
Abstract
The study aimed to gain knowledge about low back pain (LBP) in nurses working in the orthopedic departments of tertiary hospitals in Sichuan province, China. We used a cross-sectional survey to examine the prevalence of LBP among 797 inpatient nurses who had worked for 1 year in an orthopedic department in one of 29 hospitals (Grade 3A) in Sichuan province. The survey included a questionnaire to determine the prevalence of LBP and factors related to LBP, a screening graph of LBP symptoms, the Roland Morris Disability Questionnaire (RMDQ), and the Fear Avoidance Beliefs Questionnaire (FABQ) for LBP. The 1-year period prevalence of LBP in the nursing population was 66.8% and the point prevalence was 51.3%. Among the 523 nurses who had experienced LBP, the mean total number of days that LBP had been experienced during the past year was 20.2 ± 16.3 days (range = 1-90 days). The annual number of episodes of LBP was 5.7 ± 4.5 times/year (range = 1-20 times/year). More than half the orthopedic nurses (51.1%) planned to quit, and 5.8% thought of leaving their job due to LBP. These study findings indicate that nurses in this region experience a burden of LBP similar to those in other regions in the world.
Keywords
Introduction
Low back pain (LBP) has become the most common occupational injury in many countries and one of the most common reasons for people to see a doctor, stay in the hospital, or receive surgical treatment (Manchikanti, Singh, Falco, Benyamin, & Hirsch, 2014). Research has demonstrated that most cases of LBP are self-limiting, with spontaneous recovery occurring in 95% of people affected (Manchikanti et al., 2014). However, the recurrence rate is as high as 60% to 85%, and this can seriously influence a person’s quality of work and life (Kabir-Mokamelkhah, Bahrami-Ahmadi, & Aghili, 2016; Pengel, Herbert, Maher, & Refshauge, 2003). The morbidity rate of LBP in the general population is between 12% and 33% (Chou & Shekelle, 2010). However, the high prevalence of LBP makes it difficult to determine how often these cases are work-related (Lastovkova et al., 2015). Recent studies in Greece and Australia reported prevalence estimates of 51% and 56%, respectively (Alexopoulos et al., 2011; Urquhart et al., 2013). A recent systematic review determined that the worldwide prevalence of LBP among nurses ranged from 50% to 80% (Budhrani-Shani, Berry, Arcari, Langevin, & Wayne, 2016). Furthermore, rates of 53% to 75.9% have been reported in nurses in China (Li et al., 2012; Xu et al., 2012; Yue, Liu, & Li, 2012), far higher than the rate in the general population in this country. In the United States, a study observed that 12% of nurses left the profession due to back injuries during 1980 to 2012 (Yassi & Lockhart, 2013). Thus, it is likely that LBP has resulted in a loss of working days for many nurses and caused nurses to leave their profession. LBP and the associated loss in working days results in a deficit in human resources for nursing and hampers the continuity of nursing care and the provision of a quality nursing service (Harcombe, Herbison, McBride, & Derrett, 2014; Punnett et al., 2005). Compared with other departments, patients in orthopedic departments are likely to have greater physical dysfunction and require surgical treatment (Vieira, Kumar, Coury, & Narayan, 2006). This means that nurses in orthopedic departments often have to carry rehabilitation instruments, move patients from a temporary bed to a fixed bed, and assist patients with turning in bed. In addition to this, the workload of clinical nurses is considerable. Therefore, understanding the status and characteristics of LBP and its impact on ability to work in nurses in orthopedic departments is significant and meaningful. The aim of this study was to survey nurses in orthopedic departments in Sichuan province, China to determine the prevalence of LBP. We also studied whether LBP resulted in nurses wishing to quit the profession. This information aims to increase awareness of LBP in nurses in orthopedic departments for the purpose of informing prevention strategies.
Method
Study Design and Population
This was a cross-sectional survey of the prevalence of LBP in nurses working in an orthopedic department. Cluster sampling was used to select 29 hospitals from all tertiary hospitals in Sichuan province, China. In China, tertiary hospitals are comprehensive general hospitals with a bed capacity exceeding 500, which provide specialist health services and serve as medical hubs for multiple regions. Tertiary hospitals are further subdivided into three grades, 3A (largest and most specialized/comprehensive), 3B, and 3C. The 29 hospitals included in this study were Grade 3A hospitals. LBP status was investigated in nurses who had worked for at least 1 year as inpatient nurses in orthopedic departments at the 29 tertiary hospitals in Sichuan province. Reasons for exclusion from the study included the following: being an advanced student nurse, being on probation status, and not being licensed to practice. Once enrolled in the study, investigators screened for those who had LBP caused by congenital spinal disorders, tumors, or infections; fracture or gynecological disease were also excluded.
Ethics
The Biomedical Ethics Committee of the West China Hospital of Sichuan University approved our study before it was started, and we complied with all ethical requirements. Prior to the study start, we informed the study participants about the study aims, significance, and benefits, and that all responses would be confidential. We then obtained informed consent.
Study Method
A self-designed questionnaire, Visual Analog Scale (VAS) for LBP severity, Roland Morris Disability Questionnaire (RMDQ; Roland & Fairbank, 2000), and Fear Avoidance Beliefs Questionnaire (FABQ; Waddell, Newton, Henderson, Somerville, & Main, 1993) were used to evaluate LBP.
A survey of factors related to LBP was included in the self-designed questionnaire in accordance with the study objective. The main contents of the questionnaire were 40 items that collected data regarding each participant’s basic personal information, career information, social/psychological situation, and life habits. To adhere to scientific standards, our investigation was carefully revised according to suggestions from experts in the field, and the contents of the survey of factors related to LBP underwent validity testing. The content validity rate (CVR) of our questionnaire was 0.930 overall and ranged from 0.840 to 1.000 for each dimension (0.840 for basic personal information, 1.000 for career information, 0.900 for social/psychological situation, and 1.000 for life habits). The reliability of our questionnaire was tested using the results from a sample of 50 nurses who were selected independently prior to the start of this study; these 50 nurses were selected by convenience sampling, using the same inclusion criteria as the main study, from the orthopedic department of West China Hospital of Sichuan University. The overall reliability coefficient (Cronbach’s alpha) of the questionnaire was .909, and the reliability coefficient for each dimension ranged from .701 to .987 (.701 for basic personal information, .987 for career information, .835 for social/psychological situation, and .796 for life habits). Both study reliability and validity were high.
The VAS for LBP severity was used to evaluate the degree of backache, including the levels of current pain, the most severe pain, the mildest pain, and pain during ordinary days.
Screening graph of LBP symptoms
A screening graph of LBP symptoms was drawn after consulting experts in spinal surgery and rehabilitation medicine, in accordance with the definition of LBP by the American Association for Health Care Policy and Research (Bigos, Bowyer, & Braen, 1994). This system was chosen because it is commonly used in hospitals in Sichuan province. The aim was to characterize the current issues and obtain the prevalence of LBP over 1 year. LBP was defined as pain or discomfort occurring in the shadowed section in Figure 1 (the back at levels C7 to S1 and the buttock area).
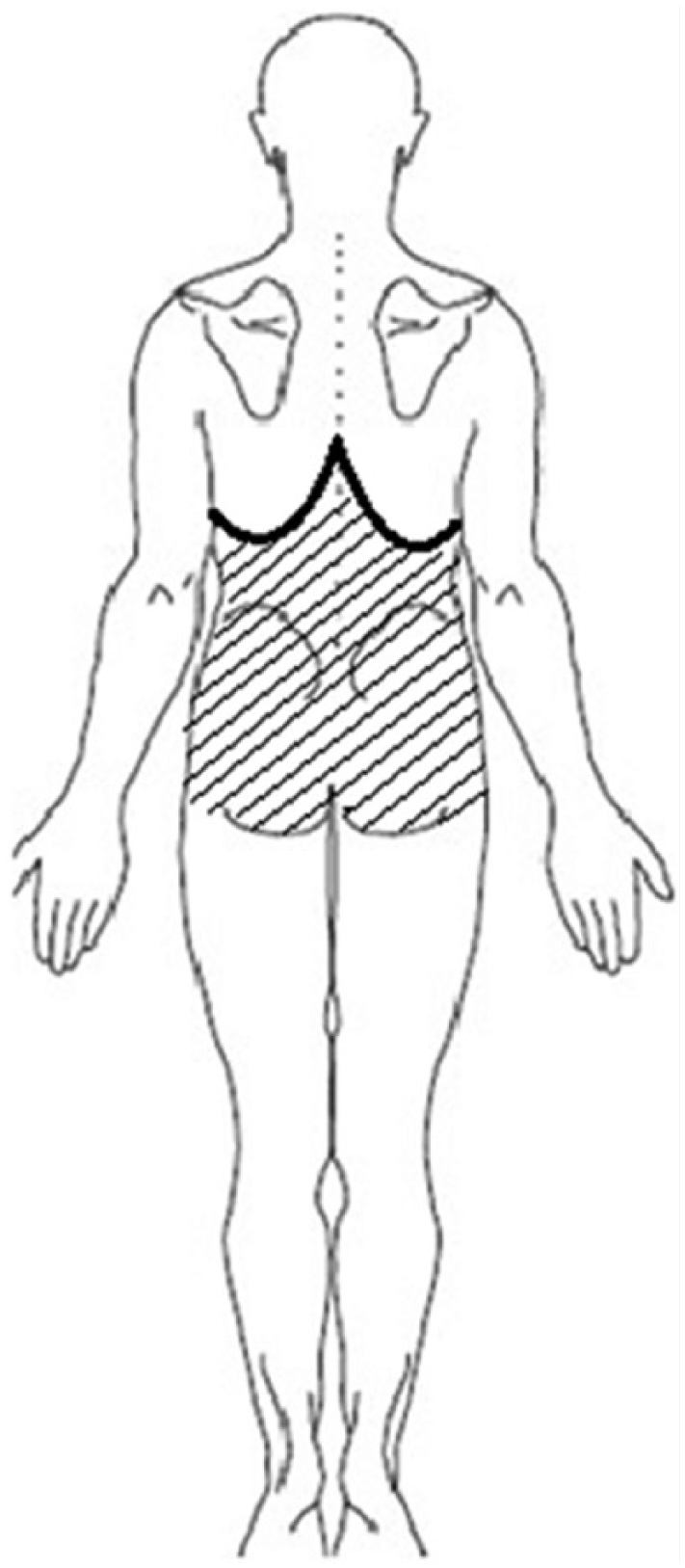
Screening graph used for symptoms of low back pain.
Medical history of LBP
Based on our literature search, we designed a questionnaire to determine the medical history of LBP. This was composed of 13 items including most recent LBP episode, amount of sick leave, number of episodes of pain during the past 1 year, duration of pain, type of pain, mode of pain, and plans to leave work.
RMDQ
The RMDQ was used to evaluate the functional status of nurses with LBP (Roland & Fairbank, 2000). We utilized the Chinese version of RMDQ, which is considered to have good validity and reliability (Fan, Hu, Hong, & Zhao, 2012). The questionnaire contains 24 questions concerning the impact of LBP on walking, bending, sitting, being in the supine position, dressing, sleeping, psychological status, self-care ability, and daily life. Each question was limited by “due to LBP” to differentiate from other causes of pain, which made the questions clear and straightforward to answer. The CVR and reliability coefficient of RMDQ were tested in the 50 participants included before the start of the main study, as described above. The CVR was 1.00 and the reliability coefficient was .915.
FABQ
The FABQ was adopted for the evaluation of fear avoidance beliefs brought about by LBP with regard to physical activities and working ability (Waddell et al., 1993). A Chinese-language version of the FABQ developed in 2010 has good validity and reliability for use in China (Pei, Xia, & Yan, 2010). The CVR of the FABQ was 1.00 and the reliability coefficient was .916, which was determined in the 50 participants included before the start of the main study, described above.
Participant recruitment and data collection
First, our researchers trained the head nurses from each hospital at an academic exchange conference by explaining the purpose, significance, and workflow of this research, to ensure that the study was conducted successfully and correctly. Then, the detailed inclusion and exclusion criteria and other matters requiring attention were communicated to the head nurses via email. The head nurses assisted with screening nurses for the initial exclusion criteria, which included, for example, being an advanced student nurse, being on probation status, and not being licensed to practice.
A self-designed table (“List of nurses in tertiary hospitals of Sichuan province”) created by the researchers was sent to the head nurses by email to ensure that the copies of the questionnaires were correctly distributed. The table contained the hospital names, number of orthopedic wards, number of orthopedic nurses, and number of orthopedic beds. The questionnaires were sealed in paper bags and collected with the assistance of the orthopedic head nurses. Once completed, investigators used the collected data to screen and exclude those who had LBP caused by congenital spinal disorders, tumors, or infections; fracture or gynecological disease were also excluded.
Data analysis
Questionnaires were reviewed and excluded if necessary, and data from valid questionnaires were input into the database. Then, the data were compared and judgments were made regarding false and missing records, validity, truth, and reliability. If a survey was returned with less than 90% of the questions answered, it was defined as unusable and excluded. In addition, correction for logic errors was undertaken to identify and exclude unreasonable responses such as out-of-range values (e.g., reporting a pain score of 12 when the range was 0-10) as well as to identify inconsistencies between responses. The latter involved comparing the same or similar questions within or between surveys to ascertain whether they were answered consistently and, if not, to determine which answer was correct.
The participants were classified into categories according to body mass index (BMI) using standard criteria for Asian populations (World Health Organization [WHO] Expert Consultation, 2004). The participants were also classified into two groups according to age: young orthopedic nurses (19-34 years) and middle-aged orthopedic nurses (35-55 years); it should be noted that the minimum age for a qualified nurse in China is 19 years, while the mandatory retirement age is 55 years.
Statistical Method
SPSS Version 17.0 (SPSS Inc., Chicago, IL, USA) was used for data entry and statistical analysis. Any participant survey with less than 90% of the questions answered was excluded, and correction for logic errors was conducted after data entry. Appropriate statistical methods were utilized based on the data type and distribution, and the alpha level was set at .05. For measurement data, the central tendency was described by the mean or median and discrete trends by standard deviation or interquartile range. Data counts were described as percentages. Correlation analysis of the prevalence of LBP characteristics and adverse effects was made. For the analysis of risk factors for LBP, the annual prevalence of LBP was considered a dichotomous outcome variable (yes, no). The annual prevalence was defined as the percentage of all nurses surveyed who had reported LBP during the previous year. Point prevalence was defined as the percentage of all nurses surveyed who had reported LBP during the previous week.
Results
A total of 797 copies of the questionnaires were returned, resulting in a return rate of 100%. Based on the exclusion criteria, 783 copies of the questionnaires were considered valid, so the effective return rate was 98.2%. Among the 783 participants, 771 were female (98.5%) and 12 were male (1.5%). The mean age was 30.0 ± 8.2 years (Table 1).
Demographic and Personal Characteristics of Orthopedic Nurses at the 29 Tertiary Hospitals in Sichuan Province, China (N = 783)
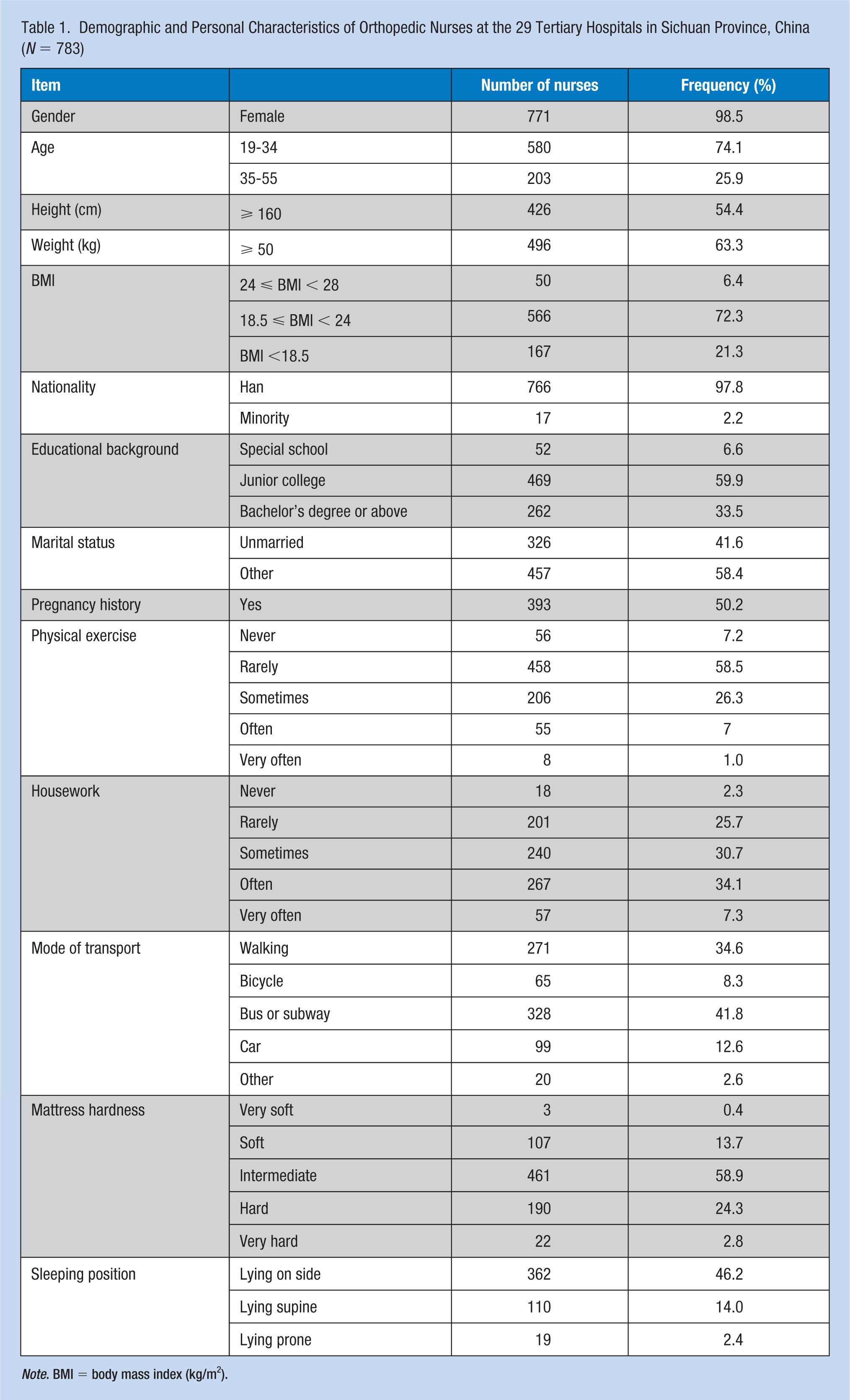
Note. BMI = body mass index (kg/m2).
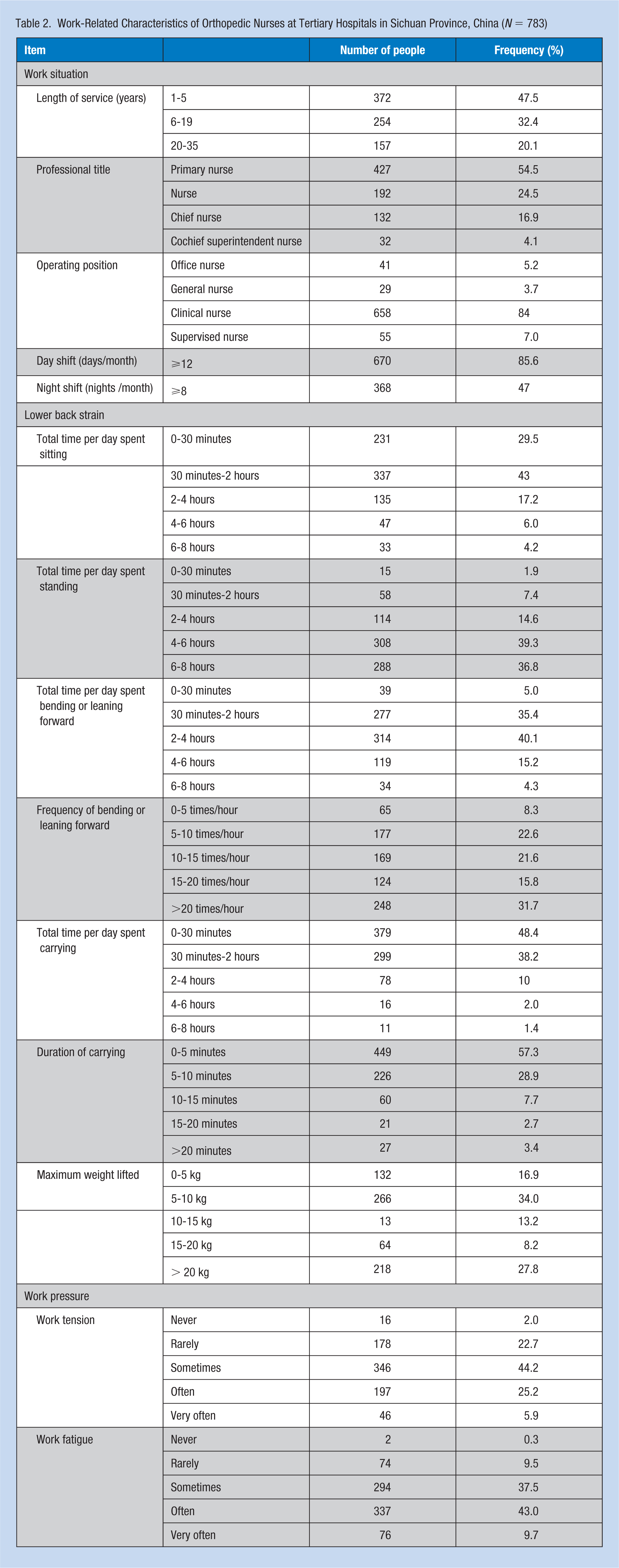
Most (47.5%) of the nurses had been working for less than 5 years and were (84.0%) clinical primary nurses working for more than 12 days/month (Table 2). The low back strain duration ranged from 0 to 30 minutes per day (29.5%) up to 6 to 8 hours (4.2%). As expected, nurses spent a considerable amount of time (4 to 8 hours per day) standing (76.1%), along with other activities of bending and leaning forward.
Work-Related Characteristics of Orthopedic Nurses at Tertiary Hospitals in Sichuan Province, China (N = 783)
Among the 783 participants, 523 orthopedic nurses had experienced LBP within the previous year and 402 had experienced LBP within the past week (Table 3), resulting in a 12-month prevalence of 66.8% and a point prevalence of 51.3%. The 12-month prevalence of LBP was 63.8% (370/580) in nurses aged 19 to 34 years and 75.4% (153/203) in those aged 35 to 55 years. The mean duration of each episode of LBP was 4.3 ± 3.1 days, and the number of working days lost reached 186 days/year, with a mean value of 0.36 days/person/year. The mean age of the nurses at the time when LBP first developed was 25.7 ± 5.5 years (range = 19-45 years). The overall FABQ score was 49.2 ± 18.6 points (range = 3-96 points), and the dimension subscores were 22.1 ± 8.7 for fear avoidance beliefs due to work, 6.3 ± 7.5 for work prediction, and 20.8 ± 6.4 for fear avoidance beliefs due to physical activity (Table 4). Among the 523 nurses who had experienced LBP, the mean total number of days on which LBP had been experienced during the past year was 20.2 ± 16.3 days (range = 1-90 days). The annual number of episodes of LBP was 5.7 ± 4.5 times/year (range = 1-20 times/year).
Nature of Low Back Pain Among Orthopedic Nurses at Tertiary Hospitals in Sichuan Province Who Reported Low Back Pain (N = 523)
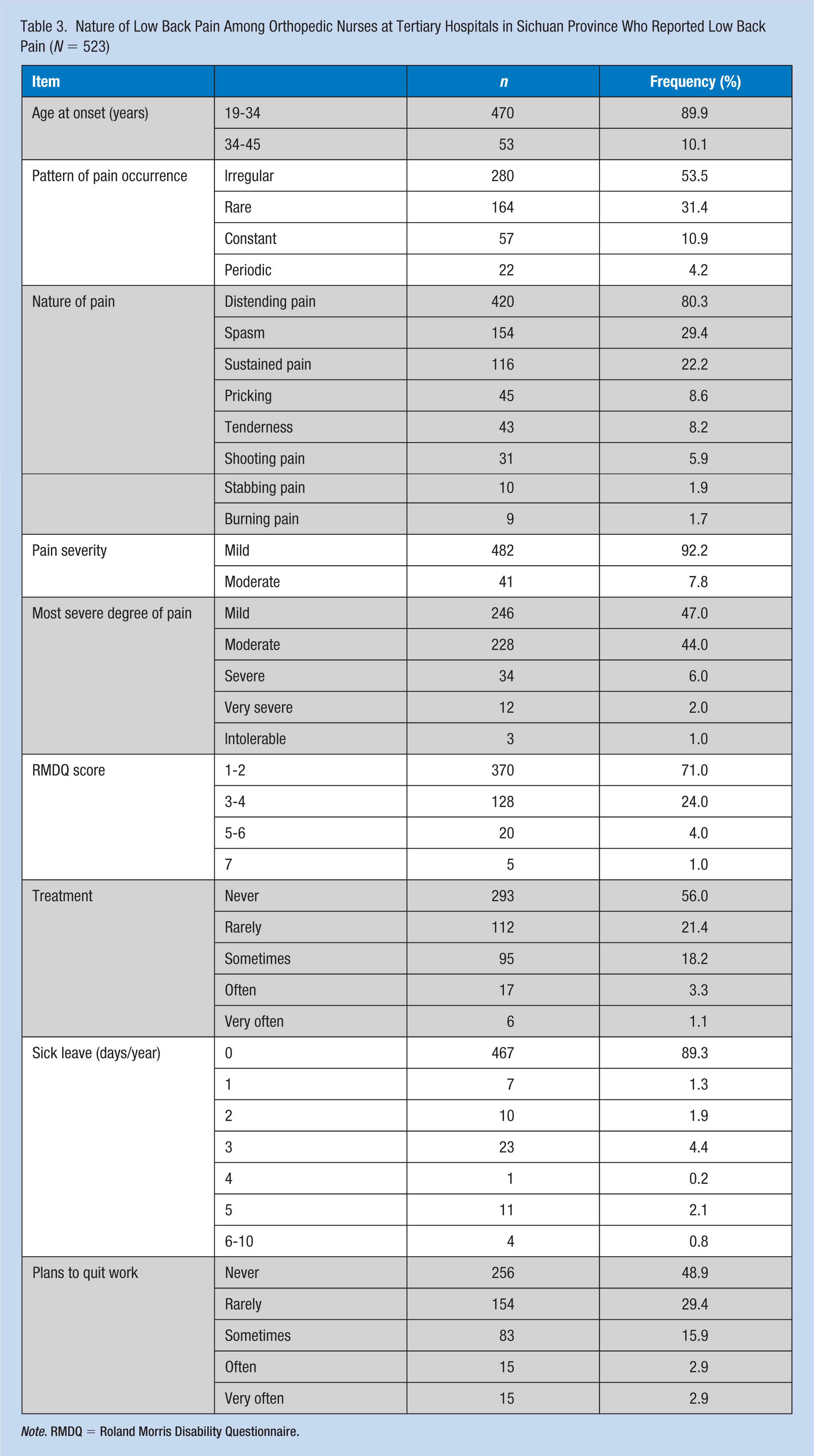
Note. RMDQ = Roland Morris Disability Questionnaire.
FABQ Score, Annual Number of Sick Days, and Annual Incidence of Episodes in Orthopedic Nurses Who Reported Low Back Pain at Tertiary Hospitals in Sichuan Province, China (N = 523)
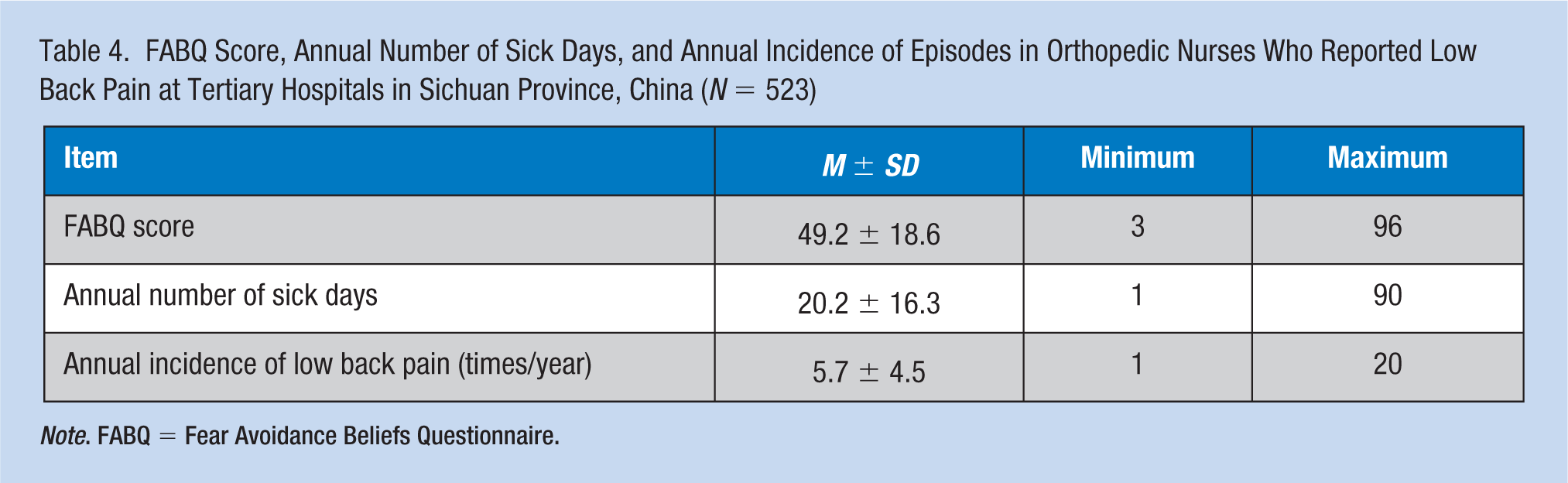
Note. FABQ = Fear Avoidance Beliefs Questionnaire.
For the RMDQ survey, 370 nurses (70.7%) scored 1 to 2 points, 128 (24.5%) scored 3 to 4 points, 20 nurses (3.8%) scored 5 to 6 points, and five nurses (1.0%) scored 7 points (Table 5). The top five responses to “because of LBP . . .” were “I change positions frequently to make my lower back comfortable,” “I bend or squat as little as possible,” “I avoid doing some heavy housework,” “I lie down to rest frequently,” and “I walk more slowly than usual.”
RMDQ LBP Scale Scores in Orthopedic Nurses With LBP at Tertiary Hospitals in Sichuan Province, China (N = 523)
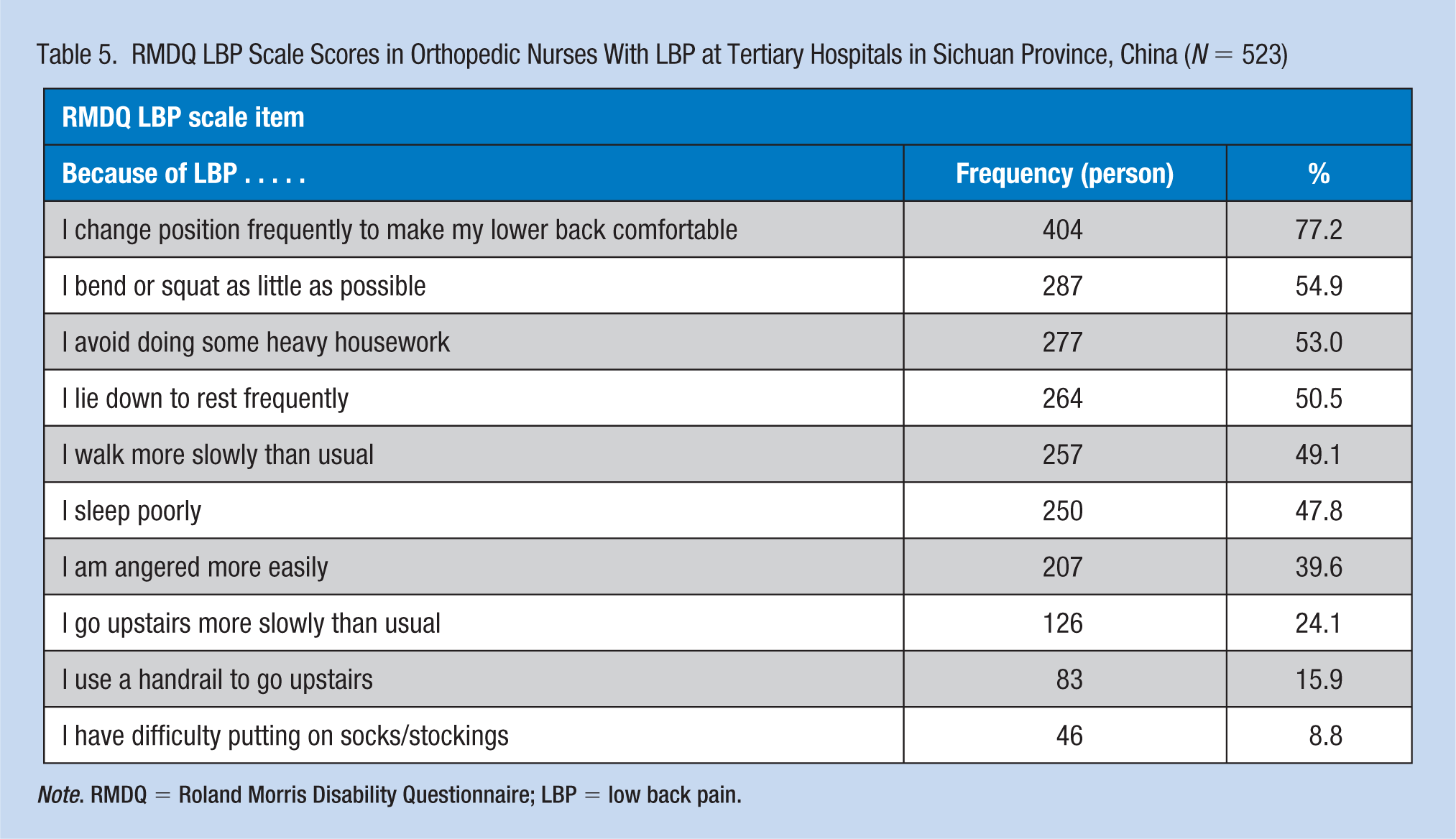
Note. RMDQ = Roland Morris Disability Questionnaire; LBP = low back pain.
Mild or moderate LBP was experienced by 474 of the 523 nurses (90.6%), with only 9.4% experiencing severe, very severe, or intolerable pain (see Table 6). More than half the orthopedic nurses (51.1%) planned to quit, and 5.8% thought of leaving their job due to LBP. The ideation to quit orthopedic nursing was also positively associated with having very/very severe/intolerable LBP relative to mild/moderate LBP (p < .001).
Frequency of Job Resignation Thoughts in Orthopedic Nurses Who Reported Low Back Pain at Tertiary Hospitals in Sichuan Province, China (N = 523)
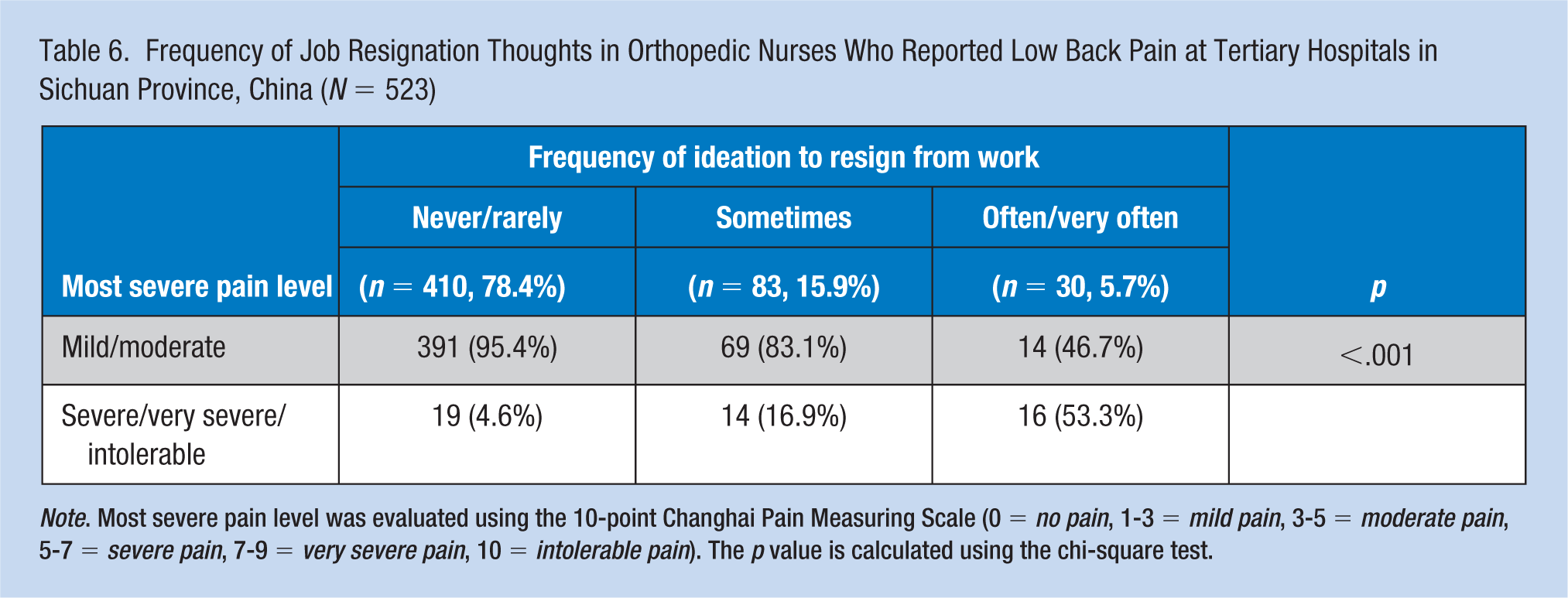
Note. Most severe pain level was evaluated using the 10-point Changhai Pain Measuring Scale (0 = no pain, 1-3 = mild pain, 3-5 = moderate pain, 5-7 = severe pain, 7-9 = very severe pain, 10 = intolerable pain). The p value is calculated using the chi-square test.
Discussion
According to our investigation, the annual prevalence and point prevalence of LBP was high (66.8% and 51.3%, respectively) in orthopedic nurses from tertiary hospitals in Sichuan province. The results of our surveys suggest that over half the orthopedic nurses planned to quit their jobs and 5.8% of the orthopedic nurses considered leaving their job due to LBP. In addition, ideation to resign from work increased with LBP severity.
LBP has certain characteristics and is either an irregular or continuous pain. The degree of pain in the study participants was mainly either mild or moderate and dysfunction predominantly manifested as mild disabilities. In our study, the annual prevalence of LBP in middle-aged orthopedic nurses (aged 35 to 55 years) was 75.4%, higher than the value of 63.8% in younger orthopedic nurses (aged 19 to 34 years). Similarly, other studies have reported that the odds of LBP are increased by 7% to 8% for each 1-year increase in age (Sadeghian, Hosseinzadeh, & Aliyari, 2014; Sanjoy, Ahsan, Nabi, Joy, & Hossain, 2017), suggesting that orthopedic nurses are more likely to have LBP with increasing age (Tan et al., 2014). Middle-aged orthopedic nurses had some severe LBP episodes and their physiology is more prone to degradation with increasing age, which increases occupational hazards and decreases back muscle strength and endurance (Tan et al., 2014). Consequently, middle-aged orthopedic nurses are more likely to develop LBP than younger nurses.
In our study, the top two responses in the RMDQ questionnaire were “Because of LBP, I change positions frequently to make my lower back comfortable” and “Because of LBP, I bend or squat as little as possible.” These findings are consistent with a previous report that orthopedic nurses have to frequently change posture for lower back comfort and tend to bend or squat as little as possible (He et al., 2013). However, orthopedic nurses have to bend or squat when they change bed sheets, turn patients on the bed, carry patients, assist patients with functional rehabilitation exercises, record the amounts of urine produced, carry out injections/infusions, and perform other common care-related procedures. Therefore, when LBP occurred, the nurses would have been limited in their ability to fully perform some of these procedures, which in turn would have affected the quality of their work. In addition, the orthopedic nurses in our study reported that they frequently had to lie down to rest at home and so were not able to do their usual housework because of LBP; this would have detrimentally affected their daily life, in agreement with the findings of previous research (Bentsen, Hanestad, Rustoen, & Wahl, 2008). Our results also show that the rate of treatment of LBP in orthopedic nurses was low. More than half the nurses who reported LBP had never received treatment and only 4.4% of orthopedic nurses said they often or always received treatment for LBP. Furthermore, one study found that Chinese nurses held more pessimistic views about the consequences of LBP than their Australian counterparts (Tan, Smith, O’Sullivan, Chen, & Burnett, 2015), and the number of patients that a nurse treats in China is higher than in most Western countries (Wu, Chi, Chen, Wang, & Jin, 2010). Indeed, it has been estimated that there are 1.05 nurses per 1,000 population in China as compared with 9.37 per 1,000 population in the United States (Kalisch & Liu, 2009). Most of the medical expenses arising from LBP were borne by the individual in this study. This suggests that measures should be taken to provide better occupational protection for nurses in China; these measures might include more planned breaks such as holidays, lower numbers of patients per nurse, and improved support for the medical needs of nurses with LBP. In addition, it may be helpful to implement educational programs to increase nurses’ awareness of LBP and its treatment and prevention (Sharafkhani, Khorsandi, Shamsi, & Ranjbaran, 2016).
The rate of sick leave for orthopedic nurses was low according to our investigation. Of 523 nurses who had LBP, 89.3% had never asked for leave and only 56 persons had asked for sick leave once. The cumulative amount of sick leave was only 1 to 3 days in 1 year. This is similar to another study of nurses in a tertiary care setting (Abolfotouh et al., 2015). The reason for this may be that a large proportion of the nurses in our study (90.6%) only suffered mild or moderate pain and their dysfunction was not obvious.
One major consideration from these results is that orthopedic nurses thought more often about leaving their profession when they experienced LBP. More than half the 523 nurses (51.1%) planned to quit due to LBP and 5.8% said they usually or often wanted to leave their job due to LBP. The nurses were also more likely to think about leaving their work as the pain became more severe. This is a problem that is likely to have an impact on nurse retention in orthopedic departments although the turnover of nurses was not measured in this study. To minimize the potential negative effects of LBP on nurse retention, we suggest that strategies are implemented to increase nurses’ awareness of the prevention and treatment of LBP. Furthermore, it should be explained that LBP is a common condition, and that fear and avoidance behavior can in fact worsen rather than alleviate the situation, resulting in reductions in activities of daily life and work ability. In addition, appropriate support and training should be provided by occupational health services to improve the working environment and promote the use of correct techniques (e.g., during lifting and carrying) to minimize lower back injury.
This study has some limitations. First, only orthopedic nurses were surveyed, so drawing any inferences from these results to other professional nurses should be done with caution. Second, only tertiary hospitals were investigated, so the applicability of these findings to primary and secondary hospitals is not known. Third, the study was limited to one province, so the generalizability of the findings to other regions of China is unknown. Fourth, the analysis did not investigate whether the use of mechanical lifting equipment/patient assist devices might be associated with the prevalence or severity of LBP.
Conclusion
Greater attention needs to be paid to mitigating the occupational hazards faced by orthopedic nurses to reduce the incidence and prevalence of LBP. To extend the current findings, we suggest that a prospective, longitudinal follow-up study over several years be carried out to describe the trends in LBP among orthopedic nurses over time. In addition, we would recommend repeating the study on a much wider scale in China to obtain details about the geographical distribution of LBP among orthopedic nurses.
Applying Research to Occupational Health Nursing Practice
Our study revealed that LBP interfered with the regular work of nurses in orthopedic departments, caused working days to be lost, and resulted in many nurses considering whether they should leave their job. The involvement of occupational health nurses would facilitate the design and implementation of educational and patient-handling programs to prevent and treat LBP in nurses in orthopedic departments, thereby reducing the number of working days lost and improving nurse retention. This could be supported by strategies to reduce fear and avoidance behavior and ensure adequate nursing resourcing in orthopedic departments to reduce the risk of injury.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Lingli Li, Female, PhD in Nursing, Associate Chief Nurse, Head Nurse of Orthopedics, Worked in Department of Orthopeadics, West China Hospital of Sichuan University, Chengdu 610041, China
Xiaofan Deng, Male, PhD in Medicine, Associate Chief Physician, Worked in Department of General Surgery, Sichuan Provincial people’s hospital, Chengdu 610041,China
Hongxia Zhang, Female, Bachelor Degree, Associatet Chief Nurse, Director of Nursing Department, Worked in Department of Nursing, Karamay Municipal People’s Hospital, Xinjiang, Karamay 0990, China
Hui Yang, Female, Master Degree, Supervisor Nurse, Worked in Department of Medical Oncology, Sichuan Provincial Cancer Hospital, Chengdu 610041, China
Jiali Chen, Female, Master Degree, Supervisor Nurse, International Wound Therapist, Worked in Department of Orthopeadics, West China Hospital of Sichuan University, Chengdu 610041, China
Xiaoling Hou, Female, Bachelor Degree, Associate Chief Nurse, Head Nurse of Orthopedics, Worked in Department of Orthopeadics, West China Hospital of Sichuan University, Chengdu 610041, China
Ning Ning, Female, Bachelor Degree, Professor, Postgraduate Tutor, Head Nurse of Surgical Department,Worked in Department of Orthopeadics, West China Hospital of Sichuan University, Chengdu 610041, China
Jiping Li, Female, Bachelor Degree, Professor, Doctoral Tutor, Worked in Department of Nursing,West China Hospital of Sichuan University, Chengdu 610041, China