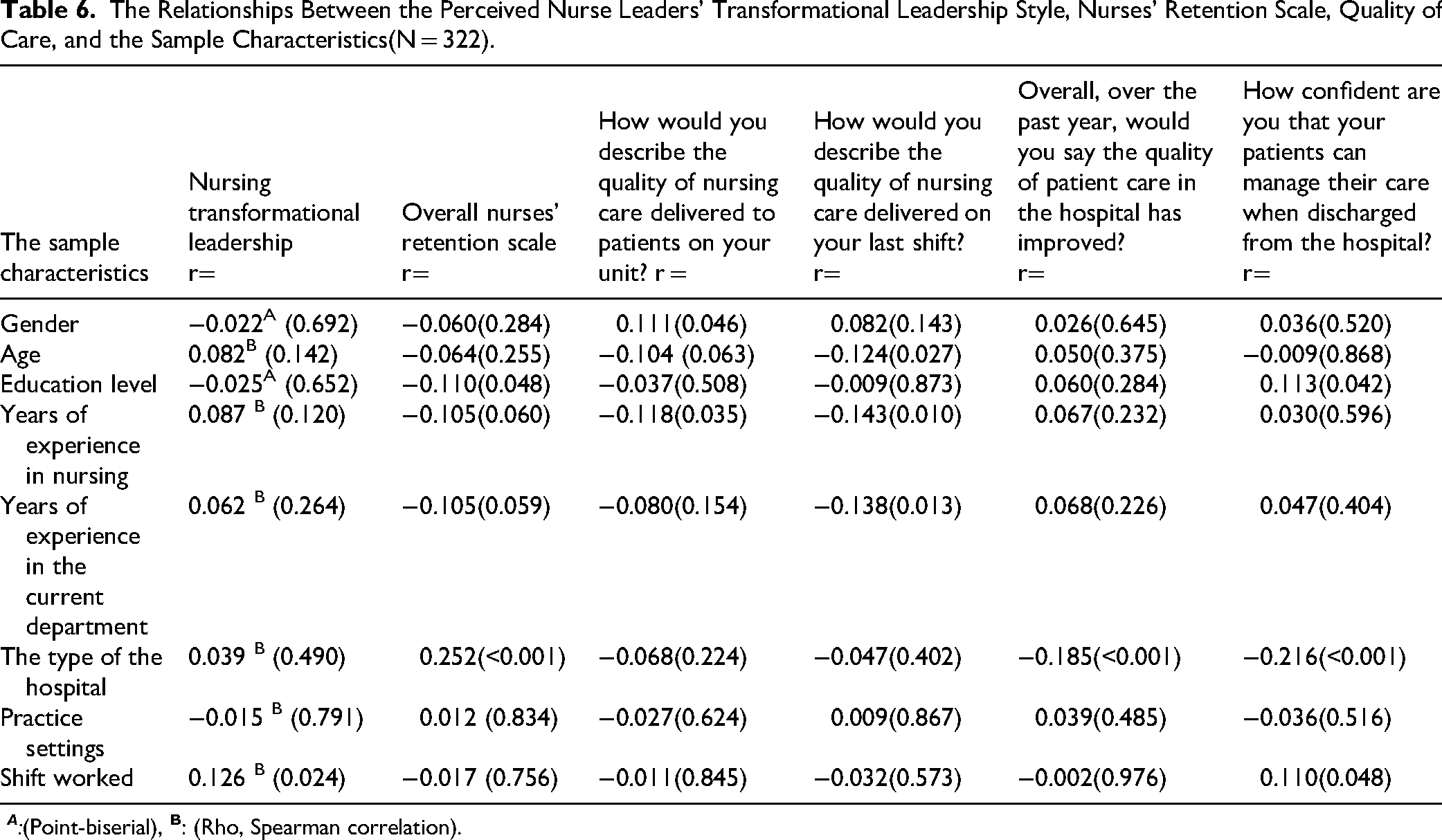
The correlation coefficient showed a statistically significant weak positive relationship between the level of perceived nurse leaders’ transformational leadership style and the shift worked (r = 0.126, p = 0.024). For nursing retention, there was a statistically significant weak negative correlation between the overall perceived nurses’ retention and educational level (r = −0.110, p = 0.048) and a statistically significant weak positive correlation with the type of hospital (r = 0.252, p < 0.001). For the QONC, the correlation coefficients indicated significant relationships between the sample characteristics and the first item of the perceived QONC, “In general, how would you describe the QONC delivered to patients on your unit?” indicated a statistically significant weak positive relationship with gender (r = 0.111, p = 0.046), a statistically significant weak negative relationship with years of experience in nursing (r = −0.118, p = 0.035). The correlation coefficients indicated significant relationships between the sample characteristics and the second item of the perceived QONC, “How would you describe the QONC delivered on your last shift?” yielded a statistically significant weak negative relationship with age in years (r = −0.124, p = 0.027), a statistically significant weak positive relationship with years of experience in nursing (r = −0.143, p = 0.010), and a statistically significant weak negative significant relationship with years of experience in the current department (r = −0.138, p = 0.013) (Table 6).
The Relationships Between the Perceived Nurse Leaders’ Transformational Leadership Style, Nurses’ Retention Scale, Quality of Care, and the Sample Characteristics(N = 322).
The Differences in the Perceived Nurse Leaders’ Transformational Leadership Style, Nurses’ Retention, and the Quality of Nursing Care Based on the Sample Characteristics
The one-way ANOVA was used to test whether significant differences existed in the perceived nurse leaders’ transformational leadership style based on the sample characteristics. There was a significant difference in the levels of the perceived nurse leaders’ transformational leadership style based on years of experience in the current department (F = 2.46, DF = 4, p = 0.045). Scheffe's post hoc test revealed that nurses with 16 years or more of experience in their current department (Mean = 25.73, SD = 7.11) reported significantly higher perceptions of their nurse leaders’ transformational leadership style compared to nurses with 1 year (Mean = 21.15, SD = 5.72), 6–10 years (Mean = 22.21, SD = 6.23), or 11–15 years (Mean = 21.67, SD = 7.09) of experience. The independent t-test was used to determine the significant differences that existed in the perceived nurse leaders’ transformational leadership style based on nurses’ sex and level of education; no differences were found (Table 7).
The Differences in the Perceived Nurse Leaders’ Transformational Leadership Style Based on the Sample Characteristics(N = 322).
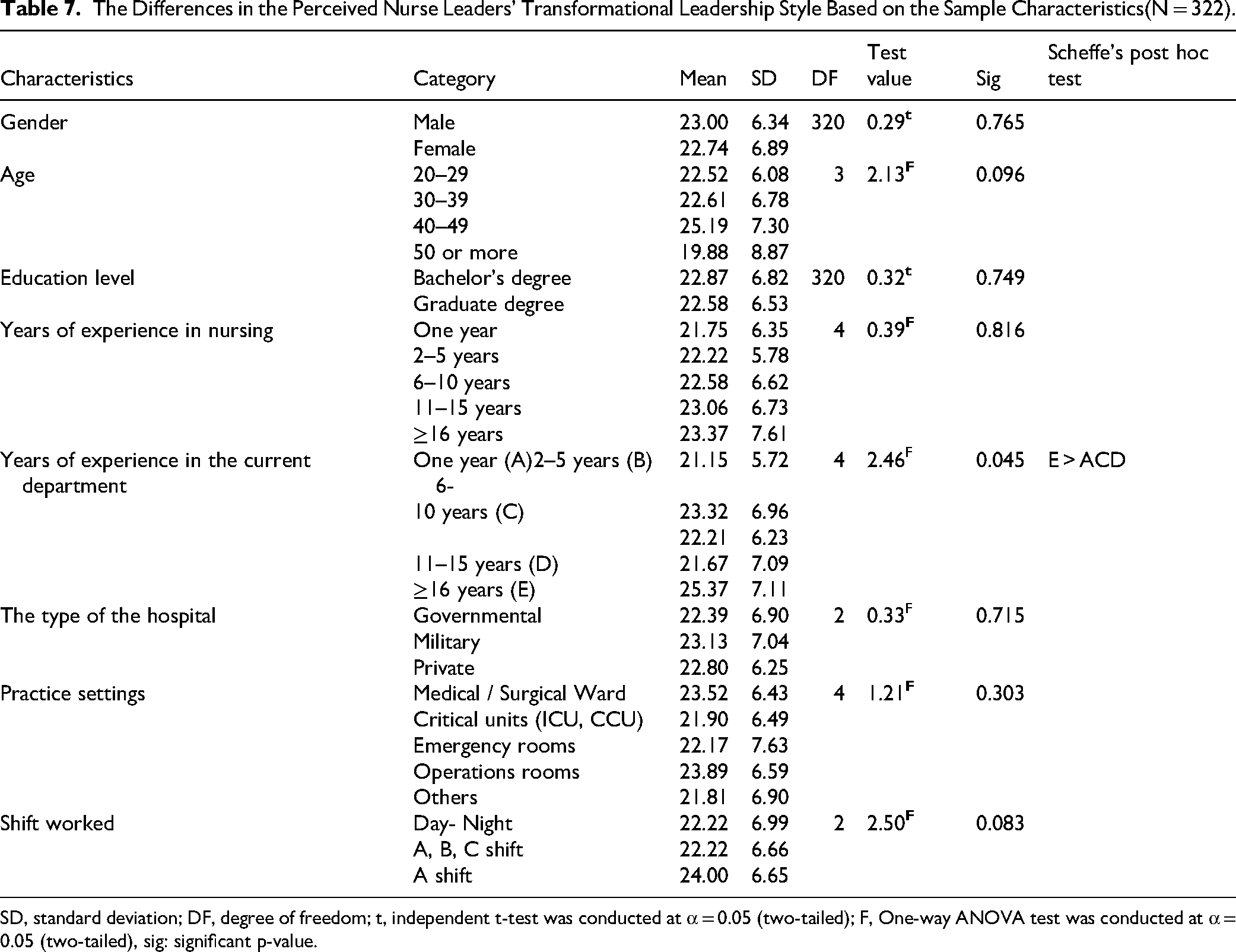
SD, standard deviation; DF, degree of freedom; t, independent t-test was conducted at α = 0.05 (two-tailed); F, One-way ANOVA test was conducted at α = 0.05 (two-tailed), sig: significant p-value.
The one-way ANOVA was used to test whether significant differences existed in the overall level of perceived nurses’ retention based on the sample characteristics. There were significant differences in the overall levels of perceived nurses’ retention based on the type of hospital (F = 9.34, DF = 2, p < 0.001; all the following statistics are not reported in the tables). Scheffe's post hoc test demonstrated that nurses in private hospitals (Mean = 97.45, SD = 11.70) had significant transformational leadership and higher levels of perceived nurse retention than nurses in governmental hospitals (Mean = 88.66, SD = 17.01) and military ones (Mean = 91.71, SD = 14.29). The study employed the independent t-test to identify whether there were significant differences in the overall perceived nurses’ retention based on the sample characteristics of sex and level of education; no significant differences were found.
For the QONC, no significant difference in the perceived levels in the first item, “In general, how would you describe the QONC delivered to patients on your unit?” with the sample characteristics. The independent t-test was used to determine whether significant differences existed in the level of the 1st item of the perceived QONC based on nurses’ gender or education level. There were significant differences in the level of the first item of the perceived QONC based on sex (t = 2.00, DF = 320, p = 0.046). Female nurses (Mean = 2.03, SD = 0.76) reported significantly lower levels of QONC compared to male nurses (Mean = 1.84, SD = 0.67). Nevertheless, it is important to restate that a low score for QONC indicates a high level of quality.
A significant difference in the level of the second item of the perceived QONC, “How would you describe the QONC delivered on your last shift” (F = 2.89, df = 4, p = 0.022). Scheffe's post hoc test demonstrated that nurses who had 1 year of experience in nursing in the current department (Mean = 2.41, SD = 0.66) had significant transformational leadership lower levels of QONC than nurses who had been in 2–5 years (Mean = 2.04, SD = 0.73), 6–10 years (Mean = 1.98, SD = 0.74), (11–15) years (Mean = 2.00, SD = 0.65), and more than or equal 16 years of experience in in the current department (Mean = 1.89, SD = 0.72); however, a low mean score of QONC indicates a high level of quality.
There was a significant difference in the level of the third item of the perceived QONC, “Overall, over the past year, would you say the quality of patient care in your hospital has….?” based on the type of hospital (F = 7.54, df = 2, p < 0.001). Scheffe's post hoc test showed that nurses working in private hospitals had the lowest mean score (M = 1.28, SD = 0.51), indicating that they reported significantly higher levels of QONC on this item compared to nurses working in military hospitals (M = 1.57, SD = 0.67) and governmental hospitals (M = 1.56, SD = 0.64).
There was a statistically significant difference in the level of the fourth item of the perceived QONC, “How confident are you that your patients can manage their care when discharged from the hospital?” was based on the type of hospital (F = 7.25, df = 2, p = 0.001). While the low score on the QONC indicates a high level of QONC, Scheffe's post hoc test revealed a mean score of 2.33(SD = 0.74) in governmental hospitals, indicating that nurses had significantly transformational leadership lower levels of QONC than those in military hospitals (M = 2.07, SD = 0.82) and the private ones (M = 1.91, SD = 0.75).
On the other hand, there were statistically significant differences in the level of the fourth item of the perceived QONC based on the shift worked (F = 4.97, df = 2, p = 0.007). Scheffe's post hoc test demonstrated that nurses who worked on the day-night shift had significant transformational leadership with higher levels of the QONC (M = 1.82, SD = 0.72) than nurses who worked on the A, B, and C shifts (M = 2.19, SD = 0.82), and the A shift (M = 2.13, SD = 0.76). To determine if there were any significant differences in the level of the fourth item of the perceived QONC based on nurses’ sex and the level of education, a t-test was employed; no significant differences were found.
Discussion
This study examined the relationships between perceived nurse leaders’ transformational leadership style, nurse retention, and the QONC, while also exploring how these factors vary according to sample characteristics among RNs in selected Jordanian hospitals. The sample was predominantly young female nurses, reflecting the gender distribution of the nursing workforce in Jordan, where females constitute the majority. This demographic pattern aligns with previous studies in Jordan and Pakistan, which similarly reported higher female representation in nursing (Kalaani et al., 2020; Suliman et al., 2024).
This study reinforces international evidence that transformational leadership plays a critical role in enhancing nurse retention and the QONC. Consistent with studies from Canada, Australia, and Saudi Arabia, transformational leaders are perceived to create supportive environments that foster professional growth, empowerment, and commitment among nurses (Baškarada et al., 2017; Caro, 2016; Saad Alessa, 2021), suggesting that the benefits of this leadership style transcend cultural and organizational contexts. In this study, nurses perceived their leaders as exhibiting a moderate level of transformational leadership, aligning with findings by Wang et al. (2018) and Abdul Salam et al. (2023), though contrasting with Al-Thawabiya et al. (2023), who reported higher perceived transformational leadership, particularly among directors rather than head nurses. The moderate perception observed here indicates that transformational behaviors are present but not consistently experienced, potentially limiting nurses’ motivation, engagement, and professional development—key factors for retention and high-quality care.
Regarding nurse retention in Jordanian hospitals, the study found overall satisfactory levels, with the highest retention in schedule flexibility and mentorship/recognition reward subscales, while retention related to professional nursing roles was unsatisfactory. These findings mirror Wang et al. (2018), who reported low turnover rates among Chinese nurses. Nurses expressed satisfaction with recognition for team efforts but noted gaps in support and mentorship from unit managers and educators, highlighting areas for improvement in Jordanian hospitals. The study identified four key factors impacting retention: mentorship, recognition and reward, clearly defined professional roles, and flexible scheduling, with scheduling flexibility emerging as the most influential. This suggests that daily flexibility and individualized support can have a significant effect on retention, even as systemic supports and strategic leadership remain essential for long-term workforce stability and high-quality patient care.Watts-Isley et al. (2024) study in the US found that nearly half of public health nurses reported dissatisfaction and retention issues in their local health departments. In Jordan, healthy workplaces, leadership styles, quality improvement projects, and organizational policies contribute to satisfactory nurse retention. Strategic planning, including opportunities for professional growth, fair pay, and a friendly work environment, can effectively retain nursing staff despite the global challenge of retaining qualified, experienced nurses.
The perceived QONC in Jordanian hospitals is moderate to high, consistent with previous studies performed by Ma et al. (2015). In the US, 58% of participants reported excellent care, while 40% reported improved care. In Turkey, 63.90% rated the quality as excellent, and 87.9% would recommend the hospital (Karaca & Durna, 2019). In Portugal, the overall mean value is good, contributing to managerial performance and leadership (Lucas et al., 2023).
The study identified significant positive correlations between transformational leadership and nurse retention, suggesting that this leadership style enhances productivity, job satisfaction, and organizational commitment, consistent with findings by Goens and Giannotti (2024) and Wang et al. (2018). While transformational leadership positively influences retention and career satisfaction, the study noted that other leadership styles may also play a role. Transformational leadership is thus a practical strategy for improving nursing care quality, particularly in managerial roles that require leadership training to sustain a positive organizational culture (AbdELhay et al., 2025).
Additionally, weak positive correlations were observed between perceived transformational leadership and the QONC, aligning with Labrague (2024), who reported links to fewer adverse patient events and better care quality. However, findings contrast with Lavoie-Tremblay, Fernet, Lavigne and Austin (2016), who reported stronger associations between transformational leadership, higher QONC, and lower nurse turnover.
This study found a weak positive relationship between nurses’ retention and overall QONC in selected Jordanian hospitals, with moderate positive relationships observed for nurses’ perceptions of care quality over the past year and their confidence in patients’ ability to manage care after discharge. High nurse turnover remains a critical issue, contributing to job dissatisfaction and workload challenges, underscoring the importance of retention for maintaining high-quality care, consistent with Kelly and Hearld (2020) and Al Zamel et al. (2020).
A weak correlation was observed between transformational leadership and shift work, suggesting that transformational leaders can promote favorable workplace conditions that enhance safety and job satisfaction, contrasting with ALFadhalah and Elamir (2021). Retention showed a weak negative correlation with educational level and a weak positive correlation with hospital type, aligning with Al-Hamdan et al. (2017), which potentially reflects hospital-specific policies. Other factors, such as age, years of experience, and shift worked, showed weak correlations with perceived QONC and confidence in patient self-care, consistent with findings by Ma et al. (2015) and Buffington et al. (2012), which emphasize the role of experience in care quality.
The study also highlighted gender disparities, with female nurses exhibiting significant transformational leadership but lower perceived care quality, likely influenced by societal and cultural expectations that increase stress and burnout, echoing findings from Indonesia (Mamo & Shaker, 2024). Additionally, less experienced nurses reported lower perceived care quality due to reduced confidence and a need for support. These findings emphasize the importance of structured orientation, mentorship, and supportive leadership to enhance nurse retention, professional development, and overall QONC.
Strengths and Limitations
This study investigates the relationship between nurses’ perceptions of transformational leadership, retention rates, and QONC in Jordanian hospitals. It is the first of its kind in Jordan, providing insights based on reported experiences. While reflecting perceptions rather than objective realities, the findings suggest practical implications for enhancing leadership and nurse retention. Limitations include a cross-sectional design that restricts causal inferences and potential sampling biases from convenience methods and WhatsApp distribution, which may affect the diversity and generalizability of the results.
Implications for Practice
Nurses need education on leadership styles, particularly transformational leadership, to lead effectively. Healthcare institutions should support mentorship for nurses in leadership and decision-making. Promoting flexible scheduling and professional development opportunities improves job satisfaction, teamwork, and communication.
Conclusion
The study indicates that nurses’ perceptions of transformational leadership significantly impact retention and QONC in Jordanian hospitals. Experienced nurses view transformational leadership more positively, and private hospitals with higher retention may practice effective leadership. Investing in leadership development for nurse managers is recommended to enhance leadership behaviors, improve nurse satisfaction, reduce turnover, and elevate patient care quality.
Supplemental Material
sj-docx-1-son-10.1177_23779608251413844 - Supplemental material for The Roles of Transformational Leadership in Nurses’ Retention and the Quality of Nursing Care: A Cross-Sectional Study
Supplemental material, sj-docx-1-son-10.1177_23779608251413844 for The Roles of Transformational Leadership in Nurses’ Retention and the Quality of Nursing Care: A Cross-Sectional Study by Kholoud Faraj Alhusban, Majd T Mrayyan and Salam Bani Hani in SAGE Open Nursing
Supplemental Material
sj-pdf-2-son-10.1177_23779608251413844 - Supplemental material for The Roles of Transformational Leadership in Nurses’ Retention and the Quality of Nursing Care: A Cross-Sectional Study
Supplemental material, sj-pdf-2-son-10.1177_23779608251413844 for The Roles of Transformational Leadership in Nurses’ Retention and the Quality of Nursing Care: A Cross-Sectional Study by Kholoud Faraj Alhusban, Majd T Mrayyan and Salam Bani Hani in SAGE Open Nursing
Footnotes
Acknowledgments
The authors would like to thank all the participants for their valuable contributions to the data they provided. All authors have read and approved the final version of the manuscript. All authors had full access to the data in this study and took complete responsibility for the integrity of the data and the accuracy of the data analysis. The supporting source/financial relationships had no such involvement. This work did not receive any specific grant from funding agencies in the public, commercial, or non-profit sectors.
Informed Consent
The invitation letter informed the participants that their participation in the survey constituted their consent to participate in the study.
Ethical Considerations
The study obtained approval from the Hashimite University, where the first author was studying, and other relevant authorities before collecting data. The IRB was obtained from the MOH (Ref.: #8913), the Royal Medical Services (Ref.: #9/2024), and the Private Hospital of (Ref.: # 062400001).
Author Contributions
KFH contributed to conceptualization and methodology; MM contributed to formal analysis, supervision, and editing; SBH contributed to writing the final draft and editing. All authors have read and approved the final version of the manuscript. The corresponding author had full access to all of the data in this study and took complete responsibility for the integrity of the data and the accuracy of the data analysis.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study will be available upon reasonable request.
Reporting Method
The author of this manuscript has adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist was used to guide the study.
Patient and Public Involvement
Patients and/or the public were not involved in the design, conduct, reporting, or dissemination plans of this research. The sample included nurses recruited from different hospitals.
Declaration of Generative AI and AI-Assisted Technologies in the Writing Process
During the preparation of this work, the authors used Grammarly edit language. After using this tool, the authors reviewed and edited the content as needed and took full responsibility for the content of the publication.
Statistics
The authors have checked to make sure that our submission conforms as applicable to the Journal's statistical guidelines described here.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.