
Abstract
In this quantitative, cross-sectional study, the authors identified the impact of workplace bullying on nursing staff employed at select Greek public hospitals. They conducted the study using the Negative Acts Questionnaire with a convenience sample of 841 participants employed by five Greek hospitals in the 1st Regional Health Authority of Attica. One third of the respondents reported having been psychologically harassed at work in the past 6 months. According to the results, the impact workplace bullying has on nursing staff varies depending on the existence of a supportive familial or friend environment and if nurses parent children. These findings demonstrate the value of family and friend support when coping with workplace bullying.
Andrea Adams, a British journalist, coined the term “workplace bullying” in 1992 in a series of BBC radio programs that increased public concern about this issue. In response, young researchers in the United Kingdom began studying this specific type of bullying (Rayner, 1997). However, research on workplace bullying actually began in the 1970s when psychiatrist Carrol Brodsky (1976) conducted a pioneering study recording workers’ complaints of workplace bullying. In the early 1990s, Brodsky’s research attracted interest in the study of human aggression, which included workplace aggression (Spector, Zhou, & Che, 2013). In the early 1980s, Helen Cox, a nursing professor, studied verbal abuse in health care when it was made clear that talented nursing students were choosing to leave nursing and seek other professions in which abuse was not endemic. Homicides in the workplace spawned a multitude of studies over the next two decades (Allen & Lucerno, 1996; Baron & Neuman, 1998; Chen & Spector, 1992; Neuman & Baron, 1997; Piquero, Piquero, Craig, & Clipper, 2013).
Over the years, academic interest in bullying has included studies on injustice, rudeness, and ill-treatment (Andersson & Pearson, 1999; Keashly, 1998). In the late 1990s, research interest shifted to emotional abuse in the workplace, a concept often synonymous with bullying (Keashly, 1998). Around this time, Namie and Namie (2000) published a self-help book on the subject and founded the Workplace Bullying Institute (WBI) to support victims. In the early 2000s, the phenomenon of workplace bullying in the United States received more attention from researchers, demonstrating that bullying is a significant occupational problem (Vessey, Demarco, Gaffney, & Budin, 2009).
Literature Review
The term workplace bullying distinguishes between organizational and individual dynamics (Einarsen et al., 2003; Fox & Cowan, 2015). Workplace bullying is a complex social phenomenon that encompasses both organizational and individual factors (Aquino, 2000), but is difficult to define because of the symbiotic relationship between organizations and individuals (O’ Leary-Kelly, Griffin, & Glew, 1996); both individual and organizational factors influence the occurrence of the phenomenon (Bolman & Deal, 2013). Occupational rivalry and envy regarding other workers’ circumstances are among the most common causes of bullying (Bjorkqvist, Osterman, & Hjelt-Back, 1994; D’Cruz & Noronha, 2014). Both the victim being targeted and the bully demonstrate ineffective communication and conflict-management skills, which would better enable them to address these situations (Zapf & Einarsen, 2003).
Organizational patterns, factors, and motives can incite individuals to bully their colleagues. Eliminating any one of these factors alone will not prevent workplace bullying but in tandem they may impact its occurrence (Lee, Bernstein, Lee, & Nokes, 2014; Salin, 2003). Changes in the work environment (Baron & Neuman, 1998; Hoel & Salin, 2003; Rayner, 1997; Sheehan, 1999), redundancies (Salin, 2003; Vickers, 2001; Zapf, 1999), leadership, or job descriptions (Harvey, Treadway, & Heames, 2007), which can increase workers’ insecurity, loss of control, or perceptions of greater workload (Harvey, Treadway, & Heames, 2006), can affect the occurrence of workplace bullying (Salin, 2003). Last, differences in age, race, gender, nationality, and education can aggravate conflicts and increase intimidating behaviors in the workplace (Skogstad, Matthiesen, & Einarsen, 2007). Changes within the organization, particularly in work duties and the composition of the workforce, are prognosticators of workplace bullying (Baron & Neuman, 1998; Olson, Nelson, & Parayitam, 2006; Salin, 2003; Skogstad et al., 2007).
Spector et al.’s (2013) review article reported on the form and source of bullying phenomena among nursing staff; the authors suggested that of 151,347 nurses, 36.4% had been physically assaulted, 66.9% had been otherwise assaulted, 39.7% had been victims of bullying, 25% had been sexually harassed, and 32.7% reported injuries from aggravated assaults. The rates of exposure varied depending on geographic location, with the highest rates of physical abuse and sexual harassment reported in English-speaking countries, and the highest rates of non-physical violence and bullying reported in the Middle East. These findings demonstrate that the incidence of workplace bullying constitutes a serious psychosocial phenomenon with negative impact on both victims and organizations (Vartia & Leka, 2011).
Method
This quantitative cross-sectional study identified the impact of workplace bullying on nursing staff of Greek public hospitals using four axes: (a) psychological harassment, (b) personal bullying, (c) work-related bullying, and (d) physical bullying. The surveyed population was a convenience sample of 841 members of the nursing staff of five Greek National Health Service Hospitals in the 1st Regional Health Authority of Attica. The appropriate permissions were obtained from the University Institutional Review Board and each hospital’s Ethical Research Committee.
The Negative Acts Questionnaire (NAQ; Einarsen & Hoel, 2001) was used for this study after receiving appropriate permission from its authors. The NAQ consists of 23 items, which compose three sub-scales: (a) Personal Bullying: Items 2, 4 to 7, 10 to 13, 15, 17, and 20, with a total score of 12 to 60; (b) Work-Related Bullying: Items 1, 3, 14, 16, 18, 19, and 21, with a total score of 7 to 35; and (c) Physical Bullying: Items 8, 9, and 22, with a total score of 3 to 15. Questionnaire responses were Likert-type on a 5-point scale, with specific temporal anchors (e.g., daily, weekly) to measure the incidence of bullying behaviors; higher scores represent more negative behavior. The 23rd item on the questionnaire (“Have you been bullied at work in the past 6 months?”), which is not included in any of the three sub-scales, measures psychological harassment and has the following possible responses: (a) no; (b) yes, but only rarely; (c) yes, at times; (d) yes, a few times a week; and (e) yes, almost daily.
The NAQ was translated into Greek using the double backward technique. After translation, a pilot study with a sample of 50 nurses and nurse assistants was conducted to establish the questionnaire’s reliability and face validity. Cronbach’s alpha for the pilot study data was .81, suggesting adequate internal consistency. To determine face validity, interviews of pilot study participants were conducted and appropriate instrument revisions, minor wording, and syntactic modifications in the Greek version of the questionnaire, were made.
The NAQ is considered a valid bullying measure because the questionnaire minimizes possible respondent bias (e.g., knowledge about the phenomenon) by refraining from using the term bullying. The questionnaire has been validated via numerous studies in multiple countries (Giorgi, Arenas, & Leon-Perez, 2011). The internal consistency of the full questionnaire for the main study was .92, suggesting excellent internal consistency. The Cronbach’s alpha coefficients for the scales Personal Bullying and Work-Related Bullying were .88 and .82, respectively, suggesting acceptable internal consistency. The Cronbach’s alpha coefficient for the scale titled Physical Bullying was .70, suggesting adequate internal consistency.
The questionnaire (Greek version), accompanied by a brief description of the study and a cover letter, were distributed by the principal investigator to the nurse managers of each hospital department. Of the 1,000 questionnaires distributed, 841 (84.1% response rate) were returned completed in sealed envelopes. Participation in the survey was voluntary and responses confidential. Survey data were collected over 5 months (March 2013 to July 2013).
Participants’ responses were initially analyzed using descriptive statistics. The degree of participants’ agreement with each questionnaire item is presented as a mean value, standard deviation, and range. To explore relationships between the sub-scales and the demographic and professional characteristics of the participants (independent variables), bivariate analyses were calculated. If the dependent variable was continuous and more than two independent variables were significant at the p < .2 level in bivariate analysis, multivariate linear regression using the backward stepwise model was applied. For multivariate linear regressions, coefficients’ beta values, 95% confidence intervals, and p values are presented. If the dependent variable was dichotomous and more than two independent variables were significant at the p < .2 level in bivariate analysis, multivariate logistic regression using the backward stepwise model was applied. For multivariate logistic regression calculations, odds ratios, 95% confidence intervals, and p values are presented. Last, multinomial linear and logistic regression were used to develop a model of those independent variables, found to be significantly correlated to the dependent variables in bivariate analyses, and the dependent variables, the sub-scales of the questionnaire. The two-tailed significance level was set at p < .05. The researchers used IBM SPSS 21.0 to calculate the various statistics.
Results
The average age of the participants was 40.1 years, the majority were women, almost half were married and had children, 51% were higher technological institute graduates, and the average number of years of previous hospital experience was 16.1. The detailed demographic features of the study population appear in Table 1. More than 69% of the respondents reported they had not been psychologically harassed in the workplace in the past 6 months. Of those who reported harassment in the past 6 months, 17.2% reported rarely being psychologically harassed, 9.9% occasionally, 2% a few times per week, and 1.1% bullied almost daily.
Study Participants’ Demographic Characteristics
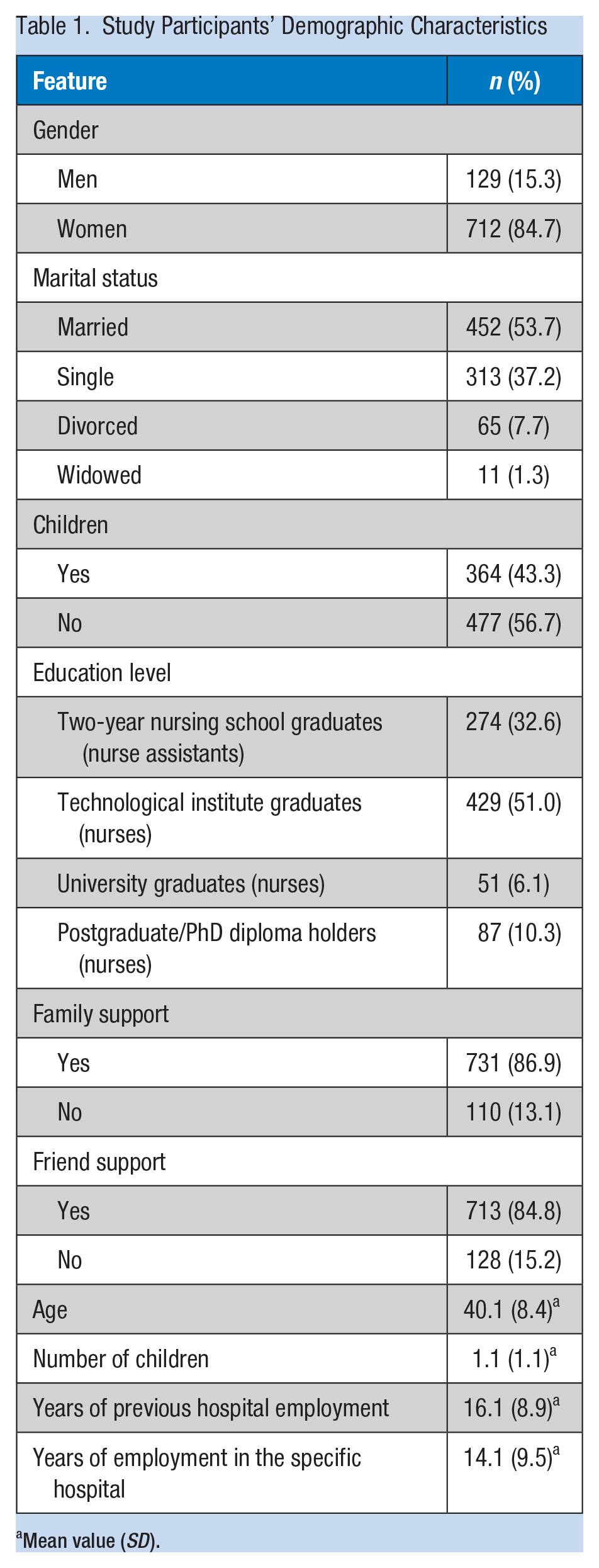
Mean value (SD).
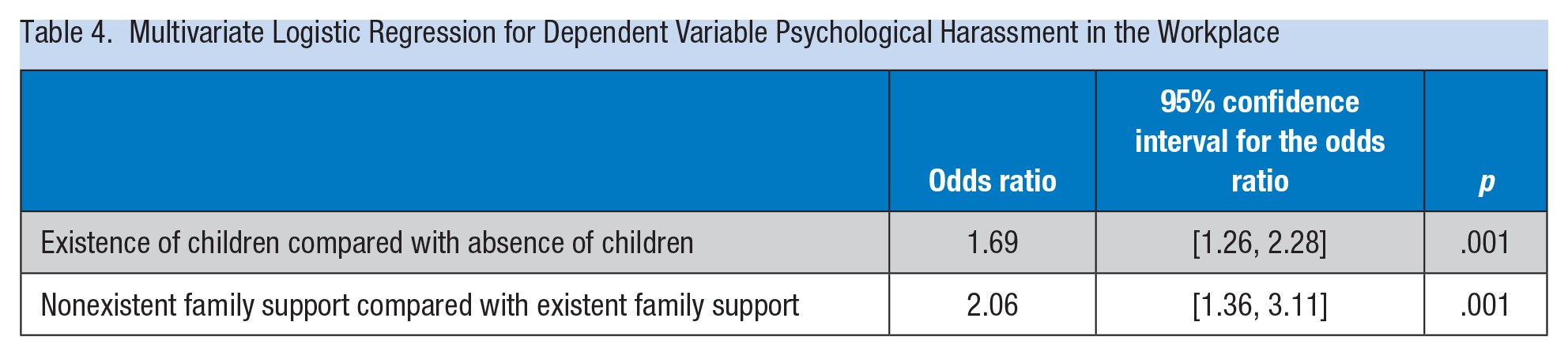
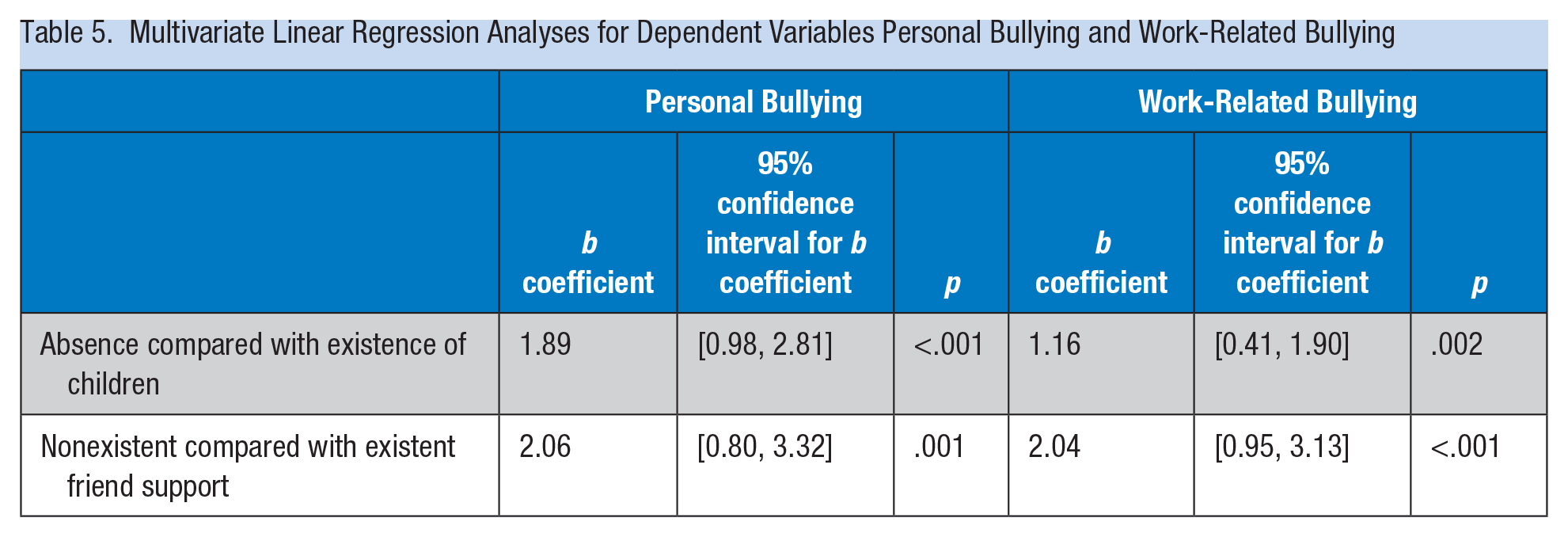
Table 2 presents the results of the bivariate associations between participants’ demographic characteristics and “psychological harassment in the workplace in the past 6 months.” Table 3 presents the results of the bivariate relationships between the participants’ demographic characteristics and the scores on the sub-scales, Personal Bullying, Work-Related Bullying, and Physical Bullying. The findings of the multivariate logistic regression with dependent variable “psychological harassment in the past 6 months” are presented in Table 4. Those participants with children and those who reported they did not receive familial or friend support experienced workplace psychological harassment more often than those with no children and those who reported they had the support of family and friends. The results of the multivariate linear regression analyses for the scales Personal Bullying and Work-Related Bullying are presented in Table 5. Those study participants with no children scored higher on the Personal Bullying and Work-Related Bullying scales than participants with children. Also, those respondents who reported less support from their friends scored higher on the Personal Bullying and Work-Related Bullying scales compared with those who reported more support from friends. No demographic characteristics were related to scale scores for Physical Bullying using multivariate linear regression.
Bivariate Analysis Between (Participants’) Demographic Characteristics and “Psychological Harassment in the Workplace in the Past 6 Months”
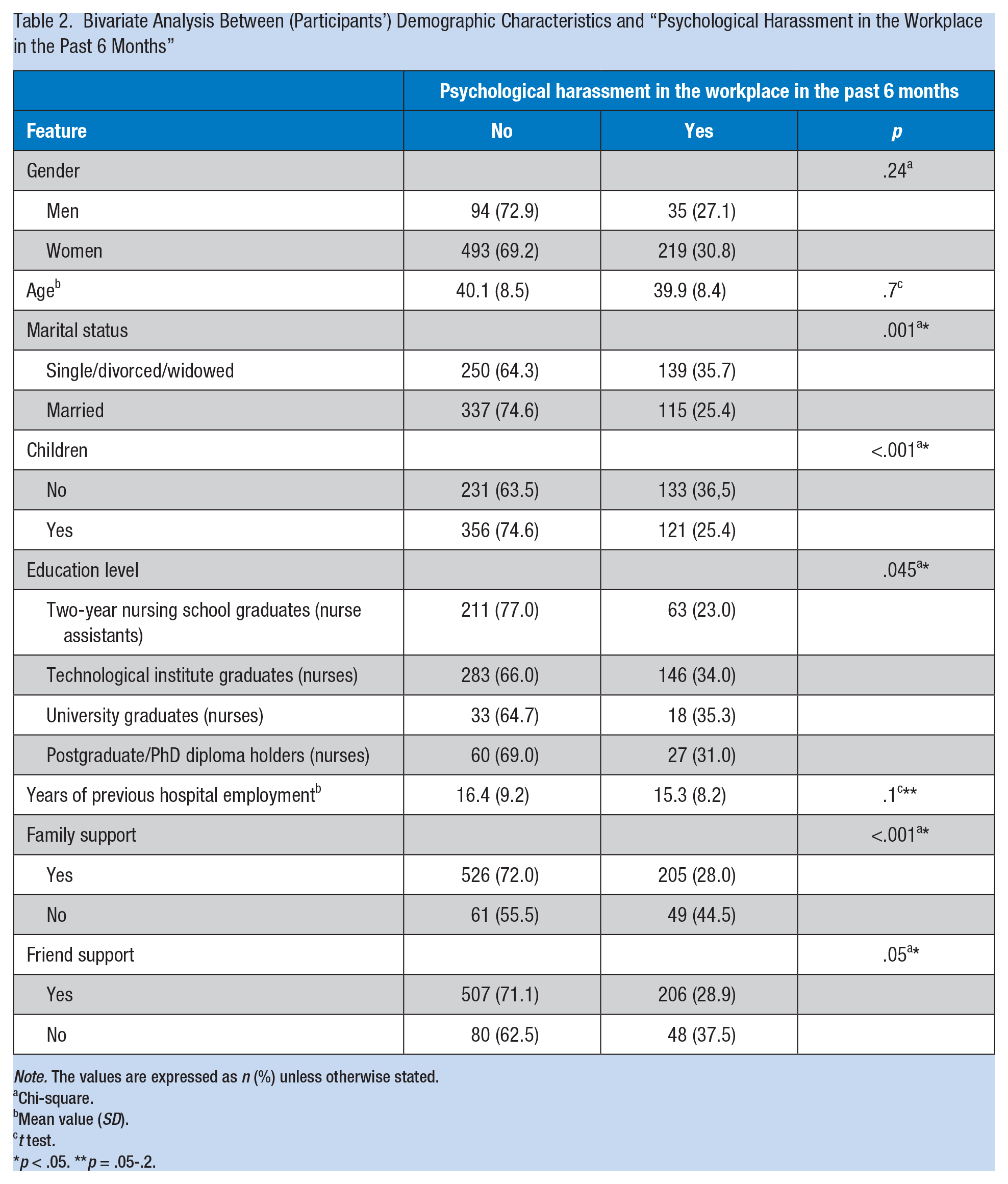
Note. The values are expressed as n (%) unless otherwise stated.
Chi-square.
Mean value (SD).
t test.
p < .05. **p = .05-.2.
Bivariate Analyses Between Study Participants’ Demographic Characteristics and (a) Personal Bullying Score, (b) Work-Related Bullying Score, and (c) Physical Bullying Score
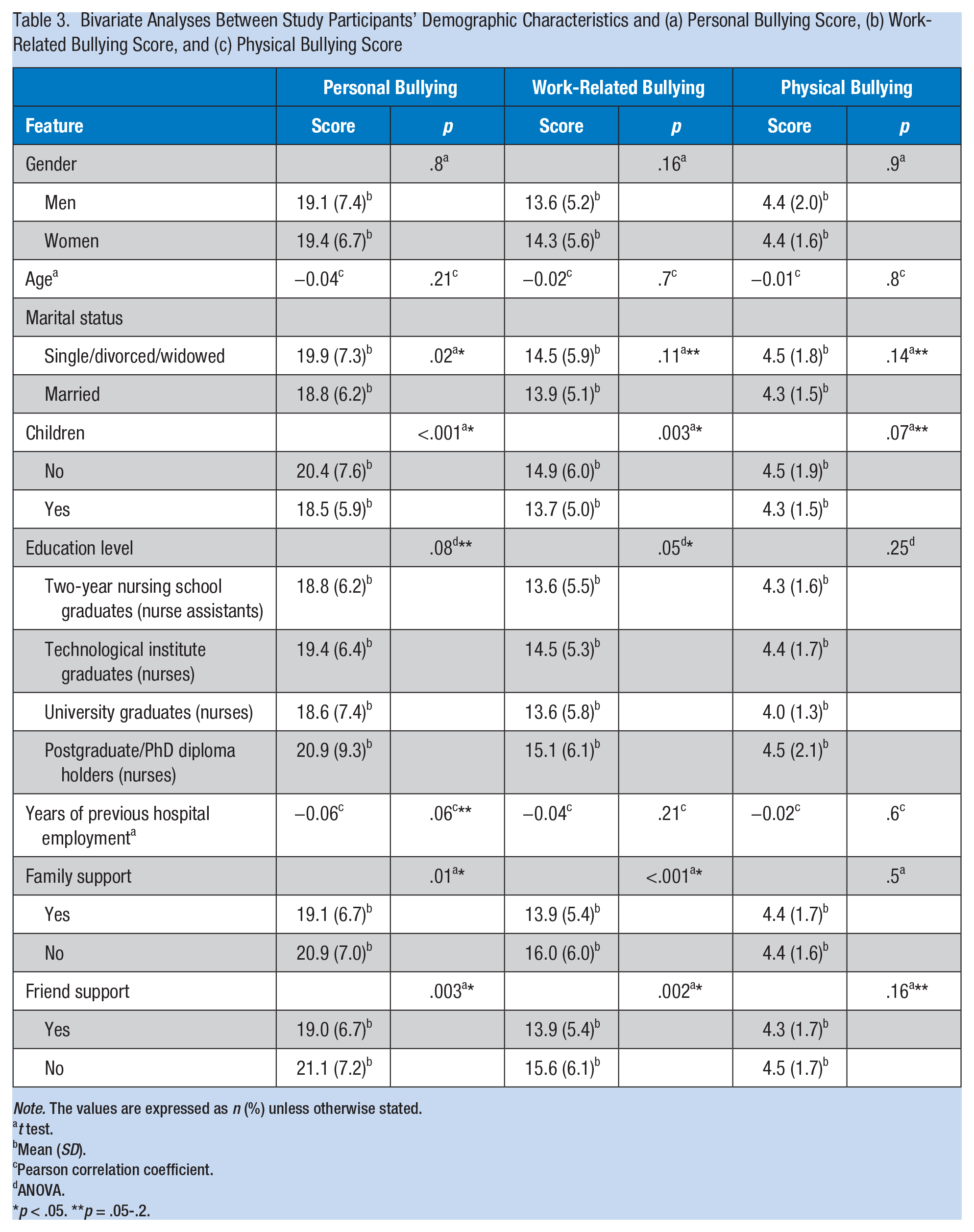
Note. The values are expressed as n (%) unless otherwise stated.
t test.
Mean (SD).
Pearson correlation coefficient.
ANOVA.
p < .05. **p = .05-.2.
Multivariate Logistic Regression for Dependent Variable Psychological Harassment in the Workplace
Multivariate Linear Regression Analyses for Dependent Variables Personal Bullying and Work-Related Bullying
Discussion
One third of the participants in this survey reported they had been victims of psychological harassment in the workplace during the past 6 months. This percentage is higher than the findings of the Sá and Fleming’s (2008) study of nursing staff (N = 107) working in Portuguese public hospitals, 13% of whom reported they had suffered psychological harassment in the workplace in the past 6 months but lower than the findings of other international studies: Quine (2001), in Great Britain, reported the percentage to be 44% of respondents and Etienne (2014) reported 48%. The correlation analysis showed that those participants with children and those who reported they did not receive support from their families and friends experienced more frequent psychological harassment. In addition, those with children and those who said they did not receive support from family and friends perceived more negative behaviors related to personal bullying and work-related bullying. These findings demonstrate the value of support systems in the lives of hospital-employed nurses.
Study Limitations
This quantitative cross-sectional study identified the impact of workplace bullying on nursing staff at select Greek public hospitals. These data are not static but dynamic depending on external and internal situations. Therefore, the survey data may have limited value. The study population was drawn from five Greek National Health Service Hospitals in the 1st Regional Health Authority of Attica, so the generalization of results should be considered accordingly. Given the importance and sensitivity of workplace bullying, the authors are planning more extensive investigations using qualitative research methods to better understand Greek hospitals.
Implications for Occupational Health Nursing Practice
The phenomenon of bullying is a serious problem for the Greek nursing community because bullying has been associated with work-related stress, nurses’ intention to leave the profession, and the quality of patient care delivered (Etienne, 2014; Yildirim, 2009). Therefore, it is imperative that bullying be addressed by assessing and managing the health and safety of nursing staff. The prevention and management of bullying in the workplace concerns both individual workers and their organizations (Vartia & Leka, 2011).
A basic strategy for the primary prevention of bullying is the establishment of an anti-bullying policy (Duffy, 2009; Needham, 2003; Yamada, 2008) that requires changes in values, attitudes, verbal communication, and ways of interacting (Cassitto et al., 2004). Occupational health nurses hold a central role on the inter-professional occupational health and safety team along with occupational physicians, occupational psychologists, and safety professionals. Organizations’ commitment to regularly scheduled education can change organizational culture and climate by focusing on workers and their work-related behaviors. In addition, organizational leadership plays an essential role because executives must role model open, honest, and mutually respectful communication (Yamada, 2008). The organization’s commitment to eliminate bullying and clear expectations of nurse managers’ responsibilities for implementing anti-bullying policies, managing complaints, and applying disciplinary procedures if warranted must be institutionalized (Duffy, 2009; Holme, 2006; Rayner & Lewis, 2011; Vartia & Leka, 2011).
Recruitment procedures should include assessing individuals’ likelihood of bullying other employees (Blackman & Funder, 2002; Fodchuk, 2007; Gardner & Johnson, 2001; Glendinning, 2001), so that candidates with desirable attributes (e.g., integrity and emotional intelligence) are selected for company positions (Yamada, 2008). At the same time, appraisal management policies, including employee rewards, promotion procedures, and effective communication, should be implemented through human resources if complaints of workplace bullying are to be eliminated (Needham, 2003). When an organization identifies bullying, policies and procedures for conflict management and dispute resolution must direct management and workers to immediate negotiation; mediation could also be implemented if necessary (Fox & Stallworth, 2009). A critical element of such procedures is the assurance that retaliation toward or further victimization of the complainant does not occur (Fox & Stallworth, 2009). Management training to implement these strategies for both the prevention of and response to workplace bullying is essential, as numerous studies have demonstrated limited skills in this area (Ferris, 2004) resulting in victims seeking assistance from and alliance with peers who have also been victimized (Cassitto et al., 2004). Peer support, counseling, personal empowerment, and the provision of appropriate guidelines have been shown to be the best practices for many organizations (Lutgen-Sandvik, 2008).
Occupational health nurses can design educational programs to meet the special needs of nurse managers and nursing staff. Such educational programs should enhance awareness of the incidence and effects of workplace bullying and promote a supportive workplace environment (Etienne, 2014). Programs such as cognitive rehearsal training of suggested responses to common bullying behaviors have been demonstrated to decrease workplace bullying (Stagg, Sheridan, Jones, & Speroni, 2013). Other effective strategies include assertiveness training and cultivation of emotional intelligence (Etienne, 2014). Educational programs targeting nurse leaders have been considered even more effective as they can directly transform organizational climate and result in a more positive work environment (Johnson & Rea, 2009). A basic prerequisite for managing bullying is the regular assessment of current and past exposures to violence in each department using comprehensive, reliable, and valid tools, the findings of which can guide future actions.
Conclusion
Effective bullying prevention encompasses a combination of primary, secondary, and tertiary interventions that hinge on the quality of organizational leadership. The strategies for bullying prevention include training, the development of behavioral codes that are acceptable in the workplace, and zero-tolerance for bullying behavior. Support from family and friends also plays a key role in the prevention of workplace bullying among nurses practicing in select Greek hospitals.
Applying Research to Practice
The phenomenon of bullying is a serious problem for the Greek nursing community. The exposure of nurses to workplace bullying is associated with worse overall health (especially mental health).
A basic prerequisite for managing bullying is the regular assessment of exposures to violence in each health service using reliable and valid tools, the findings of which can guide future actions.
Occupational health nurses hold a central role on the establishment of an anti-bullying policy. This policy must be focused on
(a) nurses who do not have children (“person-related bullying” and “work-related bullying”) compared with those who have children,
(b) nurses who are not supported by a friendly environment (“person-related bullying”) in relation to those who are supported by a friendly environment, and
(c) nurses who are not supported by their families (“work-related bullying”) compared with those who are supported by their families.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Christine Karatza completed her PhD at the Faculty of Nursing, University of Peloponnese, Greece. At present, she works in the Perfecture of Attica, Greece, in the sector of public health.
Sofia Zyga is an associate professor, Faculty of Nursing, University of Peloponnese, Greece. Her research interests relate to the field of basic nursing.
Styliani Tziaferi is an assistant professor, Faculty of Nursing, University of Peloponnese, Greece. Her research interests relate to the field of community nursing, focused on occupational health and public health nursing.
Panagiotis Prezerakos is an associate professor, Faculty of Nursing, University of Peloponnese, Greece. His research interests relate to the field of health services management, focused on nursing services.