
Abstract
Long-haul truck drivers are significantly affected by musculoskeletal injuries with incidence rates 3.5 times higher than the national average. Yet, little is known about injuries that affect long-haul trucks drivers. In 2010, interviewers collected data from 1,265 long-haul truck drivers at 32 truck stops across the United States. These surveys were analyzed to describe all self-reported musculoskeletal injuries. Injuries to the arm (26.3%) and back (21.1%) were the two areas most reported in the survey. Musculoskeletal injuries were most often caused by falls (38.9%) and contact with an object or equipment (33.7%) resulting most commonly in sprains/strains (60%). This large scale survey highlights the significance of musculoskeletal injuries in long-haul truck drivers and suggests the need to develop interventions to prevent injuries and improve recovery once injuries occur.
Keywords
Commercial truck drivers are one of the largest employee groups in the United States. In 2015, the Bureau of Labor Statistics reported that 1,797,700 individuals were employed as heavy/tractor-trailer truck drivers in the United States (Bureau of Labor Statistics, 2015a). The commercial driver industry is significantly affected by the cost of workers’ compensation claims; in fact, this industry had the highest average cost per workers’ compensation claim for all age groups and all occupational sectors (Davis, Dunning, Jewell, & Lockey, 2014). Long-haul truck drivers (LHTD) operate trucks with a gross vehicle weight capacity (i.e., the combined weight of the vehicle, passengers, and cargo) exceeding 26,000 pounds and have delivery routes that require them to sleep away from home (National Institute for Occupational Health Safety and Health, 2015). The unique work environments for LHTDs require significant lifestyle changes compared with workers in other industries due to the solitary time drivers spend away from home. This work is also notable for being predominately sedentary with intermittent periods of physical exertion during the loading, unloading, and securing of cargo (Bureau of Labor Statistics, 2015a). LHTDs typically drive vehicles with large box or flatbed trailers; the latter add an additional physical workload due to the use of heavy chains and tarps. Drivers of flatbed trucks are thus at increased risk for occupational injuries.
LHTDs experience one of the highest rates of injury in the United States. Heavy/tractor-trailer drivers experience injuries and illnesses involving days away from work at rates of 355.4 incidences per 10,000 full-time workers. This incidence rate is 3.5 times higher than for all other occupations (Bureau of Labor Statistics, 2015b) and is higher than the rate for other hazardous occupations (e.g., construction and extraction, 168.9 injuries per 10,000 full-time workers; health care practitioners and technical workers, 92.9 injuries per 10,000 full-time workers; and farming, fishing, and forestry, 147.8 injuries per 10,000 full-time workers; Bureau of Labor Statistics, 2015c). Work-related musculoskeletal injuries (WMSI) are among the most common reasons for LHTD work absences. The incidence rate of WMSIs among heavy/tractor-trailer truck drivers is 3 times higher than for all occupations, 108 WMSIs and 31 WMSIs, respectively (Bureau of Labor Statistics, 2015b). In 2014, sprains and strains (151.4 injuries per 10,000 full-time workers) were the most common WMSI among heavy and tractor-trailer truck drivers and pain due to soreness (56.9 injuries per 10,000 full-time workers) was second. The back was the most commonly injured area of the body (61.2 injuries per 10,000 full-time workers) followed by the shoulder (51.4 injuries per 10,000 full-time workers; Bureau of Labor Statistics, 2015b).
The National Institute for Occupational Safety and Health (NIOSH) developed a National Occupational Research Agenda (NORA) to guide the development of research focused on specific occupational groups. In 2009, the NORA report was published, and included four strategic research goals for the Transportation, Warehousing, and Utilities sector (including LHTDs). These goals were (a) reduce lost-workday occupational traumatic injury and fatality rates, (b) reduce the incidence and severity of WMSI, (c) improve health and reduce premature mortality through workplace programs and practices, and (d) identify, evaluate, and reduce chemical, biological, and physical occupational hazards and exposures (NORA Transportation Warehousing and Utilities Sector Council, 2009). Therefore, studies of WMSI among LHTD are both timely and highly significant.
A significant body of prior LHTD research has focused on health status, access to health care, lower back injuries, fatigue, vibration, and injuries related to vehicular accidents. However, few studies have examined WMSIs or studies have targeted all commercial truck drivers, not only LHTDs. Previous studies have shown that LHTDs are significantly affected by WMSIs to the back and shoulder (Davis et al., 2014; McCall & Horwitz, 2005; Smith & Williams, 2014; van der Beek, Frings-Dresen, van Dijk, Kemper, & Meijman, 1992), commonly due to overexertion or repetitive motion (Reiman, Pekkala, Vayrynen, Putkonen, & Forsman, 2014). WMSI occur most often (51%) in drivers with less than a year of work experience (McCall & Horwitz, 2005). LHTDs are also at increased risk of partial or total disability due to WMSIs (Smith & Williams, 2014). Given the frequency and severity of WMSIs among LHTDs, further research about the cause and nature of these injuries is urgently needed.
Due to the unique nature of the work and personal environments of LHTDs, occupational health nurses should understand how WMSIs affect this population. The purpose of this study was to describe LHTDs who report work-related injuries, characterize WMSIs among LHTDs, and identify any associations between LHTDs’ characteristics and specific WMSIs. In this study, WMSIs are defined as a reported occupational injury to the soft tissue, bone, or cartilage that limits an employee’s ability to move and work.
Method
The current study involved a secondary analysis of a subset of NIOSH data following University of Alabama at Birmingham Institutional Review Board approval and the completion of a Data Sharing Agreement between NIOSH and the University of Alabama at Birmingham School of Nursing. A de-identified 2010 dataset from a national survey of LHTD was transferred from NIOSH to the investigators’ fully encrypted and password-protected computers.
This cross-sectional parent study included data from face-to-face interviews of LHTDs at 32 truck stops across the United States. To garner a nationally representative sample, NIOSH used a three-stage sampling process. The first stage targeted sections of interstates or other limited-access highways based on geographic region and truck traffic volume to access the largest possible number of potential participants. In Stage 2, individual truck stops with restaurants and paved overnight parking lots with at least five parking spaces were identified along selected state-highway segments. These features were determined to provide interviewers with the largest possible number of potential participants. Stage 3 included the recruitment of truck drivers by a three-person interview team entering truck stops over a 3-day period.
Potential participants were approached by one member of the interview team to assess their interest in the study. Individuals who agreed to participate were then directed to another team member, who collected informed consent and conducted the interview. Inclusion criteria included driving a truck with three or more axles as a primary occupation for at least 12 months and taking at least one mandatory 10-hour rest period during each delivery run while away from home. A more detailed description of the study and its design, survey, and data collection can be found in Sieber et al. (2014).
Survey Questionnaire
During a meeting of trucking industry health and safety personnel and other trucking industry stakeholders, researchers solicited input for survey instrument development for the parent study. The questionnaire focused on factors which could account for the significant burden of occupational injuries among LHTDs. These factors were represented by eight different categories: work environment, work history, driving practices, health conditions, health risk factors, health insurance coverage, sleep, and demographics (Sieber et al., 2014).
Given that the aim of the current study was to investigate WMSIs in LHTD, the variables of interest were the population demographics, mechanism of injury, types of injury, body area injured, and days of work missed per injury. The mechanism of injury responses included bodily reaction or exertion, contact with an object or equipment, fall to same or lower height, assault, or other. Sprains/strains, fractures, sprains/strains with a fracture, and other were the injury types included in the survey. When injuries were reported as other, participants were asked to specify in their own words the type of injury they experienced. These responses were reviewed to ensure they fit the definition of WMSIs used in this study. Some of the types of injuries that were included in this category were cartilage tears, cervical and lumbar disc herniation, and contusions. Although these injuries did not fit the categories of sprain/strain or fracture, they did impact LHTDs. The area of the body injured was categorized by arm, head, back/neck, leg, foot/ankle, and two or more locations. These injuries were all self-reported and were not linked to any Occupational Injury and Illness Classification System event or exposure code.
Statistical Analysis
After the dataset was received, it was reviewed and cleaned. Descriptive statistics, including means and standard deviations, were calculated for continuous variables; frequency distribution and proportions were computed for all categorical variables. Association rule and chi-square analyses assessed relationships among variables. Association rule analysis is a data mining technique used to analyze categorical data. The technique provides rules for two or more categories that frequently occur together. Association rules are if/then statements that uncover relationships between variables created by analyzing data for frequent if/then patterns and using criteria support and confidence to identify the most important relationships (Agrawal, Mielinski, & Swami, 1993; Agrawal & Srikant, 1994). Association rules are reported with three different statistics: support, confidence, and lift. Support indicates the percentage of times a particular association rule occurs in the entire dataset and the confidence is the probability that the consequent was present based on the antecedent. For instance, a support of 0.5 indicates that the association rule occurs 50% of the time in the dataset, and a confidence of 0.90 indicates that the consequent was present 90% of the time the antecedent occurred in the data. Last, the lift statistic gives the degree of measure (likelihood) one variable is present when along with a different variable. For example, a lift of 1.3 indicates that for a given variable, it is 1.3 times more likely for the other variable to be present. Although association rules were initially developed for consumer market–based analysis, these rules are often successfully applied to other research areas, including health care. For example, Ivancevic et al. (2015) identified risk factors associated with early childhood caries, Pham, Raju, Jiang, and Williams (2016) assessed the black-cloud versus white-cloud phenomenon in apheresis medicine, and Kost, Littenberg, and Chen (2012) demonstrated disease specific co-occurrences using Association Rules.
A statistically significant p value is not the only requirement for a reliable association (American Statistical Association, 2016). Effect sizes are also used to measure the strength of the relationship between two variables on a numeric scale. Several methods can be used to calculate effect size based on the type of data being analyzed. Cramer’s V is used to assess effect sizes for categorical data. The effect size for chi-square, assessed using Cramer’s V, is defined as small (0.1), medium (0.3), and large (0.5; Durlak, 2009). All statistical analyses were completed using R Studio Version 0.99.473 (R Core Team, 2013). Package arules (Hahsler, Gruen, & Hornik, 2005) were used to calculate association rules and the lsr (Navarro, 2015) package was used to calculate Cramer’s V effect size.
Results
In the parent study (Sieber et al., 2014), 5,514 individuals were approached for recruitment as described above; of those, 3,759 met inclusion criteria. The survey was completed by 1,265 LHTDs (34% of eligible drivers). The most common reason for declining participation was perceived time constraints. Participant location was distributed as noted across five geographic regions of the United States: South (29.2%), Great Lakes (25.8%), Central (20.3%), West (17.6%), and Northeast (7.2%).
The Current Study Sample
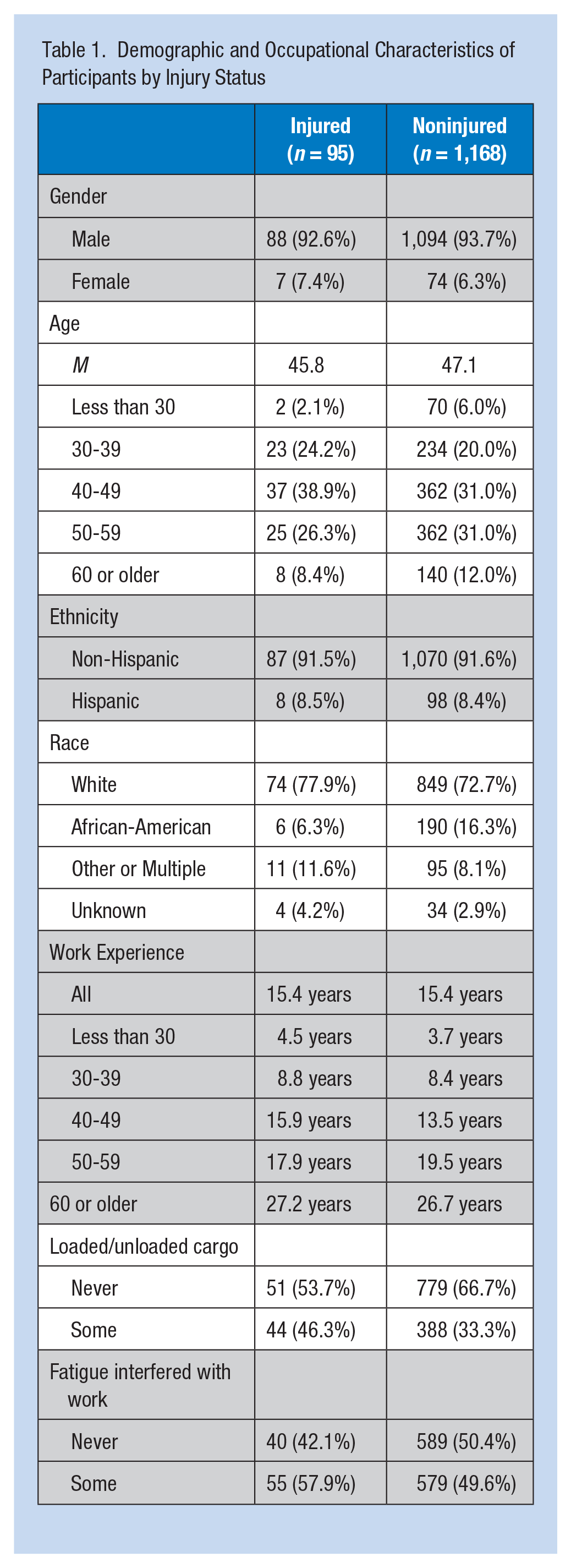
Of the 1,265 LHTDs who completed the survey, 95 (7.5%) reported they had experienced a work-related injury within the 12 months preceding the date of survey completion (Table 1). The demographics of LHTDs who reported work-related injuries within the last 12 months were similar to those LHTDs who did not report an injury (Table 1). The majority of these LHTDs were men (93%) with a mean age of 45.8 years. The LHTDs were mostly middle aged; the age distribution across decades of life for those LHTDs who reported injuries was less than 30 years (2%), 30 to 39 years (20%), 40 to 49 years (39%), 50 to 59 years (31%), 60 years or older (8%). Seventy-nine percent of those LHTDs who reported injuries were Caucasian, 6% were African American, and 8% were Hispanic.
Demographic and Occupational Characteristics of Participants by Injury Status
Work-Related Injuries
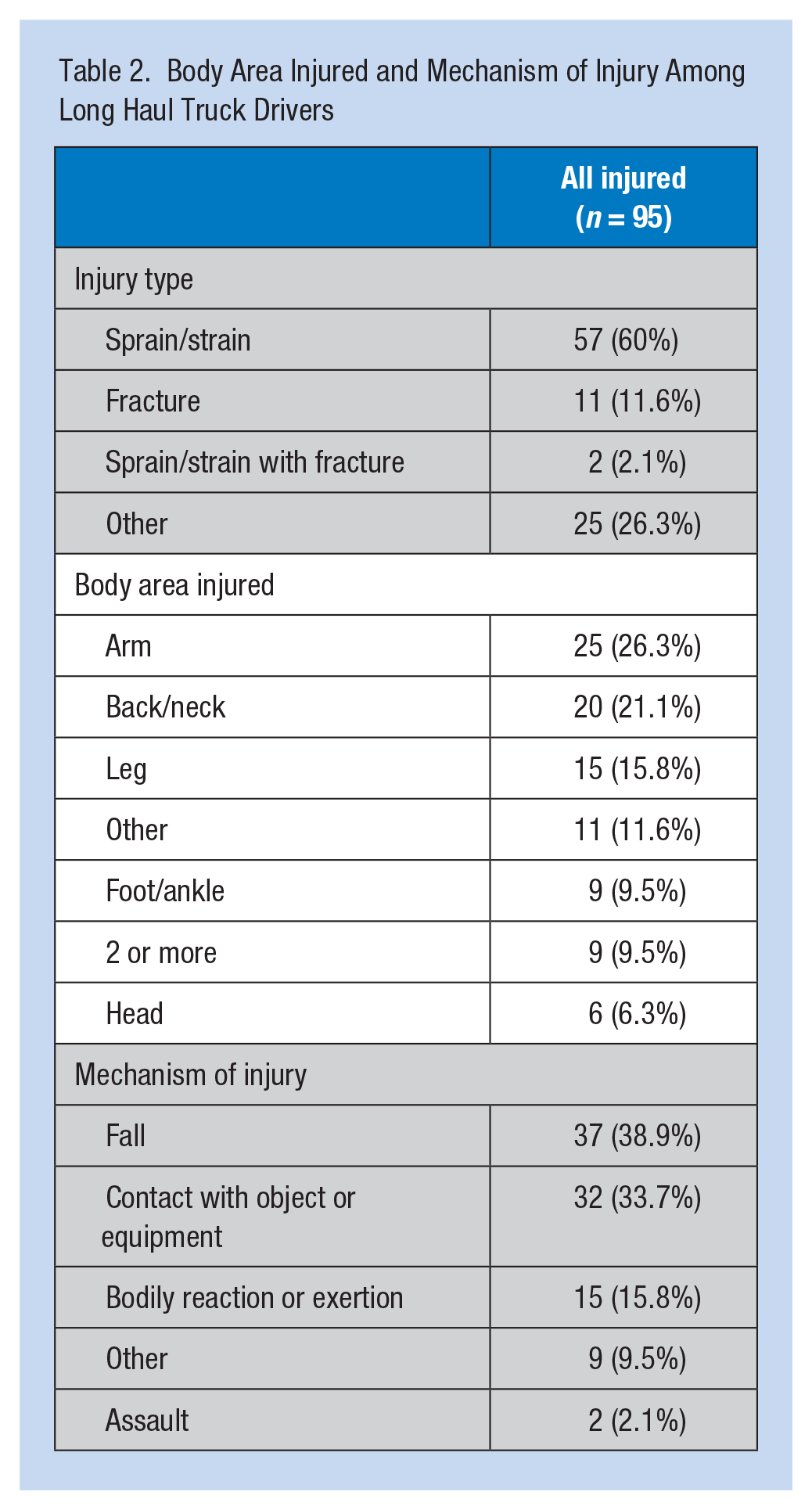
Fifty-three percent of reported injuries within the previous 12 months required at least some time away from work; the median days away from work was 21. The LHTDs reported that the most common area of the body injured was the arm (26%) which includes injuries from the shoulder to the hand (Table 2). The second most commonly affected area was the back and neck (21%). Thirty-seven percent of all injuries reported were the result of a fall to the same or lower level, 32% were the result of contact with an object or equipment, and 15% were the result of the body’s reaction to exertion. A majority of the injuries were reported as sprains, an injury to the muscle, or strains, an injury to a ligament (60%; Table 2). Injuries to the arm, back/neck, and leg required a mean of 9.6, 9.4, and 9.2 days away from work, respectively. When injuries resulted in a sprain/strain, LHTDs missed on average 28 days of work; those injuries resulting in fractures required an average of 24 days away from work.
Body Area Injured and Mechanism of Injury Among Long Haul Truck Drivers
Individuals with work-related injuries reported slightly more instances in which they were required to perform loading and unloading of cargo (47%), and fatigue somewhat interfered with their work (58%; Table 1). Interestingly, only 55% of LHTDs who stated they had an injury in the previous 12 months reported the injury to their employers or filed workers’ compensation. Association rules were run between the mechanism of injury, body area injured, and injury type. The association rules indicated that (Table 3) if the mechanism of injury was body reaction and exertion, it was 1.44 times more likely for the injury to be a sprain/strain with a support of 0.14 and confidence of 0.87. When the body area injured was back or neck, it was 1.55 times more likely for the injury to be a sprain/strain with a support of 0.19 and confidence of 0.90. The body area injured was found to have a statistically significant relationship with both the mechanism of injury (p < .01, Cramer’s V = 0.47) and type of injury (p < .05, Cramer’s V = 0.43; Table 4).
Association Rules Results for Injured Long Haul Truck Driver Participants
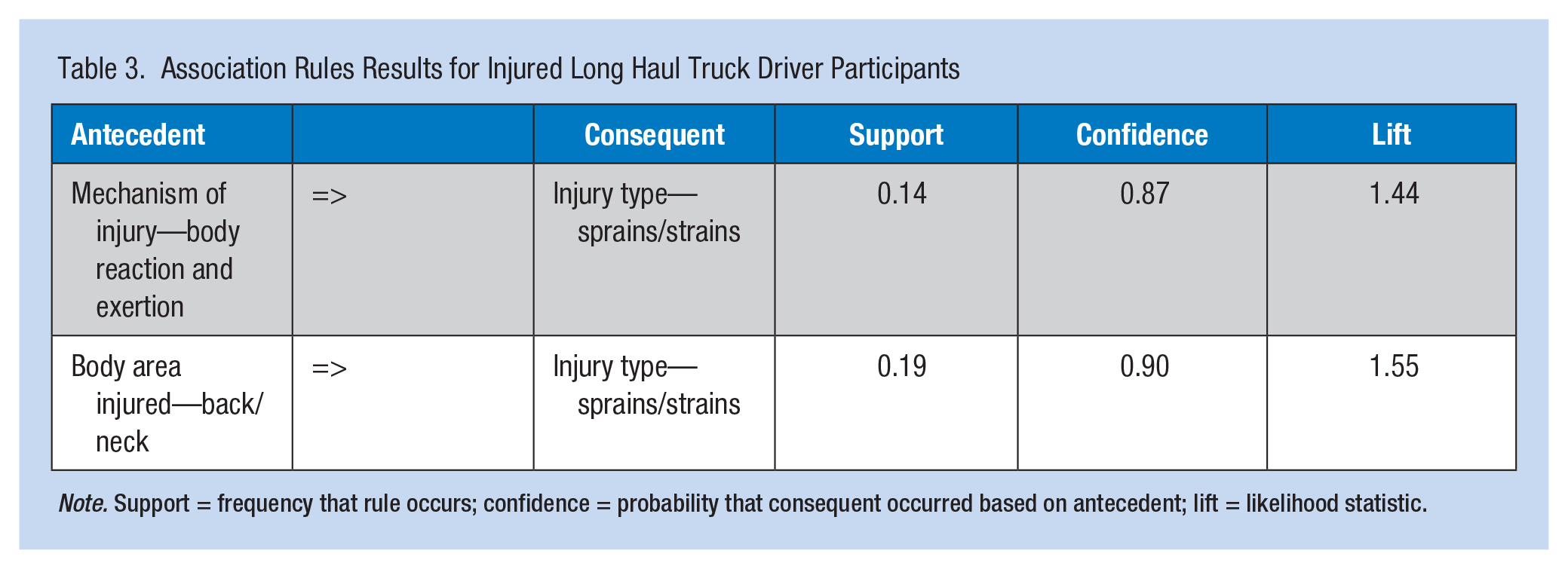
Note. Support = frequency that rule occurs; confidence = probability that consequent occurred based on antecedent; lift = likelihood statistic.
Relationships Between Mechanism, Body Area and Injury Type Among Long Haul Truck Drivers
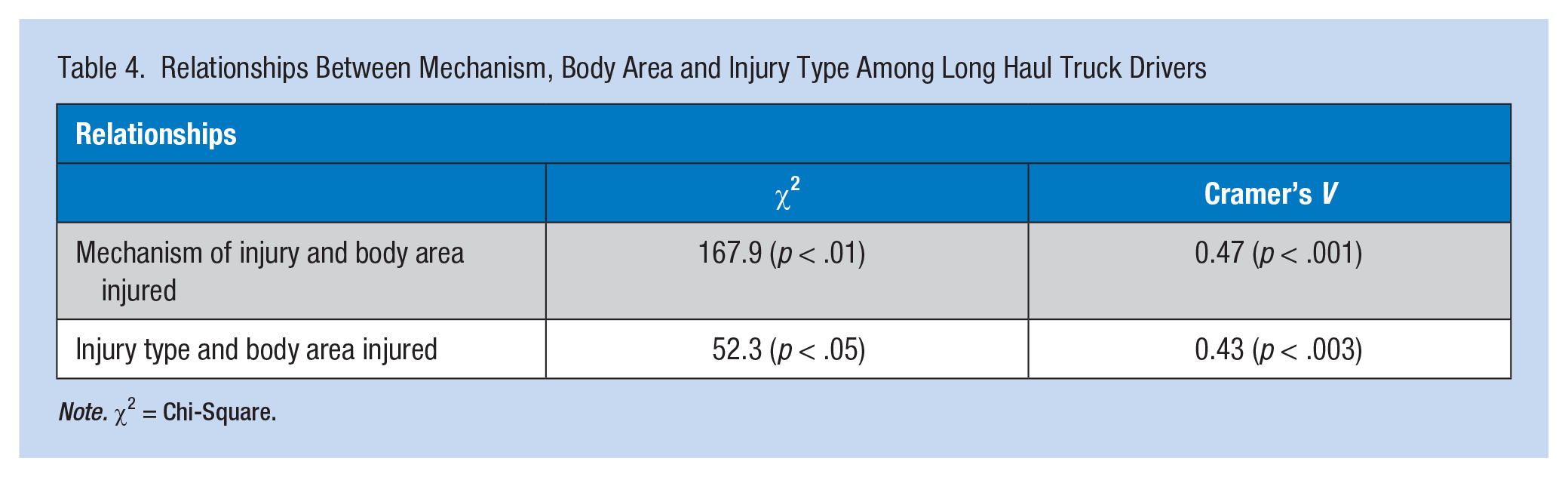
Note. χ2 = Chi-Square.
Discussion
Understanding WMSIs in the LHTD population is critical to building and improving rehabilitative and preventive interventions. This study provides the first representative survey on work-related injuries in a national sample of LHTDs within the United States. The 95 individuals who reported work-related injuries in the previous 12 months did not differ on any demographic variables from those who did not report injuries. The two groups were composed primarily of Caucasian non-Hispanic men between the ages of 30 and 59 with approximately 15 years of long-haul truck driving experience. Consistent with prior research about commercial truck drivers, the largest proportion of work-related injuries occurred among LHTDs within 40 and 60 years of age (65%). This finding supports past commercial truck driver research (Davis et al., 2014; Smith & Williams, 2014). Close examination of work experience showed that injuries to the arm and back/neck occurred predominately among LHTD with less than 15 years of work experience: at an average of 14.8 years for those with arm injuries and 14.4 years of experience for those with back/neck injuries. Also consistent with previous research on commercial truck drivers and via annual OSHA reports, LHTDs reported that the arm and back/neck were the two most frequently injured body areas (Bureau of Labor Statistics, 2015c; Davis et al., 2014; McCall & Horwitz, 2005; Smith & Williams, 2014; van der Beek et al., 1992).
Falls to either the same or lower levels were the mechanism of injury in 39% of reported injuries. The other significant mechanism of injury was contact with an object or equipment which accounted for 32% of the injuries. Past research has also shown that falls and contact with objects are two of the most common mechanisms of LHTD injuries but other researchers did not look at the mechanisms of injury related to the specific joints or body areas affected (Bureau of Labor Statistics, 2015b).
This study confirms previous research on the prevalence of injury mechanism and body area injured in LHTDs and is the first to describe the mechanism of injury in relation to the body area injured. Sixty-two percent of all injuries reported by LHTDs were to the arm, back/neck, and leg. Survey results revealed that the mechanism of injury for arm injuries was most commonly contact with an object (42%), with falls being the second most frequent (31%). Arm injuries were reported to most often be sprains/strains (60%) followed by “other” (28%). Injuries described as “other” included lacerations, contusions, and impalements. Back injuries were reported to be caused by three different, but equally common mechanisms (i.e., contact, 30%; falls, 35%; and body reaction/exertion, 35%); however, the actual injury type was almost exclusively sprains/strains (90%). Leg injuries were most frequently attributable to falls (60%) and body reaction/exertion (26%). Sprains/strains accounted for 60% of all leg injuries; injuries described as “other” accounted for 33% of injuries reported.
Sprains and strains were the most common injury types and it is not surprising that they were also found to be associated with the mechanism of injury, body reaction/exertion, and the body area injured, primarily back/neck. Association rules showed that sprains/strains were found more often than expected when the cause of the injury was body reaction/exertion and the body area affected was back/neck. The area of the body injured was shown to have a statistically significant relationship with the mechanism of injury and the injury type.
This study confirms that, as with all commercial drivers, injuries to the arm and back—most frequently, sprains/strains and fractures caused by falls and contact with an object—significantly affect LHTDs, resulting in physical distress and lost days of work and impacting both drivers and employers (Bureau of Labor Statistics, 2015b; Davis et al., 2014; McCall & Horwitz, 2005; Smith & Williams, 2014; van der Beek et al., 1992). These results can clarify the injuries most likely to occur among LHTDs, and assist health care providers and companies in developing effective preplacement assessments focused on the most affected body areas and tools to decrease stressors on those areas, with the ultimate goal of improving the health and productivity of LHTDs.
Strengths/Limitations
One of the main strengths of this study was the use of association rules as part of the analysis process. The use of association rules is a new and novel approach to data analysis in health care research; this study illustrates its potential applications and benefits. Limitations of the initial study design include the following: the self-report nature of the survey or limited health care literacy and incomplete understanding of musculoskeletal injuries may have led to recall bias; the cross-sectional study design cannot determine causality but rather associations and risk factors; and the small number of participants who reported WMSIs. Due to the limited size of the sample and because weighted samples could not be created for this study, the findings cannot be generalized nationally. Although it is beneficial to describe the sample and reported injuries, more research with larger samples is needed to truly understand the risk factors and causes of these injuries. A more detailed discussion of the general strengths and limitations of this NIOSH survey is included in the initial study report (Sieber et al., 2014).
Conclusion
The NIOSH parent survey was the first study to examine a national population of LHTDs. It revealed that WMSIs are the most commonly reported work-related injuries. This secondary analysis revealed that injuries were most often sprains and strains and affected the arms and back more often than other body areas. Although this study described demographics, mechanisms of injury, type of injury, and affected areas of the body for reported work-related injuries, more research is needed. These injuries impact LHTDs but little is known about their causes or risk factors. This study suggested a need for further research to investigate the most common injuries experienced by LHTDs to uncover risk factors and mechanistic causes. Future research could provide additional information needed to develop prevention and intervention protocols to address the needs of and decrease the burden of WMSIs on LHTDs, employers, and the health care system.
Applying Research to Practice
This study suggests a need for further research to investigate the most common injuries experienced by LHTDs with the goal of uncovering risk factors and mechanistic causes. By applying what has been learned in this study, future research can be done to advance the health care of LHTDs. Future research will lead to a better understanding necessary to develop prevention and intervention protocols to address the needs of the LHTD and decrease the burden of WMSIs on LTHDs, employers, and the health care system. This study will also help current occupational health nurses better understand the injuries sustained by LHTDs which in turn will allow them to help workers manage their injuries more effectively and to develop the most appropriate plan of care.
Footnotes
Acknowledgements
The authors thank all the individuals who assisted in the development of the survey questionnaire and conducted the initial study. They particularly thank the participating truck stops and drivers without whom this study would not have been possible.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute for Occupational Safety and Health with partial funding from the Federal Motor Carrier Safety Administration, U.S. Department of Transportation.
Author Biographies
Bryan Combs has been a faculty member at the UAB School of Nursing for 1 year. He has extensive experience in orthopedics as both a certified athletic trainer and a registered nurse. He currently teaches in the Family Nurse Practitioner Program and works as a Family Nurse Practitioner at the UAB School of Nursing Foundry clinic as his faculty practice. He has begun his doctoral work at the UAB School of Nursing and will be concentrating his education on occupational health and orthopedics.
Karen Heaton’s program of research is primarily focused on the effects of sleep deprivation and obstructive sleep apnea on cognition and injury risk in workers. For example, she has been involved in projects that explored the impact of distraction and health issues on driving and driving performance issues among aging truck drivers, and self-assessment of driving performance compared with real-time simulated driving performance among truck drivers.
Dheeraj Raju has more than 6 years of statistical and research expertise, with a strong academic background in applied statistics, data mining, industrial engineering, and research. With the rapid increase in the amount of data that is being collected, he believes that data mining techniques can effectively extract expedient information. He is particularly interested in using these contemporary statistical data mining and machine learning techniques as they have not been explored in the areas of nursing and health sciences research.
D. E. Vance actively researches neurocognitive aging and HIV. His funded studies focus on cognitive training, cognitive prescriptions, transcranial direct current stimulation, olfactory dysfunction, aging with HIV, and HIV-Associated Neurocognitive Disorder (HAND). He chairs the Neurocognitive Working Group of the Women’s Interagency HIV Study, a national longitudinal cohort study. He has been an invited participant to a specially convened White House forum and an NIH Think Tank, both focused on aging with HIV.
W. Karl Sieber is a research health scientist in the Division of Surveillance, Hazard Evaluations, and Field Studies at the National Institute for Occupational Safety and Health (NIOSH) in Cincinnati, Ohio. He received the PhD and MS (Hyg) in biostatistics from the University of Pittsburgh, Graduate School of Public Health and has been with NIOSH since 1982. His fields of expertise include statistics, epidemiology, survey design, and industrial hygiene.