
Abstract
This study aimed to estimate the point prevalence and 1-year period prevalence of skin disorder symptoms (SDS) among health care workers (HCWs) and to explore the possible risk factors. A random sample of 400 HCWs from 13 government health centers in Brunei Darussalam self-administered an adapted Nordic Occupational Skin Questionnaire (NOSQ-2002/SHORT). The point and 1-year prevalence of SDS were 12% and 19%, respectively. Having a history of SDS before the current job, exposure to SDS-exacerbating materials at the workplace, and having clinical roles were correlated for both prevalence estimates. Frequent handwashing and moderate use of latex gloves were associated with higher risk of SDS at 1-year. Female HCWs were more likely to report SDS. In multivariate analyses, only contact with SDS-exacerbating materials at the workplace, prejob SDS, and moderate glove usage were significant predictors of SDS.
Introduction
Occupational skin disease (OSD) is one of the most prevalent occupational diseases globally, second to musculoskeletal disorders (Diepgen, 2012; Kurpiewska, Liwkowicz, Benczek, & Padlewska, 2011). Broadly defined as the “excessive redness, infiltration of the skin, scaling, edema, blisters, areas of hyperkeratosis, cracks, erosions” on the hand, wrist, or forearm (Diepgen et al., 2015), hand eczema or dermatitis accounts for up to 90% of OSD in many industries, including the health care industry (Meding, 2000). It varies in type and is dependent on the triggers (Lakshmi & Srinivas, 2012). For example, irritant contact dermatitis (ICD) occurs as a result of exposure to mild irritants such as disinfectants, and allergic contact dermatitis results from an exposure to allergic substances such as fragrance, whereas atopic dermatitis typically has biological causes (Coenraads, 2012). Other types of hand eczema with varied etiologies and those with no known etiology also exist (Lakshmi & Srinivas, 2012).
Studies have reported a high prevalence of skin disorders among health care workers (HCWs). For instance, up to 8% of nurses in Taiwan, 11.8% in Korea, 27.6% in Japan, and 70% in India have reported the occurrence of hand dermatitis (Bhatia & Sharma, 2017). In Australia, 81% of HCWs were diagnosed with occupational skin disease (Higgins, Palmer, Cahill, & Nixon, 2016). Compared with other occupations, HCWs have been reported to be disproportionately affected by OSDs. In Poland, for example, HCWs (41% physicians, 67% midwives, and 64% dentists) had reported higher occurrence of OSDs than non-HCWs (18% bartenders, 18% painters, and 41% welders; Kurpiewska et al., 2011). Similar findings of higher prevalence of OSD among HCWs than non-HCWs were also reported in the United States, with female HCWs being more affected (Kadivar & Belsito, 2015). Personal history of SDS was also found to aggravate OSDs (Yan, Wang, Wu, & Xu, 2015).
The high incidence of OSDs among HCWs was correlated with exposure to occupational agents such as latex gloves, certain medications, disinfectants, wet work, as well as cleaning detergents used in a health care facility (Graeve et al., 2017; Liu et al., 2013; Zack, Arrandale, & Holness, 2017). Allergic contact dermatitis (ACD) among HCWs was mainly caused by exposure to occupational agents such as thiuran mix (a chemical found in rubber gloves) and formaldehyde; whereas ICD was triggered by excessive wet work, use of alcohol-based hand rubs and other hand cleansers (Higgins et al., 2016; Kadivar & Belsito, 2015). The implications of OSD in HCWs include impaired quality of life, loss of productivity due to sickness absenteeism, change of occupation, monetary compensation, and even disability (Higgins et al., 2016; Lakshmi & Srinivas, 2012; Liu et al., 2013; Oranye, 2018).
This epidemiologic study of OSD was carried out to estimate the prevalence of aggregated SDS and to determine their contributing factors among HCWs in Brunei Darussalam. It is also aimed at developing appropriate preventive and counteractive strategies such as workplace training, health education programs, and policy enactments.
Method
Study Design
This is a cross-sectional study of self-reported SDS among HCWs measured using an adapted Nordic Occupational Skin Questionnaire (NOSQ-2002/SHORT; Susitaival et al., 2003).
Study Subjects and Eligibility
The sample was randomly drawn from 13 government health care facilities via cluster sampling. Cluster sampling allowed for a representative sample from all districts in Brunei Darussalam. There are four districts in Brunei Darussalam, each with an average of 12 health facilities. Three health facilities were randomly drawn from each district (n = 12). We also added the only tertiary and largest health facility for a total of 13 health facilities included in this study. At every health facility, depending on staff population and eligibility criteria, 20 to 35 HCWs among 40 to 50 HCWs present in the facility self-administered the questionnaire. To be included, HCWs had to be older than 18 years of age, employed in a clinical or nonclinical role for at least 1 year, and a willingness to participate via written consent. Clinical roles (e.g., medical doctors and dentists) and nonclinical roles (e.g., medical record clerks and social workers) were defined according to Campion et al. (2015).
Data Collection
The HCWs self-administered an adapted and validated English version of NOSQ-2002/SHORT (Susitaival et al., 2003). For the question “When did you last have eczema on your hands, wrists or forearms?” two answer options were retained: “I have just now” and “between 6 and 12 months.” The latter was then modified to “I have had it in the last 12 months (and not necessarily now).” We defined “I have it now” as point prevalence and “I have had it in the past 12 months” as 1-year prevalence, in this study. The adapted NOSQ-2002/SHORT was tested for reliability and validity and found to be acceptable (overall interrater reliability = .90 and Cronbach’s α = .88). Data collection among participants occurred from March to May 2017.
Outcome Definition
Skin disorder symptoms in this study was defined as any form of hand eczema exhibited by the presence of any “excessive redness, infiltration of the skin, scaling, edema, blisters, areas of hyperkeratosis, cracks, erosions” on the hand, wrist, or forearm (Diepgen et al., 2015; Susitaival et al., 2003).
Data Analysis
The point prevalence and 1-year prevalence estimates were expressed in frequencies and 95% confidence intervals (CIs). Chi-square test (Mchugh, 2013) was used to assess the level of difference in SDS between groups such as between male and female HCWs. Multiple logistic regression was used to calculate the odds ratios to identify which of the variables among gender, job role, contact with any material at work worsened SDS, such as frequency of handwashing, usage of latex gloves. A history of SDS before the current job was associated with SDS.
In the regression models, forward Likelihood Ratio (LR) methods were used for variable selection, and possible interaction terms were checked. Multicollinearity was checked using Variance Inflation Factor (VIF) and the model of of fitness was assessed with Hosmer-Lemeshow test. Multicollinearity was defined as a variable with VIF of >10, and Cook’s influential statistics >1 was considered an influential outlier (Sarkar, Midi, & Rana, 2011). A statistical difference at p < .05 (two-sided) was considered significant. IBM|SPSS version 22.0 was used for all analyses.
Ethical Considerations
Written consent was obtained from the study participants. The study protocol was reviewed and approved by the Joint Research Ethics committee of Institute of Health Sciences, Universiti Brunei Darussalam and Ministry of Health, Brunei Darussalam.
Results
Sample Characteristics
Of 510 HCWs invited, 400 responded and completed the survey (response rate 78.4%), representing about 9.5% of the estimated total number of workers employed in the health sector in Brunei Darussalam (Brunei Ministry of Health, 2016). Seventy-seven percent of the sample were females (n = 308), and 23% were males (n = 92), of whom 56% (n = 222) had clinical roles (Table 1; 142 nurses, 51 doctors of all grades, 20 midwives, 5 phlebotomists, and 4 dentists) and 44% (n = 178) had nonclinical roles (63 pharmacy technicians, 36 pharmacists, 34 medical record officers/clerks, 15 housekeepers/cleaners, 12 health inspectors, 11 social workers, 4 biomedical engineers, and 3 health education officers; data not shown). The mean (SD) age was 42 (19.6) years (range: 20-63 years).
Association of SDS With Demographic and Occupational Factors (n = 400)
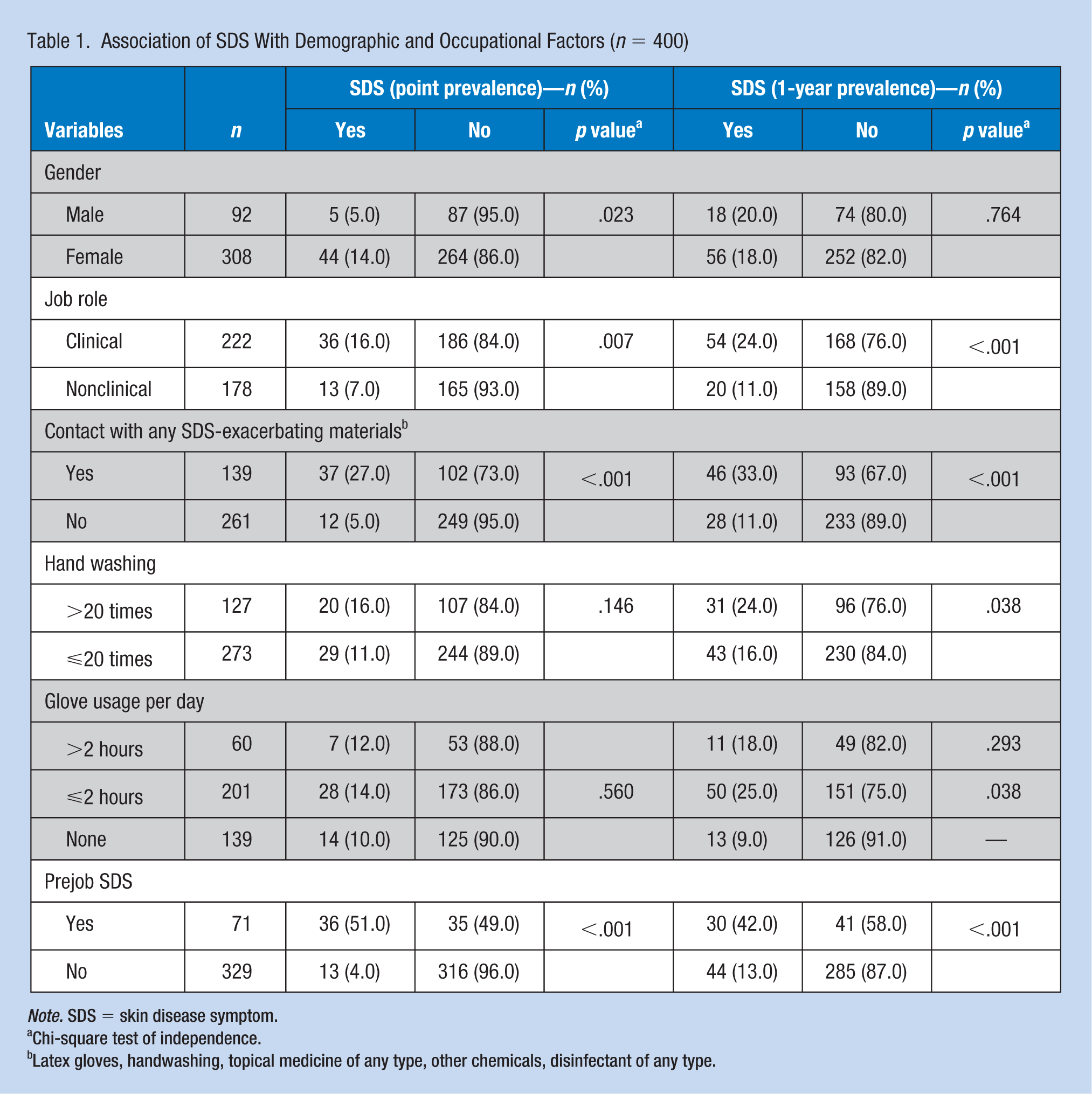
Note. SDS = skin disease symptom.
Chi-square test of independence.
Latex gloves, handwashing, topical medicine of any type, other chemicals, disinfectant of any type.
Prevalence of SDS Among HCWs
Point prevalence
The prevalence of participating HCWs with SDS at the time of the survey was 12.0%. Clinical staff (16%) reported a higher occurrence of SDS than nonclinical staff (7%; p = .007), whereas female HCWs (14%) reported higher occurrence than their male counterparts (5%; p = .023; Figure 1 and Table 1).
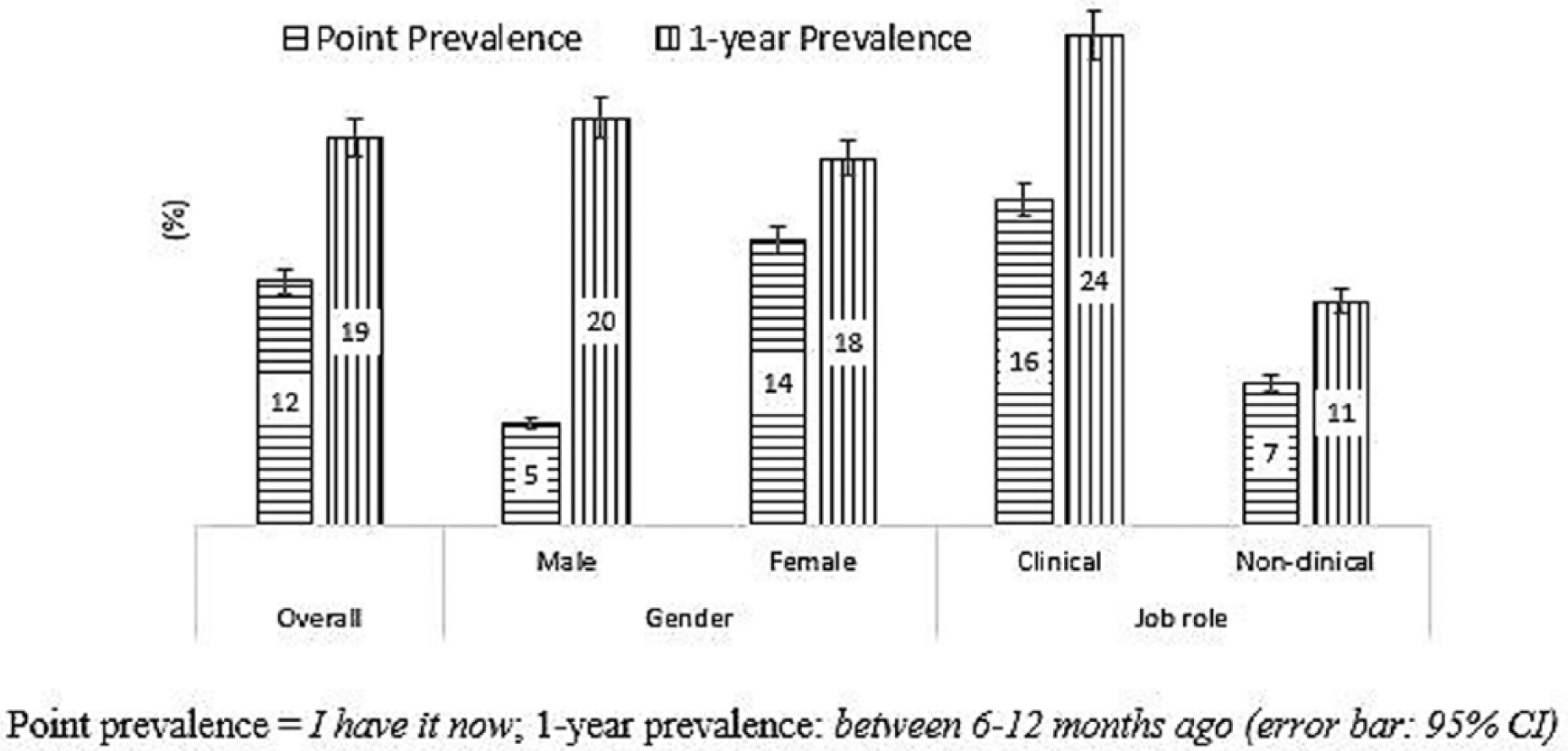
Self-reported SDS on hands, wrist, or forearm among HCWs (n = 400).
1-year prevalence
The 1-year prevalence of SDS among the sampled HCWs in Brunei Darussalam was 19.0%. Similar to point prevalence, clinical staff reported a higher occurrence of SDS (24.3%) than nonclinical staff (11%; p < .001). However, the difference between SDS occurrence in females (20%) and males (18%) was not significant (Figure 1 and Table 1).
SDS-Exacerbating Materials at the Workplace
The proportion of SDS-exacerbating materials at the workplace as reported by the HCWs for both point prevalence and 1-year prevalence were 2% for latex gloves, 2% for handwashing, 3% for topical medicine of any type, 4% for other chemicals, 5% for disinfectant of any type, and 19% for a combination of two or more of the aforelisted materials. Of the total sample, 20% believed their skin symptoms improved when they were away from the workplace (on weekends or leaves), 5% did not believe so, and 12% did not know (data not shown).
Association of SDS With Occupational Factors Among HCWs
Point prevalence
There was a higher occurrence of SDS among HCWs who reported contact with any SDS-exacerbating material at the workplace (27%) compared with those who did not have any contact with such materials (4.6%; p < .001). Similarly, HCWs with a history of SDS before their current job (51%) reported a higher occurrence of SDS than HCWs without a history of SDS (4%; p < .001). However, there was no significant difference in SDS occurrence between HCWs who used latex gloves for more than 2 hours per day/shift (12%), used latex gloves moderately (2 hours or less per day/shift; 14%), and HCWs who did not use latex gloves (10%). Also, there was no significant difference between HCWs who washed their hands frequently (>20 times per day; 16%) and those who washed their hands less frequently (20 times or less a day; 11%; Table 1).
1-year prevalence
Significant difference were seen in the occurrence of SDS between clinical staff (24%) and nonclinical staff (11%; p < .001), between HCWs with contact with any SDS-promoting materials at the workplace (33%) and HCWs with no contact with any SDS-promoting materials at the workplace (11%; p < .001), and between HCWs with history of SDS before their current job (42%) and HCWs without history of SDS before their current job (13%; p < .001).
HCWs who washed their hands more than 20 times a day (24%) reported higher SDS than HCWs who washed their hands 20 times or less a day (16%; p < .05). Likewise, HCWs who used latex gloves for 2 hours or less per day/shift (25%) reported significant higher occurrence of SDS than HCWs who did not use latex gloves at all (9%; p < .038), and no significant difference between HCWs who wore latex gloves for more than 2 hours per day/shift (18%; p = .293; Table 1).
Risk Factors for SDS Among HCWs
Point prevalence
Univariate logistic regression showed that female HCWs had three times the odds of reporting SDS than their male counterparts (p = .014), clinical staff had 2.5 times higher odds than nonclinical staff (p = .006). HCWs with exposure or contact with SDS-promoting materials at the workplace were 7.5 times more likely to report SDS than those who did not have such exposure or contact (p < .001), and HCWs with prejob SDS had 25 times the odds of having SDS than those with no prejob SDS (p < .001; Table 2).
Factors of SDS Among HCWs Using Univariate Logistic Regression (n = 400)
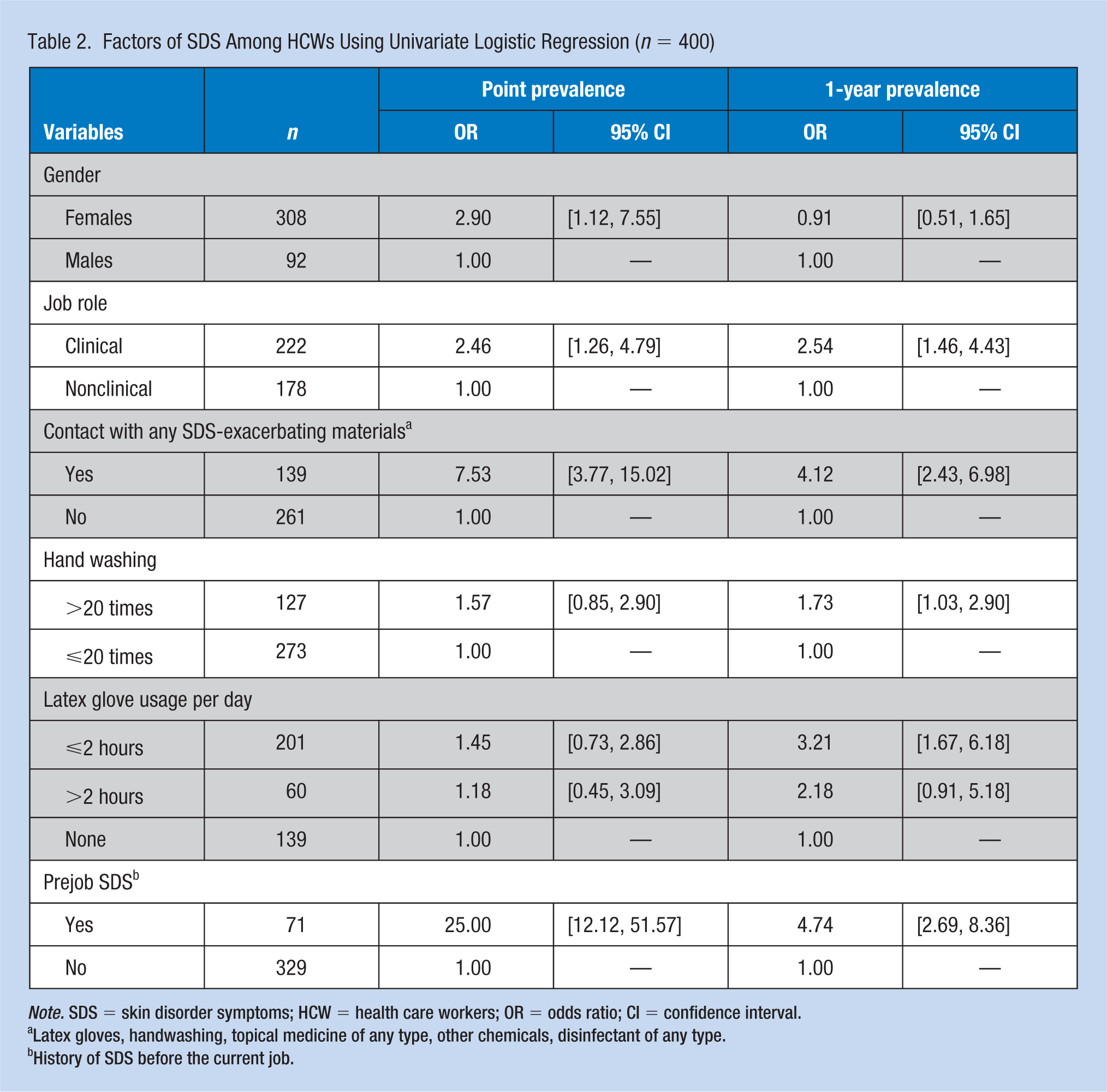
Note. SDS = skin disorder symptoms; HCW = health care workers; OR = odds ratio; CI = confidence interval.
Latex gloves, handwashing, topical medicine of any type, other chemicals, disinfectant of any type.
History of SDS before the current job.
In the multivariate analyses, only two factors (contact with SDS-promoting materials at work and prejob symptoms) out of the 5 factors considered (others being: gender, clinical or nonclinical role, and use of latex gloves), contributed to 22% causal factors predicting the occurrence of reported SDS among HCWs (Coz & Snell R2 = .223), remained significant in the multiple logistic regression model. The adjusted odds of reporting SDS was 3.7 times higher among HCWs with exposure to SDS-promoting materials at the workplace than those with no such exposure (p < .001), and 17 times higher for HCWs with prejob SDS than those with no prejob SDS (p < .001; Table 3).
Factors of SDS Among HCWs Using Multiple Logistic Regression (n = 400)
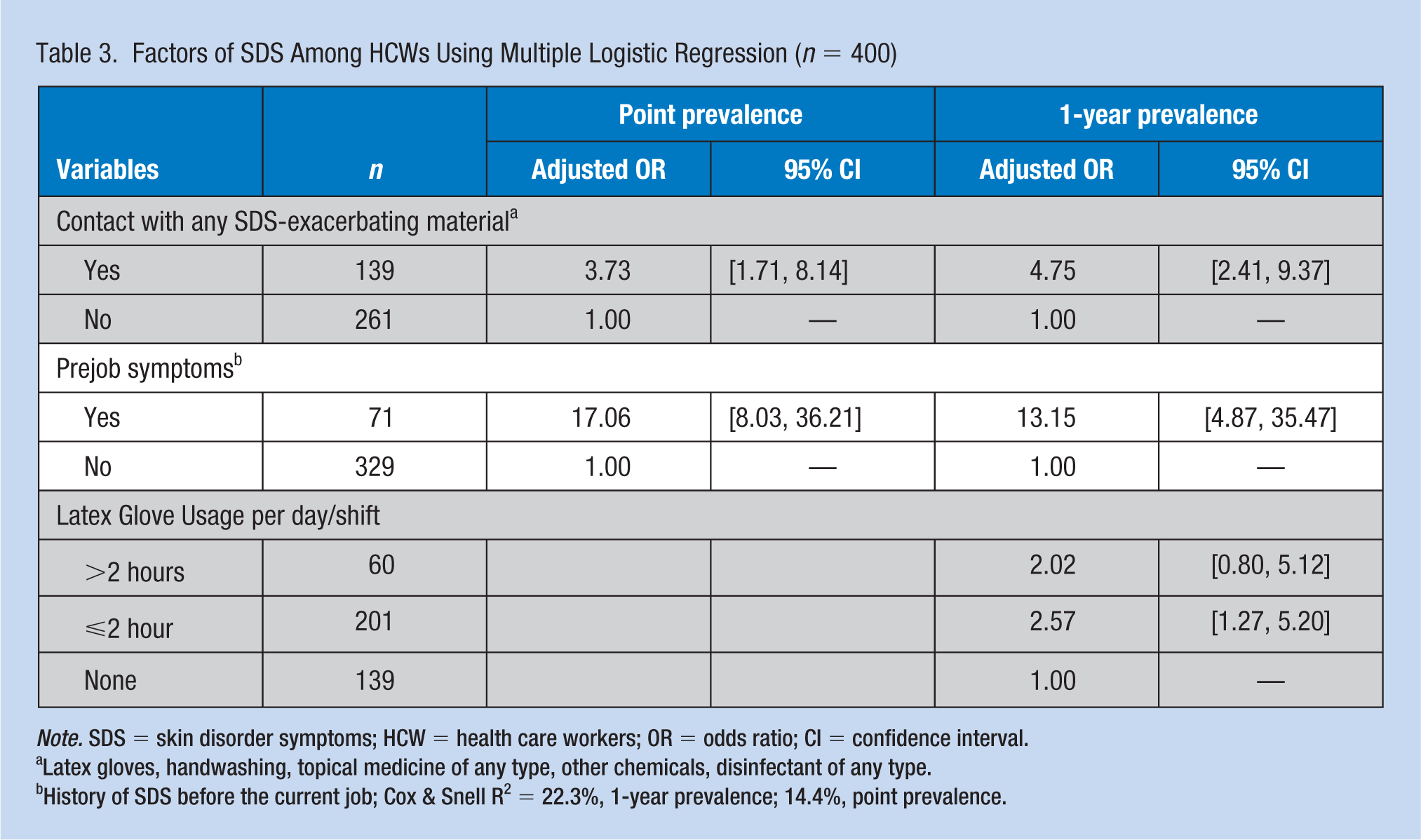
Note. SDS = skin disorder symptoms; HCW = health care workers; OR = odds ratio; CI = confidence interval.
Latex gloves, handwashing, topical medicine of any type, other chemicals, disinfectant of any type.
History of SDS before the current job; Cox & Snell R2 = 22.3%, 1-year prevalence; 14.4%, point prevalence.
1-year prevalence
When using simple logistic regression, clinical staff showed 2.5 times higher odds of reporting SDS than nonclinical staff (p < .001), four times higher for HCWs with exposure to SDS-promoting materials than those who did not have such exposure (p < .001), and 1.73 times higher odds for HCWs who washed their hands for more than 20 times per day than those who washed their hands for 20 times or less a day (p = .041). The odds of reporting SDS among HCWs with prejob SDS were 4.7 times higher than those without prejob SDS (p < .001). HCWs who used latex gloves for 2 hours or less per day/shift were three times more likely to report SDS compared with those who did not use gloves (p < .001), but the difference between those who wore latex gloves for >2 hours per day/shift and those who did not use latex gloves at all was borderline insignificant (p = .079; Table 2).
The HCWs who used latex gloves for 2 hours or less per day/shift were 2 times more likely to report SDS compared with those who did not use latex gloves (p = .009), but the difference between those who wore latex gloves for >2 hours per day/shift and those who did not was not significant. HCWs with prejob SDS were 13 times more likely to report SDS than those with no prejob SDS (p < 0.001); HCWs with contact with SDS-promoting materials at the workplace were five times more likely to report SDS than those with no such contact (p < .001). Three factors (use of latex gloves, contact with SDS-promoting materials at the workplace, and prejob SDS) remained relevant in the adjusted model and contributed about 14% of the causal factors predicting the occurrence of reported SDS among HCWs (Coz & Snell R2 = .144; Table 3). The logistic regression models no multicollinearity (VIF < 10) nor influential outlier (Cook’s influential statistics < 1) and fit well (Hosmer–Lemeshow test: p > .05) for both point prevalence (p = .139) and 1-year prevalence (p = .146) models.
Discussion
Our study found that occupational skin disease was a problem among our sample of HCWs employed at health care facilities in Brunei Darussalam, with point prevalence and 1-year prevalence of 12% and 19%, respectively. Factors such as prejob SDS, exposure to SDS-promoting materials at the workplace, and having clinical roles were associated with higher risks of SDS occurrence at both point prevalence and 1-year prevalence. Frequent handwashing and moderate latex glove use were linked with higher risk of SDS among HCWs at 1-year prevalence, but not at point prevalence. Female HCWs, compared with their male counterparts, were more likely to report SDS at point prevalence, but not at 1-year prevalence. In multivariate analyses, contact with SDS-promoting materials at the workplace, prejob SDS and glove usage for less than 2 hours per day/shift (only at 1-year prevalence) were significantly associated with SDS among HCWs in Brunei Darussalam. The most reported SDS-exacerbating materials at the workplace were the combination of two or more occupational materials such as disinfectants and latex gloves.
Our results are generally comparable with findings of other studies conducted in other countries. For example, a cross-sectional study of self-reported work-related skin symptoms among HCWs in the United Kingdom in 2013 reported an overall point prevalence of 15% (Campion et al., 2015). Clinical role, history of hand dermatitis, and excessive handwashing and exposures to certain materials at the workplace were factors associated with higher proportion of work-related skin symptoms. A similar study among HCWs in Denmark found excessive handwashing to be a significant predictor of hand dermatitis (Ibler, Jemec, & Agner, 2012).
Another survey among Swedish dentists reported 14% 1-year prevalence of self-reported hand eczema, which was confirmed by a clinical investigation in 94% of them; ICD was confirmed in 67%, and ACD in 28% of the dentists (Wallenhammar et al., 2000). In another clinical examination of patients who underwent patch test to confirm their skin disorders from 1994 to 2014 in two American cities (Kansas and New York), there was higher prevalence of hand dermatitis in HCWs compared with non-HCWs, with females having occurrences of work-related ICD (and less occupational ACD) than their male counterpart (Kadivar & Belsito, 2015). Similar findings of females HCWs having a higher occurrence of hand dermatitis than their male counterparts was reported elsewhere (Kadivar & Belsito, 2015). The female HCWs likelihood of reporting skin symptoms more than the male HCWs have been attributed to their disproportionately higher exposures to nonoccupational triggers (Meding, 2000). Prejob personal history of skin disease as a major indicator of OSD was reported in China, where sanitation workers had a significantly higher occurrence of OSD compared with administrative staff (Yan et al., 2015).
Our study is not without limitations. The self-reporting of SDS, unlike clinical examinations, has been criticized for its tendency to overestimate skin disorders (Campion et al., 2015; Ibler et al., 2012; Liu et al., 2013). Furthermore, our study only highlighted the overall extent of aggregated SDS among HCWs thereby suggesting the need for further studies among HCWs in Brunei Darussalam. However, one of the strengths of our study is that the HCWs assessed were a representative sample of HCWs in Brunei Darussalam.
Our study established the aggregated prevalence of SDS, and some of their associated factors, among the sample of HCWs in Brunei Darussalam. This is the first study to do so, thereby setting the baseline description of the extent of SDS in the country. This is important because, although the epidemiology of occupational skin diseases in Europe and other Western countries are often available due to the presence of reporting and notification systems, data on occupational skin diseases in Asia are limited due to the lack of established OSD reporting systems (Bhatia & Sharma, 2017).
The findings have shown that self-reported skin disorders and their exacerbating factors are widespread among HCWs, thereby laying a foundation upon which further studies and workplace health promotion programs will need to be built upon.
Applying Research to Practice
Approximately two in every 10 health care workers (HWCs) in our study reported at least one skin disorder symptoms (SDS) in the past year. Some of the reported risk factors for the SDS at the workplace include having prejob SDS, contact with certain materials at the workplace and the use of latex gloves. Upon hiring, HCWs should be evaluated for a history of SDS to determine if they are at risk of developing occupational skin disease (OSD) and plan preventive and supportive strategies. A further assessment of the materials at health facilities should be carried out to determine which specific materials that SDS and OSD and find ways to replace or reduce exposure.
Footnotes
Acknowledgements
We greatly appreciate the support of the Director General of Health Services, Director General of Medical Services, and the RIPAS Hospital Chief Executive Officer, as well as contribution from staff of the Occupational Health Division Ministry of Health, Brunei Darussalam.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Mohammed Mohammed Alhaji is a PhD Candidate in Public Health at the Universiti Brunei Darussalam, and trains with the University of Cambridge for a year-long Leading Change course, courtesy of The Queen Elizabeth’s Young Leader Award. His research training and interests traverse the public health spectrum, from biostatistics and epidemiology to health policy and social determinants of health.
Alice Lai is a Specialist in Occupational Medicine at the Occupational Health Division, Ministry of Health, Brunei Darussalam. She is also an Adjunct Senior Assistant Professor at the Universiti Brunei Darussalam and teaches the OEH module of the MPH programme. She has a keen research interest in healthcare workers and has authored and co-authored several papers on topics related to occupational health.
Lin Naing is a Biostatistician with a wide Public Health background, at the Universiti Brunei Darussalam. His research interests are in occupational diseases, questionnaires development and validation, and cancer survival studies.
Nik Ani Tuah is an academic and researcher in Public Health at the Universiti Brunei Darussalam. In the last 10 years, she has developed knowledge, expertise and skills in research on NCDs prevention and control, particularly in human behavior modifications. Her current research interest focuses on developing and using m-Health to assist individuals in controlling excess body weight and promoting health at schools, community and workplace settings.